
ABSTRACT
Acute kidney injury (AKI) – an abrupt deterioration in renal function – causes a rise in serum creatinine (SCr) or fall in urine output. It is common, occurring in up to 20% of hospital admissions. Importantly, even small rises in SCr are associated with increased risk of death and longer hospital stays. A 2009 National Confidential Enquiry into Patient Outcome and Death report found that a proportion of AKI in secondary care was avoidable. In addition, management of established AKI was ‘good’ less than half the time. In practice, AKI represents a heterogeneous group of conditions, encompassing impairments in both kidney structure and function. Delivering disease-specific treatment early in the course of AKI may improve outcomes. The provision of best-practice care for all will rely on a better understanding of risk, and frameworks of care that can be applied across a diverse patient group.
Acute kidney injury (AKI) reflects a heterogeneous group of structural and functional diseases of the kidney.
It is common, and associated with significant morbidity and mortality.
A proportion of AKI is predictable, preventable or recognised late.
Risk relates to both acute insults and comorbid disease.
Care bundles can ensure timely diagnosis, appropriate supportive care, targeted therapy and referral.
Introduction – definitions and importance
Acute kidney injury (AKI) – an abrupt deterioration in renal function- causes a rise in serum creatinine (SCr) and/or fall in urine output. The magnitude of these changes is used to stratify the severity of AKI, as defined in an internationally agreed system of classification designed for clinical practice and research (KDIGO).1 Using this classification, AKI is common, occurring in up to 20% of hospital admissions.2 Importantly, even small rises in SCr are independently associated with an increased risk of death.2 Some 40,000 excess deaths are attributed to AKI each year in England alone;3 a mortality burden greater than that attributable to MRSA and venous thromboembolism combined.4 Morbidity is also high in AKI; it is associated with an increased length of stay,3 and the development of chronic kidney disease.5 This is expensive; one recent economic analysis estimated the associated healthcare costs for England alone to be over £1 billion per annum; a yearly cost that exceeds treatment for some major cancers.3
In practice, AKI represents a heterogeneous group of conditions, encompassing impairments in kidney structure and function. Of those diagnosed with AKI in hospital, roughly half will have effective hypovolaemia or sepsis.6 The remaining cases are caused by a mixture of obstructive uropathy, nephrotoxins and a variety of parenchymal renal diseases. The London AKI Network has produced comprehensive guidelines and care pathways, designed to assist clinicians in routine management. Their summary of the main causes of AKI is shown in Box 1.
Understanding risk in AKI
A 2009 National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report found that the care of patients with established AKI was ‘good’ less than half the time.7 The potential for the reduction of patient morbidity, mortality and healthcare costs in AKI are thus clear. Alongside sepsis, the NHS Five year forward view identified improving AKI care as an area that will maximally reduce avoidable mortality.8 Improving outcomes at scale will depend on better understanding of risk, and the consistent delivery of best-practice care.
The primary causes of AKI. Reproduced with permission from the London AKI Network.
The 2009 NCEPOD report also highlighted that up to 20% of AKI in secondary care was avoidable. The chance of developing AKI following exposure to an insult depends on a host of individual factors. These relate to both underlying susceptibilities (eg existing chronic kidney disease or diabetes) and exposures in hospital (eg sepsis or major surgery).9 Care should be taken to ensure that these exposures are minimised for patients at risk; this will include ensuring volume status is optimised and the avoidance of nephrotoxins. Monitoring of serum creatinine and urine output is also important for early recognition of AKI; but it should also be borne in mind that rises in SCr will lag behind any drops in in glomerular filtration rate following an insult to the kidneys by several days.
An organised approach to patient management
While the relationship between AKI, critical illness and comorbidities is complex, there is broad recognition that a strategy of early intervention may avoid significant parenchymal injury in patients with multi-system illness.10,11 Early review by a nephrology team may help ameliorate AKI,12 but the numbers of patients developing AKI and the centralisation of services make this impossible for all. As a result, local and regional care protocols exist for monitoring, investigation and supportive care (see Fig 1 for an example of such a pathway).13

An AKI care bundle. Reproduced with permission from the London AKI Network. ACE = angiotensin-converting-enzyme; AKI = acute kidney injury; ARB = angiotensin-receptor blocker; Bili = bilirubin; CK = creatine kinase; CRP = C-reactive protein; HUS = hemolytic-uremic syndrome; LDH = lactate dehydrogenase; NSAIDs = non-steroidal anti-inflammatory drugs; PCR = protein-creatinine ratio; retics = reticulocytes; TTP = thrombotic thrombocytopenic purpura.
Managing complications and tertiary referral
Patients with established AKI must also be monitored for complications; some may need to be cared for in higher acuity areas of care. Care protocols can guide immediate management and ensure patient safety (see Fig 2).
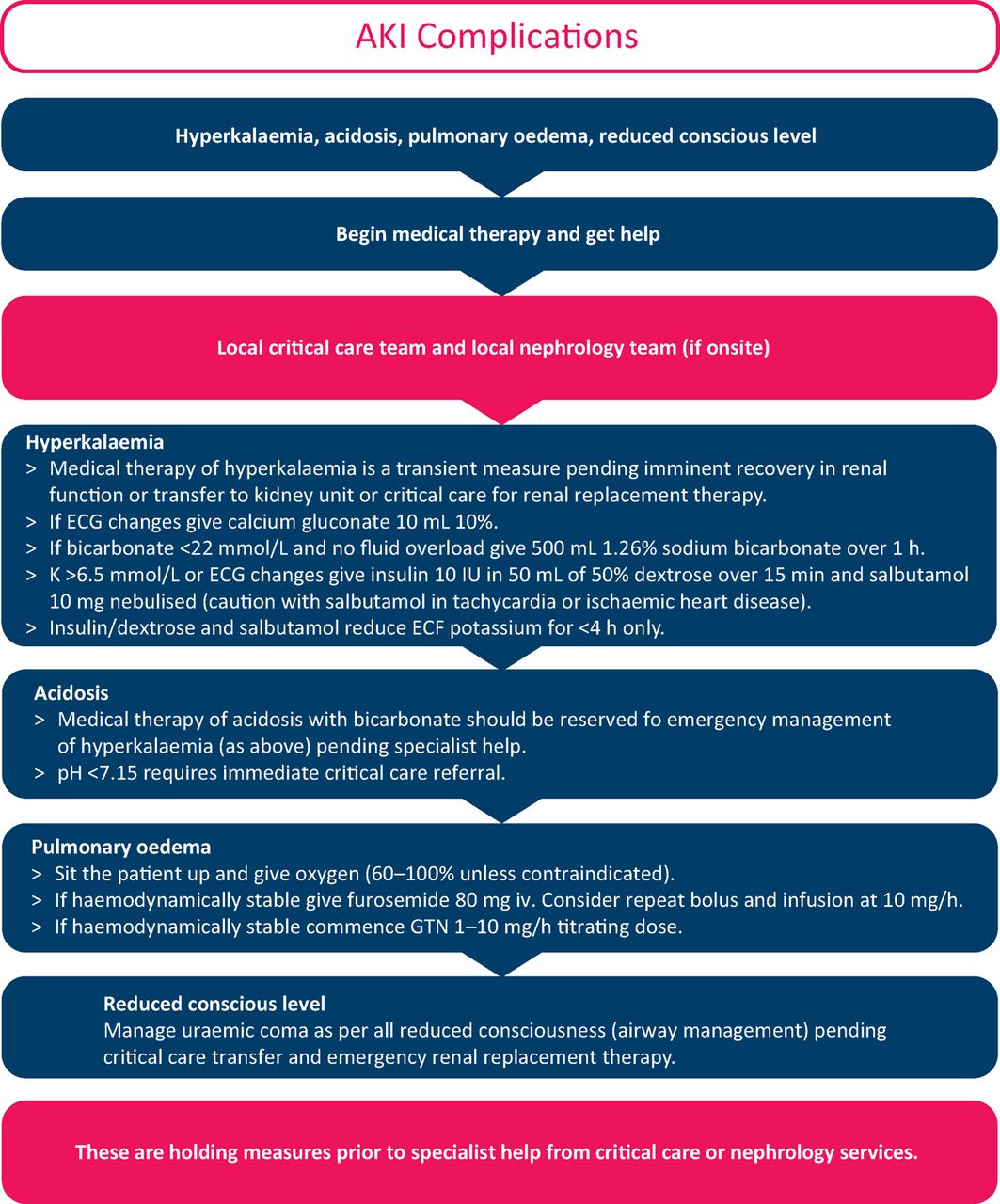
Managing complications in AKI. Reproduced with permission from the London AKI Network. AKI = acute kidney injury; ECG = echocardiogram; ECF = extracellular fluid; GTN = glyceryl trinitrate.
In addition, for any AKI patient with one of the above complications, local critical care services should be contacted for patients with AKI3 (serum creatinine >3X baseline OR >354 μmol/L OR initiation of renal replacement therapy), or those in whom imminent recovery is unlikely. Urgent referral to local urological services is warranted for those with obstruction on ultrasound. In the first instance, referrals to local nephrology services should be reserved for patients with AKI and the following:
myeloma
suspected autoimmune disease or glomerulonephritis (positive autoimmune screen; blood or protein on urine dip)
suspected hemolytic–uremic syndrome and thrombotic (history of diarrhoea or rash)
thrombocytopenic purpura
suspected poisoning.
Future frameworks for care
Recent local and national initiatives have focused on early recognition and timely intervention, leading to the adoption of real-time automated diagnostic algorithms.14 NHS England have produced one such algorithm, mandating that it be incorporated in some way into all hospital laboratory information management systems. Alerts for patients with AKI are to be displayed in patient management systems and reported centrally.15 However, trials of automated clinical decision support tools have had mixed results. A recent randomised controlled trial testing the efficacy of simple electronic e-alerting for AKI resulted in no significant differences in patient peak creatinine, requirement for dialysis or risk of death.16 As discussed above, patients with AKI form a heterogeneous group, and therapy is not standardised; a new process may be needed to guide the nature and scale of clinical response in the right timeframe. It has already been demonstrated that existing patient data can be used to reduce false positive alerts (eg patients with chronic kidney disease or on renal replacement therapy).17 As computers become more powerful and patient-specific data are coded with greater granularity, the potential for more advanced risk prediction using artificial intelligence is huge.
Current approaches in the diagnosis of AKI are also limited by the regularity with which SCr or urine output are measured. In the future, strategies may focus on fostering early detection and more targeted therapy. Numerous novel biomarkers reflecting function or structural damage to the kidney have been investigated (neutrophil gelatinase-associated lipocalin, kidney injury molecule 1). Although there is hope that they may one day facilitate earlier diagnosis or differentiate separate causal pathways, current approaches lack sensitivity and may be less effective at the level of the individual patient. Crucially, they have yet to consistently show value in clinical decision making above and beyond existing SCr and urine output monitoring. Future efforts may focus on their use alongside existing biochemical and clinical information.18
- © Royal College of Physicians 2015. All rights reserved.
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Scoping review exploring the impact of digital systems on processes and outcomes in the care management of acute kidney injury and progress towards establishing learning healthcare systems
- A scoping review exploring the impact of digital systems on processes and outcomes in the care management of acute kidney injury and progress towards establishing learning healthcare systems