Article Text

Abstract
AIMS To measure the concentrations of total IgA in the milk secreted by both breasts, throughout the first year of lactation, in a cohort of Gambian mothers of infants at high risk of infection.
SUBJECTS AND METHODS Sixty five women and their infants were studied monthly from the 4th to 52nd postpartum week. Samples of milk were obtained from each breast by manual expression immediately before the infant was suckled. Milk intakes were measured by test weighing the infants before and after feeds over 12 hour periods; IgA concentrations were determined by enzyme linked immunosorbent assay.
RESULTS A total of 1590 milk samples was measured. The median (interquartile range) concentration of IgA for all samples was 0.708 (0.422–1.105) g/l; that in milk obtained from the left breast was 0.785 (0.458–1.247) g/l, and that in milk obtained from the right breast was 0.645 (0.388–1.011) g/l (p < 0.0001). There was no significant change in milk or IgA intakes with advancing infant age, but there was a close concordance of IgA concentrations between the two breasts, with “tracking” of the output of the left and right breasts. There was a significant (p < 0.01) negative correlation between maternal age and parity, and weight of milk ingested by infants. During the dry season (December to May) the median (interquartile range) IgA concentration was significantly higher at 0.853 (0.571–1.254) g/l than during the rainy season (June to November), when it was 0.518 (0.311–0.909) g/l (p < 0.0001).
CONCLUSIONS Sustained IgA secretion is likely to protect suckling infants from microbial infection.
-
Human milk is rich in protective proteins, including IgA, which plays a part in the prevention of microbial infection in suckling infants
-
IgA secretion is maintained at around 0.5 g/day by Gambian mothers throughout the first year of lactation
-
There is a negative correlation between maternal age and parity, and weight of milk ingested by infants
-
During the dry season, when food is most plentiful, milk IgA concentrations are higher than during the rainy season, when food is scarcer
-
There is a close concordance of milk IgA concentrations between the two breasts, with “tracking” of output of the left and right breasts, suggesting control of secretion above the level of the mammary gland
- immunoglobulin A
- human milk
- lactation
Statistics from Altmetric.com
Human milk is rich in protective proteins which play a part in the prevention of microbial infection in suckling infants. These include IgA, lactoferrin, lysozyme, antiproteases, complement, and many other factors.1 2 IgA is foremost of these in terms of its concentration in human milk, and in the breadth and sophistication of its protective effects.
IgA is produced by the secretory cells of the breast as a dimeric molecule composed of two pairs of heavy and light chains linked together by secretory component and a J chain. Via the enteromammary circulation a lactating mother may secrete in her milk specific IgA that protects her infant from microbial antigens to which both she and her infant have been exposed. Antigens ingested by mothers are “recognised” by M cells at the mucosal surface of the small intestine, where local lymphocytes are primed, whence they migrate via the lymphatic system to the breast.3 There plasma cells secrete specific IgA which acts to protect the mucosal surface of the gastrointestinal tract of the infant from those antigens. Human colostrum contains more than 1 g/l of IgA and the fully breast fed infant ingests as much as 1 g of IgA each day.1 2
There have been a number of prospective studies of the changes in IgA concentrations of human milk throughout lactation,4-6 but none has measured interbreast variations in output, nor sequential changes throughout every month of lactation, and during each season of the year.
The aim of this study was to measure the concentrations of total IgA in the milk, secreted by both breasts, of a cohort of mothers throughout the first year of lactation and to quantify the intake of IgA by their infants during this time.
Subjects and methods
A prospective cohort study design was used. The project took place at the overseas research unit of the MRC Dunn Nutrition Unit in the village of Keneba in the Gambia.7 All the mothers in this village breast feed their infants for at least one year. The median age of the first introduction of non-milk, local weaning foods is 3 months.
Eighty one mothers were eligible for enrolment to the study. Two mothers declined to participate and 14 dropped out because of illness or absence from the village. Sixty five Gambian mothers were studied monthly during the first year of lactation. A 5 ml volume of milk was collected before each feed from both breasts by manual expression and samples were stored at −20°C and transported to the UK, packed in solid carbon dioxide, where analyses were performed.
Twelve hour weighed milk intakes (0700 to 1900 h) were measured for all 65 mothers on five occasions during the year at 9, 17, 27, 39, and 51 weeks postpartum. The volume of milk ingested by each infant was measured by weighing the infant before and after each feed using an electronic balance accurate to 1 g (Mettler, Switzerland).
Milk samples were assayed for total IgA using an enzyme linked immunosorbent assay (ELISA) on 96 well polystyrene microtitre plates (Immulon 4, Dynax, Billinghurst) coated with a human colostral standard (Sigma, Poole). The plates were coated and left overnight at 4°C with 100 μl/well (4 μg/ml) goat antihuman IgA (Sigma) diluted in 0.1 mol/l carbonate buffer (pH 9.6). After three washes with pH 7.3 phosphate buffered saline (PBS) containing 0.05% Tween, the plates were blocked with 1% w/v bovine serum albumin (BSA) (Sigma) in PBS for one hour at room temperature. After a further three washes the milk samples and colostrum standards were diluted in 1% w/v BSA/PBS and loaded onto the plate at 100 μl/well and incubated overnight at 4°C. After washing with PBS/Tween, 100 μl/well of horseradish peroxidase conjugated goat antihuman IgA (Sigma) (diluted 1:12 000 in 1% w/v BSA/PBS) were added and the plates were incubated at room temperature for two hours. Finally, the plates were washed a further three times with PBS/Tween and 100 μl of 0.4 mg/ml freshly preparedO-phenylenediamine dihydrochloride dissolved in 0.05 mol/l phosphate-citrate buffer (pH 5.0) containing 0.4 μl/ml hydrogen peroxide (0.04%) was added. The reaction was stopped after 20 minutes by adding 1 N sulphuric acid and the absorbance was determined at 490 nm using a Dynatech MR5000 ELISA plate reader (Dynax).
Changes in IgA concentration over time, between each breast, and in relation to season, maternal age, and parity were analysed using appropriate parametric and non-parametric tests of statistical significance. The study was undertaken with the approval of the joint MRC-Gambian Government ethical committee and was performed with the informed consent of the mothers and a meeting of the village elders.
Results
A total of 1590 milk samples was assayed (798 from the right breast and 792 from the left breast). The median (interquartile range) concentration of IgA from all samples was 0.708 (0.422–1.105) g/l. There was a significant difference in the median (interquartile range) IgA concentration of milk obtained from the left breast, which was 0.785 (0.458–1.247) g/l and that from the right breast, which was 0.645 (0.388–1.011) g/l (p < 0.0001) (fig 1).
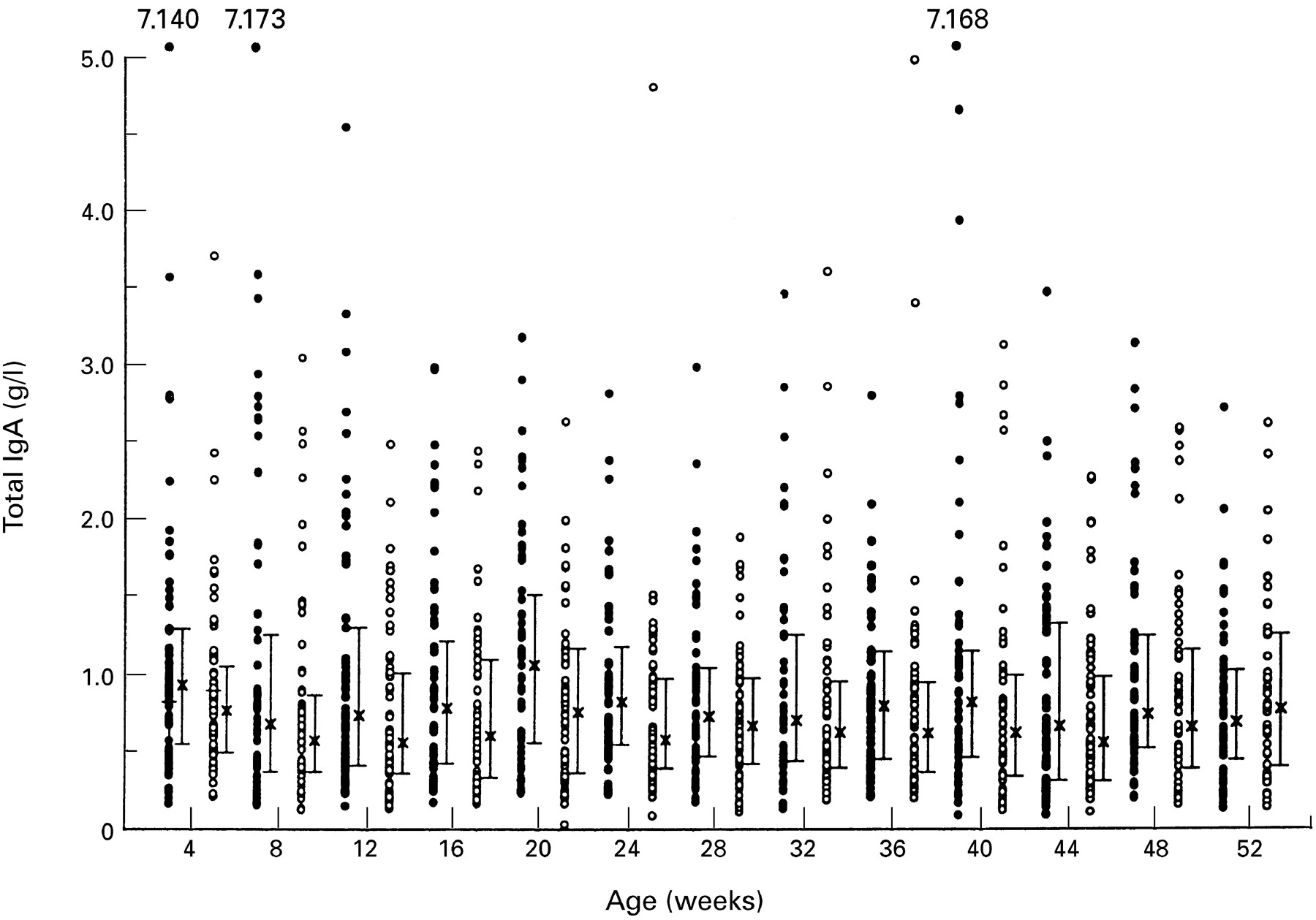
Total IgA concentrations in milk samples obtained from the left (closed symbols) and right (open symbols) breasts of mothers during the first year of lactation. The median and interquartile ranges are shown.
There was no significant change in the median IgA concentrations from the whole population over time during the first year (fig 1). There were, however, significant degrees of variation within individual mothers, with a close concordance of IgA concentrations between the two breasts, with “tracking” of the output of both breasts. Figure 2shows four examples of these parallel changes in IgA concentration in milk obtained from the two breasts.

Total IgA concentration of milk obtained from the left (closed symbols) and right (open symbols) breasts from four mothers, showing parallel changes during the first year of lactation.
Table 1 gives the results for the five periods when milk intakes were measured. The mean (SD) weight of milk ingested in 12 hours by infants ranged between 376 (98) g (at 8–9 weeks) and 312 (94) g (at 51–52 weeks). The median (interquartile range) of IgA concentrations in milk ranged from 0.625 (0.376–0.959) g/l (at 8–9 weeks) to 0.746 (0.408–1.067) g/l (at 51–52 weeks). The median (interquartile range) weight of IgA ingested in 12 hours by infants ranged from a maximum of 279 (151–363) mg at 16–17 weeks to a minimum of 208 (151–336) mg at 51–52 weeks. There was no significant change in weight of IgA ingested with advancing age. There was no significant correlation between the weight of milk ingested and IgA concentrations at any age except at 9 weeks, when it was p < 0.002.
Changes in milk ingested (mean, SD), total IgA concentration (median, interquartile range), and total IgA ingested/12 hours (median, interquartile range) for all 65 mother-infant pairs
The results from each mother were averaged over the year and there was a significant (p < 0.01) negative correlation between maternal age and parity, and the weight of milk ingested by their infants, but the correlations with the concentration of milk IgA and weight of IgA ingested were barely significant.
During the two dry seasons (December to May) the median (interquartile range) milk IgA concentration was significantly higher (p < 0.0001) at 0.853 (0.571–1.254) g/l than during the three rainy seasons (June to November), when it was 0.518 (0.311–0.909) g/l. The weight of milk ingested was less in the wet season (330 g/12 hours) than in the dry season (median 361 g/12 h) (p < 0.03). The weight of IgA ingested was significantly higher in the dry seasons (p < 0.0001) (310 (212–418) mg/12 hours) than during the rainy seasons (175 (118–266) mg/12 hours) (fig 3).

{kind=link}
{kind=link}
{kind=link}
Total IgA ingested in 12 hours throughout the year showing seasonal changes. Median and interquartile ranges are shown.
Discussion
We have shown that mothers maintain a steady output of IgA throughout the first year of lactation, that there is a difference in the concentration of IgA secreted by each breast, and there is a variation throughout the year according to season. The seasonal changes are due more to fluctuations in milk IgA concentrations than the weights of milk ingested. These findings confirm and extend those of other studies of lactating mothers in both the developing and developed world,4-6 and underline the potential value of prolonged breast feeding in infancy. Human milk has been shown to confer protection against several enteric and respiratory infections,2 8 and in circumstances of poor hygiene and high risk of infection it is likely to be of significant importance to the suckling infant.
IgA acts at the mucosal surface of the gastrointestinal tract to protect against potentially harmful microbial and food antigens. Although the infants continued to ingest a constant amount of IgA each day, the amount relative to body weight decreased. The length of the small intestine increases by 56% during the first year of postnatal life, in parallel with an increase in body weight of 55% and length of 50%.9 IgA survives passage through the gastrointestinal tract10 and its detection in the faeces of breast fed infants throughout the first year suggests that the amounts ingested remain sufficient to provide mucosal protection in spite of the increasing surface area of the gastrointestinal tract.
The amount of IgA ingested by the infants was dependent on both the weight of milk consumed and the concentration of IgA within it. For the whole cohort IgA concentrations did not change significantly between 8 and 52 weeks (fig 1), but seasonality affected the intake through an effect largely on the IgA concentration, resulting in an almost doubling of the IgA ingested by infants during the dry season (fig 3). The Gambian dry season is a time of plentiful food, good maternal nutritional status, and low prevalence of infection. In contrast, food stocks are depleted, nutritional status declines, and infection is common in the wet season. The influence of season on milk IgA concentrations and output has been described previously, but it is not thought to be due to variations in the prevalence of infectious diseases.11 Lower parity and maternal age were both associated with higher concentrations of IgA in milk, as described previously in the Gambia,12 but in a study in Zaire milk IgA concentrations were highest in multiparous women.6
The parallel changes in concentrations of IgA in milk obtained from each breast suggests that the synthesis or secretion of IgA is controlled above the level of the breast. This hypothesis is strengthened by our observation of seasonal effects in which changes in milk output and IgA concentrations parallel changes in maternal nutritional status.11 These have been well described previously during pregnancy in the same population, albeit in smaller numbers of mothers.13 Regulation must, however, be by factors other than maternal nutrition alone, as dietary supplementation has been shown not to abolish variations.5 Unilateral breast dysfunction can affect milk composition, but the average milk output is not usually compromised.14
The method used to measure milk intakes has been used for many years in Keneba5 11 13 and its reliability has been validated using isotopic analysis.15 There appeared to be no change in milk IgA concentrations in response to complementary feeding. We have previously shown16 that the introduction of a weaning (non-milk) diet is associated with a transient decrease in breast milk output, but that this is not long lasting.
The differences in IgA concentrations in milk obtained from the two breasts may be related to the tradition of starting infant feeding on the right side. In 19 mothers in whom suckling was closely observed, 18 offered their infants the right breast first. In four mothers, who were studied at 48 weeks of lactation, the mean milk intake from the right breast was 244 g/12 hours, and from the left breast 84 g/12 hours. There was no significant difference in the time infants were suckled on each side (29 minutes on the right and 27 minutes on the left). It is therefore possible that the larger volumes of milk secreted by the right breast could, through a dilutional effect, account for the smaller concentrations of IgA in milk from that side. We found no significant correlation between milk volumes and IgA concentrations, however, except at 9 weeks of age.
Breast milk not only makes a major contribution to the nutrition of infants, but also provides a range of non-nutritional, bioactive factors,17 including immunoproteins.1 In conditions where infectious disease is common, and where weaning foods may be suboptimal,18 mothers can provide their infants with quantities of IgA in milk that are likely to play a significant part in improving their health.
Acknowledgments
We thank Dorothy Stirling, Ann Prentice, Esther Oostenveld, Momodou Darboe, Baba Jobarteh, Mustapha Sanyang, Lamin Sanyang, Mustapha Sise, and Jean Hyslop for their help with this project, and the Thrasher Research Fund and Bristol-Myers Research Foundation for their support.