Article Text

Abstract
Objectives: To examine seasonality and long-term trends in the incidence and prevalence of gout.
Methods: A retrospective study (1994–2007) using routinely collected surveillance data from the Royal College of General Practitioners Weekly Returns Service sentinel general practice network in England and Wales. New cases and acute attacks of gout per 10 000 population were calculated for age groups 0–44, 45–64, 65–74 and ⩾75 years. Long-term trends of annual incidence were assessed by regression analysis. Seasonality indices were calculated using 4-weekly data, and the relative risk of gout incidence during the summer was estimated. Annual prevalence was estimated from the consulting patient population (2001–7) and from prescribing data on defined daily doses (DDD) of allopurinol (2003–7).
Results: The annual incidence rate of new gout cases was stable over the period 1998–2007; acute attacks decreased on average 4% per annum. New gout cases and acute attacks combined into 4-weekly incidence rates peaked during the “summer” period of each year. There was an increased risk of gout diagnosis during summer months (late April to mid-September; odds ratio 1.22, 95% CI 1.18 to 1.26). The annual prevalence of gout in 2001–7 was 0.46%, with highest rates in men ⩾75 years (2.57%). Estimated prevalence based on a DDD of 400 mg allopurinol was 0.37%.
Conclusion: The incidence of gout is seasonal. This has implications for the management of patients who currently have gout, and for those who are at risk of future attacks. The decreasing trend in the incidence of acute attacks suggests that patient management is improving.
Statistics from Altmetric.com
Gout is one of the most commonly diagnosed rheumatic diseases in general practice. The prevalence of gout in the UK population has been estimated to be 1.4%.1 2 The second and fourth UK National Morbidity Studies demonstrated a threefold increase in gout prevalence between 1971 and 1991.3 4 In the USA, a number of studies have estimated overall gout prevalence to be in the range of 0.5% and 1% and up to 4.6% in men and 2% in women.5 Prevalence increases with age.2
In England and Wales the population aged 65 years or older has increased from 5.5 million in 1961 to over 8.5 million in 2007, and is projected to increase to over 11 million by 2020, considerably increasing the societal burden of gout.6 A study from the USA estimated the cost of new cases of gout in men to be US$27.4 million per year;7 there are no similar estimates available for the UK.
General practitioner (GP) databases have previously been used to estimate national gout morbidity.1 2 8 In this study we utilised the Royal College of General Practitioners Weekly Returns Service (WRS), a sentinel GP network located across England and Wales that routinely monitors all disease episodes from every consultation diagnosed in the network on a weekly basis.9 10 Currently, the WRS consists of approximately 500 GPs located in 100 practices. The denominator patient population currently monitored is 920 000 patients (1.7% of the national population), and is representative of the national population structure. The WRS extracts data from differing clinical software systems, thus removing any potential bias presented from using one system. The clinical data captured by the WRS are of a high quality: GPs are encouraged to record morbidity data using diagnostic terms rather than symptomatic terms describing their assessment of the problems using the most concise term possible. GPs in the WRS are required to specify the episode type, which is classified as the first time ever encountered, a new occurrence of a previously encountered episode, or an ongoing consultation for the same episode.
The main aim of this study is to identify and describe seasonal patterns in the incidence of gout in order to improve awareness of periods when patients are at higher risk of having the disease. A secondary aim is to examine the long-term trend of gout incidence and prevalence to provide indications of the current and likely burden for GPs.
Methods
Incidence data
Incidence of new gout cases
Clinical incidence data for new cases of gout were analysed. New gout cases were defined as the first consultation for a first time ever occurrence of a diagnosis of gout (International Classification of Diseases, version 9, code 274). Weekly incidence rates of new cases of gout per 10 000 population were calculated over the period 1994 to 2007 using aggregated weekly numbers of new cases diagnosed in the network and the weekly reporting population; 4-weekly, quarterly and annual incidence rates were calculated similarly. New case incidence data were analysed for men and women separately, and for each of four age groups; 0–44, 45–64, 65–74 and 75 years and older using the age-specific weekly population as the denominator.
Incidence of acute gout attacks
Acute attacks of gout were defined as a new occurrence of a previously diagnosed case of gout, regardless of when the first episode occurred. Although the GP clinical systems differ in their definition of the time period required to differentiate a new case and an acute attack, in the WRS we rely on the clinical judgement of the GP to determine whether a diagnosis is a first diagnosis or new attack of gout. Incidence rates of acute attacks of gout were calculated as described for new cases.
Prevalence data
Annual prevalence data are available from the WRS practices over the years 2001–7.11 We defined annual prevalence as a count of individuals presenting to a GP or other primary care health professional with a particular disease/condition within a calendar year regardless of the episode type. Annual prevalence rates per 10 000 individuals were calculated.
Prescribing data
Prescribing analysis and cost data (PACT) report the number of dispensed prescriptions issued by GPs in England in the NHS.12 PACT data were provided by the NHS Business Services Authority Prescription Pricing Division for the years 2003–7 covering monthly numbers of items (and cost per item) of the gout-specific drugs colchicine and allopurinol coded in the British National Formulary (10.1.4 and 10.1.4, respectively).13 For allopurinol, data were also obtained as defined daily doses (DDD), indexed at 400 mg per day.14
Analysis
The annual male and female incidence rates of new cases and acute attacks of gout were first examined graphically and, when appropriate, regression analyses were performed to model long-term trends. The age-specific annual incidence rates (men and women combined) were similarly analysed.
To investigate seasonality, new cases and acute attacks were aggregated and 4-weekly incidence data were calculated using the total number of gout episodes diagnosed and the mean weekly population over the period for the numerator and denominator, respectively. The resulting 182 incident rate values were first examined graphically and then analysed by the well-established multiple decomposition method,15 whereby a time series is described by the product of trend, seasonality, a long-term periodic feature and a random error component. An output from this analysis is the production of seasonality indices, one for each of the 13 4-weekly time intervals. A value of unity signifies an average rate for that period, ie, no seasonal excess or deficiency. Incidence rates over 4-weekly periods exhibiting different seasonal features were thus identified and contrasted. It was not possible to measure the contribution of any long-term periodic feature of these data, so this component was put equal to unity.
Results
Incidence of new gout cases
Long-term trend
The annual episode incidence rate of new cases of gout per 10 000 population is shown for the years 1994–2007 (fig 1A). The mean annual incidence was 12.4 cases per 10 000 (31.5 per 10 000 using individuals aged ⩾45 years as the denominator) and there was no evidence of increasing or decreasing trend.
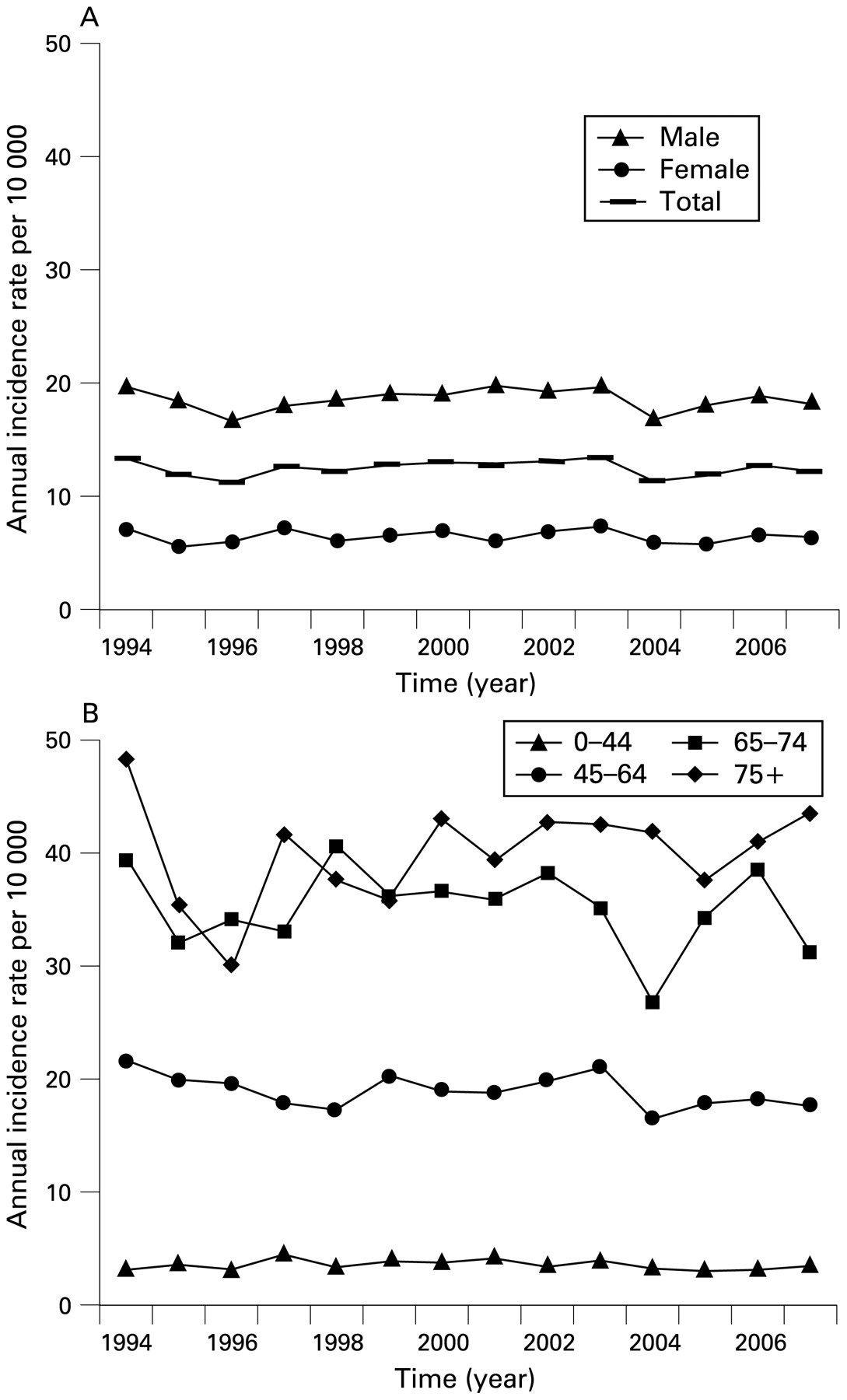
(A) Annual incidence of new cases of gout per 10 000 population (1994–2007); data are shown for all ages (total) and male and female-specific rates. (B) Age-specific annual incidence of new cases of gout per 10 000 population (1994–2007).
The annual incidence of new gout cases in men (mean incidence 18.6 per 10 000; 49.3 per 10 000 individuals ⩾45 years) was approximately three times the female incidence (mean incidence 6.4 per 10 000; 15.7 ⩾45 years). The ratio between male and female cases was relatively constant over time (fig 1A) but varied between age groups: 45–64 years, 5 : 1; 65–74 years, 3 : 1; 75 years and older, 2 : 1 (table 1).
Annual incidence of new cases of gout per 10 000 in men and women, England and Wales 1994–2007
Age-specific analysis
Incidence rates of new cases of gout for each of four age groups (men and women combined) are shown in fig 1B. Incidence increased with age: incidence rates in individuals under 45 years were extremely low and therefore this age group has been excluded from further analysis. Incidence was maximum in the 75 years and older age group (mean incidence 40 per 10 000), with decreasing incidence across the other age groups (65–74 years and ⩾45 years, 35.1 and 18.9 per 10 000, respectively).
Incidence of acute gout attacks
Long-term trend
The annual episode incidence rate of acute attacks of gout per 10 000 population is shown for the years 1994–2007 (fig 2A). The mean annual incidence was 18.4 cases per 10 000 (46.9 per 10 000 individuals ⩾45 years). A decreasing linear trend was evident, especially over the years 1998 to 2007. A log-linear regression analysis applied to the combined male and female annual rates (1998–2007) confirmed there was a small but significant decreasing trend (slope −1.05, 95% CI −1.06 to −1.04); a reduction of one per 10 000 acute gout attacks per year, or 4% per annum.

(A) Annual incidence of acute attacks of gout per 10 000 population (1994–2007); data are shown for all ages (total) and male and female-specific rates. (B) Age-specific annual incidence of acute attacks of gout per 10 000 population (1994–2007).
Age-specific analysis
Further information is given for acute attacks of gout in each of four age groups (men and women combined; fig 2B). As with the incidence of new cases of gout, rates were highest in the 65–74 and 75 years and older age groups (57.7 and 50.9 per 10 000, respectively). The incidence in men was approximately four times the female incidence. The ratio between male and female attack rates was relatively constant over time; however, there were differences within certain age groups: in the 45–64 year age group the ratio was 9 : 1, the 65–74 year age group 4 : 1 and the 75 years and older age group 3 : 1 (table 2).
Annual incidence of acute attacks of gout per 10 000 in men and women, England and Wales 1994–2007
The seasonality of gout
Age-specific incidence rates were calculated for new cases and acute attacks of gout combined for each 4-week period; the mean 4-weekly incidence rates over the 14-year period are shown in fig 3A. Incidence increased with age for each of the 13 4-weekly periods. There was evidence of increased activity during 4-weekly periods 5 to 8 (late April to mid-September, ie, the “summer” period). This was evident across the 45–64, 65–74 and 75 years and older age groups.

(A) Four-weekly incidence of gout per 10 000 over the years 1994–2007; data are presented for the 45–64, 65–74 and 75 years and older age groups (men and women combined). (B) Seasonal indices computed for gout incidence data (all ages, men and women combined).
The seasonality indices for the 13 4-weekly intervals are shown in fig 3B. Values for the first four 4-weekly intervals are near unity and indicate very little seasonal effect. For each year, new cases and acute attacks during this period were treated as a control group in an unmatched control study of the cases occurring during the subsequent 4-weekly periods 5–8.
We calculated an approximate relative risk of gout occurring during the later period (“summer”) for each year. The minimum odds ratio (OR) of gout occurred during the summer of 2007 (OR 1.02, 95% CI 0.92 to 1.12) and the maximum during 1995 (OR 1.46, 95% CI 1.26 to 1.69). An estimate of the OR over the 14 years included in the study was calculated by combining the individual years by using the logit method for giving a pooled estimate of an OR and its derived CI (OR 1.22, 95% CI 1.18 to 1.26).16 It is inappropriate to compare the decreased risk similarly during the last five 4-weekly periods of the year because these lower than average rates will balance out the higher than average incidence of cases during the “summer” period, a harvesting effect.
Prevalence of gout
The overall prevalence of gout in 2001–7 was 0.46%; the highest prevalence (2.57%) was in the male 75 years and older age group (table 3). Between 2001 and 2007 there was an increase in the prevalence of gout, this was most evident in female patients aged 65–74 years. We extrapolated the data to estimate the numbers in the national population for England and Wales.6 During 2001, we estimated that 225 148 individuals (179 020 men and 42 857 women) consulted their GP for a gout-related episode. This figure rose to 252 525 individuals in 2007, an increase of 12%, or 27 377 cases. The estimates increased by 50% and 11% in the female age groups 65–74 and 75 years and older, respectively, compared with a 1% decrease and 12% increase, respectively, for equivalent male age groups.
Annual prevalence (%) of gout in men and women, England and Wales 2001–7
Prescribing data
PACT data for gout-specific drugs were available as monthly items dispensed over the years 2003–7. The two most commonly prescribed drugs were allopurinol and colchicine; allopurinol was prescribed much more frequently than colchicine, the sum of items dispensed was 13.6 million and 660 000, respectively, over the 5 years. These were transformed to mean numbers of items dispensed per quarterly period to enable a direct comparison with quarterly gout incidence rates. Items of colchicine were most commonly dispensed during quarters 2 and 3, concurring with the quarterly incidence data for gout (fig 4A and B). Over the years 2004–7 there were on average 65.1 million annual DDD of allopurinol, which equates to an annual “use prevalence” of 0.37% of the population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Mean quarterly incidence of gout per 10 000 over the years 1994–2007 and mean monthly items dispensed per quarterly period for (B) colchicine.
Discussion
We have utilised data collected from a sentinel GP surveillance network to examine recent trends and seasonal patterns in gout in England and Wales. We have made the distinction in the GP morbidity data between new cases (first ever diagnoses) of gout and acute attacks (new occurrences). Since 1994 the overall incidence of new cases of gout has remained relatively stable. The incidence of acute attacks has gradually declined since 1998. These data imply that the occurrence of patients presenting to their GP with their first ever attack of gout remained relatively constant over the study period, but the number of patients consulting with subsequent acute attacks has fallen. It is therefore possible that the treatment of gout patients in the UK has improved since the 1990s, resulting in fewer subsequent repeat gout attacks prompting a GP consultation.
Annual prevalence increased over 2001–7, suggesting that patients were seen more frequently and probably receiving more rigorous treatment regimes. DDD data demonstrated that the number of patients receiving allopurinol therapy increased (2004–7) confirming our prevalence findings. Estimates of prevalence in the WRS data (0.46%) slightly exceeded the estimates from prescribing data (0.37%) based upon a DDD of 400 mg,14 but if based upon the commonly used dosage regime of 300 mg a day, the estimates are similar. However, there may be additional cases of gout unrecognised in the WRS because they have received repeat prescriptions but not consulted in the respective annual periods. We believe this possibility has decreased in recent years and may explain the recent small increase in prevalence. If the optimal dose of allopurinol exceeds 400 mg, these data are indicative of suboptimal dosage.
The greatest increase in prevalence was observed in women aged 65–74 years. Patients within this group will be post-menopausal, including some who may be on diuretic therapy or obese, both of which are recognised risk factors for gout.17 18 Recent increases in the incidence of diabetes in this age group, especially among women might also be relevant.19
We describe and quantify a seasonal trend of gout (new and acute attacks combined) in England and Wales, with peak incidence during summer, which has been reported in other countries.20 21 22 The peak incidence during the summer months suggests that environmental conditions precipitate attacks of gout. We hypothesise that temperature may be important, especially by influencing dehydration. We found that, after deseasonalising the data, there was a positive association between gout incidence in a given week and temperature in the same week and that in the previous week. Gout patients (or at-risk patients) should be advised to maintain adequate levels of hydration during these periods. Other factors may also influence the risk of gout: increased physical activity may accentuate local joint trauma; fluctuations in weight may lower uric acid levels and trigger gout attacks; changes in atmospheric pressure and relative humidity have been shown to affect other rheumatic diseases including osteoarthritis.23 24
The PACT data showed that allopurinol is prescribed much more frequently than colchicine. We found concurrent peaks of episodes of gout and the number of colchicine items dispensed, thereby illustrating the use of this drug for treating gout (colchicine is as likely to be prescribed by GPs for managing recurrent episodes as it is for new cases). Prescribing data provide an indication of the current cost of gout treatment. The cost of dispensed allopurinol over the 5 years 2003–7 averaged £6.9 million per year and of colchicine £1.2 million per year. There are also the indirect costs, which include absenteeism from work that combine to disclose the high economic burden imposed by gout and should stimulate further cost-effectiveness studies.
The WRS is a clinical information system that collates diagnostic data from a network of GP practices across England and Wales. The quality of data collected in the network is high and have been validated in previous National Morbidity Studies.3 4 By recording the episode type in relation to each morbidity entry, new episodes of disease are distinguished from ongoing consultations. However, the WRS does not collect prescription data from the recording practices, and thus the number of gout patients receiving gout-specific drugs could not be ascertained. PACT data are collated from NHS prescriptions issued by GPs (but not hospital or dental prescriptions) and submitted to the prescription pricing division after dispensing in retail pharmacies.
There have been several reports documenting an increase in gout prevalence during the 1990s. Arromdee et al25 reported that the age and gender-adjusted annual incidence of gout in the USA more than doubled from 1977–8 to 1995–6. There was a threefold increase in UK gout prevalence over a 30-year period, as demonstrated by data originated from the UK National Morbidity Studies of 1971–2, 1981–2 and 1991–2;3 4 8 26 those studies were based upon the WRS network and therefore the data are directly comparable with the prevalence estimates made in this study. A recent study by Mikuls and colleagues2 used data from the UK General Practice Research Database (GPRD) over the years 1991–9. The estimates from the GPRD demonstrated that annual incidence rates of gout fell between 1994 and 1999. Our results confirm that acute attacks of gout have continued to fall; however, our annual incidence data for new cases remained relatively stable. An advantage of the WRS is the ability to differentiate initial diagnoses from exacerbations and follow-up consultations; it is not clear how this distinction is made in the GPRD.
The data generated from the GPRD for the UK were examined in 1999 and yielded an estimated gout prevalence of 1.4%, peaking in the male 75–84 years age group at 7.3%.2 Our prevalence estimates (0.5% and 2.6%, respectively) were much lower and were consistent with estimates that might be derived from prescribing data. Furthermore, the WRS estimates are identical to data from a similar sentinel GP network in The Netherlands, where overall estimates were 0.5%, peaking in men aged 75 years and older at 2.45%.27 28 We believe in this instance that prevalence in the GPRD study was the cumulative prevalence, whereas our estimates and those from The Netherlands are based upon annual prevalence, ie, a count of all individuals presenting to a GP for a gout-related consultation during a calendar year.
The WRS data show that the incidence of new gout cases has remained stable over the past 14 years. The falling incidence of acute attacks suggests that patient management of gout has improved. Health professionals should be aware of the increasing risk of gout in older women (aged 65–74 years) and of the increased risk of gout during summer months.
Acknowledgments
The authors gratefully acknowledge the contribution of the WRS sentinel practices and their staff to providing the GP episode data. They are grateful to Dr Helen Kendall and Alison Bowes (NHSBSA Prescription Pricing Division) for providing access to the prescribing data.
REFERENCES
Footnotes
Funding The RCGP Research and Surveillance Centre (registered UK charity no 223106) is funded by the Department of Health. AJE is jointly funded by the Royal College of General Practitioners and the Health Protection Agency.
Competing interests None.