Article Text

Abstract
Objectives: To investigate whether longstanding illnesses, social context, and current socioeconomic circumstances predict quality of life.
Design: Secondary analysis of wave 1 of the English longitudinal study of aging. Missing data were imputed and multiple regression analyses conducted.
Setting: England, 2002
Participants: Nationally representative sample of non-institutionalised adults living in England (n = 11 234, 54.5% women, age 65.1 (SD 10.2) years).
Main outcome measure: Quality of life as measured by CASP-19, a 19 item Likert scaled index.
Results: The quality of life was reduced by depression (β −0.265), poor perceived financial situation (β −0.157), limitations in mobility (β −0.124), difficulties with everyday activities (β −0.112), and limiting longstanding illness (β −0.112). The quality of life was improved by trusting relationships with family (β 0.105) and friends (β 0.078), frequent contacts with friends (β 0.059), living in good neighbourhoods (β 0.103), and having two cars (β 0.066). The regression models explained 48% variation in CASP-19 scores. There were slight differences between age groups and between men and women.
Conclusions: Efforts to improve quality of life in early old age need to address financial hardships, functionally limiting disease, lack of at least one trusting relationship, and inability to move out of a disfavoured neighbourhood. There is the potential for improved quality of life in early old age (the third age) if these factors are controlled.
- quality of life
- third age
- social networks
- long term illness
- depression
Statistics from Altmetric.com
The nature of old age in countries like Britain is changing because of a combination of the increase in life expectancy at middle age,1 the tendency towards early retirement,2 and the availability of pensions.3,4 Consequently, an increasing proportion of the population can expect to spend from 10 to 20 years after retirement from paid employment in reasonable health and comparative affluence.5
Former notions of old age are being made obsolete by these sociodemographic changes.6 Laslett usefully has divided old age into a third age and a fourth age; although these are stages of the life course, not chronologies, the core of early old age or the third age can be regarded as those in their 60s and 70s with a periphery of those in their late 50s and early 80s7 Essentially, the third age stretches from labour market exit to the onset of physical dependency; and the fourth age spans from the onset of physical dependency (or vulnerability) until death. Although Laslett’s ideas have been challenged, he is describing a real phenomenon that has important policy implications. Policies such as statutory regulation of institutional care and financial support for informal carers are needed to preserve quality of life in the fourth age whereas the third age involves market relations (the grey pound), autonomy, and policies designed to maximise quality of life and postpone the onset of physical dependency, with its need for health and welfare services.
Aging is perceived to decrease quality of life 8; however, when controlled for other factors, the effects of age may disappear.9 The emergence of the third age demands that we look for predictors of quality of life other than age. Significant events during this stage of the life span include loss of income because of exit from the labour force and the increasing probability of illness. Measures of subjective wellbeing have been shown to be associated with financial situation and health and functioning.10,11 The Berlin aging study12 found that good health (measured as self reported illnesses and self assessed health) was important for a strong sense of wellbeing in its sample of people aged 70–105 years; an age spread that includes the third age.13 The study also found that income and satisfaction with income influenced subjective wellbeing in old age.14 Although life satisfaction does not show gender differences,15 the gendered dimension of aging cannot be neglected.16 Contextual factors like social capital, social networks, and social participation also can contribute to the quality of life in older ages.17–19
There is a burgeoning literature on quality of life. A systematic review on quality of life as measured using patient assessed health outcomes showed that only a small portion of the studies deal with older age groups,20 although the volume of relevant literature will increase if studies from social sciences on wellbeing, life satisfaction, and happiness are included.21 Most of these studies used a measure of quality of life that is either subjectively assessed or measured through proxies like health status. Recently, a new measure of quality of life, CASP-19, has been developed as a reaction to the under theorised nature of existing measures and with the premise that any quality of life measure should be distinct from the factors that influence it.22 In a small nationally representative sample of Boyd Orr cohort aged between 65 and 75 years, Wiggins and his colleagues found that the quality and the density of the social networks, recent loss, inadequate pension provision, and living in a poor or deprived neighbourhood were good predictors of CASP-19.23 The Boyd Orr sample was numerically small with a narrow age range that does not encompass the full scope of the third age. It is not known whether the same influences on CASP-19 will be selected in larger populations with a wider age range.
Fortunately, newly available data from the first sweep of the English longitudinal study of aging (ELSA) includes CASP-19 allow us to explore the influences on quality of life in a large national sample of older English residents living in private households.
METHODS
Sample
We have used data from the first wave of the ELSA. The technical details of this study and the results of primary analyses have been published24 (also available at the web site of the Institute of Fiscal Studies http://www.ifs.org.uk/elsa/report.htm). The study collected information on the personal, economic, and social circumstances of aging from a national sample of the non-institutionalised adults aged 50 years or more living in England in 2002. ELSA sample was drawn from three years (1998, 1999, and 2001) of health survey for England (HSE). The issued sample for ELSA wave 1 was 18 813 and the achieved sample was 12 100. The main reason for non-response was refusal. The distributions of issued and achieved samples were similar with only a minimal bias towards younger age groups in the issued sample (see tables 9.1 and 9.3 reference 24). The data included weighting to reduce non-response bias and to be representative of the population. Our analyses were restricted to study members who answered the interview directly, without the use of a proxy respondent; a total of 11 234 subjects (age 50–100 years), from a total sample of 12 100 were in this category. There were varying degrees of missingness (or item non-response) for the variables selected for the analyses; 8038 (72%) sample members had complete data (no item missingness) on the variables of interest.
Outcome
Our outcome variable was CASP-19, an index based on 19 Likert scaled items spanning four theoretically derived dimensions of quality of life in early old age: control, autonomy, self realisation, and pleasure.22 Each Likert scaled item was numerically coded so that the most positive response was scored as 3 and the most negative response as 0. Some of the items were reverse coded so that all item responses were in the same direction. The CASP-19 score used in the analysis was the arithmetic sum of the scores for all of the 19 items, ranging from 0 to 57. High scores corresponded to higher quality of life. The information for CASP-19 was collected using a self completion questionnaire.
Explanatory variables
We selected variables related to health, functioning, social relations, and material circumstances as our predictor variables. Health variables included binary variables to note the presence of longstanding illness and limitations attributable to longstanding illness, and a depression indicator based on the eight item Center for Epidemiological Studies depression scale dichotomised so that a score of 3 or more denotes depression.25 Difficulties with physical functioning were divided into two groups: (1) mobility and ambulation ((both upper and lower limb functions) and (2) combined activities of daily living (ADL) and instrumental activities of daily living (IADL) (see chapter 7 reference 24). Any recorded difficulty in each group was simply summed to create final scores. There was also a variable to indicate whether support for limitation in every day activities was available or not.
A number of binary variables referring to the nature of a person’s social relations were adopted: living alone (not in a couple); caring for somebody; doing volunteer work; retired; looking after home; unemployed or unable to work because of sickness, and other causes (combined together because of small numbers). We have distinguished three aspects of social network: the quality (whether participants felt their relationships with children, family, and friends were based on understanding, confidence, and support), frequency (how often a participant met or contacted by phone or email children, family and friends), and the existence of close or confiding relationships (a count of the number of children, family, and friends with whom the participant had close relationships). These were elicited in the survey as multiple item questions with ordinal multiple responses. In all instances of multiple item scales, we created summary scores by adding item responses after recoding to ensure uniform direction of response.
We combined quality and frequency scores for children and family while those for friends were kept separate. In addition, we included the characteristics of the neighbourhood based on a nine item scale, recording area characteristics such as presence of vandalism, a sense of belonging, and perceptions of trust and support. For this simple summary index, higher scores meant better neighbourhoods.
Three variables represented material circumstances: a binary variable representing membership in the top 40% of the income distribution, ownership of one car, ownership of two or more cars, and perceived poor financial situation. We also adjusted for age, sex, education, and socioeconomic position based on the three group version of National Statistics—socioeconomic classification (NS-SEC).26
Treatment of missing values
Our analysis was conducted in two phases: firstly, we analysed the sample with complete data (n = 8038) and secondly, we repeated the analyses after replacing records that had any missingness (an additional 3196 cases providing a filled in dataset of n = 11 234).
In the original (a matrix with 11 234 rows (cases) and 49 columns (variables)) there were 6.3% of the cells empty. Most of the missing cells were among the items for CASP-19 (10.2%) and neighbourhood characteristics (10.5%). For a rate of missing information at 6%, analysing five replicate datasets with imputed data will be 99% efficient.27 We used software NORM, which uses EM algorithm and data augmentation to create the replicate datasets (NORM: multiple imputation of incomplete multivariate data under a normal model, version 2.0, software for Windows 95/98/NT, 1999, available from http://www.stat.psu.edu/~jls/misoftwa.html). The analyses were repeated for these imputed datasets and the final parameter estimates obtained by using Rubin’s rule.27
We fitted multiple regression models with CASP-19 score as our dependent variable. To investigate the effect of age and sex further we repeated the analysis separately for three age groups: 50–64, 65–74 and 75+ years, and separately for men and women.
All analyses were done using Stata version 8.1, routinely using population weights to adjust for any differential probabilities of selection.
RESULTS
The average age of 11 234 participants in ELSA wave 1 sample was 65.1 (SD 10.2) years with a majority of women (6123, 54.5%). A large proportion of them (4775, 42.6%) had no formal educational qualifications from accredited courses and 5147 (46.9%) were in routine occupations (like routine sales and services occupations or manual labour) or had been in their last period of employment. Table 1 shows the distributions for the variables used in the study including the amount of missing data.
Distributions of the variables used in the study
We had complete data on CASP-19 for 9300 people and table 2 shows the CASP-19 scores in different sociodemographic strata The average CASP-19 score for the whole sample was 42.5 (SD 8.7). Only the oldest age group, 75+ years group, had a CASP-19 score (40.0, 95%CI 39.5 to 40.4) that was significantly lower than younger age groups. Women had a significant, albeit small, advantage over men. People with no educational qualifications had significantly lower CASP-19 score (40.5, 95%CI 40.2 to 40.8) than those with some qualification (43.7, 95%CI 43.5 to 43.9). There was a gradient in CASP-19 scores according to NS-SEC, with those in the management occupations having the highest level of CASP-19 scores. A steeper gradient existed for income quintile with CASP-19 scores falling from 45.5 (95%CI 45.2 to 45.8) for the highest quintile to 40.3 (95%CI 39.8 to 40.7) for the lowest quintile.
Unadjusted CASP-19 scores according to sociodemographic variables in a sample of 9300 participants with complete information on CASP19
Multiple regression
We repeated analyses for the complete and the five filled in datasets. As the resulting regression coefficients did not vary significantly, we are presenting here the results for the complete data (table 3), with those for the filled in data given in the appendix 2 for comparison (appendix 2 is available on line http://www.jech.com/supplemental).
Multiple linear regression of CASP19 scores using complete data
We found physical health, functioning, and mental health had great influence on quality of life. A longstanding illness could reduce quality of life scores by half a unit (−0.481, 95%CI −0.827 to −0.136) while if the illness was limiting, the reduction would be almost four times larger (−2.062, 95%CI −2.504 to −1.620). Limitations in physical activities reduced quality of life (mobility −0.434, 95%CI −0.545 to −0.323; ADL/IADL −0.605, 95%CI −0.758 to −0.452). Similarly having no support with limitations in everyday activities also reduced quality of life (−0.716, 95%CI −1.036 to −0.396). The impact of depression in reducing quality of life was the highest (−5.464, 95%CI −5.875 to −5.054).
Equally strong was the influence of factors representing material wellbeing. Perceiving financial circumstances to be poor had a very high effect on lowering quality of life scores (−2.878, 95%CI −3.202 to −2.555), while owning cars and being on the high end of income distribution improved quality of life scores. Economic inactivity because of unemployment reduced quality of life; conversely retirement improved it.
Social relationships and circumstances can have positive effects on quality of life. Quality of life increased with trusting relationships with children and family (0.108, 95%CI 0.083 to 0.133) and with friends (0.144, 95%CI 0.100 to 0.188). Similarly, greater frequency of contacts with friends significantly raised quality of life (0.157, 95%CI 0.098 to 0.217). Having a number of close relationships improved the CASP-19 scores 0.072, 95%CI 0.048 to 0.096). Living in a neighbourhood perceived to be good increased quality of life (0.137, 95%CI 0.113 to 0.161) and so did living alone. But all social relationships need not have such positive outcomes. Greater frequency of contacts with children and family, caring for someone, and looking after home or family could significantly reduce quality of life. Conversely doing volunteer work would improve quality of life (0.771, 95%CI 0.371 to 1.170).
The standardised β coefficients permit direct comparison between variables. Significant negative influences on quality of life scores were financial situation perceived as poor (−0.157), depression (−0.265) limitation in physical activities (ADL/IADL −0.112; mobility −0.124), and limitations attributable to longstanding illness (−0.112). Significant positive influences were good neighbourhood (0.103), trusting relationships with children and family (0.105) and with friends (0.078), and having two or more cars (0.066).
Our regression models explained 48% variation in quality of life scores.
Age effects
We repeated the above analyses for three age groups: 50–64, 65–74, and 75+ years (results not shown). The influence of different factors varied between age groups. The 50–64 years old had results similar to the general model described above. In this age group, being retired (1.284, 95%CI 0.806 to 1.761) and living alone (0.748, 95%CI 0.331 to 1.164) seem to be significant boosters to the quality of life score. In the older age groups (65–74 and 75+ years), access to car, unemployment, longstanding illness in itself, and lack of support with limitations in everyday activities lost significance. In 65–74 years old volunteer work and looking after home were also not significant while frequency of contacts with children and family significantly reduced quality of life in this group only. For the oldest group having no educational qualification, being in the top 40% of income distribution and frequency of contacts with friends were also not significant. But they had greater positive impact of volunteer work (2.011, 95%CI 1.032 to 2.990) and negative impacts of being retired (−4.665, 95%CI −7.895 to −1.435) and looking after home (−5.015, 95% CI −8.429 to −1.601).
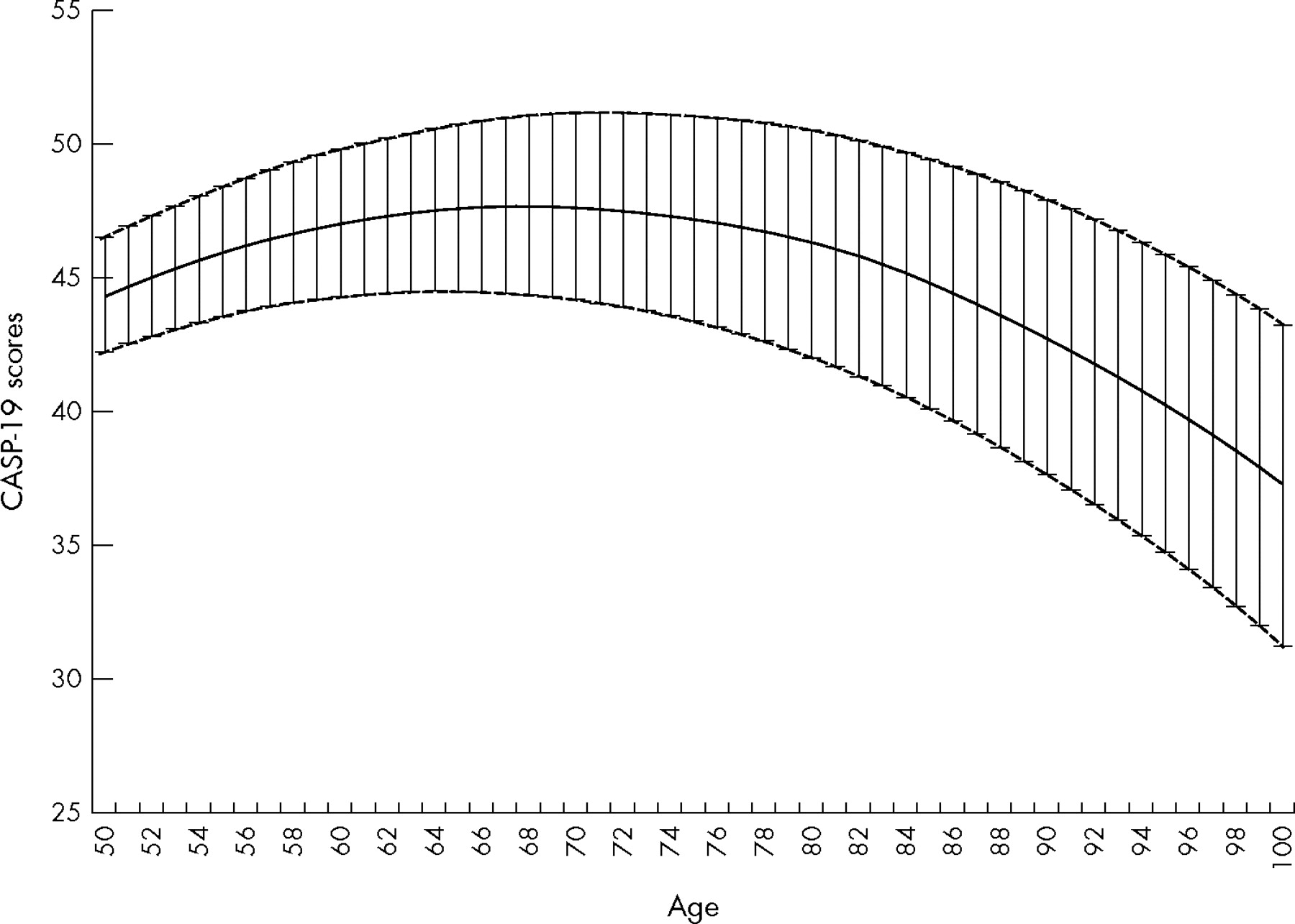
Figure 1 show the estimates, from our cross sectional data, of influence of aging on quality of life, when all other factors are controlled. Quality of life increases from 50 years (CASP-19 score 44.4) to peak at 68 years (CASP-19 score 47.7). From there it gradually starts to decline, reaching the same level as at 50 years by 86 years. By 100 years, CASP-19 score has declined to 37.3.

{kind=link}
Age curve* for quality of life from 50 to 100 years. Point estimates and 95% confidence intervals English longitudinal study of aging (wave 1). *Adjusted for sex, education, income, car, perceived financial inadequacy, volunteering, retirement and economic inactivity, longterm illness, limiting illness, disability in ADL and IADL, frequency, quality and closeness of relationships with friends, and children and family, support for disability, carer, living in good neighbourhood, and depression.
Gender effects
We examined for gender effects by running models separately for men and women (results not shown). For women the quality of life was reduced by being a carer, being not in employment because of looking after home and family, and having increased frequency of contact with children and family. For men all these factors were not significant. Women had better quality of life when living alone whereas for men the β coefficient was negative albeit non-significant. Retirement significantly increased quality of life in men but was not significant for women. On the other hand, longstanding illness reduced quality of life significantly in men but not in women.
DISCUSSION
There was no single key determinant of quality of life; and all the variables in our model were statistically significant. In this sense our quality of life measure, CASP-19, may be interpreted as a summary response to these factors. There are key influences that have a negative impact on quality of life and may be amenable to change or adaptation. These include having a perceived poor financial situation, depression, functional limitations attributable to longstanding illness, and limitations in mobility, activities of daily living, and instrumental activities of daily living. The factors that had positive effect on quality of life included being resident in a neighbourhood perceived to be good, having trusting relationships with children, family, and friends, and affluence as shown by having access to (owning) two or more motor cars.
The study draws strength from addressing the changed nature of old age both demographically and theoretically, from its use of an important new national dataset on aging and its use of a measure of quality of life that is valid and reliable when applied to older age groups.22,23,28,29 The use of CASP-19 allowed us to measure quality of life directly, without relying on proxies such as health status or level of social participation30; hence we were able to distinguish between quality of life and the factors that may influence it. Our data come from a large nationally representative sample of the older population of England,24 which makes our findings directly relevant to policy makers.
What is known on this topic
Aging is perceived to decrease quality of life, but the emergence of a third age demands we look for predictors of quality of life other than age. Many factors are suspected, both positive and negative, but little is known about their relative importance.
What this study adds
No single factor determines quality of life in older ages and there is evidence that quality of life can increase during early old age. Factors like perceived poor financial situation, depression, functional limitation attributable to longstanding illness, and limitations in everyday activities can affect quality of life negatively, while those like residence in an appreciated neighbourhood, having trusting relationships with children, family, and friends, and affluence can improve quality of life.
One limitation to our study is the relatively large proportion of missing data on two self completion questionnaire items: neighbourhood characteristics and quality of life (CASP-19). We have addressed this problem by using multiple imputations that have the advantage of not ignoring observations with incomplete information and, at the same time, reflect the uncertainty of the imputation process.27,31 The results from the complete data and those from the imputed data were similar. A further limitation is the presence of items in the CASP-19 questionnaire that might be related to the explanatory variables. We did sensitivity analyses by calculating summary scores after excluding these items and repeating the regression modelling. There were no substantial changes in the results (not shown).
Our study can be compared directly with two other studies. The first of these used CASP-19 scores to investigate quality of life in a small cohort of British people in early old age (Boyd Orr sample).23 The same factors were identified as important to quality of life, although their relative importance differed somewhat; for example, social networks had a greater impact in the Boyd Orr sample and health status seemed comparatively less important. We found health status, as measured by different variables, a very significant predictor of quality of life. To some extent these differences in emphasis were attributable to the difference in the ages of the two study populations; our results showed that longstanding illness was not significant for 65–74 years old, the age range of Boyd-Orr sample. However, it should be emphasised that the important impact of health status on quality of life was attributable to functional limitations rather than illness itself. CASP-19 was constructed and validated using the small Boyd Orr sample and with this study we were able to show that it behaves as well in larger studies too. This is important as the scale has become popular in many large national surveys in Europe and USA (see appendix 1 for a list, available on line http://www.jech.com/supplemental).
Policy implications
Quality of life at older ages could potentially be high and policies should be directed towards the development of this potential. Such policies would include those increasing confidence in their financial future in older people, those fostering trust in social networks and neighbourhoods, and those reducing the impact of functional limitations. Policies should also take cognisance of increasing proportion of women in older age groups and the importance of their role in informal care has on their quality of life.
Our study’s much larger estimate of the importance of health status agrees with the Berlin aging study, where health status was shown to be a critical influence on subjective wellbeing.12,13 However, because the Berlin aging study used a different measure of health status, it is not possible to make direct comparisons with our findings.
We are reassured by the fact that a national study on lay perceptions on factors contributing to quality of life identified many factors we identify in this study.32 Similarly a large meta-analysis underscores our findings on socioeconomic position and social networks.17 Such evidence can guide central and local government initiatives to direct resources towards ways and means of facilitating friendship ties and community support.
The gradients in quality of life we found in the descriptive analysis are supported by our regression analysis also. The impact of age on quality of life was seen only in the people 75 years or older. We found that if adjusted for all other factors, one would see an improvement in quality of life from 50 to 65 years and it would be only beyond 85 years that quality of life starts to decline. This is compatible with the concept of third age, which in UK started emerging in the middle of the past century.33 The age curve we presented in figure 1 might be the first empirical demonstration of this new period in the life span. Although the wide confidence intervals show large amounts of variation, especially in older ages, the curve shows that potentially the third age could be a period with high quality of life.
Women had significantly higher quality of life than men. A woman’s quality of life was decreased by those factors representing domestic labour: informal care, looking after the home and family, and more frequent contact with children and family; and it was increased by living alone and affluence. For men none of these factors were significant. Some of these differences might be because of the longer life expectancy of women, with the consequently greater chance that when living in a couple the woman will be the carer rather than the man.
Our study found that material circumstances influence quality of life, but the perception of financial inadequacy was more than three times stronger than objective factors like income and number of cars. This might be because of older people’s perception being more complex, for example, by attaching greater importance to their social network than to their financial circumstances.34
In the Duke aging study, how people perceived their retirement was more important than the simple fact of being retired.35 This might explain how in our study, for men and for all at ages above 75+ retirement was a negative influence, while among those in the 50–64 years age group it had a positive impact. This might also be a reflection of financial circumstances: while exit from labour force might mean financial hardship, to retire at younger age groups might signify greater affluence. Indeed, in our sample, the average income of retired 50–64 years old was £12 650 compared with £9840 in 65–74 years old and £7633 in 75+ years old.
Working as a volunteer increased quality of life and it was one of the few significant factors for the oldest group. Volunteerism is an important part of successful aging.36 In the 75+ years old other types of social interaction like frequency of contacts with children, family, and friends were not significant. These findings are in agreement with the theory of socioemotional selectivity37 according to which people develop a strategy to selectively involve in activities that give them most satisfaction, especially when they are aware of the narrow horizon of time they have.
Health variables contributed significantly to quality of life. The strongest relations were for functional limitations attributable to illness and limitations in every day activities. Bur quality of life is not simply reducible to personal circumstances. While income and functional capacity are crucial in determining their quality of life, good neighbourhood environments, valued interaction with friends and family members, as well as, the existence of close confiding relationships can make a difference to a person’s life. Our identification of both positive and negative factors that influence quality of life is important because it relates our findings to the literature on resilience, with its emphasis on both risk and protective factors.38
Acknowledgments
We have benefited from comments by Professor Ann Bowling and an anonymous reviewer on previous versions of this paper.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Funding: this research was funded by ESRC grant L326253061.
-
Competing interests: none declared.
-
Ethical approval: not required.
Linked Articles
- In this issue