Article Text

Abstract
Objectives To assess the trends concerning utilisation of maternal and child health (MCH) services before, during and after the Ebola outbreak, quantifying the contribution of a reorganised referral system (RS).
Design A prospective observational study of MCH services.
Setting Pujehun district in Sierra Leone, 77 community health facilities and 1 hospital from 2012 to 2017.
Main outcome measures MCH utililization was evaluated by assessing: (1) institutional deliveries, Cesarean-sections, paediatric and maternity admissions and deaths, and major direct obstetric complications (MDOCs), at hospital level; (2) antenatal care (ANC) 1 and 4, institutional delivery and family planning, at community level. Contribution of a strengthened RS was also measured.
Results At hospital level, there is a significant difference between trends Ebola versus pre-Ebola for maternal admissions (7, 95% CI 4 to 11, p<0.001), MDOCs (4, 95% CI 1 to 7, p=0.006) and institutional deliveries (4, 95% CI 2 to 6, p=0.001). There is also a negative trend in the transition from Ebola to post-Ebola for maternal admissions (−7, 95% CI −10 to −4, p<0.001), MDOCs (−4, 95% CI −7 to −1, p=0.009) and institutional deliveries (−3, 95% CI −5 to −1, p=0.001). The differences between trends pre-Ebola versus post-Ebola are only significant for paediatric admissions (3, 95% CI 0 to 5, p=0.035). At community level, the difference between trends Ebola versus pre-Ebola and Ebola versus post-Ebola are not significant for any indicators. The differences between trends pre-Ebola versus post-Ebola show a negative difference for institutional deliveries (−7, 95% CI −10 to −4, p<0.001), ANC 1 (−6, 95% CI −10 to −3, p<0.001), ANC 4 (−8, 95% CI −11 to −5, p<0.001) and family planning (−85, 95% CI −119 to −51, p<0.001).
Conclusions A stronger health system compared with other districts in Sierra Leone and a strengthened RS enabled health facilities in Pujehun to maintain service provision and uptake during and after the Ebola epidemic.
- paediatrics
- public health
- community gynaecology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study uses data from a remote rural district in Sierra Leone, with a 6-year observational period. Data have been collected in a prospective way, reducing the potential bias in the accuracy of the data reported by other studies carried out in countries affected by Ebola.
Data from pre, intra and post-Ebola periods allowed comparisons between trends, something rarely carried out in countries heavily affected by Ebola.
The data refer to a single area of Sierra Leone: the sample cannot be considered representative of the country as a whole.
In addition to measures put in place to reduce the impact of the disease on mothers and children, Pujehun had far fewer Ebola cases than other districts, which may also have led to the utilisation of health services.
Introduction
The 2014–2015 Ebola virus disease (EVD) outbreak was the most severe in history, mainly affecting three West African countries; Guinea, Sierra Leone and Liberia. Overall 28 616 people were infected of which 11 310 died and the outbreak was declared a global public health emergency by the WHO.1 Of the three countries affected, Sierra Leone had the most confirmed cases (8704), which accounted for 50% of all confirmed cases in West Africa, and 3589 deaths.2–4 All 14 districts in Sierra Leone were affected, but at different times and to varying degrees.5 During the Ebola crisis, the population’s trust in the national health system declined in Sierra Leone, leading to an overall reduction in the use of health services, including reproductive, maternal and child services.6–8 Underlying factors for the decrease in the use of health services included fear of infection, for both healthcare workers and patients, the underlying fragility of the health systems, the reduced numbers of available health personnel and the death of healthcare workers due to EVD.9 10 It has been estimated that 30% of health workers who died of EVD in West Africa were maternal and child health (MCH) care providers.11 However, there were considerable variations in the reduction of health service uptake when looked at by district level in Sierra Leone.6 12–14 While districts such as Kambia, Port Loko and Bonthe showed large reductions in facility-based delivery (between 38% and 41%), the district of Pujehun showed only a 5% decrease in the same service. Similar geographic variations were seen in the reduction in antenatal care (ANC) visits.12 13
The number of confirmed EVD cases—and deaths—varied considerably by district. There were no >100 confirmed cases in both Bonthe and Pujehun, and up to 4000 confirmed cases in both Port Loko and Bombali.15 However, public fear of Ebola, regardless of the actual number of cases per district, may still have prevented many people from accessing services. The challenge of providing adequate levels of care during a humanitarian emergency such as the EVD crisis was further exacerbated by the weak health system in Sierra Leone, particularly in rural areas where the poor condition of the roads and high transport costs cause delays in accessing services, and contribute to increased maternal and neonatal mortality.16
Doctors with Africa (DwA) CUAMM is an Italian non-governmental organization (NGO) working in Sierra Leone since 2012. It is present in the Pujehun district focusing on MCH care both at hospital and community level.17 18 In this paper, community level refers to peripheral health units (PHUs), that is, all health facilities outside the hospital. As described in our previous reports,17 18 a number of measures were put in place to control the Ebola epidemic in the Pujehun district which might have reduced the impact of the disease on mothers and children compared with other districts. During this EVD epidemic, the predominantly vertical focus on outbreak control was associated with failures in providing effective care for routine health needs.19–21 In contrast, the approach implemented in the Pujehun district was not based on vertical actions and ‘humanitarian response to health emergencies with a short half-life’.21 Rather, it worked on strengthening all the components of the health system—governance, human resources, community involvement—before, during and after the epidemic. A rapid response to the crisis by the local health authorities was implemented adopting public health measures before any other district in Sierra Leone.22 The activities were mainly concentrated on keeping the health service open and properly functioning in order to reduce the collateral effects of the epidemic on routine health services. No health units in the Pujehun district were closed during the epidemic. Measures to empower community leaders and use culturally appropriate methods of communication helped to dispel community mistrust in the health services. At community level, a number of strategies were implemented such as the regular rotation of health facility staff, which strengthened teamwork and effective leadership. In Sierra Leone, healthcare workers based at community health centres may often work alone in isolated centres with limited support from clinical colleagues or management. By rotating staff through the various facilities, they gain on the job training, peer support and develop new working relationships. At the start of the Ebola epidemic, many expatriate healthcare workers in NGOs left Sierra Leone, negatively affecting care delivery and staff morale. The continued presence of international teams in the daily activities in Pujehun hospital and the acceptance of the professional risks by both national and international staff may have contributed to maintaining an attitude of ‘normality’ in an extremely stressful environment. This might also help to explain the population’s positive receptiveness towards the health services.17 18
Different types of referral systems (RSs) such as motorbikes were present in the country in the pre-Ebola period to transport patients from the villages to the nearest health facility. Ambulances were also present in several districts with 73% of health facilities nationwide having a functioning RS, 59% of them consisting of an ambulance on call.12 23 In the Pujehun district, the RS was barely functioning, only able to support the activity of a limited number of PHUs. The service was also entirely funded by the patients themselves, resulting in underutilisation of the service. Utilisation was further reduced during the outbreak, when the ambulances were identified by the population with the transport of Ebola-infected patients, and their use occasioned fear and distrust. In January 2015, in collaboration with the Ministry of Health and Sanitation (MoHS) of Sierra Leone and UNICEF, DwA began the reorganisation and reinforcement of the RS, transferring pregnant women and paediatric cases from PHUs to the Pujehun hospital.
Our previous studies18 provided information only on three MCH indicators, namely paediatric admissions, maternity admissions and institutional deliveries; in addition, it did not assess the trends in the post-EVD period. Existing studies examining the influence of EVD on MCH services targeted the outbreak and the immediate post-outbreak periods.24–27 Understanding the trends in the use of MCH services before, during and after the EVD outbreak will help to guide post-EVD interventions, increasing access to MCH services in rural Sierra Leone. This information will also be useful in preparing a more organised and structured RS. With this background, the aims of this study are (1) to assess trends in institutional deliveries, C-sections, paediatric and maternity admissions, paediatric and maternity deaths, and major direct obstetric complications (MDOCs), before, during and after the EVD in the Pujehun hospital, thus complementing the results of the previous report which were limited to three MCH indicators; (2) to assess trends in ANC 1 and 4, institutional delivery and family planning, at community level. This study was carried out in conjunction with the strengthening of an RS initiated a few weeks after the Pujehun district was declared Ebola-free.
Methods
Setting
Sierra Leone has four provinces that are divided into 14 districts. Pujehun is one of four districts in the southern province (figure 1). It has a population of ~375 000 inhabitants. The primary care network included 77 MoHS PHUs, 5 of which provide basic emergency obstetrics care (BEmOC). The secondary care system consists of the MoHS provided district hospital, which comprises the MCH complex, providing comprehensive emergency obstetric and newborn care (CEmONC) services. Connections between the community and health facilities are difficult because of the very poor condition of the roads. Furthermore, the district is divided by a major river (Moa River) and has a riverine area reachable only with boats, which further hinders access. The first case of Ebola in Pujehun district was reported on the 7 July 2014. The district was declared Ebola free on the 10 January 2015.28 A total of 49 patients were registered with a case fatality rate of 85.7% (42/49).

Study area, the Pujehun district in Sierra Leone.
Referral system
In the Pujehun district, two ambulances managed by the District Health Management Team (DHMT) were functioning in the pre-Ebola period, but only 63% of the PHUs were able to use the service.12 23 Emergency calls were not coordinated by the hospital and the transport costs were covered by the patients, dissuading many from using the service. During the outbreak, people came to associate the ambulances with transporting Ebola-infected patients, which further discouraged their use. A 24-hour free-of-charge ambulance RS, transferring pregnant women with obstetric complications from the health centres to Pujehun hospital was implemented in January 2015. In the hospital, a call centre was established and the call centre number was distributed to all the 77 PHUs. Private calls were considered only in the case of an emergency or if the staff of the PHU were not available. After confirming an emergency condition together with the PHU staff, the hospital midwife had the responsibility to authorise the referral. A nurse on duty from the maternity hospital accompanied the driver in each referral. Health personnel at hospital and PHUs levels were trained on Life Saving Skills—Emergency Obstetric and Newborn Care, including referral criteria and definition of MDOCs.29
Referrals were carried out by three ambulances, two positioned in the Pujehun MCH complex, and a third one in Jendema, bordering Liberia, on the opposite side of the Moa River. Around the Jendema area, 15 PHUs were located serving a population of ~80 000 inhabitants. Referrals in this area were made using the ambulances and by transferring patients at the river crossing point via a barge or a motor boat, depending on the flow rate of the river. Paediatric referrals were performed using private motor bikes available in the villages and hired from PHUs staff without the involvement of the call centre. A referral form describing the clinical case and the justification for the referral was distributed to all the PHUs. The bike rider, after bringing the patient to the paediatric ward, delivered the referral form and received the reimbursement. For all patients carried to the hospital information was collected, including demographics, location and the reason for contacting the RS. Community awareness activities were organised about the RS through meetings and radio discussions held by the DMHT, hospital health personnel and local authorities.
Study design, population and period
A prospective observational study using routinely collected health services data, from January 2012 to December 2017, was carried out. Three time periods were considered: pre-Ebola period (1 January 2012 to 30 May 2014); Ebola period (1 June 2014 to 28 February 2015); post-Ebola period (1 March 2015 to 31 December 2017). We considered the Ebola period from 1 month before the first confirmed case in the district (ie, June 2014) to 1 month after the country being declared Ebola-free (ie, February 2015). This was done because in Sierra Leone the outbreak had started in other districts of the country before the first case registered in Pujehun and continued to affect other districts until November 2015. It is realistic to assume that public fear of potential EVD cases and lack of confidence in the health services persisted in the Pujehun population during that time.14 In addition, expanding the Ebola period enabled a full assessment of the impact of the disease with an adequate comparison with the two long periods before and after the Ebola epidemic.
Data collection
Data on MCH indicators were prospectively collected from hospital registers (maternity ward, delivery unit, paediatric ward, operating theatre). The following variables were collected on a monthly basis: (1) paediatrics admissions; (2) paediatric deaths; (3) maternity admissions; (4) maternal deaths; (5) deliveries; (6) C-sections; (7) MDOC cases. MDOC cases were collected using a dedicated database within the hospital and confirmed by a gynaecologist. All hospital maternal deaths were reviewed by DHMT and classified according to Maternal Death Surveillance and Response policy by MoHS. Paediatric deaths did not include stillbirths and early neonatal deaths, but only deaths of children admitted to the paediatric ward.
At community level, the following variables were collected from the local district Health Management Information System: (1) family planning consultations per month; (2) deliveries per month; (3) ANC 1 per month; (4) ANC 4 per month. Different variables were collected from the two types of sites, based on the different services provided at community level (BEmOC) and at hospital level (CEmONC). Quarterly review meetings were organised with the staff in charge of the health facilities to address data discrepancies in the reports. Technical assistance was provided to the DHMT to improve timeliness, completeness and accuracy of data regarding CEmOC and BEmONC services.
For the RS, data were collected from records of all of the study sites, including delivery registers, delivery logbooks, prenatal registers, referral registers and death registers. Additional data were collected from the ambulance database and logbook. Records in the database were then validated by cross-checking the records with registers at the study sites.
Statistical analysis
For each indicator, a segmented seasonal autoregressive model of order 1 was estimated. The segments defined the three periods: before the EVD epidemic (January 2012 to May 2014), during the epidemic (June 2014 to February 2015) and after the epidemic (March 2015 to December 2017). Differences were considered statistically significant at p<0.05. The analysis was performed using R.30 The full description of the methodology of the statistical analysis is available in online supplementary annex 1.
Supplemental material
Patient and public involvement
No patients were involved in defining the research question or the outcome measures, nor were they involved in the design and implementation of the study. There are no plans to involve patients in the dissemination of the results. The full statistical analysis is available in online supplementary annex 2.
Supplemental material
Results
Hospital level: pre-Ebola period
At hospital level, for all indicators, the trend is stable during the pre-Ebola period, without significant changes (figures 2 and 3).

Maternal and paediatric admissions at hospital level.

C-sections, deliveries, MDOCs, paediatric and maternal deaths at hospital level. MDOCs, major direct obstetric complications.
Hospital level: Ebola versus pre-Ebola period
At hospital level, the differences between Ebola period versus pre-Ebola averages show a statistically significant increase for institutional deliveries (11, 95% CI 2 to 21, p=0.02) and for the reduction of maternal deaths (−1, 95% CI -2 to 0, p=0.042) (table 1). There is also a statistically significant difference between the trend of Ebola period versus pre-Ebola period, for maternal admissions (7, 95% CI 4 to 11, p<0.001), MDOCs (4, 95% CI 1 to 7, p=0.006) and institutional deliveries (4, 95% CI 2 to 6, p=0.001) (figures 2 and 3).
MCH indicators at hospital and community level
Hospital level: Ebola versus post-Ebola period
At hospital level, the differences between averages of the post Ebola versus Ebola are statistically significant for all indicators: institutional deliveries, C-sections, paediatric and maternity admissions, paediatric and maternity deaths, and MDOCs (table 1). There is also a negative trend in the transition from Ebola to post-Ebola for maternal admissions (−7, 95% CI −10 to −4, p<0.001), MDOCs (−4, 95% CI −7 to −1, p=0.009) and institutional deliveries (−3, 95% CI −5 to −1, p=0.001) (figures 2 and 3).
Hospital level: pre-Ebola versus post-Ebola period
The differences between averages of the pre-Ebola versus post-Ebola periods are also statistically significant for all indicators, except for maternal deaths (table 1). The differences between trends between pre-Ebola versus post-Ebola period are only significant for paediatric admissions (3, 95% CI 0 to 5, p=0.035) (figures 2 and 3).
Community level: pre-Ebola period
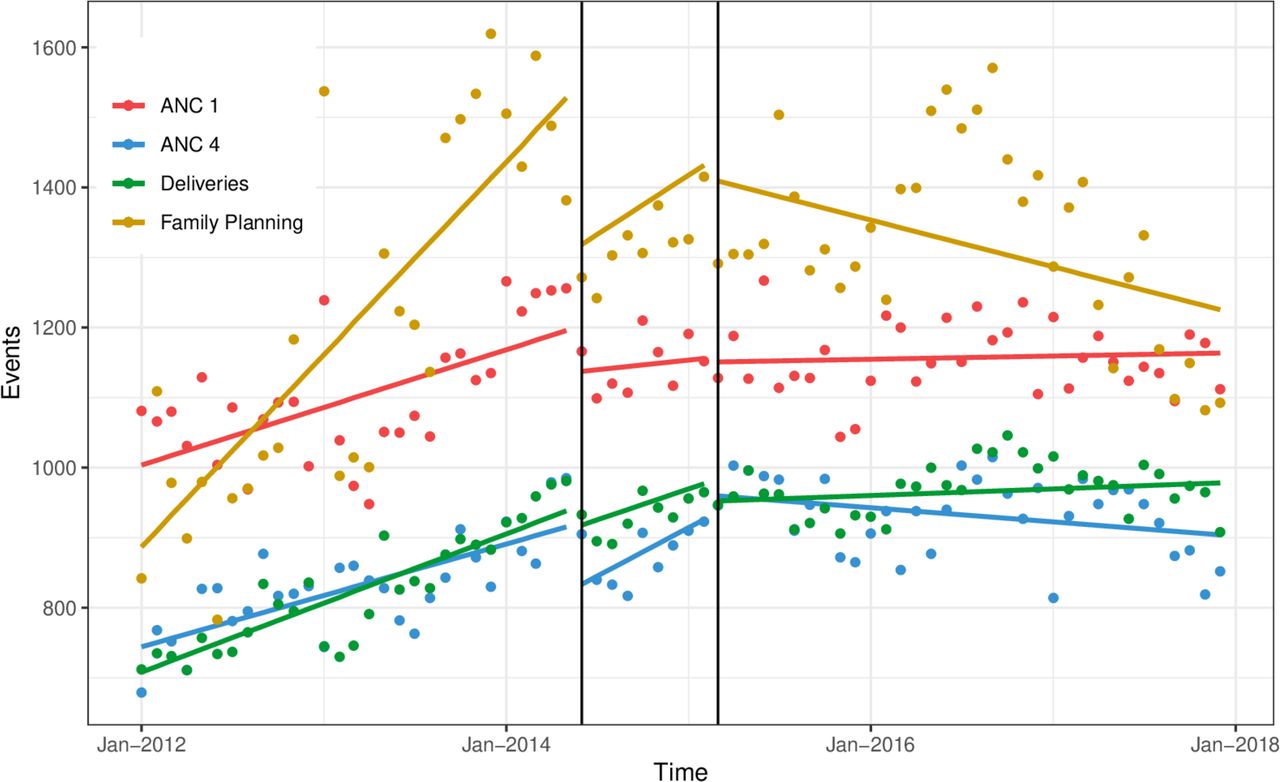
At community level, all indicators in the months before Ebola showed a positive trend. There was a monthly average increase of 8 institutional deliveries (95% CI 6 to 10, p<0.001); a monthly average increase of 7 ANC 1 (95% CI 4 to 10, p<0.001) and 6 ANC 4 (95% CI 4 to 8, p<0.001), and a monthly average increase of 69 women accessing family planning services (95% CI 42 to 95, p<0.001) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ANC 1, ANC 4, deliveries and family planning at community level. ANC, antenatal care.
Community level: Ebola versus pre-Ebola period
At community level, with the exception of family planning, the differences between averages of Ebola period versus pre-Ebola are statistically significant for all indicators: institutional deliveries (148, 95% CI 99 to 196, p<0.001), ANC 1 (74, 95 % CI 3 to 145, p=0.042) and ANC 4 (80, 95% CI 21 to 139, p=0.008) (table 1). The difference between trends (figure 3) of the Ebola versus pre-Ebola period are not significant for any of the indicators considered (figure 4).
Community level: Ebola versus post-Ebola period
At community level, the differences between averages (table 1) and the difference between trends (figure 4) of the Ebola versus post-Ebola period are not significant for any of the indicators considered.
Community level: pre-Ebola versus post-Ebola period
The differences between averages of the pre-Ebola versus post-Ebola are statistically significant, with an increase in institutional deliveries (138, 95% CI 93 to 183, p<0.001) and ANC 4 (103, 95% CI 48 to 157, p<0.001) (table 1). However, there is a negative difference between trends among the two periods, for all the variables considered: institutional deliveries (−7, 95% CI −10 to −4, p<0.001), ANC 1 (-6, 95% CI −10 to −3, p<0.001), ANC 4 (-8, 95% CI −11 to −5, p<0.001) and most significantly for family planning (−85, 95% CI −119 to −51, p<0.001) (figure 4).
RS: obstetric and paediatric results
Between January 2015 and December 2017, there were 2450 obstetric referrals. Of these, 1574 (64%) were MDOC, which represent 70% of all the 2233 MDOCs treated in the hospital over the same period. The baseline characteristics and reasons for MDOCs collected through the RS are reported on table 2. At the same time, 4671 paediatric patients were admitted in the hospital through the RS, representing 72% of the 6518 total admission during the same period. Reasons for paediatric referrals are shown on table 3.
Baseline characteristics and reasons for MDOCs collected through RS, period 2015–2017
Reasons for paediatric RS, period 2015–2017*
Discussion
This study presents for the first time trends in utilisation of MCH services before, during and after Ebola, at hospital and community level from the country most heavily affected by the Ebola epidemic. It also presents data on the restructured and reorganised RS, which started immediately after the EVD outbreak. The study shows that there was a decrease in all MCH indicators and service uptake immediately after the onset of the outbreak, with a levelling or increase during the EVD period. In the post-Ebola period, all indicators (except for maternal deaths) showed an increase, in comparison with the pre-Ebola period. This was particularly marked at hospital level because the post-Ebola reinforcement of the RS led to an increase in paediatric admissions, maternal admissions, and consequently a rise of institutional deliveries, C-sections and MDOCs. In addition, while at the hospital level trends in the post-Ebola period are in line with the pre-Ebola, at community level there is a negative trend compared with the pre-Ebola period for all indicators taken into consideration. The study presents results in contrast to other studies that showed a decline in MCH services in the Ebola and post-Ebola periods.6 31 32
Pre-Ebola and Ebola periods
As mentioned above, the approach implemented in the Pujehun district17 28 avoided vertical interventions only focused on the containment of the EVD epidemic. It worked on strengthening all the components of the health system—before, during and long after the epidemic. This approach may have contributed to reducing the spread of infection and the impact of the disease on MCH services.17 18 As shown in this paper, at community level family planning, ANC and institutional deliveries were affected only at the beginning of the Ebola outbreak with a small decrease in service utilisation. In contrast, Jones et al evaluated the number of antenatal and postnatal visits, institutional births, emergency obstetric care, maternal deaths and stillbirths across 13 districts of Sierra Leone for 10 months during, and 12 months prior to the epidemic. They found that following the onset of the epidemic there was an 18% decrease in the number of women attending ANC visits and an 11% decrease in the number of women attending for birth at healthcare facilities.14
During the Ebola epidemic, the Pujehun hospital maintained C-sections and delivery volume at pre-Ebola levels. There was a stable number of patients attending the hospital during the Ebola outbreak, as shown by the number of maternal and paediatric admissions. The study of Brolin Ribacke and colleagues focused on in-hospital deliveries and C-section volume in Sierra Leone. They showed that nationwide, although with substantial variation between districts, in-hospital deliveries and C-sections decreased by over 20% during the Ebola outbreak, mainly because of the closure of not-for-profit hospitals.6 Brolin Ribacke also noted that in general, at hospital level, in Sierra Leone those facilities that remained open performed about the same number of deliveries and C-sections after the onset of the EVD outbreak as they did before.6 This seems to indicate that the decrease observed at national level was related to the closing of key health facilities. The number of Ebola cases was not uniform throughout districts in Sierra Leone and Pujehun was one of the least affected districts. The low number of cases may also have helped to maintain public confidence in service provision and uptake of services.7 8
Post-Ebola period
There is a shortage of data in Sierra Leone and the other West Africa countries affected regarding the resumption of services after the epidemic. Pujehun district showed contrasting results at community level. Results of the post-Ebola versus pre-Ebola show an increase of activities for institutional delivery and ANC 4. However, there is a negative trend among the two periods, for the variables taken into consideration, namely institutional deliveries (−7, 95% CI −10 to −4, p<0.001), ANC 1 (−6, 95% CI −10 to −3, p<0.001), ANC 4 (−8, 95% CI −11 to −5, p<0.001) and family planning (−85, 95% CI −119 to −51, p<0.001). In 2017, the Pujehun district showed a coverage of 98% for ANC 1 (98% in 2013), 91% for ANC 4 (76% at national level in 2013) and 90% for institutional deliveries (62% in 2013).33 34 The initial intervention carried out by DwA in the period 2012–2014 at the community level probably increased these percentages, with an initial growth of the trend that had been slowing down in the years 2016–2017. Possible explanations for this may include bypassing, that is, using alternative healthcare instead of free or subsidised public clinics; increased opportunities to get transport to seek healthcare in neighbouring districts; reduced demand for MCH services at community level; and reduced quality of MCH services at PHUs.
A study by Camara et al in a rural district of Guinea showed a considerable recovery gap in the post-Ebola period for ANC (37%) and institutional deliveries (34%).31 Also, Delamou et al noted a significant reduction in the average number of ANC visits and institutional deliveries during the Ebola outbreak, in six districts of Guinea, and the overall post-outbreak trends did not suggest recovery.32 By contrast, Wagenaar et al, which analysed 10 primary care indicators in Liberia, before, during and after the Ebola outbreak, showed significant positive trends during the post-EVD period for ANC and institutional deliveries.35
There are multifactorial and complex reasons for the decline of family planning in the Pujehun district. The activities that MoHS and DwA implemented from 2012 onwards were maintained during and after the EVD epidemic. However, a general decrease in the availability of healthcare personnel and international aid was observed and this could be a factor in the family planning decline. A possible stock-out of family planning methods has also been suggested as a reason for the decrease.25 In addition, a reduction in demand for family planning in the post-Ebola period could account for the decline of the service. Experiencing a disaster can trigger the desire to ‘rebuild’ communities, reducing the need for family planning methods,36 or communities may prefer traditional methods of contraception.37 However, the reduction in family planning use in Pujehun district did not translate into an increase in institutional deliveries as occurred in neighbouring Liberia.38 Although no further transmissions of Ebola took place in the Pujehun district after November 2015, the awareness of the ongoing transmission elsewhere in Sierra Leone, in Guinea and Liberia might have influenced health seeking behaviours.39 40 However, this does not seem to have influenced other types of MCH services at community level. For comparison, the above mentioned study of Camara et al showed that the utilisation of family planning declined by 51% during the Ebola outbreak but recovered in the post-Ebola period.31
At hospital level, the situation is different. In the post-Ebola period, there was a significant increase in the volumes of activities: paediatric and maternal admissions, MDOC cases, deliveries and C-sections. This increase can be directly linked to the reorganisation and strengthening of the RS immediately after the Ebola epidemic. Based on the three delays theory,41 in Pujehun it was decided to tackle the second delay, a lack of accessibility to health services. The distance to the hospital as well as lack of accessible and affordable vehicles were recognised as significant barriers when attempting to access CEmONC services at the hospital.42 43 The success of the RS service can be linked to the integration of the key components needed for a successful service, namely: (1) a transport system which took account of the specific geographical characteristics of the district42; (2) an effective communication system with a call centre in contact with all PHUs of the district, the ambulance drivers and the hospital; (3) training of all the PHU staff on the recognition of obstetric emergencies and on the RS.44 45 Several meetings were planned with local community leaders and religious leaders to raise awareness of the importance of giving birth in health facilities. Prohibitive costs have been shown to be a major factor in preventing women accessing health facilities during childbirth in Sierra Leone.42 46 47 Meetings were also organised to inform the population that the service was free of charge, and to give reassurance that the ambulances carried no risk of Ebola infection to people using them. The increase in complicated cases treated at the hospital did not translate into an increase in maternal and paediatric deaths, reflecting positively on the quality of care provided. The maternity ward death rate remained around 1% throughout the 2012–2017 study period. The differences in average death rates during the period 2015–2017 among referred and not referred paediatric patients were 10.5% and 4.3%, respectively. This showed that the paediatric RS works for the most critical cases able to reach the hospital in time.
Conclusions
There are a number of contextual factors and limitations that should be taken into account in the analysis of the results of this study. The data refer to a single area of Sierra Leone and therefore our sample cannot be considered representative of the country as a whole. We defined our distinct period of EVD outbreak arbitrarily, from 1 month before the first case in the district to 3 months after the last case in the district. This was done because the EVD crisis affected areas of the country outside Pujehun prior to and after outbreak within Pujehun. The official end of the EVD epidemic for Sierra Leone was declared on 17 March 2016, and for the countries of Guinea and Liberia was declared on 1 June 2016. All the results should be taken with some degree of statistical caution, because no correction was performed to take into account the multiplicity of the tests carried out. Finally, our study assumed that no other interventions in addition to those described occurred concurrently with the Ebola epidemic.18 Similarly, we assumed that no other substantial interventions in addition to the reorganisation of the RS happened in the post-Ebola period which would have affected the service trends that we observed. The Pujehun district had 49 confirmed EVD cases. This number is much lower than in other districts. If it is true that the fear of Ebola may have prevented people from accessing health services, the small number of EVD cases in the community may have also raised confidence, leading to the increase of utilisation rates after the initial drop. The strength of this study is that it uses data from a remote rural district in Sierra Leone, with a 6-year observational period. The pre, intra and post-Ebola periods data allowed a comparison between trends. DwA was working in this community before the outbreak began, which gave an advantage of knowledge of the setting when the epidemic began, which in turn facilitated mitigating measures to be put in place. In addition, this allowed a collection of data in a prospective way, reducing the potential bias in the accuracy of the data reported by other studies.6 14 32 35
Failures in providing effective healthcare are associated with a chiefly vertical focus on outbreak control.19–21 The approach implemented in the Pujehun district worked on strengthening all the components of the health system—governance, human resources, community involvement—before, during and after the epidemic.
The strengthening of the health system in the district, compared with other districts, allowed the containment of the epidemic and, above all, to maintain and strengthen MCH services as shown by the data reported in the paper. Health facilities in the district, both at community and hospital level, were able to maintain their services during the epidemic, overcoming public fear of Ebola and lack of confidence in service providers, which led to the public staying away from facilities in other districts in Sierra Leone.14 In postcrisis situations, ‘windows of opportunity’ are opened for redirecting the policies of the national health systems, renovating specific sectors (eg, human resources, epidemiological surveillance systems, financing and so on) and renewing services/practices at the operational level.48 In Pujehun, the implementation of an RS immediately after the acute Ebola phase might have reduced delays in patients accessing care and enabled a significant improvement in all MCH indicators at hospital level. Other studies have also found that using this window of opportunity to introduce systems such as performance-based financing can also produce positive outcomes.49 As Sierra Leone continues its recovery, there is a need to quantify the impact of the outbreak on MCH care to guide long-term strategies for MHC services. This study provides evidence on strategies to increase the resilience of fragile healthcare services and the importance of NGOs and government collaboration to bring about change.
Acknowledgments
We are deeply grateful to all the staff of Pujehun district hospital and Peripheral Health Units, District Health Management and the personnel of Doctors with Africa CUAMM who worked in Pujehun during the epidemic. We thank James Dean for his help with proofreading.
References
Footnotes
Contributors GQ, FT and GP contributed to study design, literature review, data analysis, data interpretation, writing and review of the final manuscript. LF, FDG, DP and CM performed data analysis, data interpretation and drafting of the manuscript. DB, SS, AK, ZB and VP contributed to data collection and data interpretation. BSC, AS, WM and SJ contributed to data interpretation and review of the final manuscript. All coauthors contributed to the improvement of the article.
Funding This work was undertaken and funded by Doctors with Africa CUAMM.
Disclaimer The views expressed in this publication are the sole responsibility of the authors and do not necessarily reflect the views of the affiliated organisations.
Competing interests None declared.
Ethics approval Sierra Leone Ethics and Scientific Review Committee, Directorate of Policy, Planning and Information, Ministry of Health and Sanitation, Sierra Leone.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data underlying the findings described in the manuscript are fully available without restriction.
Patient consent for publication Not required.
Map disclaimer The depiction ofboundaries on the map(s) in this article do not imply the expression of anyopinion whatsoever on the part of BMJ (or any member of its group) concerningthe legal status of any country, territory, jurisdiction or area or of itsauthorities. The map(s) are provided without any warranty of any kind, eitherexpress or implied.