


Abstract
Background: Resting heart rate is linked to risk of coronary artery disease, stroke, sudden death and noncardiovascular diseases. We conducted a meta-analysis to assess these associations in general populations and in populations of patients with hypertension or diabetes mellitus.
Methods: We searched PubMed, Embase and MEDLINE from inception to Mar. 5, 2016. We used a random-effects model to combine study-specific relative risks (RRs). We used restricted cubic splines to assess the dose–response relation.
Results: We included 45 nonrandomized prospective cohort studies in the meta-analysis. The multivariable adjusted RR with an increment of 10 beats/min in resting heart rate was 1.12 (95% confidence interval [CI] 1.09–1.14) for coronary artery disease, 1.05 (95% CI 1.01–1.08) for stroke, 1.12 (95% CI 1.02–1.24) for sudden death, 1.16 (95% CI 1.12–1.21) for noncardiovascular diseases, 1.09 (95% CI 1.06–1.12) for all types of cancer and 1.25 (95% CI 1.17–1.34) for noncardiovascular diseases excluding cancer. All of these relations were linear. In an analysis by category of resting heart rate (< 60 [reference], 60–70, 70–80 and > 80 beats/min), the RRs were 0.99 (95% CI 0.93–1.04), 1.08 (95% CI 1.01–1.16) and 1.30 (95% CI 1.19–1.43), respectively, for coronary artery disease; 1.08 (95% CI 0.98–1.19), 1.11 (95% CI 0.98–1.25) and 1.08 (95% CI 0.93–1.25), respectively, for stroke; and 1.17 (95% CI 0.94–1.46), 1.31 (95% CI 1.12–1.54) and 1.57 (95% CI 1.39–1.77), respectively, for noncardiovascular diseases. After excluding studies involving patients with hypertension or diabetes, we obtained similar results for coronary artery disease, stroke and noncardiovascular diseases, but found no association with sudden death.
Interpretation: Resting heart rate was an independent predictor of coronary artery disease, stroke, sudden death and noncardiovascular diseases over all of the studies combined. When the analysis included only studies concerning general populations, resting heart rate was not associated with sudden death.
Heart rate reflects the balance of sympathetic and parasympathetic activity, and is influenced by several nonmodifiable and modifiable factors.1 High natural resting heart rate is associated with traditional risk factors for cardiovascular diseases, levels of inflammatory markers2–4 and functional decline,5 which suggests that resting heart rate might be related to the risk of various disease states. We previously found that resting heart rate was an independent predictor of total mortality related to cardiovascular disease in the general population.6 However, the predictive values of resting heart rate for cardiovascular-specific outcomes, including coronary artery disease, stroke and sudden death, as well as noncardiovascular diseases, have not been quantified in the general population. Although the potential importance of resting heart rate has been recognized,7 it has not been included for cardiovascular risk assessment in European and US guidelines7,8 because the benefit of a reduction in resting heart rate for noncardiac patients is unknown. In addition, the magnitude of associations between resting heart rate and the abovementioned outcomes varies across studies, and the optimal resting heart rate can be expected to differ with disease state.9 Therefore, we conducted a meta-analysis of prospective cohort studies, in accordance with the PRISMA checklist (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC1), to quantitatively assess these associations in general populations and in populations of patients with hypertension and diabetes mellitus.
Methods
Literature search and study selection
Two investigators (D.Z., W.W.) identified articles independently through a systematic search of PubMed, Embase and MEDLINE from inception to Mar. 5, 2016, and by searching the reference lists of selected articles. The search was restricted to studies involving humans and published in English or Chinese. Details of the search strategy and results are presented in Appendix 2 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC1). There was no protocol for this meta-analysis.
Two investigators (D.Z., F.L.) independently selected studies using the following criteria: the participants were from the general population or were patients with hypertension or diabetes (excluding studies in cardiac patients); the exposure of interest was resting heart rate; the outcome of interest was coronary artery disease, stroke, sudden death, noncardiovascular diseases, all types of cancer or noncardiovascular diseases excluding cancer; the study reported relative risks (RRs) or hazard ratios with 95% confidence intervals (CIs), with all current results being presented as RRs; and the study had a prospective cohort design. If the same data were reported in more than one study, we included the study with the longest follow-up duration.
Data extraction
Two investigators (W.W., F.L.) independently extracted the following data using a standardized data collection form: first author’s name, year of publication, country where the study was conducted, duration of follow-up, participants’ age, sample size, sex, number of events, method of measuring resting heart rate, adjusted covariables, health status of participants at baseline and RR (with 95% CI) for each category of resting heart rate. We extracted the RRs that reflected the most inclusive but significant adjustment for potential confounders.
Statistical analysis
Detailed information about the analysis is available in our previous paper.6 In brief, we combined study-specific logarithms of RRs for an increment of 10 beats/min in resting heart rate using a random-effects model. We used the I2 statistic to evaluate between-study heterogeneity. We conducted subgroup analyses and meta-regression to explore potential sources of heterogeneity and to perform comparisons between groups. We performed a sensitivity analysis and evaluated publication bias. We assessed study quality using the 9-star Newcastle–Ottawa Scale (www.ohri.ca/programs/clinical_epidemiology/oxford.asp).
We also conducted a 2-stage random-effects dose–response meta-analysis.10 Where cases were missing from a given category, we inferred the data from the total numbers of cases and the reported risk estimates.11 In separate analyses, according to the threshold level of resting heart rate in the general population (80–85 beats/min)12 and the cut-offs used in the included studies, we combined the resting heart rate categories into 4 groups: reference (lowest category in each study, i.e., < 60 beats/min), 60–70, 70–80 and > 80 beats/min. We did not conduct this analysis for sudden death, all cancers or noncardiovascular diseases excluding cancer because of the relatively small number of studies. All statistical analyses were performed with STATA version 12.0. All reported probabilities (p values) were 2-sided, with p < 0.05 considered significant.
Results
Literature search and study characteristics
After exclusion of nonrelevant and duplicate articles, 523 records were reviewed in full. Another 478 records were excluded for other reasons (Appendix 2), and 45 prospective cohort studies were included in this meta-analysis. Of the 45 studies (38 studies in general populations and 7 studies in populations of patients with hypertension or diabetes), 30 provided results for coronary artery disease (1 227 511 participants and 18 364 cases), 17 provided results for stroke (1 002 667 participants and 11 515 cases), 12 provided results for noncardiovascular diseases (443 192 participants and 12 749 cases), 10 provided results for all types of cancer (115 388 participants and 5714 cases), 7 provided results for noncardiovascular diseases excluding cancer (81 332 participants and 2174 cases), and 7 provided results for sudden death (426 332 participants and 563 deaths). The follow-up duration ranged from 2 to 40 years. The study quality ranged from 5 to 9 stars (Appendix 3, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC1). Detailed information about the included studies appears in Appendix 4 (available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC1).
Quantitative synthesis
Cardiovascular-specific diseases
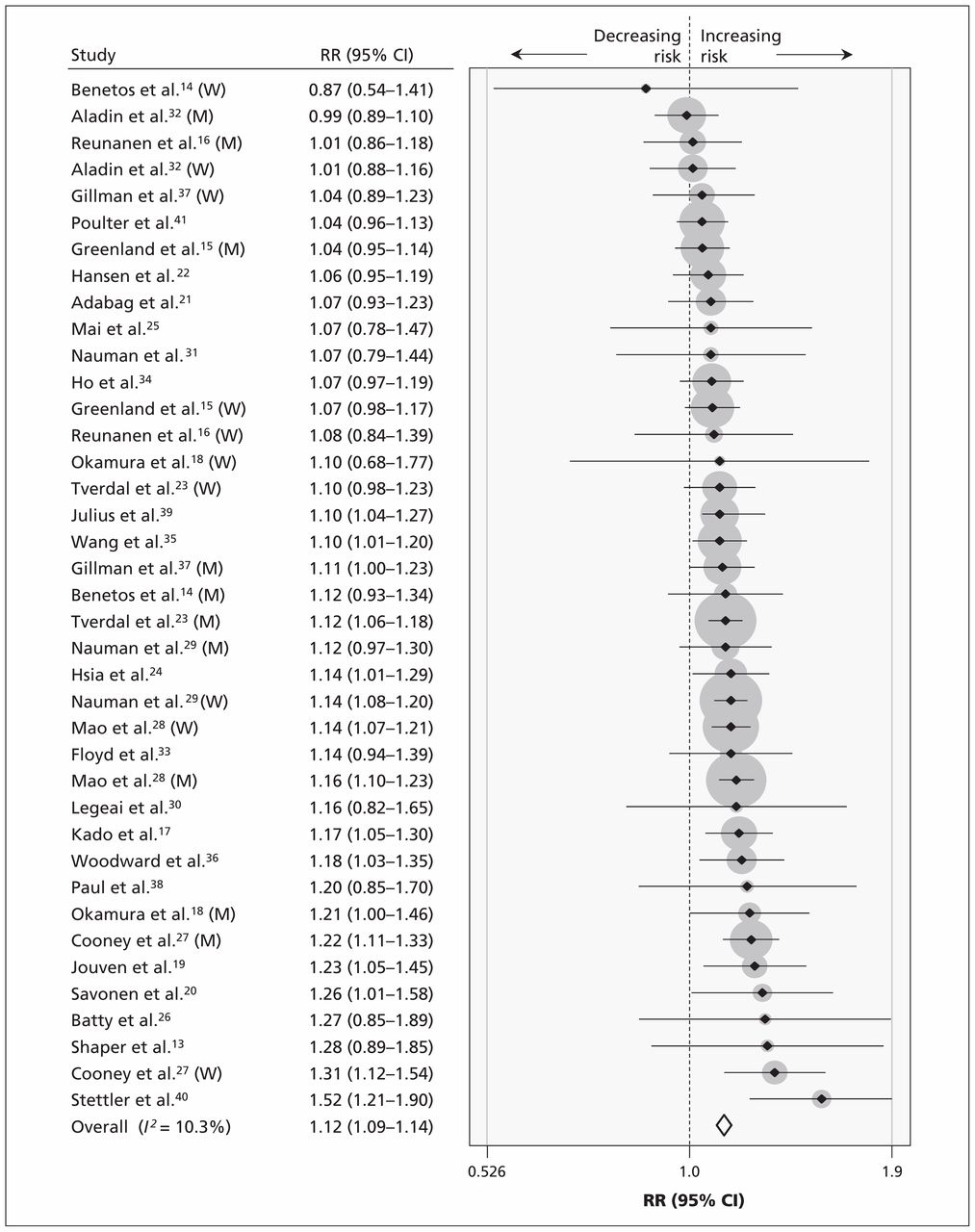
The multivariable-adjusted RR for coronary artery disease with every increment in resting heart rate of 10 beats/min was 1.12 (95% CI 1.09–1.14; I2 = 10.3%; Figure 113–41). There was no evidence of publication bias (p = 0.8). Relative to those with resting heart rate below 60 beats/min, the RR for coronary artery disease was 0.99 (95% CI 0.93–1.04) for those with resting heart rate of 60–70 beats/min, 1.08 (95% CI 1.01–1.16) for those with resting heart rate of 70–80 beats/min and 1.30 (95% CI 1.19–1.43) for those with resting heart rate above 80 beats/min (Table 1).
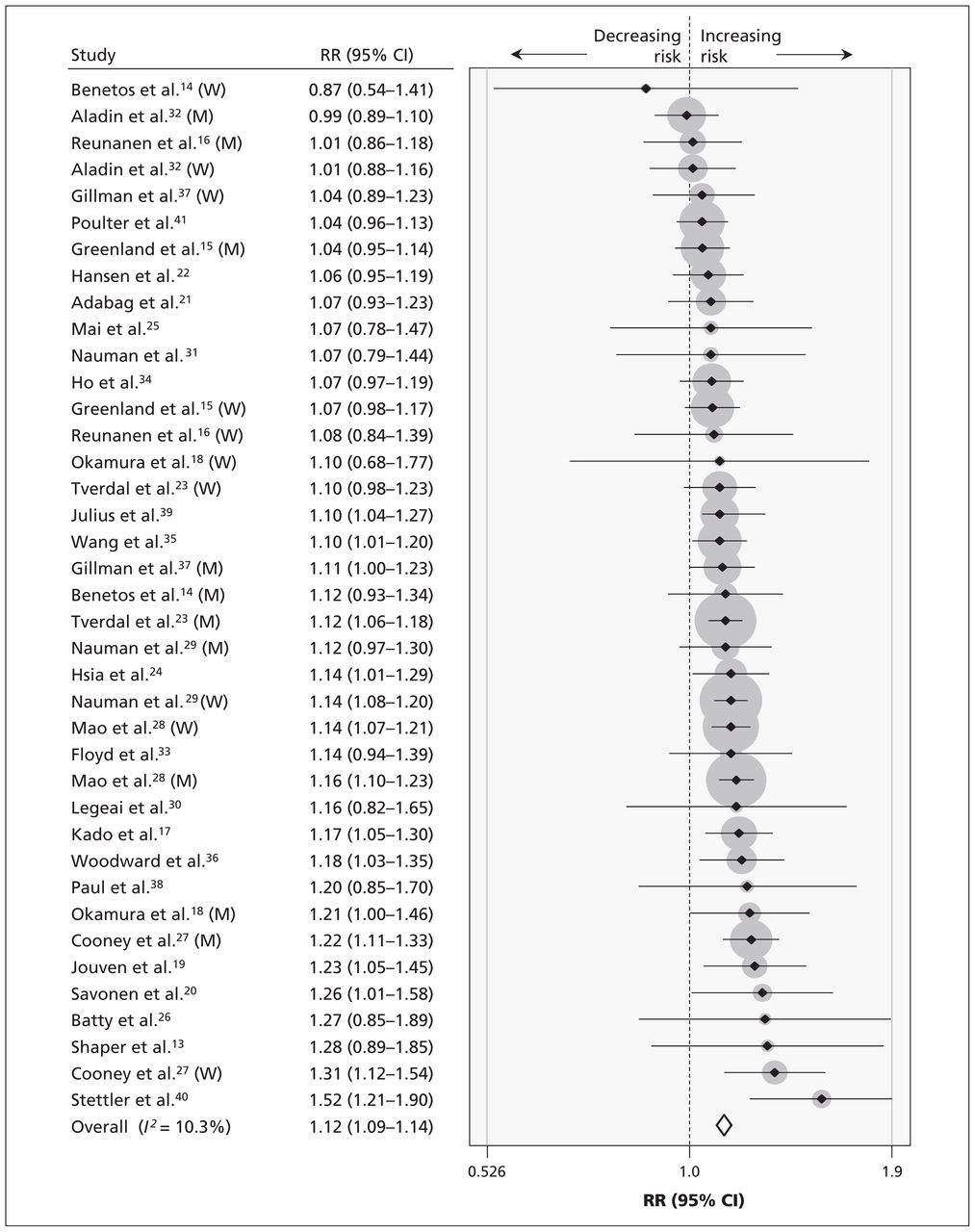
Forest plot of each increment in resting heart rate of 10 beats/min in relation to risk of coronary artery disease. The size of each grey circle is proportional to the weight assigned to that study. Covariable-adjusted risk estimates were used because the raw numbers were not provided in the original studies. Note: CI = confidence interval, M = men, RR = relative risk, W = women.
Pooled results for risk of coronary artery disease, by resting heart rate (reference: < 60 beats/min)
The multivariable-adjusted RR of stroke with every increment in resting heart rate of 10 beats/min was 1.05 (95% CI 1.01–1.08; I2 = 48.6%) (Table 2). There was no evidence of publication bias (p = 0.9). Relative to those with resting heart rate below 60 beats/min, the RR for stroke was 1.08 (95% CI 0.98–1.19) for those with resting heart rate of 60–70 beats/min, 1.11 (95% CI 0.98–1.25) for those with resting heart rate of 70–80 beats/min and 1.08 (95% CI 0.93–1.25) for those with resting heart rate above 80 beats/min.
Pooled risk of stroke, noncardiovascular diseases, all types of cancer and noncardiovascular diseases excluding cancer with increment of 10 beats/min in resting heart rate*
The multivariable-adjusted RR of sudden death with every increment in resting heart rate of 10 beats/min was 1.12 (95% CI 1.02–1.24; I2 = 50.3%; n = 8). There was no evidence of publication bias (p = 0.7).
Noncardiovascular diseases
The multivariable-adjusted RR for noncardiovascular diseases with every increment in resting heart rate of 10 beats/min was 1.16 (95% CI 1.12–1.21; I2 = 64.9%; Figure 214,22,23,30,42–48). There was some evidence of publication bias (p = 0.05). Relative to those with resting heart rate below 60 beats/min, the RR for noncardiovascular diseases was 1.17 (95% CI 0.94–1.46) for those with resting heart rate of 60–70 beats/min, 1.31 (95% CI 1.12–1.54) for those with resting heart rate of 70–80 beats/min and 1.57 (95% CI 1.39–1.77) for those with resting heart rate above 80 beats/min.

Forest plot of each increment in resting heart rate of 10 beats/min in relation to risk of noncardiovascular diseases. The size of each grey circle is proportional to the weight assigned to that study. Covariable-adjusted risk estimates were used because the raw numbers were not provided in the original studies. Note: CI = confidence interval, M = men, RR = relative risk, W = women.
The multivariable-adjusted RR for all types of cancer with every increment in resting heart rate of 10 beats/min was 1.09 (95% CI 1.06–1.12; I2 = 0.00%) (Table 2). There was no evidence of publication bias (p = 0.4).
The multivariable-adjusted RR for noncardiovascular diseases excluding cancer with every increment in resting heart rate of 10 beats/min was 1.25 (95% CI 1.17–1.34; I2 = 67.7%) (Table 2). There was no evidence of publication bias (p = 0.4).
Sensitivity analysis, subgroup analysis and meta-regression
No individual study had an excessive influence on the pooled effect in a sensitivity analysis. We assessed confounding by the following 8 traditional risk factors for cardiovascular diseases: blood pressure, smoking, body mass index, physical activity, serum cholesterol or triglycerides, diabetes or blood glucose level, alcohol use, and education or social class, all of which are correlated with heart rate.2 Overall, meta-regression and subgroup analysis showed that these traditional risk factors for cardiovascular diseases, the methods of measuring heart rate and the population characteristics did not contribute significantly to heterogeneity in most of the analyses (Appendix 5, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC1). Similar results were obtained in a sensitivity analysis that excluded studies involving patients with hypertension or diabetes, but no association was found with sudden death.
In particular, to exclude the potential influence of heart rate–lowering medications and disease states on the associations, we performed a sensitivity analysis that included only participants without cardiovascular disease at baseline. In this sensitivity analysis, the multivariable-adjusted RR with every increment in resting heart rate of 10 beats/min was 1.12 (95% CI 1.10–1.15) for coronary artery disease, 1.05 (95% CI 1.00–1.10) for stroke, 1.16 (95% CI 1.10–1.22) for noncardiovascular diseases, 1.07 (95% CI 1.02–1.11) for all types of cancer and 1.23 (95% CI 1.13–1.35) for noncardiovascular diseases excluding cancer.
Dose–response analysis with restricted cubic spline functions
The departure from a linear relation with resting heart rate was not significant for risk of coronary artery disease (15 studies,13,14,16,21,23,24,26,28–32,35,36,49 p for nonlinearity = 0.05, Figure 3A), stroke (10 studies,14,16,23,24,26,28,35,36,50,51 p for nonlinearity > 0.9), noncardiovascular diseases (8 studies, 14,23,30,42–45,49 p for nonlinearity = 0.2, Figure 3B), cancer (6 studies,16,26,42,45,52,53 p for nonlinearity = 0.9), noncardiovascular diseases excluding cancer (3 studies,16,18,42 p for nonlinearity = 0.4) and sudden death (3 studies,13,21,23 p for nonlinearity = 0.6). When we used the lowest value in the included studies (49 beats/min) as the reference level, the risk of noncardiovascular diseases and of all types of cancer increased significantly with increasing levels of resting heart rate in a linear relation, but a significantly increased risk of coronary artery disease was observed at about 80 beats/min (Appendix 6, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC1).

Dose–response analysis of resting heart rate with risk of (A) coronary artery disease and (B) noncardiovascular diseases. The solid line and the long-dash lines represent the estimated relative risk (RR) and its 95% confidence interval (CI), respectively. The short-dash line represents the linear relation.
Interpretation
The multivariable-adjusted risk of coronary artery disease, stroke, sudden death, noncardiovascular diseases, all types of cancer and noncardiovascular diseases excluding cancer increased significantly, by 12%, 5%, 12%, 16%, 9% and 25%, respectively, with every 10 beats/min increment in resting heart rate. The departure from a linear relation between resting heart rate and each of these end points was not significant.
These results may occur by various mechanisms. High resting heart rate could increase hemodynamic stress and shorten the diastolic phase, which could then increase mechanical load, tensile stress, low and oscillatory shear stress, blood pressure and cardiac work, thereby increasing oxygen consumption; these direct detrimental effects could cause coronary atherosclerosis and myocardial ischemia.2,9,54
High resting heart rate is a marker of sympathetic overactivity, which is associated with an increased risk of sudden death that usually results from ventricular fibrillation.55 Ischemic episodes are more likely to trigger serious arrhythmias in the context of high heart rate, and the beneficial effect of β-blockade on ventricular fibrillation may be mediated primarily by heart rate reduction.9 In addition, coronary lesions are present in most cases of sudden death in adults.56 Sympathetic overactivity may confer an increased risk of obesity that could induce insulin resistance, higher levels of uric acid, lipid abnormalities and hypertension.2 Therefore, these adverse events associated with sympathetic overactivity may account for the observed association between high heart rate and noncardiovascular diseases. High heart rate might be a marker of chronic stress and anxiety that may be related to an increase in the risk of cancer.45 In addition, common elements such as growth factors may be associated with hemodynamic parameters and the evolution of cancer.57
Although it seems desirable to maintain resting heart rate substantially below the traditionally defined tachycardia threshold of 90 or 100 beats/min,9 the results of this meta-analysis show that the desirable resting heart rate differs with the end point of interest. Compared with 70 beats/min, a linear dose–response analysis indicated a significantly protective effect of lower resting heart rates on the risk of all-cause mortality in general populations in our previous study.6 The results of the current meta-analysis showed that, compared with 70 beats/min, lower resting heart rate was also associated with a significantly decreased risk of mortality from noncardiovascular diseases. These findings indicate the possibility that “the slower the heart rate, the better”58 for all-cause mortality and mortality from noncardiovascular diseases in general populations.
We observed a significantly increased risk of total cardiovascular mortality at 90 beats/min in the previous meta-analysis.6 However, the current meta-analysis indicated that the association with stroke was weak, whereas resting heart rate had a significant positive association with coronary artery disease above a threshold value of about 80 beats/min (Appendix 6). At a resting heart rate above 60 beats/min, a linear association was observed between resting heart rate and heart failure, with an overall hazard ratio of 1.13 (95% CI 1.07–1.18, per 10 beats/min increment).59 In addition to the various end points, demographic and measurement factors should also be taken into account when considering a desirable or optimal resting heart rate.9
Limitations
This study has some limitations. First, night-time heart rate has better prognostic value than resting heart rate in a population with no apparent heart disease3 and in people with hypertension.60 In addition, ambulatory heart rate might have better predictive power than clinic-based resting heart rate; however, there was a high degree of correlation between these 2 measurements, and ambulatory heart rate did not add prognostic information beyond that provided by clinic heart rate.47 Although resting heart rate may change over time, a single measurement of resting heart rate was found to be as strong a predictor of cardiovascular outcomes as repeated measurements over the course of 8 years.34
The number of covariables and the extent to which the potential confounders were adjusted for varied across studies; as such, collaborative pooling of individual participant data would be a better way to explore the relations. Third, as shown in Appendix 4, some studies did not exclude participants with prevalent cardiovascular diseases and noncardiovascular diseases. As such, we were not studying the incidence of disease. However, we obtained similar cardiovascular-specific results after excluding participants with cardiovascular diseases at baseline.
Because of the small sample size, no association with heart failure was found in the sensitivity analysis. In addition, a positive association was detected in 2 studies61,62 in general populations that did not meet the criteria for inclusion in this meta-analysis.
Conclusion
Resting heart rate was an independent predictor of coronary artery disease, stroke, sudden death and noncardiovascular diseases over all of the studies combined. When the analysis included only studies concerning general populations, resting heart rate was not associated with sudden death. Further studies are warranted to confirm the findings in patients with hypertension or diabetes (because of the importance of reducing heart rate in these patients) and to explore the association between resting heart rate and sudden death, specific types of cancer and other specific outcomes of noncardiovascular diseases.
Routinely measured resting heart rate is worth considering in risk prediction algorithms for coronary artery disease and cancer. Although there were no trials available focusing on the effect of heart rate reduction on outcomes in the general population, our results indicate the need to consider such a trial.
Footnotes
Infographic available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.160050/-/DC2
Competing interests: None declared.
This article has been peer reviewed.
Contributors: All of the authors contributed substantially to the conception and design of the study, the acquisition of data, and the analysis and interpretation of data. All of the authors drafted the article, revised it critically for important intellectual content, gave final approval of the version to be published and agreed to act as guarantors of the work.
- Accepted April 13, 2016.
References
In this issue

{kind=link}
{kind=link}
{kind=link}
Article extras
Article tools






Jump to section
Related Articles
Cited By...
- Heart Rate as a Predictor of Mortality in Heart Failure Patients at the Time of Discharge from the Intensive Care Unit
- Health Signatures During COVID-19: A Precision Fitness Case Study
- Modeling Cerebral Hemodynamics Using BOLD Magnetic Resonance Imaging and its Application in Mild Cognitive Impairment
- Impact of changes in heart rate with age on all-cause death and cardiovascular events in 50-year-old men from the general population
- Resting heart rate, temporal changes in resting heart rate, and overall and cause-specific mortality
More in this TOC Section
Similar Articles
Collections

