Article Text

Abstract
Objectives In non-alcoholic fatty liver disease (NAFLD), hepatic steatosis is intricately linked with a number of metabolic alterations. We studied substrate utilisation in NAFLD during basal, insulin-stimulated and exercise conditions, and correlated these outcomes with disease severity.
Methods 20 patients with NAFLD (mean±SD body mass index (BMI) 34.1±6.7 kg/m2) and 15 healthy controls (BMI 23.4±2.7 kg/m2) were assessed. Respiratory quotient (RQ), whole-body fat (Fatox) and carbohydrate (CHOox) oxidation rates were determined by indirect calorimetry in three conditions: basal (resting and fasted), insulin-stimulated (hyperinsulinaemic–euglycaemic clamp) and exercise (cycling at an intensity to elicit maximal Fatox). Severity of disease and steatosis were determined by liver histology, hepatic Fatox from plasma β-hydroxybutyrate concentrations, aerobic fitness expressed as  , and visceral adipose tissue (VAT) measured by computed tomography.
, and visceral adipose tissue (VAT) measured by computed tomography.
Results Within the overweight/obese NAFLD cohort, basal RQ correlated positively with steatosis (r=0.57, p=0.01) and was higher (indicating smaller contribution of Fatox to energy expenditure) in patients with NAFLD activity score (NAS) ≥5 vs <5 (p=0.008). Both results were independent of VAT, % body fat and BMI. Compared with the lean control group, patients with NAFLD had lower basal whole-body Fatox (1.2±0.3 vs 1.5±0.4 mg/kgFFM/min, p=0.024) and lower basal hepatic Fatox (ie, β-hydroxybutyrate, p=0.004). During exercise, they achieved lower maximal Fatox (2.5±1.4 vs. 5.8±3.7 mg/kgFFM/min, p=0.002) and lower  (p<0.001) than controls. Fatox during exercise was not associated with disease severity (p=0.79).
(p<0.001) than controls. Fatox during exercise was not associated with disease severity (p=0.79).
Conclusions Overweight/obese patients with NAFLD had reduced hepatic Fatox and reduced whole-body Fatox under basal and exercise conditions. There was an inverse relationship between ability to oxidise fat in basal conditions and histological features of NAFLD including severity of steatosis and NAS.
- Fatty Liver
- Lipid Metabolism
- Lipid Oxidation
- Glucose Metabolism
- Chronic Liver Disease
Statistics from Altmetric.com
Significance of this study
What is already known on this topic
-
Non-alcoholic fatty liver disease (NAFLD) is the most prevalent liver disease in industrialised countries and is associated with a number of metabolic alterations.
-
In NAFLD, studies investigating whole-body and hepatic fat oxidation have reported conflicting results. Further, it is not known whether the severity of NAFLD is associated with whole-body substrate oxidation rates.
-
Maximal fat oxidation achieved during exercise has not been studied in NAFLD.
What this study adds
-
Whole-body fat oxidation at rest and during exercise is reduced in overweight/obese patients with NAFLD.
-
In overweight/obese patients with NAFLD, reduced whole-body fat oxidation in basal conditions is associated with degree of steatosis and histological severity of disease, independently of BMI, body fatness and visceral adipose tissue.
-
Basal hepatic fat oxidation is reduced in overweight/obese patients with NAFLD.
How might it impact on clinical practice in the foreseeable future?
-
Behavioural or pharmacological therapies that can promote whole-body and hepatic fat oxidation in basal and exercise conditions may be useful for the treatment of NAFLD.
-
Exercise training may be a suitable treatment option for NAFLD because, in addition to improving aerobic fitness and insulin sensitivity, it also promotes fat oxidation in basal and exercise conditions.
Introduction
The most prevalent liver disease in industrialised countries is non-alcoholic fatty liver disease (NAFLD).1 NAFLD encompasses a spectrum of histological features ranging from simple steatosis to non-alcoholic steatohepatitis (NASH), fibrosis and cirrhosis. Development and progression of NAFLD are intricately linked with a number of factors including genetic predisposition,2 ,3 physical inactivity, obesity and insulin resistance (IR).4 ,5 Hepatic steatosis appears to be a prerequisite for more severe liver injury and occurs when the rates of de novo hepatic fatty acid synthesis and hepatic fatty acid uptake from plasma exceed the rate of hepatic fat oxidation and triglyceride (TG) export.6 There is evidence that patients with NAFLD have increased free fatty acid (FFA) delivery from the adipose tissue,7 increased de novo hepatic fatty acid synthesis8 and increased TG export.9 On the other hand, it is less clear whether patients with NAFLD have altered whole-body and hepatic fat oxidation (Fatox).
An ideal framework for studying whole-body substrate metabolism is to assess substrate oxidation rates under a number of physiological conditions including the basal state (resting and fasting conditions), after a meal or insulin stimulation, and during exercise.10 Studies investigating whole-body substrate oxidation of patients with NAFLD in the basal state have reported conflicting results. Perseghin et al 11 found lower rates of whole-body Fatox in obese adolescents with NAFLD compared with counterparts without fatty liver. In contrast, Bugianesi et al 12 reported a tendency for higher rates of whole-body Fatox in 12 non-obese patients with NAFLD when compared with six body mass index (BMI)-matched controls. Similarly, Sanyal et al 13 found higher Fatox in six obese NAFLD than six obese NASH patients, although neither group differed from six lean controls. Kotronen et al 14 found no significant difference between 29 moderately overweight individuals with NAFLD and 29 leaner healthy controls. In the latter group of studies,12–14 between-group differences in hepatic Fatox mirrored those for whole-body Fatox. In the insulin-stimulated state, results were more uniform, with patients with NAFLD showing reduced insulin-mediated suppression of Fatox compared with controls.11 ,12 ,14 To date, substrate oxidation during exercise has not been compared between patients with NAFLD and counterparts without fatty liver. It is important to better understand substrate metabolism during exercise because whole-body metabolic demands are increased and potential abnormalities not seen in the resting state may become apparent. Further, exercise training is increasingly recommended clinically as a component of lifestyle interventions.15 ,16
Differences in severity of liver disease in previous cohorts may have contributed to the contrasting results reported on basal substrate metabolism in NAFLD. However, the relationship between severity of disease (which can only be assessed by liver histology) and substrate oxidation under various metabolic conditions has not been investigated to date in adults with NAFLD. In obese adolescents with NAFLD, hepatic steatosis (measured by magnetic resonance spectroscopy) and impairment in basal whole-body Fatox were shown to be positively correlated, independently of BMI.11
The objective of this study was to measure substrate utilisation under basal, insulin-stimulated and exercise conditions in adult patients with NAFLD and to explore whether these outcome measures correlated with degree of steatosis and severity of liver disease.
Methods
Participants
Twenty overweight/obese patients with NAFLD and 15 lean healthy controls participated in the study. Patients were recruited from outpatient hospital clinics, and NAFLD was diagnosed clinically and on liver biopsy. Exclusion criteria included the presence of other causes of liver disease (serologically and on history), evidence of cirrhosis or decompensated liver disease, alcohol consumption >40 g/day in men or >20 g/day in women (assessed by detailed clinical history) and type 2 diabetes. Control participants were healthy non-obese adults with normal liver enzymes (alanine transaminase <35 U/l; aspartate transaminase <35 U/l), no evidence of liver disease (serologically and on history), no hepatomegaly on clinical examination, and no features of the metabolic syndrome.17 Controls were non-smoking, not taking regular medications, and had minimal alcohol intake. In individuals meeting the same criteria, the prevalence of steatosis has been shown to be 5%18 or lower.19 The study was approved by the Human Research Ethics Committees of the Princess Alexandra Hospital and the University of Queensland. Informed written consent was obtained from all participants.
Although we considered the benefit of an additional obese non-NAFLD control group, the prospective liver biopsy of control participants for the purpose of this study was deemed unethical by the ethics committee and therefore exclusion of NAFLD in an obese control was not possible for this study. Further, it could be argued that obese individuals without steatosis are metabolically atypical20 and therefore not an appropriate control group. Instead, it has been proposed that healthier physically active individuals should be assigned as a control group.21 Accordingly, this study compares measurements in NAFLD with a healthy reference and then further explores study aims regarding disease severity within the NAFLD group alone.
General design
Each participant undertook testing in the morning after a 10–12 h overnight fast on two occasions within a 7-day period. The first testing session involved a hyperinsulinaemic–euglycaemic clamp with indirect calorimetry measurements to assess substrate oxidation rates in two conditions: basal (in resting and fasted conditions) and insulin-stimulated (during the steady-state of a hyperinsulinaemic–euglycaemic clamp). The second testing session involved indirect calorimetry measurement during a graded exercise test on a cycle ergometer to assess substrate oxidation rates and  (aerobic fitness).
(aerobic fitness).
Histological analysis of liver biopsy
Liver biopsy specimens were fixed in 10% neutral buffered formalin, embedded in paraffin, and subsequently scored by an expert hepatopathologist. The percentage of hepatocytes with steatosis was estimated. The severity of liver injury was assessed using the NAFLD activity score (NAS)22 and the criteria described by Brunt.23 A diagnosis of steatosis alone or NASH was made using conventional histological criteria, independent of NAS.24
Body composition
Fat mass and fat-free mass (FFM) were measured by dual-energy x-ray absorptiometry (GE Lunar Prodigy enCore 2005; General Electric, Madison, Wisconsin, USA). In the NAFLD group, distribution of abdominal fat (visceral and subcutaneous) was determined by computed tomography (Philips Brilliance 16; Philips, Cleveland, Ohio, USA) as previously described.25
Hyperinsulinaemic–euglycaemic clamp
Insulin sensitivity was evaluated by the hyperinsulinaemic–euglycaemic clamp technique,26 with a protocol previously described. 12 Teflon catheters were placed into an antecubital vein for infusions, and into a dorsal hand vein (heated to 55°C to achieve arterialisation of venous blood) for sampling. After a basal blood sample had been obtained, primed insulin infusion was initiated at a rate of 1 mU/kg/min (Humulin R; Eli Lilly, Indianapolis, Indiana, USA) and maintained at a constant rate throughout the procedure (120 min). Plasma glucose concentration was monitored every 5 min using an automated glucose analyser (YSI 2300 Stat Plus; YSI Life Sciences, Yellow Springs, Ohio, USA). Euglycaemia was maintained by infusing a 25% glucose solution at a variable rate.26
The glucose infusion rate at the steady-state of the hyperinsulinaemic–euglycaemic clamp (M-value) represented the whole-body glucose disposal rate. Non-oxidative glucose disposal rate was calculated by subtracting the oxidative glucose disposal rate (CHOox during the insulin-stimulated state determined by indirect calorimetry) from the M-value. The insulin sensitivity index (M/I), a measure of the quantity of glucose metabolised per unit of insulin concentration, was calculated by dividing M-value by the insulin concentration reached in the insulin-stimulated state.26 An index of adipocyte IR (adipo-IR) was calculated as the product of the fasting plasma FFA and insulin concentration.27
Biochemical analysis
Blood samples were drawn at 10 min intervals during the last 40 min of the hyperinsulinaemic–euglycaemic clamp. Glucose was analysed using an automated glucose analyser (interassay coefficient of variation (CV) 2%). Insulin was assayed using an immunoenzymatic assay with chemiluminescence detection (Unicel DxI 800 Immunoassay System, Beckman Coulter, Brea, California, USA). Total cholesterol, high-density lipoprotein (HDL)-cholesterol and TG were assayed by an enzymatic colorimetric assay with a Roche Modular Chemistry Analyser (South San Francisco, California, USA). Low-density lipoprotein (LDL)-cholesterol and very-low-density lipoprotein (VLDL)-cholesterol were calculated using the Friedewald equation.28 Serum FFA concentrations were measured with an in vitro enzymatic colorimetric method (Wako NEFA Assay; Wako Chemicals, Richmond, Virginia, USA; CV 2.3%). Plasma β-hydroxybutyrate concentration, an index of hepatic ketogenesis,29 was measured enzymatically (Stanbio, Boerne, Texas, USA; CV 2.2%).
Graded exercise test
Maximal aerobic power and substrate utilisation were assessed with a graded exercise test on a cycle ergometer. Testing included a sub-maximal phase to assess energy expenditure, Fatox and CHOox at various intensities, and a maximal phase to determine peak oxygen consumption ( ). The starting workload for the submaximal phase was individualised at 20% of the theoretical maximal mechanical work.30 Workload was increased by 10% at each stage until the respiratory exchange ratio was above 1.0 during the last minute of the stage. Stages lasted 5 min and were separated by 2 min rest intervals. The maximal phase started at a workload corresponding to two stages below the intensity reached at the end of the submaximal phase, and workload was incremented by 10% every minute until volitional exhaustion.
). The starting workload for the submaximal phase was individualised at 20% of the theoretical maximal mechanical work.30 Workload was increased by 10% at each stage until the respiratory exchange ratio was above 1.0 during the last minute of the stage. Stages lasted 5 min and were separated by 2 min rest intervals. The maximal phase started at a workload corresponding to two stages below the intensity reached at the end of the submaximal phase, and workload was incremented by 10% every minute until volitional exhaustion.
Indirect calorimetry
Indirect calorimetry measurements (TrueOne 2400 Metabolic Measurement System; Parvo Medics, Utah, USA) to determine oxygen consumption ( ) and carbon dioxide production (
) and carbon dioxide production ( ) were performed in three conditions: (1) basal, (2) insulin-stimulated and (3) exercise. Basal and insulin-stimulated measurements lasted 20 min with participants lying supine and breathing through a ventilated hood. Measurements during the graded exercise test were performed continuously, with participants wearing a mouthpiece and nose clip.
) were performed in three conditions: (1) basal, (2) insulin-stimulated and (3) exercise. Basal and insulin-stimulated measurements lasted 20 min with participants lying supine and breathing through a ventilated hood. Measurements during the graded exercise test were performed continuously, with participants wearing a mouthpiece and nose clip.
Whole-body respiratory quotient (RQ) was calculated as  . Whole-body Fatox and CHOox were calculated using stoichiometric equations and appropriate energy equivalents, with the assumption that the urinary nitrogen excretion rate was negligible.31 Average values of
. Whole-body Fatox and CHOox were calculated using stoichiometric equations and appropriate energy equivalents, with the assumption that the urinary nitrogen excretion rate was negligible.31 Average values of  and
and  were calculated during the last 10 min of basal and insulin-stimulated periods, and during the last minute of each submaximal exercise stage. Subsequently, Fatox values determined at each stage of the exercise test were graphically depicted as a function of exercise intensity. The stage at which the value of measured Fatox rate was maximal (maximal fat oxidation (MFO)) was determined and the corresponding intensity identified (Fatmax).32 Data measured at Fatmax were used for comparison between groups. M-value, energy expenditure and substrate oxidation rates were corrected for FFM.
were calculated during the last 10 min of basal and insulin-stimulated periods, and during the last minute of each submaximal exercise stage. Subsequently, Fatox values determined at each stage of the exercise test were graphically depicted as a function of exercise intensity. The stage at which the value of measured Fatox rate was maximal (maximal fat oxidation (MFO)) was determined and the corresponding intensity identified (Fatmax).32 Data measured at Fatmax were used for comparison between groups. M-value, energy expenditure and substrate oxidation rates were corrected for FFM.
Statistical analysis
Data are expressed as the mean±SD for all variables. Student t tests for independent samples were used to compare the mean values between groups categorised according to cohort (NAFLD vs controls), disease severity (NAFLD with NAS<5 vs NAFLD with NAS≥5), and BMI (NAFLD with BMI< or ≥33 kg/m2). Paired Student t tests were used to compare energy expenditure and substrate oxidation rates in different conditions within groups. Analysis of covariance was used to adjust for FFM. Association between continuous variables was assessed using Spearman's non-parametric rank correlation coefficient and multivariate analysis. Statistical analysis was performed with the software SPSS V.17.0 for Windows and GraphPad Prism V.5.0 for Mac. For all statistical analyses, the level of significance was set at p<0.05.
Results
Participant characteristics
Characteristics of study groups are presented in table 1. Liver histology from patients with NAFLD showed macrovesicular steatosis ranging from 10% to 100%, with an average of 71±31%. Sixteen patients were diagnosed with NASH, while four were diagnosed with steatosis alone. Fourteen patients had a NAS≥5, while six patients had a NAS<5. Fibrosis was observed in 10 patients (stage 1 in three, stage 2 in four, and stage 3 in three).
Demographic, anthropometric and laboratory characteristics of the study groups
Age and gender were not significantly different between NAFLD and controls. BMI and percentage of body fat were higher in the NAFLD group than the controls. Patients with NAFLD had higher fasting plasma TG, insulin and glucose, while fasting plasma FFA did not differ between groups. In the NAFLD cohort, visceral adipose tissue (VAT) area was 194±94 cm2, while subcutaneous adipose tissue area was 384 ±197 cm2.
Insulin resistance
Patients with NAFLD were severely insulin resistant (table 2), with lower M-value than lean controls (4.1±1.5 vs 9.1±2.2 mg/kgFFM/min, p<0.001), and demonstrated impairment in both the oxidative (3.0±0.7 vs 3.6±0.7 mg/kgFFM/min, p=0.04) and non-oxidative (1.8±1.3 vs 5.1±2.4 mg/kgFFM/min, p<0.001) glucose disposal pathways.
Metabolic variables during basal, insulin-stimulated and exercise conditions in NAFLD versus control
The insulin sensitivity index, M/I, was also significantly lower in NAFLD (5.9±3.6 vs 17.1±5.1 (mg/kgFFM/min)/(mU/l), p<0.001), showing that the differences between groups were maintained after adjustment for the insulin levels reached (80.6±26.9 in NAFLD vs 51.2±7.9 mU/l in controls, p<0.001). Adipo-IR was more severe in patients with NAFLD than in controls (11.1±8.6 vs 2.2±1.3 (mmol/l)·(mU/l), p<0.001) and in NAFLD patients with fibrosis compared with those without (17.5±10.2 vs 7.2±4.1 (mmol/l)·(mU/l), p=0.013). Within the NAFLD cohort, adipo-IR was associated with BMI (r=0.70, p<0.001), VAT (r=0.53, p=0.02) and M-value (r=−0.50, p=0.003), but not with hepatic steatosis (r=0.23, p=0.35).
Substrate oxidation under basal conditions
After adjustment for FFM, total energy expenditure in the basal state did not differ between groups (p=0.26). However, the proportion of energy derived from fat and CHO did differ between groups, with patients with NAFLD oxidising more CHO (2.41±0.73 vs 1.6±0.77 mg/kgFFM/min, p=0.004) and less fat (1.22±0.28 vs 1.49±0.39 mg/kgFFM/min, p=0.024) than controls (figure 1A,B). This was confirmed by the higher RQ in patients with NAFLD (0.82±0.04 vs 0.78±0.03, p=0.007, figure 1C).
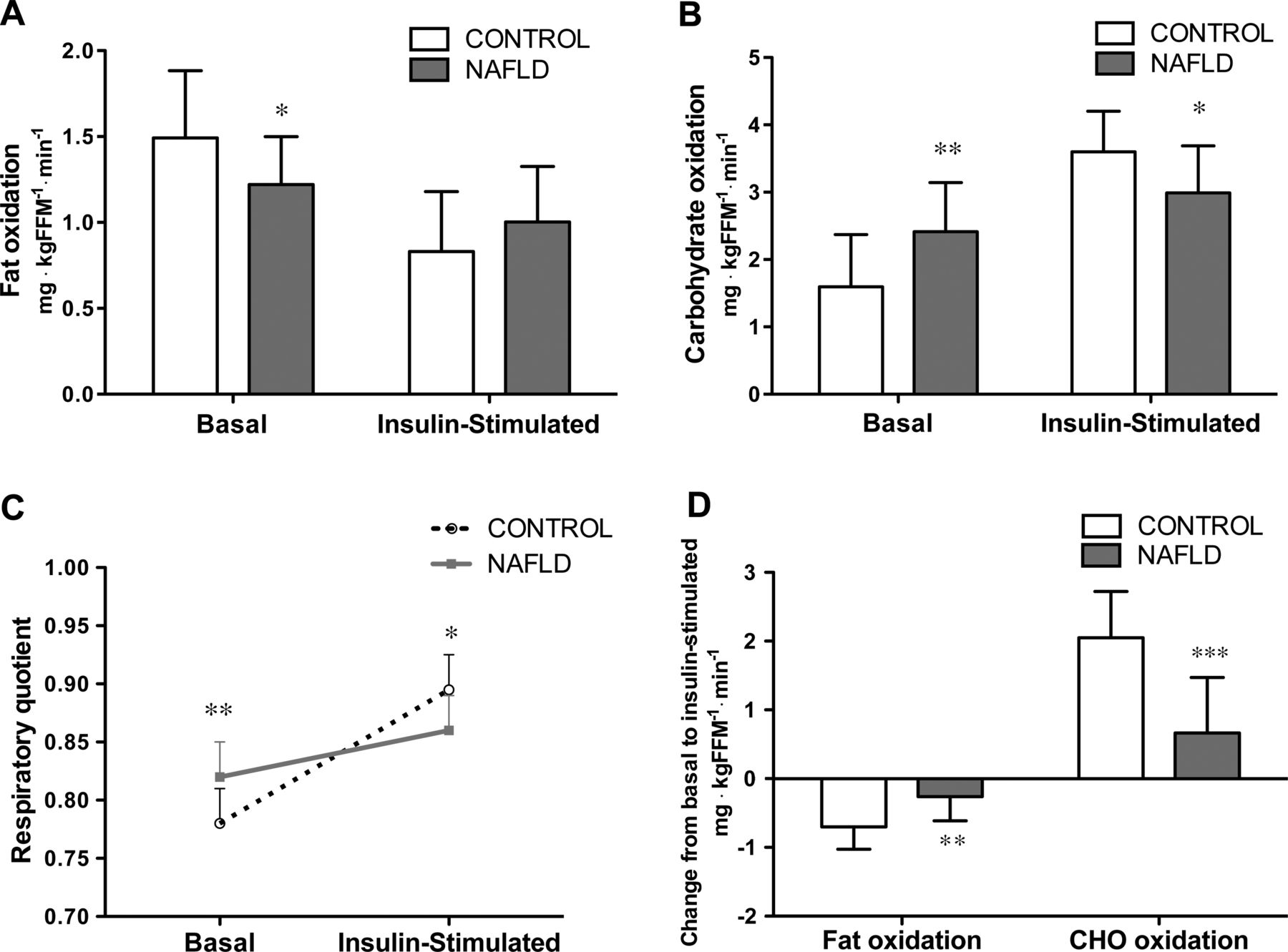
Fat oxidation (A) and carbohydrate oxidation (B) under basal and insulin-stimulated conditions in 15 control vs 20 non-alcoholic fatty liver disease (NAFLD) participants. (C) Respiratory quotient under basal and insulin-stimulated conditions. (D) Change in substrate utilisation from basal to insulin-stimulated state. *p<0.05, **p<0.01 and ***p<0.001 between control and NAFLD.
Within the overweight/obese NAFLD group, basal RQ correlated positively with hepatic steatosis (r=0.57, p=0.01, figure 2A). This association was confirmed by linear regression multivariate analysis, after BMI, % body fat, VAT, subcutaneous adipose tissue, age and gender had been controlled for (standardised β=0.56, p=0.021). Indeed, basal RQ did not correlate with VAT (r=0.07, p=0.77), % body fat (r=0.31, p=0.19) and BMI (r=0.29, p=0.23, figure 2B), and was not significantly different in patients with NAFLD with BMI < or ≥33 kg/m2 (online supplementary table 1). Further, basal RQ was significantly lower in the six patients with NAS<5 than in the 14 patients with NAS≥5 (0.79±0.02 vs 0.83±0.03, p=0.008, figure 2C), and this difference also persisted after adjustment for VAT (p=0.01), % body fat (p=0.01) and BMI (p=0.02).

(A) Correlation between % hepatic steatosis and basal respiratory quotient (RQ) in 20 overweight/obese patients with non-alcoholic fatty liver disease (NAFLD). The positive association between basal RQ and hepatic steatosis was maintained after body mass index (BMI), % body fat, visceral adipose tissue (VAT), subcutaneous adipose tissue, age and gender had been controlled for (standardised β=0.56, p=0.021). (B) Correlation between basal RQ and BMI in 20 overweight/obese patients with NAFLD. (C) Basal RQ in patients with NAFLD having a NAFLD activity score (NAS)<5 (n=6) versus patients having a score ≥5 (n=14). The difference persisted after adjustment for VAT (p=0.01), % body fat (p=0.01) and BMI (p=0.02).
Patients with NAFLD showed evidence of reduced hepatic ketogenesis with lower basal plasma concentrations of β-hydroxybutyrate than lean controls (0.09±0.03 vs 0.14±0.07 mmol/l, p=0.004, figure 3A). Within the NAFLD cohort, fasting concentrations of β-hydroxybutyrate correlated inversely with fasting plasma TG (r=−0.64, p=0.002, figure 3B) and VLDL-cholesterol (r=−0.67, p=0.002), but did not correlate with fasting insulin (p=0.42), fasting FFA (p=0.42), % hepatic steatosis (p=0.96) or basal RQ (p=0.40). β-Hydroxybutyrate concentrations did not differ between patients with NAS<5 and those with NAS≥5 (0.10±0.04 vs 0.09±0.2, p=0.60), nor between patients with BMI<33 kg/m2 and those with BMI≥33 kg/m2 (online supplementary table 1). When NAFLD and control groups were combined, fasting concentrations of β-hydroxybutyrate also correlated inversely with fasting plasma TG (r=−0.64, p<0.001) and VLDL-cholesterol (r=−0.63, p<0.001).

(A) Fasting β-hydroxybutyrate in 15 control vs 20 non-alcoholic fatty liver disease (NAFLD) participants. **p<0.01. (B) Correlation between fasting β-hydroxybutyrate and fasting triglycerides in 20 overweight/obese patients with NAFLD.
Substrate oxidation under insulin-stimulated conditions
Under insulin-stimulated conditions, there was no apparent difference between groups in total energy expenditure (p=0.27). However, patients with NAFLD had lower CHOox (p=0.036, figure 1C) and a lower RQ (p=0.037, figure 1C). The switch in substrate oxidation in response to insulin stimulation was different between groups: patients with NAFLD increased CHOox and suppressed Fatox to a lesser extent than controls (0.67±0.81 vs 2.05±0.68 mg/kgFFM/min, p<0.001, and −0.26±0.35 vs −0.7±0.33 mg/kgFFM/min, p=0.001, respectively, figure 1D). Consistently, the change in RQ from the basal state was smaller in NAFLD (0.04±0.03 vs 0.11±0.04, p<0.001, figure 1C). Hepatic steatosis did not correlate with change in RQ from basal to insulin-stimulated conditions (p=0.29); however, there was a trend for the % hepatic steatosis to correlate with the insulin sensitivity index (r=−0.40, p=0.09).
Substrate oxidation during exercise
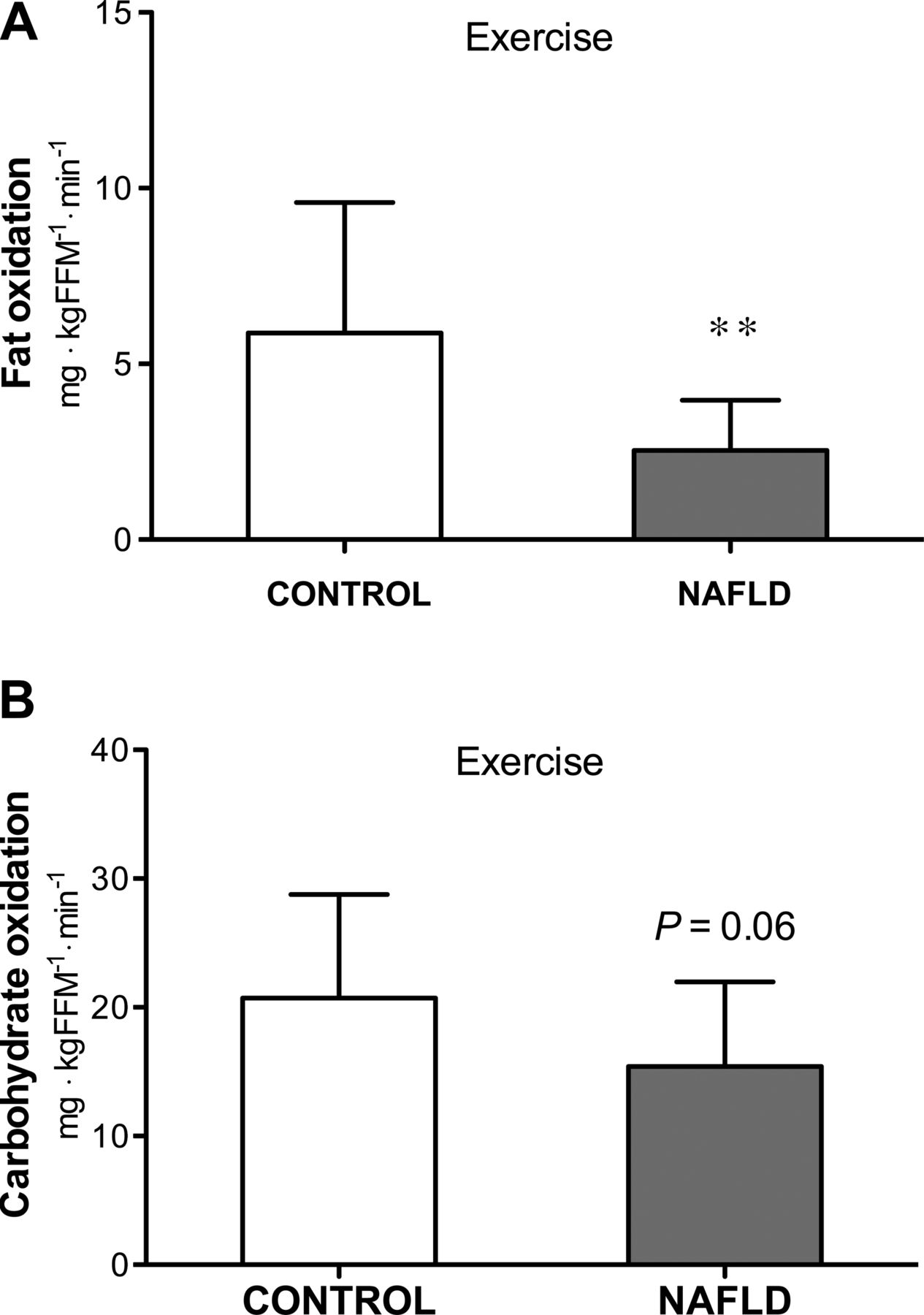
Aerobic fitness, as measured by  , was lower in the NAFLD group (33.6±6.7 vs 52.7±19.0 ml/kgFFM/min, p<0.001, table 2). When cycling at the intensity eliciting MFO (figure 4), patients with NAFLD had a lower MFO (2.54±1.43 vs 5.87±3.71 mg/kgFFM/min, p=0.002) than the control group. CHOox was not significantly different, but tended to be lower in NAFLD (p=0.06), while total energy expenditure (p<0.001) and increase in both Fatox (p=0.002) and CHOox (p=0.023) from basal to exercise were significantly lower in NAFLD. The intensity at which MFO was reached (Fatmax) was lower in NAFLD when expressed in absolute terms (45.7±17 vs 103.4±47.3 W, p<0.001), but not in relative terms (50.2±15.9% vs 48.9±11.2% of
, was lower in the NAFLD group (33.6±6.7 vs 52.7±19.0 ml/kgFFM/min, p<0.001, table 2). When cycling at the intensity eliciting MFO (figure 4), patients with NAFLD had a lower MFO (2.54±1.43 vs 5.87±3.71 mg/kgFFM/min, p=0.002) than the control group. CHOox was not significantly different, but tended to be lower in NAFLD (p=0.06), while total energy expenditure (p<0.001) and increase in both Fatox (p=0.002) and CHOox (p=0.023) from basal to exercise were significantly lower in NAFLD. The intensity at which MFO was reached (Fatmax) was lower in NAFLD when expressed in absolute terms (45.7±17 vs 103.4±47.3 W, p<0.001), but not in relative terms (50.2±15.9% vs 48.9±11.2% of  , p=0.80). After adjustment for
, p=0.80). After adjustment for  by covariate analysis, MFO did not differ between groups (p=0.13). MFO during acute exercise did not correlate with degree of steatosis (p=0.26) and was not significantly different in patients with NAS<5 compared with patients with NAS≥5 (p=0.79).
by covariate analysis, MFO did not differ between groups (p=0.13). MFO during acute exercise did not correlate with degree of steatosis (p=0.26) and was not significantly different in patients with NAS<5 compared with patients with NAS≥5 (p=0.79).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fat oxidation (A) and carbohydrate oxidation (B) during exercise in 15 control vs 20 non-alcoholic fatty liver disease (NAFLD) participants. **p<0.01 between control and NAFLD.
All the results of this study were confirmed by covariate analysis, with FFM as covariate.
Discussion
In NAFLD, hepatic steatosis is intricately linked with a number of metabolic alterations. In this study, overweight/obese patients with NAFLD showed reduced whole-body Fatox in basal conditions and during acute exercise compared with lean controls. Within the overweight/obese NAFLD group, alterations in basal substrate metabolism were associated with more severe steatosis and more severe disease, independently of BMI and fat topography. Patients with NAFLD also had reduced basal hepatic Fatox, and this was associated with increased fasting circulating TG.
This study was designed to comprehensively investigate substrate metabolism and IR. It is the largest study to assess disease severity by liver histology in conjunction with whole-body substrate metabolism and IR. Substrate oxidation was measured in three different physiological states (basal, insulin-stimulated and exercise) which forms an ideal framework for studying whole-body energy homoeostasis and understanding mechanisms of dysfunction. Gold standard techniques for the assessment of liver disease (liver histology), IR (hyperinsulinaemic–euglycaemic clamp) and body composition (dual-energy x-ray absorptiometry) were used. Patients with NAFLD with a broad spectrum of steatosis were studied (10–100%).
In the patient group studied, NAFLD and obesity coexisted, and therefore it was not possible to establish the specific contribution of each factor to the differences observed between patients and lean controls. For this reason, we did not limit our study to a comparison between NAFLD and controls, but also performed analyses within the overweight/obese NAFLD cohort, to establish the relationship between disease severity and substrate oxidation under different physiological conditions.
In basal conditions, patients with NAFLD exhibited an alteration in whole-body substrate metabolism, with a lower Fatox and a higher CHOox compared with controls. The different outcome compared with previous studies (which showed Fatox to be lower,11 similar,14 or trending to be higher12 in NAFLD vs controls) may be due to the heterogeneity of disease severity in NAFLD or to differences in plasma substrate concentrations such as fasting glucose and fasting FFA. Anthropometric characteristics of the study groups may also be implicated. Some studies have attempted to match groups for BMI by comparing lean11 or moderately overweight individuals14 with and without NAFLD. While this approach has some advantages, it also has limitations. Lean individuals with NAFLD represent only a small proportion of the clinical population18 ,19 and may have different genetic characteristics.2 In addition, BMI is a poor indicator of body composition and body fat distribution at the individual level.33
To determine if there was a dose effect between the severity of steatosis and basal substrate metabolism, we performed analyses within the overweight/obese NAFLD cohort. We found that hepatic steatosis correlated positively with basal RQ and that RQ was significantly higher in patients with more severe disease. A higher basal RQ indicates that a smaller proportion of whole-body total energy expenditure is derived from Fatox. These findings were independent of VAT, % body fat and BMI. These observations suggest that reduced whole-body Fatox in basal conditions may contribute to hepatic fat accumulation and may be implicated in the pathogenesis of NAFLD. Accordingly, a recent review proposed that alterations in fatty acid metabolism lead to an accumulation of ectopic (intrahepatic and intramuscular) TG, resulting in IR in liver and skeletal muscle.6
In addition to lower basal rates of whole-body Fatox, the patients with NAFLD we studied had lower basal concentrations of β-hydroxybutyrate, indicating reduced hepatic Fatox.29 The lower basal β-hydroxybutyrate in NAFLD despite similar basal FFA concentrations for both NAFLD and control suggests differential fatty acid partitioning in the liver between groups.34 Indeed, VLDL-cholesterol (a product of the esterification pathway) was higher in NAFLD, while β-hydroxybutyrate (a product of the oxidative pathway) was lower. Basal β-hydroxybutyrate correlated negatively with VLDL-cholesterol and TG, both when groups were combined and when the analysis was performed within the NAFLD cohort. In animal models, inhibition of hepatic Fatox leads to an increase in hepatic steatosis,35 ,36 while an increase in hepatic Fatox reduces hepatic steatosis.37 ,38 In humans, lower basal β-hydroxybutyrate concentrations were found in obese than in lean individuals39 ,40 and in hypertriglyceridaemic compared with normolipidaemic moderately obese individuals.41 Few studies have examined this issue in NAFLD, and results are inconsistent, with either higher12 or similar13 ,14 β-hydroxybutyrate concentrations in NAFLD versus controls. In these studies, the differences in hepatic Fatox between patients and controls mirror those for fasting FFA.12–14
When studying substrate oxidation in insulin-stimulated conditions, we noted that patients with NAFLD increased CHOox and suppressed Fatox to a lesser extent than controls, and this was consistent with previous observations.11 ,12 ,14 In other words, patients demonstrated metabolic inflexibility, which was defined by Kelley et al as an impaired capacity to adapt fuel oxidation to fuel availability.42 Assessment of IR revealed that the patients with NAFLD had lower M-value and lower oxidative and non-oxidative glucose disposal than the control group, indicating a global impairment in skeletal muscle glucose metabolism. Between-group differences in insulin sensitivity were even more apparent after normalisation for the insulin concentrations achieved. We acknowledge that M-value and non-oxidative glucose disposal rate may be underestimated in this study given that the hepatic glucose output was not considered; however, previous research has shown that, with the insulin dosage used in the present study, hepatic glucose output is minimal even in obese patients13 or those with NAFLD.12 Further, consistent with previous observations, we showed that patients with NAFLD had more severe IR in the adipose tissue than controls12 ,43 and that severity of adipo-IR was related to the severity of hepatic fibrosis.44 ,45
Another finding of the present study was that, during exercise, MFO in patients with NAFLD was less than half that in control participants, indicating a reduced ability to increase fat oxidation during an acute exercise session. However, the lower aerobic fitness appeared to contribute to the lower MFO observed in patients with NAFLD. After correction for  , the difference in MFO between NAFLD and control was no longer apparent. Further, the exercise intensity at which MFO occurred, Fatmax, was significantly lower in NAFLD than controls when expressed in absolute terms (W), but not when expressed in relative terms (
, the difference in MFO between NAFLD and control was no longer apparent. Further, the exercise intensity at which MFO occurred, Fatmax, was significantly lower in NAFLD than controls when expressed in absolute terms (W), but not when expressed in relative terms ( ). Outcomes of studies investigating substrate oxidation during exercise in type 2 diabetes and obesity are divided. Some reported a lower Fatox during exercise in obese patients46 and those with type 2 diabetes47 ,48 compared with controls, while other found no difference.49 ,50
). Outcomes of studies investigating substrate oxidation during exercise in type 2 diabetes and obesity are divided. Some reported a lower Fatox during exercise in obese patients46 and those with type 2 diabetes47 ,48 compared with controls, while other found no difference.49 ,50
We also observed that the aerobic fitness of patients with NAFLD was extremely low, with most patients falling in the lowest percentile according to the American College of Sports Medicine guidelines.51 Low fitness level52 and NAFLD53 have been shown to be independently associated with the risk of cardiovascular events; however, few studies have assessed physical fitness quantitatively in NAFLD.
Longitudinal studies demonstrate that lifestyle interventions aimed at increasing aerobic fitness improve IR54 and positively affect Fatox under basal55 and exercise16 ,56 conditions. A recent study showed that the magnitude of reduction in steatosis after energy restriction correlated negatively with post-treatment plasma ketone body and with post-treatment basal RQ,57 suggesting that enhanced hepatic and whole-body Fatox contribute to the reduction in steatosis. Therefore, approaches that enhance basal and exercise Fatox may have a role in the management of NAFLD. These include exercise training,55 energy restriction,57 and also some pharmacological58 and nutraceutical agents.59
In conclusion, this study shows that overweight/obese patients with NAFLD have reduced basal whole-body and hepatic Fatox, and reduced Fatox during exercise compared with lean controls. Irrespective of body composition, there was an inverse relationship between ability to oxidise fat in basal conditions and histological features of NAFLD. This suggests that reduced basal Fatox may contribute to ectopic accumulation of fat in the liver and may be implicated in the pathogenesis of NAFLD. This alteration may represent an important therapeutic target for new treatments in NAFLD. Behavioural and pharmacological approaches that promote Fatox in basal and exercise conditions warrant further investigation in this patient population.
Acknowledgments
We thank Dr William Petchey, Julianne Wilson and Fiona Henderson for clinical assistance, and Jit Pratap for radiological imaging.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors IC: drafting of the manuscript; study design; data acquisition; data analysis; interpretation of data. NMB: study design; material support; interpretation of data; critical revision of the manuscript. SC: study design; data analysis, interpretation of data; critical revision of the manuscript. APH: material support; interpretation of data; critical revision of the manuscript. VSC: data acquisition; interpretation of data; critical revision of the manuscript. ADC: data analysis; interpretation of data; critical revision of the manuscript. TMO: data acquisition; material support; interpretation of data; critical revision of the manuscript. GAM: study design; data acquisition; material support; interpretation of data; critical revision of the manuscript. JBP: study design; material support; interpretation of data; critical revision of the manuscript. IJH: study design; data acquisition; obtained funding; material support; interpretation of data; critical revision of the manuscript; study supervision.
-
Funding This study was supported by the National Health and Medical Research Council (NHMRC) Australia and the Lions Medical Research Fellowship.
-
Competing interests None.
-
Ethics approval The Human Ethics Research committee of the Princess Alexandra Hospital, Brisbane; The University of Queensland Human Ethics Research Committee; Queensland University of Technology Human Ethics Research Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.