Article Text

Abstract
Objective: To present the incidence of Parkinson’s disease (PD) in Norway and to explore gender influences on incidence and age at onset, as well as severity and pattern of parkinsonism at the time of diagnosis in a representative drug naïve cohort with newly diagnosed PD.
Methods: In four Norwegian counties comprising a base population of 1 052 075 inhabitants, multiple sources of case ascertainment and a four step diagnostic procedure were used to establish a representative cohort of patients with incident PD at a high level of diagnostic accuracy. Of a total of 604 subjects referred to the study, 265 individuals fulfilled the clinical research criteria of PD at their latest clinical visit, at a mean 28 months after identification.
Results: The incidence of PD in the study area, age standardised to the 1991 European standard population, was 12.6/105yr-1 (95% CI 11.1 to 14.2). The overall age standardised male to female ratio was 1.58 (95% CI 1.22 to 2.06), with a consistent male preponderance throughout all age groups. Clinical onset of PD was later in women than in men (68.6 vs 66.3 years; p = 0.062) whereas severity and pattern of parkinsonism in drug naïve patients was not different between genders at the time of diagnosis.
Conclusion: Incidence rates of PD in Norway are similar to those in other Western European and American countries. Female gender was associated with a considerably lower risk of PD and slightly delayed motor onset but had no impact on severity of parkinsonism or clinical phenotype in incident drug naïve PD, suggesting that the female gender influences on the nigrostriatal system are most pronounced in the preclinical phase of the disease.
Statistics from Altmetric.com
Although there is increasing awareness that misdiagnosis is common in Parkinson’s disease (PD),1 2 particularly early during the course of the disease,3 most previous incidence estimates are based on patient populations not followed prospectively over time after identification.4 This may influence the accuracy and pattern of incidence figures as well as the validity of associated demographic and clinical results presented.
It has been widely discussed whether and to what extent female gender influences the risk, severity and pattern of PD but studies addressing these issues are inconsistent or not sufficiently confirmed.5–7 This inconsistency may be due to various methodological variations between studies (ie, gender differences in case identification or access to health care in epidemiological studies, retrospective vs prospective assessment of clinical features, or whether the cohorts investigated were population representative or clinic based). In addition, gender differences in the bioavailability of dopaminergic agents have been demonstrated in PD although it is unclear how this may affect the clinical picture.8 Finally, as prevalence of a disease depends both on incidence and mortality, and mortality may differ between genders, incidence is a more accurate estimate of the true frequency and a more direct measure of gender specific risk for a disease.
We have conducted a community based study to estimate the incidence of PD in four counties of Norway using careful diagnostic procedures and standardised assessments as part of a prospective long term study of the incidence, neurobiology and prognosis of PD. Here we present the study design and the observed incidence estimates of PD by age and gender, as well as gender effects on age at onset, motor severity and clinical phenotype at the time of diagnosis in a drug naïve, population based, incident cohort with PD.
METHODS
The Norwegian ParkWest study is a prospective longitudinal cohort study of patients with incident Parkinson’s Disease from Western and Southern Norway. The study area comprises the four counties of Sogn and Fjordane, Hordaland, Rogaland and Aust-Agder, with a total population of more than 1 million inhabitants. The study was approved by the Regional Committee for Medical Research Ethics, University of Bergen. All personnel who were part of the study group received comprehensive training in diagnostic and evaluation procedures before the start of the study and thereafter twice yearly.
Case ascertainment
Patients
We sought to recruit all residents in the study area with incident PD identified during a 22 month period between 1 November 2004 and 31 August 2006. All five neurology units within the study area participated. Patients with suspected incident PD and related parkinsonian disorders in Norway are supposed to be referred to neurologists early after disease onset, according to the Norwegian Medicines Agency’s regulations and guidelines, to initiate antiparkinsonian medication. In a recent nationwide survey, 95.0% of Norwegian patients with PD reported that their disease was managed by a neurologist.9 Nevertheless, in an attempt to achieve total ascertainment of patients with incident PD the following search strategies were applied: (i) hand searching of all referral letters to the participating study centres for symptoms possibly representing incident parkinsonism; (ii) notification of all other hospital departments and all general practitioners, including consulting physicians of nursing homes, geriatric care centres and other institutions for persons of older age, by regular mail before the start of the study and by email reminders twice during the screening period; (iii) cooperation with the only neurologist exclusively working outside the five hospitals within the study area; (iv) electronic screening of hospital databases for patients being diagnosed with PD for the first time during the screening period and for 3 months after to capture delays in coding; and (v) an electronic population screening of 43 716 individuals of all ages, including institutionalised persons, within the largest participating county 6 months after the end of the screening period by one of the authors (BM) by linkage to general practitioners’ electronic medical record systems. Electronic screening comprised search for written terms including each of the four cardinal motor features of the disease, “Parkinson” and “ParkWest”, as well as the International Classification of Diseases system, 10th revision (ICD-10) diagnostic codes for PD (G20), secondary parkinsonism (G21), other degenerative diseases of the basal ganglia (G23), other extrapyramidal and movement disorders (G25) and the International Classification of Primary Care, second edition, electronic version (ICPC-2e) codes for abnormal involuntary movements (N08) and parkinsonism (N87). In addition, general practitioner files and drug prescriptions were searched electronically for antiparkinsonian drugs, including trade names of levodopa, various dopamine agonists, COMT inhibitors and selegiline. Single and combined search terms and diagnostic codes were used. Records dating back to 1 year before the start of the study were considered for screening.
Diagnostic and evaluation procedures
A multiple step diagnostic procedure was applied to identify patients with suspected incident PD. As experience from previous comprehensive epidemiological studies10 11 in the area suggested excellent compliance of general practitioners and other involved sources, we did not perform a run-in period prior to the formal recruitment period.
Screening procedures and initial study diagnosis (step 1)
The screening visit comprised assessment of the patient’s disease history, significant comorbidity, drug history, current medication and a general neurological examination by a study neurologist in all subjects, and the Mini-Mental State Examination12 when cognitive impairment was suspected. All subjects who consented to long term study participation and met the broad provisional criteria for incident PD, defined as the unequivocal presence of at least two of the four cardinal motor signs, typical disease history with evidence of progressive parkinsonism, no dementia at the onset of parkinsonism and no severe atypical signs (severe postural instability or frequent falls; prominent autonomic, pyramidal, cerebellar features or eye movement disorders), were directly forwarded to more comprehensive baseline assessments (step 2, see below). In cases in which a diagnosis of PD was difficult to determine at the screening visit because of multiple potential underlying causes (“uncertain PD”), reassessments were conducted before study entry. In addition, [123I]FP-CIT dopamine transporter imaging was available to aid in the differential diagnosis. Patients with an initial study diagnosis of PD refusing full study participation were offered routine neurological follow-up by a study neurologist. No attempt was made to systematically follow subjects who presented features definitely excluding PD, such as pre-existing dementia, or those who were free from parkinsonism. However, these and all other subjects with non-PD parkinsonism in need of a diagnostic work-up or neurological care were offered to be followed at the participating departments. In addition, general practitioners were asked to re-refer subjects if they developed a clinical picture suspicious of PD.
Baseline assessments (step 2)
Baseline investigations were conducted during two consecutive days in the presence of a caregiver, including semi-structured interviews on medical and drug history, and family history of neurological and psychiatric diseases, as well as a general neurological and medical examination.
The severity of parkinsonism and disability was assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS),13 including the modified Hoehn and Yahr staging14 and the Schwab and England scale.15 Cognitive functioning was assessed using the Mini-Mental State Examination and an extensive neuropsychological test battery, and the Informant Questionnaire for Cognitive Decline in the Elderly,16 validated for the diagnosis of dementia, was completed by the caregiver. Patients and relatives were asked if dementia had developed before, simultaneously with or within 12 months of onset of motor symptoms. Cerebral MRI scans with volume uptake were performed in close temporal relation to the baseline examinations.
Follow-up (step 3)
Patients who consented to study participation were undergoing prospective follow-up, including clinical evaluation by a study neurologist at least twice yearly. Biannual assessments comprised semi-structured interviews and standardised rating scales, including the UPDRS to evaluate changes in drug therapy, subjective and objective response to dopaminergic treatment, and development of features atypical of PD.
Final study diagnosis (step 4)
At a mean time of 28 months from the screening visit, all patients originally evaluated for the study were provided with a final study diagnosis of PD according to widely acknowledged criteria17 under the supervision of two neurologists, specialising in movement disorders (GA and JPL), taking into consideration all available patient material through to the latest study visit, including medical history, clinical and radiological examination, drug response in those on dopaminergic treatment and dopamine transporter imaging when available (n = 31). Patients who developed dementia before or within 1 year of motor onset were excluded. When not meeting the diagnostic criteria for PD, subjects were provided with a diagnosis of other parkinsonian syndromes, based on (i) the revised consensus criteria for the diagnosis of dementia with Lewy bodies (DLB),18 (ii) the consensus statement on the diagnosis of multiple system atrophy,19 (iii) National Institute of Neurological Disorders and the Society for Progressive Supranuclear Palsy clinical research criteria,20 (iv) a history of repeated stroke and/or (related) stepwise progression of parkinsonism and compatible neuroradiological findings regarding a diagnosis of “vascular parkinsonism” and (v) development of parkinsonism, preferably symmetric, in temporal relation to exposure to neuroleptics or other drugs with antagonistic properties to dopamine receptors for a diagnosis of “drug induced parkinsonism”. Diagnostic and Statistical Manual of Mental disorders, fourth edition (DSM-IV-TR) criteria were used to provide a diagnosis of Alzheimer’s disease.21 A diagnosis of monosymptomatic resting tremor was based on the Consensus Statement of the Movement Disorder Society on Tremor.22 Essential tremor was diagnosed when patients presented with predominant postural tremor of moderate amplitude, located in the upper limbs or head, with no signs of parkinsonism and not caused by medication, alcohol or hyperthyroidism.
Data analysis
Details on overall population size and age and sex distribution in the study area were obtained from Statistics Norway, which annually updates and publishes information on various demographic data for the Norwegian population. On 1 January 2005, the overall population size within the four counties covered by the participating study sites was 1 052 075. Crude incidence estimates and age and sex specific incidence rates were calculated and presented with 95% confidence intervals (CIs), assuming Poisson distribution. To account for some persons in the general population having prevalent PD, the number of cases with prevalent PD was estimated using information from a previous community based prevalence study10 conducted in parts of the study area, and subtracted from the population denominator in supplemental analyses. Furthermore, incidence figures and corresponding male to female ratios, age standardised to the 1991 standard European population, were calculated.
Disease severity is provided as the means of the UPDRS activities of daily living and motor subscores, and means and medians of the Hoehn and Yahr and Schwab and England scales. Mean scores for the motor domains tremor, ridigity, bradykinesia, as well as axial impairment were calculated to assess the pattern of parkinsonism, as described previously.23 Differences in proportions were analysed by χ2 tests. Student t tests or Mann–Whitney tests were used as appropriate. A p value <0.05 was considered statistically significant. SPSS 14.0 and R 2.6.1 were used for statistical analyses.
RESULTS
Patient recruitment
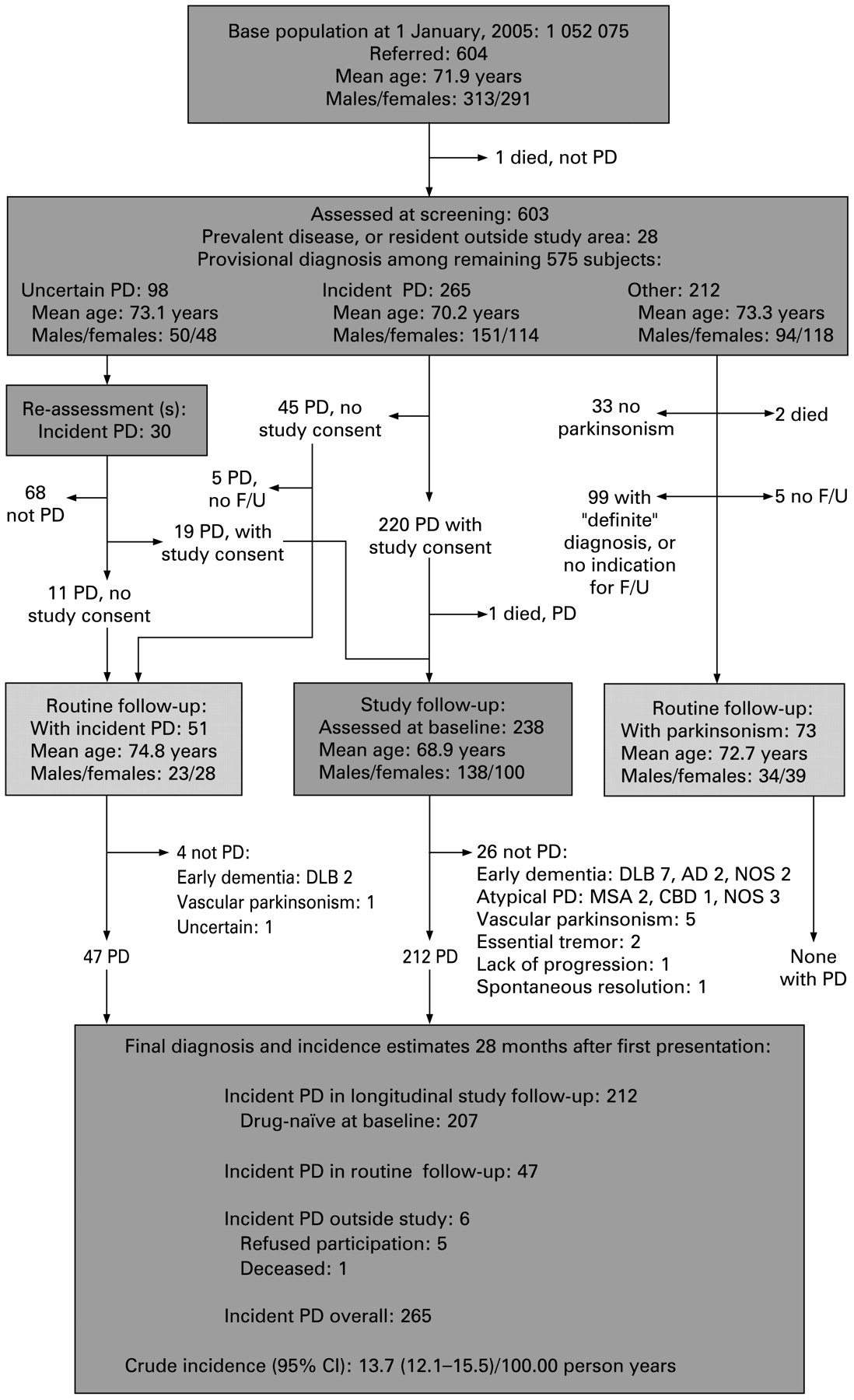
A flowchart for the screening and diagnostic procedures is shown in fig 1. A total of 604 subjects, 49 (8.1%) of whom were nursing home residents, were referred to the study from various sources or identified through screening of hospital files (table 1). No additional cases were identified by electronic screening of a subgroup of the general population. One patient referred to the study died before screening. Review of general practitioner and hospital files revealed that this subject had established dementia before the onset of parkinsonism. The remaining 603 patients were evaluated clinically during the 22 month inclusion period by a study neurologist.

{kind=link}
Flowchart illustrating the demographic characteristics and flow of 604 subjects through the screening and evaluation procedures. Broad clinical inclusion criteria were used to identify subjects with potential Parkinson’s disease (PD). Incidence estimates were calculated on average 28 months after the first clinical presentation in patients who were followed prospectively over time and fulfilled the clinical research criteria of PD at their latest visit. AD, Alzheimer’s disease; CBD, corticobasal degeneration; DLB, dementia with Lewy bodies; F/U, follow-up; MSA, multiple system atrophy; NOS, not specified.
Differential diagnoses
Twenty-seven of the 603 patients screened had prevalent disease and one patient was resident outside the study area. The final diagnoses among the remaining 575 incident cases at the latest study visit are presented in table 2.
A total of 265 patients, all Caucasians, fulfilled the diagnostic criteria of PD at their latest study visit. Mean (SD) age at motor onset was 66.3 (9.7) years for men, 68.6 (9.8) years for women (p = 0.062) and 67.3 (9.8) years overall. Mean (SD) age at diagnosis was 68.6 (9.6) years for males and 70.4 (9.8) years for females. Thirty subjects (10.2%) with an initial study diagnosis of PD were re-diagnosed during follow-up. In these, the initial study diagnosis of PD most frequently changed to DLB (nine subjects, 30%) and vascular parkinsonism (five subjects, 16.7%). Patients who were re-diagnosed during follow-up were older (mean age 75.6 years, p = 0.001) than those who remained in the study.
Incidence of PD
Age and sex specific crude incidence estimates and male to female ratios for incident PD are presented in table 3. No significant differences in incidence figures were found when the estimated number of patients with prevalent PD among the general population was subtracted from the population denominator (data not shown). When adjusted to the 1991 European population age structure, the annual incidence rate of PD was 12.6/105yr-1 (95% confidence interval 11.1 to 14.2) overall, 15.6/105yr-1 (13.2 to 18.3) in men and 9.9/105yr-1 (8.0 to 12.0) in women. The corresponding age standardised male to female ratio of incident PD was 1.58 (1.22 to 2.06).
Patient characteristics
Of the 265 patients fulfilling the research criteria for PD at their latest study visit, 212 (80.0%) had agreed to take part in a longitudinal study follow-up and participated in standardised baseline examinations. Time from motor onset to baseline assessments was not different between genders or subjects who were directly forwarded from screening to baseline examinations and those who underwent reassessments before inclusion (2.3 years vs 2.6 years; p = 0.131). A total of 207 of 212 patients had never been exposed to antiparkinson drugs at the time of their first presentation (n = 201) or had withdrawn antiparkinsonian medication at least 2 weeks before baseline examinations (n = 6). Clinical and demographic characteristics of the 207 patients according to gender are presented in table 4.
DISCUSSION
This study is the first to estimate the incidence of PD in Norway, and the first to provide incidence estimates of PD after prospective follow-up of an incipient cohort with parkinsonism. Our study fulfils recent recommendations for high quality large scale incidence studies in PD.4 The strengths of our study design are: (i) the large and representative cohort of incident patients with PD within a large and stable base population, (ii) the involvement of multiple sources of identification to achieve total case ascertainment, (iii) the assessment of all subjects by trained neurologists with an interest in movement disorders, (iv) the application of careful and standardised diagnostic procedures and (v) prospective follow-up to minimise false positive and false negative diagnoses. Furthermore, unlike previous incidence studies, virtually all subjects included were assessed drug naïve at their first presentation, eliminating a potential bias of dopaminergic medication on disease state. This made differential diagnosis less complicated, as responsiveness to dopaminergic drugs was assessed prospectively and guided the interpretation of features atypical of early untreated PD, such as visual hallucinations, indicating DLB. Therefore, we are convinced that diagnostic accuracy in our cohort was as high as possible. Nevertheless, all patients will be asked for post-mortem brain donation.
In a study area covering nearly a quarter of the total Norwegian population, we found the annual incidence rate to be 12.6 per 100 000 inhabitants, age adjusted to the 1991 European population structure. Although this figure is within the range of those for other community based Western European and American studies using comparable diagnostic criteria,24–28 we are aware that it may be an underestimate. Complete case identification is difficult to achieve in large base populations such as ours, where direct screening of all residents in the study area is impossible. However, the fact that no additional cases were identified by electronic screening of a subpopulation at least indicates that the other methods of case ascertainment in our study were successful. PD may be under-recognised among the elderly in whom clinical cardinal features of the disease may be interpreted as “normal” aging related signs. This is supported by higher incidence rates observed in studies that were dedicated to screening for PD among the elderly.29–32 Furthermore, use of strict diagnostic criteria may lead to erroneous exclusion of PD subjects in whom apparent atypical features relate to medical comorbidity rather than the disease itself.3 Retrospective autopsy studies show that about 10% of patients with pathologically proven PD do not fulfil acknowledged clinical diagnostic criteria,33 indicating that the clinical spectre of PD is broader than covered by these criteria.
On the other hand, overdiagnosis of PD using broad criteria may be substantial, particularly among the elderly, and when the incipient cohort is not followed-up over time. In our cohort, approximately 20% of patients aged 80 years or more with an initial study diagnosis of PD did not fulfil the diagnostic criteria of the disease at their last clinical visit. The corresponding revision figure for the overall sample was 10%. This is similar to a recent 29 month observational longitudinal study of an incident cohort with parkinsonism where the proportion of patients diagnosed with PD decreased by 14% during follow-up.3 In both that and our study, DLB was the most frequent reason for re-diagnosis, which confirms previous clinicopathological studies reporting DLB to be severely under recognised. DLB typically affects patients of older age34—in our cohort, 80% of DLB cases were 70 years or older—and thus misdiagnosis of DLB and other atypical parkinsonian disorders as PD cause overestimation of PD incidence, particularly in the oldest age groups. This may complicate the interpretation of incidence estimates for studies conducted before DLB became recognised as a distinct entity, and for studies without cognitive assessment and follow-up of the incipient cohort.
Gender differences in relation to the risk of developing PD have been studied previously, most studies reporting higher incidence rates in men. However, evidence is conflicting.5 Neuroprotective properties of female steroid hormones, or alternatively gender differences in exposure to environmental and occupational risk factors or gender specific genetic influences, have been discussed as possible underlying causes.5 35 In our sample, we found the age standardised incidence of PD to be 58% higher in men than women. This figure is nearly identical to that of a recently published meta-analysis, reporting a pooled estimate for an age standardised male to female ratio of 1.57 in Western populations but no gender differences in several Asian populations.5 However, while previous studies reported varying results on the extent of gender differences in incidence of PD in patients aged less than 60 years at disease onset,5 we observed a robust male preponderance even in the youngest age groups. This finding coupled with previous observations of no gender differences of PD in Asian populations suggests that the observed lower risk for PD associated with female gender at least in part is due to gender specific genetic influences as oestrogen related effects on PD risk should be observable across different ethnic populations.
Our observation of a slightly later motor onset in women than in men is in agreement with most previous incidence studies,4 and compatible with the concept of female gender being associated with neuroprotective effects. On the other hand, we found no gender differences in drug naïve subjects at the time of diagnosis in terms of severity and pattern of clinical motor features thought to relate to nigrostriatal damage. This finding extends that of a recent longitudinal clinic based SPECT study demonstrating equal deterioration rates in striatal [123I]FP-CIT binding and motor severity in men and women with PD.7 This suggests that female gender has no profound effect on the nigrostriatal system when PD has become clinically overt, not even in the early disease stages. Potential explanations are that the beneficial effects of oestrogen and possibly other determinants are diminished or lost when nigrostriatal neurons become damaged as a result of the underlying neurodegenerative process36 37 or that the lower risk of PD and delay in motor onset in women may be due to physiologically higher levels of striatal dopamine at similar rates of dopamine depletion in both genders.7 38 If the latter were true, however, one would expect the incidence of PD in women to converge with that of men in the older age groups, which is certainly not evident in our cohort or most other prospective incidence studies in PD.24 27 29–32
In summary, using multiple sources of case identification and careful diagnostic procedures, we found the incidence rate of PD in Norway to be in the range of estimates from other Western European and American countries. Our study demonstrates that female gender is associated with a considerably lower risk and slightly delayed clinical onset of PD but does not affect motor severity or pattern of clinical cardinal symptoms in drug naïve subjects at the time of diagnosis. Our findings suggest that the potential neuroprotective effects of female gender on the nigrostriatal system are limited to or most pronounced in the preclinical phase of PD. However, potential neuroprotective properties associated with female gender may affect various non-motor features of the disease, may be more prominent for certain subgroups of female PD patients or become more prominent later during the course of the disease.39 Prospective follow-up of our incident cohort may contribute to further elucidate these important issues.
Acknowledgments
The authors are grateful to the patients for their willingness to participate in this study. We thank Kolbjørn Brønnick and Odd Bjarte Nilsen for help with statistical analyses and management of databases, Magne Rekdal for assistance with conducting the electronic population screening and Karen Simonsen for expert technical support.
Appendix
This study is the result of a joint initiative from the Departments of Neurology, Haukeland University Hospital, Bergen, and Stavanger University Hospital, Stavanger, Norway. The study is coordinated by the Norwegian Centre for Movement Disorders. The Norwegian ParkWest study group consists of: study neurologists: Guido Alves, Elin Bjelland Forsaa, Michaela Dreetz Gjerstad, Karen Herlofson, Ineke HogenEsch, Jan Petter Larsen, Bernd Müller, Kenn Freddy Pedersen, Geir Olve Skeie, Wenche Telstad, Ole-Bjørn Tysnes, Corinna Vossius; study nurses: Britt Bruland, Siri Bruun, Marit Ellefseth, Liv Kari Haaland, Jane Kastet, Marianne Kjærandsen, Anita Laugaland, Ingrid Leiknes, Kirsten Lode, Kristina Rasmussen, Marit Arnevik Renså, Gro Tønnesen.
REFERENCES
Footnotes
↵* Details of the Norwegian ParkWest study group can be found in the appendix.
Funding: The Norwegian ParkWest study was funded by the Western Norway Regional Health Authority (grant No 911218) and the Research Council of Norway (grant No 177966).
Competing interests: None.
Ethics approval: The study was approved by the Regional Committee for Medical and Health Research Ethics, Western-Norway, University of Bergen, Bergen, Norway.