Article Text

Abstract
Background and objective About 9% of gastric carcinomas have Epstein–Barr virus (EBV) in the tumour cells, but it is unclear whether viral presence influences clinical progression. We therefore examined a large multicentre case series for the association of tumour EBV status with survival after gastric cancer diagnosis, accounting for surgical stage and other prognostic factors.
Methods We combined individual-level data on 4599 gastric cancer patients diagnosed between 1976 and 2010 from 13 studies in Asia (n=8), Europe (n=3), and Latin America (n=2). EBV positivity of tumours was assessed by in situ hybridisation. Mortality HRs for EBV positivity were estimated by Cox regression models stratified by study, adjusted for distributions of sex (71% male), age (mean 58 years), stage (52% tumour-node-metastasis stages III or IV), tumour histology (49% poorly differentiated, 57% Lauren intestinal-type), anatomic subsite (70% non-cardia) and year of diagnosis. Variations by study and continent were assessed using study-specific HRs for EBV positivity.
Results During median 3.0 years follow-up, 49% of patients died. Stage was strongly predictive of mortality, with unadjusted HRs (vs stage I) of 3.1 for stage II, 8.1 for stage III and 13.2 for stage IV. Tumour EBV positivity was 8.2% overall and inversely associated with stage (adjusted OR: 0.79 per unit change). Adjusted for stage and other confounders, EBV positivity was associated with lower mortality (HR, 0.72; 95% CI 0.61 to 0.86), with low heterogeneity among the study populations (p=0.2). The association did not significantly vary across patient or tumour characteristics. There was no significant variation among the three continent-specific HRs (p=0.4).
Conclusions Our findings suggest that tumour EBV positivity is an additional prognostic indicator in gastric cancer. Further studies are warranted to identify the mechanisms underlying this protective association.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
While chronic Helicobacter pylori infection is the primary cause of gastric cancer, a subset of cases also contain Epstein–Barr virus (EBV) DNA.
-
The viral genome in EBV-positive cases is monoclonal and present in all tumour cells, suggesting the virus may be a cofactor in gastric carcinogenesis.
-
Patients with EBV-positive gastric tumours have distinct demographic, clinical and pathological features compared to those with EBV-negative tumours.
What are the new findings?
-
EBV-positive gastric cancer tends to have lower tumour–node–metastasis (TNM) stage.
-
Even adjusted for TNM stage as well as other prognostic indicators, tumour EBV positivity confers a relative survival advantage.
How might it impact on clinical practice in the foreseeable future?
-
The difference in prognosis by tumour EBV status provides additional evidence that EBV-positive gastric cancer is a distinct disease entity.
-
EBV-positive gastric cancer may warrant different preventive and/or therapeutic modalities.
-
The mechanisms conferring better survival of EBV-positive tumours may lead to novel approaches to manage gastric cancer in general.
Introduction
Gastric cancer is the second leading cause of cancer-related deaths worldwide.1 Although chronic Helicobacter pylori infection is the primary cause of gastric cancer,2 most infected individuals never develop this neoplasia, suggesting that progression to cancer may require additional co-factors. One possibility may be the Epstein–Barr virus (EBV), a recognised carcinogenic agent,3 which is present in tumour cells of about 9% of gastric carcinomas.4 ,5 While the monoclonality6 of viral episomes and the distinct clinicopathological and genetic features7 of EBV-positive gastric cancer support the aetiological significance of EBV in gastric carcinogenesis, it remains unclear whether tumour viral infection influences clinical prognosis.
To further examine associations between EBV and gastric cancer with sufficient statistical power, we have assembled individual-level data from multiple international gastric cancer case series for aggregated analysis. Here we present findings for the association of tumour EBV status with duration of overall survival, accounting for surgical stage and other recognised prognostic indicators.
Methods
Patient data
We pooled individual-level data of 13 gastric cancer case series from Asia (n=8),8–15 Europe (n=3)16–18 and Latin America (n=2),19 ,20 including six that have separately published data on EBV and survival in one9–11 ,13 ,17 or two14 ,21 reports. Ten were unselected case series and three10 ,13 ,17 were enriched for EBV-positive tumours. On a total of 4599 patients diagnosed between 1976 and 2010, we included variables that may be related to both tumour EBV status and survival after diagnosis: sex, age at diagnosis, tumour–node–metastasis (TNM) stage (American Joint Committee on Cancer classification, AJCC), histological type (Lauren classification), degree of differentiation, anatomic subsite (according to the International Classification of Diseases for Oncology) and year of diagnosis. Each contributing study received local institutional review board approval, and written informed consent was obtained for all study participants.
Tumour EBV detection
For all 13 case series, the presence of EBV in cancer cells was assessed by in situ hybridisation for EBV-encoded RNA (EBER), the gold standard assay for detecting latent infection.22 For the samples from Shanxi, China (n=1039),8 Poland (n=87),18 and the European Prospective Investigation into Cancer and Nutrition cohort (EPIC) (n=87),16 EBER expression in formalin-fixed paraffin-embedded tumours (as tissue microarrays, with inclusion of known EBER-positive and -negative tumours as controls) was detected with an automated method, as previously described.23 A tumour was considered EBV-negative if EBER staining was undetected or only expressed in benign-appearing lymphoid cells, and EBV-positive if EBER staining was localised to the nucleus of malignant epithelial cells.
For the samples from the Hospital-based Epidemiologic Research Program at Aichi Cancer Center II, Japan (n=371),12 EBER detection was performed manually on formalin-fixed paraffin-embedded sections, using a complementary fluorescein-labelled oligonucleotide probe (Dako, Copenhagen, Denmark), according to the manufacturer's specifications. For the remaining case series,9–11 13–15 ,17 ,19 ,20 EBV presence in tumour cells was previously assessed following similar protocols. Validation work has been published showing excellent agreement between the manual and automated staining methods described above.23
Statistical analyses
For this aggregated analysis, the endpoint of interest was survival time between gastric cancer diagnosis and death from any cause. Follow-up time was censored on the date of death or, if death did not occur, on date last known alive. Actuarial (unadjusted) curves were constructed using the Kaplan–Meier method and their difference was evaluated by a log-rank test.
Complete data were available on age, sex and year of diagnosis. In the main analysis, missing values were included as a separate category for TNM stage (6.6%), anatomic subsite (9.3%), Lauren histological type (4.9%) and degree of differentiation (6.8%). In a sensitivity analysis, we excluded such cases for comparison to the overall dataset.
Unadjusted and multivariable logistic regression models including a study-specific random intercept were used to estimate summary OR of gastric cancer EBV positivity in relation to age at diagnosis (categorised as quintiles), sex (male vs female), year of diagnosis (categorised as quintiles), anatomic subsite (cardia, non-cardia, overlapping subsites, unspecified or surgical stump), TNM stage (I, II, III, IV or unspecified), degree of differentiation (well, moderate, poor or unspecified) and Lauren histological type (diffuse, intestinal, mixed or unspecified). To further understand the potential association of EBV positivity and stage, the three individual components of the TNM staging system (ie, tumour, lymph nodes and presence of metastases) were also evaluated.
Cox proportional hazard regression models stratified by study were used to estimate mortality HRs with 95% CIs. Tumour EBV status and other variables were initially assessed for associations with mortality in unadjusted models. Statistically significant variables in these individual analyses were included in multivariable models. Given the high correlation between histological type and degree of differentiation, separate regression models including either variable were compared using the Akaike Information Criterion (AIC) to identify the best model as having the lowest AIC value. Wald χ2 tests were used to assess statistical significance of cross-product terms for interactions between tumour EBV status and other independent variables. To further investigate heterogeneity by TNM stage, a stratified analysis was performed and the stratum-specific estimates pooled using random-effects meta-analysis. Between-group heterogeneity was assessed for statistical significance using the Q test and quantified with the I2 statistic as low (<25%), moderate (25–50%) or high (>50%).24
As a sensitivity analysis, we compared our aggregated analysis to a two-step approach.25 First, study-specific HRs and 95% CIs of the association between tumour EBV status and mortality were estimated using multivariable Cox regression models. Second, the 13 study-specific adjusted HRs for tumour EBV positivity were pooled using random-effects meta-analysis. Heterogeneity by continent (Asia, Europe or America) was evaluated by meta-regression.
A p value <0.05 was considered statistically significant for all tests except the Q test, for which p<0.10 was considered significant. All reported p values were two-sided. Statistical analyses were performed using SAS V.9.1 and Stata V.10.
Results
Among the 13 case series, there were a total of 4599 patients with invasive gastric cancer (table 1). The mean age at diagnosis was 58 years (SD 12 years) and 71% were male. Most of the cancers were diagnosed at advanced stages (52% stages III or IV), localised to non-cardia subsites (70%), and classified as Lauren intestinal-type (57%). There were 2247 (49%) deaths during a median of 3.0 (25th percentile, 1.1; 75th percentile, 5.5) years of follow-up.
Selected characteristics of the study populations
Three hundred and seventy-five (8.2%) tumours were EBV-positive overall. In unadjusted logistic regression analyses, tumour EBV positivity was higher in early stage, cardia localisation, diffuse-type histology, poorer differentiation and men (figure 1). In a multivariable model including all significant variables, the OR per unit change in TNM stage was 0.79 (95% CI 0.69 to 0.91). Considered individually in multivariable models, each of the components of TNM stage was inversely associated with tumour EBV positivity (p=0.001 for tumour, p=0.02 for lymph nodes and p=0.004 for presence of metastasis). Furthermore, both tumour and metastasis, but not lymph nodes, remained significant in a mutually adjusted model.

ORs and 95% CIs for the associations of selected clinical and demographic characteristics with gastric tumour Epstein–Barr virus positivity.
In unadjusted Cox regression analyses, TNM stage was a strong predictor of mortality, with HRs (compared to stage I) of 3.1 for stage II, 8.1 for stage III and 13.2 for stage IV. Age, anatomic subsite, histological type and degree of differentiation were each significant prognostic indicators, whereas sex and year of diagnosis were not. Median survival time was 8.5 years for patients with EBV-positive tumours and 5.3 years for those with EBV-negative tumours (log-rank test p=0.0006; figure 2).
In a multivariable model fitted for tumour EBV status, TNM stage, age, anatomic subsite and degree of differentiation, all variables were statistically significant predictors of mortality (figure 3). Specifically, advanced stage, older age and less differentiation were associated with worse prognosis. Compared to tumours localised to the cardia, tumours arising in non-cardia sites were associated with lower mortality, whereas tumours of overlapping subsites or post-gastrectomy remnants were associated with increased mortality. Adjusted for stage and the other potential confounders, EBV positivity was associated with lower mortality (HR 0.72; 95% CI 0.61 to 0.86). With the exclusion of the 915 (20%) cases that had missing data for one or more variables, the HR for EBV status was 0.71 (95% CI 0.59 to 0.88). Furthermore, there were no significant multiplicative interactions between tumour EBV status and other independent variables (data not shown).
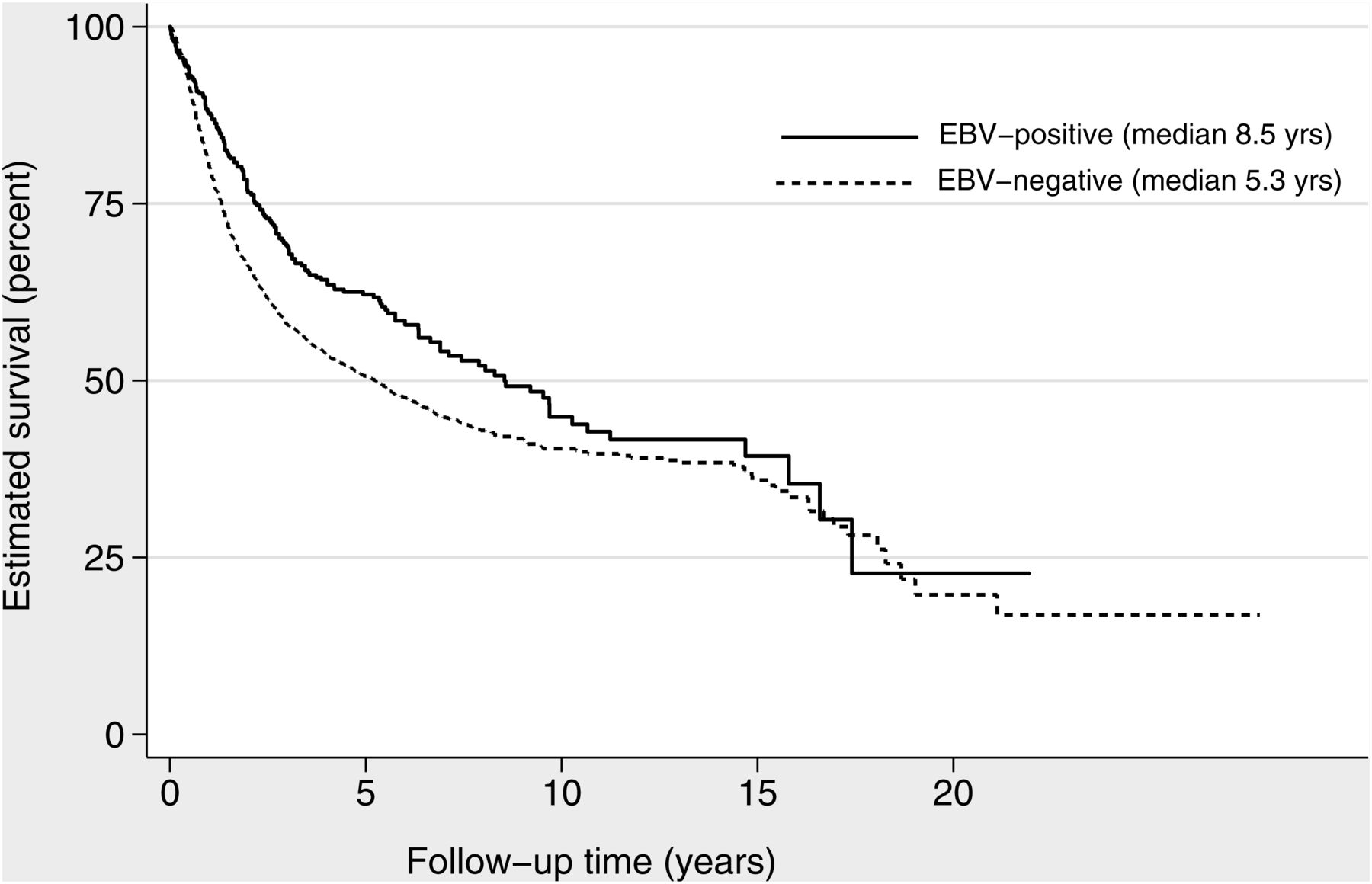
Kaplan–Meier estimated survival after gastric cancer diagnosis by tumour Epstein–Barr virus (EBV) status.
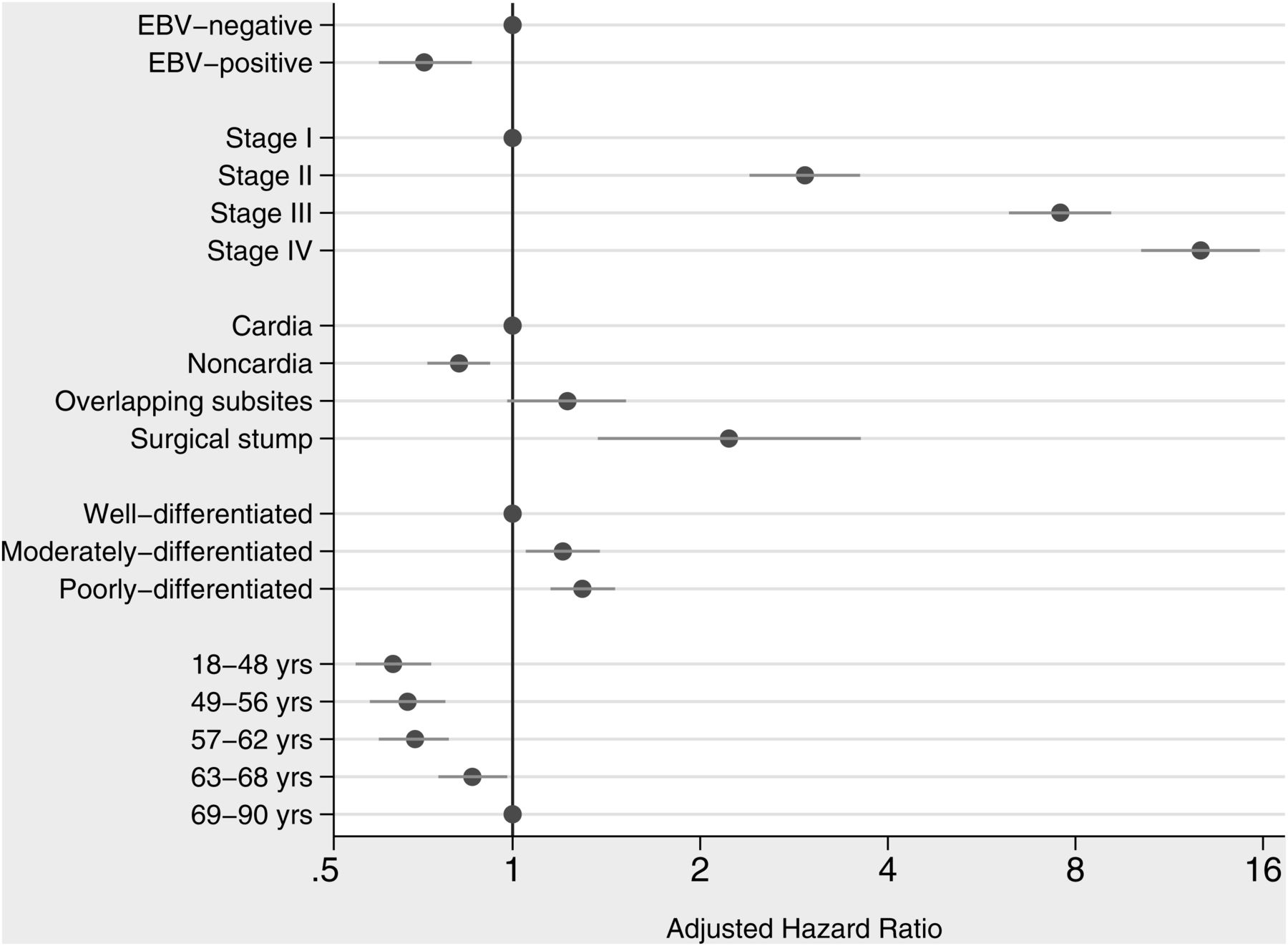
HRs and 95% CIs for associations of tumour Epstein–Barr virus (EBV) status and other selected characteristics with overall mortality after gastric cancer diagnosis.
In an alternative model including histological type instead of degree of differentiation, HRs for tumour EBV status, stage, age and anatomic subsite were generally similar. Compared to patients with tumours classified as diffuse-type histology, those with mixed or unspecified histology had similar mortality, whereas patients with intestinal-type histology had a better prognosis (HR 0.81; 95% CI 0.74 to 0.89). In this alternative model, the adjusted HR for tumour EBV positivity was 0.74 (95% CI 0.62 to 0.88), but the AIC indicated that the fit was slightly inferior to the model including degree of differentiation.
Results from the two-step analyses were similar to the estimates derived from the aggregated analysis. The summary HR for tumour EBV positivity combining the 13 study-specific HRs was 0.71 (95% CI 0.56 to 0.91), with low heterogeneity among studies (I2=21%; p=0.2). Furthermore, there was no significant variation by continent (figure 4), with HRs for tumour EBV positivity of 0.73 for Asia, 0.48 for Europe and 0.92 for the Americas (p=0.4). Likewise, the summary HR for tumour EBV positivity combining the five stage-specific HRs (ie, including unspecified stage) was 0.68 (95% CI 0.54 to 0.87), with only moderate heterogeneity among the stages (I2=33%; p=0.2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of HRs for the association of gastric cancer mortality with tumour Epstein–Barr virus (EBV) positivity for the study populations, by continent. Study-specific HRs are shown as squares, with the size of the symbol inversely proportional to the study specific variance. Summary random-effects HRs are shown as diamonds, with the middle corresponding to the point estimate and the width representing the 95% CIs.
Discussion
In both aggregated and two-step adjusted analyses of 4599 gastric cancer cases, we found longer survival associated with tumour EBV positivity. Our study represents by far the largest cancer series addressing this association, and there was no substantial heterogeneity among the study populations. Our finding for EBV-positive tumours accords with the recognised survival advantage of lymphoepithelioma-like carcinoma (LELC),26 a rare histology subtype of gastric cancer that is typically EBV-associated.4 ,27 Previous studies of EBV's prognostic significance in more common histologies of gastric cancer are limited by small numbers of EBV-positive tumours and/or inadequate accounting for key prognostic indicators; findings have been inconsistent, with some reporting a non-significant survival advantage for EBV-positive tumours,13 ,17 ,21 ,28–31 while others report a non-significant greater risk of death.10 ,11 ,32
Our results are analogous to another virus-associated malignancy, human papillomavirus (HPV)-associated oropharyngeal cancer. HPV is found in a subset of lingual and palatine tonsil tumours and is associated with distinct clinical and biological characteristics, including favourable prognosis.33 Although Herpesviridae and Papillomaviridae are highly disparate virus families, common aspects of virus–host interaction may contribute to survival advantage.
The mechanisms underlying better survival of EBV-positive gastric cancers are uncertain. A potential immunological basis is the extensive infiltration of tumour nests with cytotoxic CD8 lymphocytes that may promote eradication of EBV-positive malignant cells.34–36 An alternative hypothesis is that genetic alterations potentially associated with better survival (eg, mutated ARID1A) may be more common in EBV-positive tumours.37 It is also possible that EBV-positive tumours may be more sensitive to chemotherapy-induced apoptosis, as reported in gastric LELC38 and EBV-associated Hodgkin lymphoma.39 Additional studies are warranted to test these various hypotheses and identify the determinants.
In our data, adjusted for other clinicopathological characteristics, there were inverse associations of tumour EBV positivity with TNM stage as well as its individual components. A meta-analysis by Lee et al5 found summary ORs of 0.75 (p=0.3) for TNM stage and 0.85 (p=0.3) for lymph node spread. On the contrary, a meta-analysis by Li et al40 found a significant OR of 0.51 (p<0.05) for lymph node spread. Since stage is also associated with mortality, we decided to analyse this composite variable as a confounder. However, this approach may have underestimated the effect of EBV if the survival advantage is in fact mediated by lymph node spread and/or extent of the primary tumour.
Our data are consistent with previous reports that advanced TNM stage, older age, cardia tumour localisation, and less differentiated histology are adverse prognostic indicators.41–43 Notably, several of our Asian case series were collected as part of screening programmes, which may explain the relatively longer survival as compared to population-based data.44 Nevertheless, this study characteristic would not bias evaluation of the association with tumour EBV status.
With respect to possible study limitations, although all 13 contributing series used AJCC classification, assessment of tumour, node and/or metastasis characteristics may not have been uniform. Furthermore, although overall mortality is considered a more robust outcome, cause-specific mortality would have been additionally informative for a secondary analysis. Lastly, our study also lacked information on treatment and co-morbidity history.
EBV has been detected in a number of lymphoproliferative disorders and carcinomas.45 Regarding lymphoproliferative disorders, population-based studies and case series provide inconsistent results of EBV's prognostic significance in Hodgkin lymphoma.46 However, Minnicelli et al47 reported a significant survival advantage of tumour EBV positivity and Levine et al48 reported higher survival with elevated antibody titres to the viral capsid antigen (VCA) in sporadic Burkitt lymphoma. Perhaps more relevant to gastric cancer, EBV-positive nasopharyngeal carcinoma has been found to have better prognosis as compared with EBV-negative cases,49 ,50 in part because of better response to therapy.
Our findings on clinical prognosis provide additional evidence that EBV-positive gastric cancer may be a distinct disease entity. Several lines of evidence suggest an aetiological role for EBV in gastric carcinogenesis. EBV-positive gastric cancer exhibits uniform presence of monoclonal viral episomes in the tumour cells,6 implying the presence of EBV at the time of initial transformation and its requirement for maintenance of the transformed phenotype. EBV-positive gastric cancer also displays distinct clinical, genetic and demographic features as compared to EBV-negative cancer.7 ,29 ,51–53 Interestingly, Tang et al54 found that compared to uninfected tumours, EBV-positive gastric cancer had significant upregulation of key cellular factors in pathways related to NFKB signalling and immune response. Although seropositivity against EBV infection is nearly ubiquitous in humans, elevated titres against VCA and EBV nuclear antigen (EBNA) have been shown to precede development of preneoplastic55 and neoplastic gastric lesions,56 ,57 and have been associated with longer gastric cancer survival, particularly for cancers localised to the gastric cardia.58
In summary, this large analysis found that patients with EBV-positive gastric tumours have a significantly better outcome than those with EBV-negative tumours. Future studies should elucidate possible mechanisms underlying this protective association.
Acknowledgments
Previously presented in part at Digestive Disease Week 2012, 19–22 May 2012, San Diego, California. We thank Dr Gwen Murphy for her assistance in organising the National Cancer Institute International EBV-Gastric Cancer Consortium. We are also grateful to Dr Ti Ding and other staff of the Shanxi Cancer Hospital for recruitment and follow-up of the study participants from Shanxi, China.
References
Footnotes
-
Contributors Study concept and design: MCC, CK, SA, CSR. Acquisition of data: W-HK, AMC, K-MK, AHC, KM, JY, JJYS, RH-G, FM-G, YK, SN, LML, JL, SK, NH, CAG, YY, CK, SMH, SA, MLG, PRT. Analysis and interpretation of data, and drafting of the manuscript: MCC, CSR. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: MCC. Obtained funding: CSR. Study supervision: CSR.
-
Funding This work was supported in part by the Intramural Research Program of the USA National Institutes of Health, National Cancer Institute, and the Oak Ridge Associated Universities’ Research Associates/Specialists Program. The Hospital-based Epidemiologic Research Program at Aichi Cancer Center II was supported by Grant-in-Aid for Scientific Research on Priority Areas of Cancer (No. 17015018) and on Innovative Areas (No. 221S0001) from the Japanese Ministry of Education, Culture, Sports, Science and Technology and JSPS A3 Foresight Program. The EPIC study was supported by the Health Research Fund of the Spanish Ministry of Health (exp.PI070130 and PI081420); European Commission FP5 (ref. QLG1-CT-2001-01049); and Spanish Ministry of Health network RTICCC (ISCIII RD06/0020/0091). The Chilean study was supported by the Chilean National Fund for Scientific and Technological Development, Fondecyt (No. 1111014). The Chinese study in Guangzhou was supported by the Research Fund for the Control of Infectious Diseases, RFCID, Hong Kong (No. 11100022).
-
Competing interests None.
-
Ethics approval Each contributing study received local institutional review board approval.
-
Provenance and peer review Not commissioned; externally peer reviewed.