
Abstract
The lateralization of emotion processing is currently debated and may be further explored by examining facial expression recognition (FER) impairments in temporal lobe epilepsy (TLE). Furthermore, there is also debate in the literature whether FER deficits in individuals with TLE are more pronounced in the right than in the left hemisphere. Individuals with TLE were tested with an FER task designed to be more sensitive than those classically used to shed light on this issue. A total of 25 right- and 32 left-TLE patients, candidates for surgery, along with controls, underwent an FER task composed of stimuli shown not only at full-blown intensities (100 %), but also morphed to lower-intensity display levels (35 %, 50 %, and 75 %). The results showed that, as compared to controls, right-TLE patients showed deficits in the recognition of all emotional categories. Furthermore, when considering valence, right-TLE patients were impaired only in negative emotion recognition, but no deficits for positive emotions were highlighted in left-TLE patients. Finally, only the right-TLE patients’ impairment was found to be related to the age of epilepsy onset. Our work demonstrates that the FER deficits in TLE span multiple emotional categories and show manifestations dependent on the laterality of the epileptic focus. Taken together, our findings provide the strongest evidence for the right-hemisphere model, but they also partially support the valence model. We suggest that current models are not exhaustive at explaining emotional-processing cerebral control, and further that multistep models should be developed.
Similar content being viewed by others

Although initial research had indicated a dominant role of the right hemisphere in emotional processing, more recent research has indicated that both hemispheres contribute to such processing (Demaree, Everhart, Youngstrom, & Harrison, 2005). Brain structures that are critically involved in emotional processing, such as the amygdala and the temporal cortices (Adolphs, 2010; Haxby, Hoffman, & Gobbini, 2000; Olson, Plotzker, & Ezzyat, 2007), are affected by temporal lobe epilepsy (TLE), which is typically lateralized in focus, making the condition a window for the understanding of the laterality of emotion processing. As compared to cerebrovascular damage and transcranial magnetic stimulation (TMS), epilepsy presents several advantages. For instance, cerebrovascular damage is usually associated with a number of diverse cognitive impairments, particularly in the acute phase (Ferro, 2001). Furthermore, it is quite rare to observe a stroke patient presenting emotional deficits that are limited to “recognition,” while it is usually reported that patients are affected by productive symptoms concerning emotions (such as the “catastrophic” reaction or the “depressive” reaction; Chemerinski & Robinson, 2000). Finally, aphasia is quite common after left stroke, and this could hinder the use of a labeling task to explore FER (de Freitas, 2012). On the other hand, it is quite difficult to reach subcortical structures with techniques such as TMS, because the impairments caused by single-pulse TMS are usually restricted to cortical areas (Walsh & Cowey, 2000). Furthermore, exact stimulation of the desired area cannot be guaranteed unless fMRI-guided TMS is used (Beauchamp, Nath, & Pasalar, 2010). In summary, for several good reasons, TLE, a neurological disease affecting “emotional” areas, may be considered a good and convenient model to study emotional-processing disturbances and hemispheric dominance.
According to the right-hemisphere model (RHM), the right hemisphere is responsible for the perception, expression, and experience of emotions (Borod, Koff, & Caron, 1983; Gainotti, 1983; Heilman & Bowers, 1990; Wager, Phan, Liberzon, & Taylor, 2003). This has been supported by empirical evidence from both typical individuals and those with brain damage. For instance, emotional faces presented to the left visual field (and, so, initially processed by the right hemisphere) are discriminated better (Landis, Assal, & Perret, 1979) and rated as more intense (Levine & Levy, 1986), as well as eliciting greater autonomic response (Spence, Shapiro, & Zaidel, 1996). Similarly, Benowitz et al. (1983) found that when split-brain patients were presented with facial expression items specifically to each hemisphere separately, they only showed difficulties in FER when the stimuli were presented to the left hemisphere. Studies of individuals with TLE typically report poor FER only in right-lateralized epilepsy (Benuzzi et al., 2004; Bonora et al., 2011; McClelland et al., 2006; Meletti et al., 2009; Meletti, Benuzzi, Nichelli, & Tassinari, 2003a; Meletti, Benuzzi, Rubboli, et al., 2003b).
The research above may, however, be an oversimplification. The valence model (VM) suggests that both hemispheres participate in emotional processing, with their different contributions depending on the emotional valence of the stimulus: Positive emotions are processed by the left hemisphere, and negative emotions by the right (Davidson, 1992; Gur, Skolnick, & Gur, 1994; Silberman & Weingartner, 1986). Like the RHM, the VM is supported by evidence from both typical individuals and those with brain damage. For example, positive emotional faces are recognized faster within the right visual field, while negative faces are recognized faster within the left visual field (Reuter-Lorenz, Givis, & Moscovitch, 1983). However, evidence from individuals with brain damage is not so clear: Impairments in the recognition of positive emotions is not always observed in individuals with left-hemisphere damage (Adolphs, Damasio, Tranel, & Damasio, 1996; Borod et al., 1998). In TLE, the results from FER tasks are mixed, with some studies showing impaired recognition of several negative emotions (i.e., anger, fear, disgust, and sadness; Brierley, Medford, Shaw, & David, 2004; Meletti et al., 2009; Meletti, Benuzzi, Rubboli, et al., 2003b), and others pointing toward a selective impairment of fear recognition only (Adolphs, Tranel, Damasio, & Damasio, 1994; McClelland et al., 2006; Meletti, Benuzzi, Rubboli, et al., 2003b). A single study has also found FER impairments in left-TLE patients (Meletti et al., 2009), which the authors explained in terms of interindividual differences in the strength of emotional-processing lateralization, with some individuals having functions that were less lateralized on the right. One explanation that the authors provided for their results was that impairments in their participants with left-lateralized TLE could have been due to bilateral damage that went undetected by conventional MRI, which had shown unilateral hippocampal sclerosis when other methods, such as PET, had shown bilateral damage (Meletti et al., 2009). However, using this argument, if MRI is not sensitive enough to detect subtle bilateral damage, impairments for patients with right TLE could likewise be caused by undetected left-temporal damage. A further study found that impairment was limited to fear recognition in left TLE (Reynders, Broks, Dickson, Lee, & Turpin, 2005). This last finding, in combination with other studies that have not reported clear-cut differences based on the epileptogenic area lateralization (Benuzzi et al., 2004; Brierley et al., 2004), means that overall, no clear-cut support exists for either the right-hemisphere or the valence model of emotional processing.
On the basis of the divergent findings above, different versions of the VM have been developed (Gainotti, 2012). The approach–withdrawal model (Davidson, 1992), for instance, postulates that anterior prefrontal regions of the left hemisphere mediate approach behaviors, while anterior prefrontal regions of the right hemisphere mediate withdrawal behaviors. Despite similarities between the VM and the approach–withdrawal model, there are also noticeable differences: For instance, in the approach–withdrawal model, anger would be grouped with happiness as an approach behavior, but in VM it would be grouped with other negatively valenced emotions (Demaree et al., 2005).
Even taking into account the new models, recent experimental findings still do not differentiate between the models above, and the evidence often conflicts (Gainotti, 2012). As an alternative, Gainotti suggested that the level of processing (conscious vs. unconscious) might explain these diverse findings, as most studies whose findings oppose the RHM have adopted a cognitive (categorization) task rather than an unconscious perception task; Gainotti concluded that the latter task is right-hemisphere lateralized, owing to a fast subcortical right-hemisphere route for emotion processing (Gainotti, 2012). In contrast, TLE findings supporting the RHM have been obtained through use of categorization tasks that involve the left rather than the right hemisphere (Gainotti, 2012).
The use of low-intensity facial expressions, obtained through the morphing technique, may help to distinguish the role of lateralization and to identify subtle impairments that might be associated with left TLE (Benuzzi et al., 2004; Brierley et al., 2004; Meletti et al., 2009). In other words the greater sensitivity required to recognize morphed stimuli, particularly those of low intensity, might help determine which model is supported by TLE data. The Ekman and Friesen (1976b) pictures series is often used to evaluate FER in TLE and is composed of full-blown emotional expressions. However, previous studies on unimpaired participants have shown the relevance of not using full-blown expressions. When facial emotions are presented at lower intensities, individuals find them more difficult to recognize, limiting ceiling effects (Law Smith, Montagne, Perrett, Gill, & Gallagher, 2010). For example, Hoffmann, Kessler, Eppel, Rukavina, and Traue (2010) failed to show gender differences in unimpaired participants with full-intensity stimuli, while gender differences did emerge when the intensity of the expressions was varied. This use of various facial expression intensities has been applied also to several pathologies, including autism spectrum disorders, resolving the dilemma regarding these participants’ abilities to discriminate basic emotional facial expressions (Law Smith et al., 2010); in Parkinson disease, to clarify differences in disgust perception in medicated and unmedicated participants (Sprengelmeyer et al., 2003); and with similar aims in Alzheimer disease (Spoletini et al., 2008), schizophrenia (Huang et al., 2011), and depression (Anderson et al., 2011).
The main goal of the present study was to explore the role of the lateralization of the epileptogenic area by using facial expression stimuli of varied intensities. A varied-intensity facial expression test was administered to 25 individuals with right-lateralized TLE and 32 with left-lateralized TLE, all of whom were candidates for surgery. The use of morphed facial expression stimuli of different intensities was expected to increase the sensitivity of the test for detecting subtle deficits that may arbitrate between different theories of emotional laterality. In summary, following the RHM predictions, only right-TLE patients would be expected to show impairment across all facial expressions, as that model postulates that the right hemisphere is responsible for the perception, expression, and experience of all emotions (Borod et al., 1983; Gainotti, 1983; Heilman & Bowers, 1990; Wager et al., 2003). Furthermore, previous studies showed that right amygdala damage before 6 years of age results in permanent FER impairments in TLE patients, while a later epilepsy onset leaves FER abilities intact (Hlobil, Rathore, Alexander, Sarma, & Radhakrishnan, 2008; Meletti, Benuzzi, Rubboli, et al., 2003b). This effect, in agreement with the RHM predictions, was also investigated. Previous studies of TLE had not shown totally convincing evidence for the RHM, as they failed to show deficits in the recognition of happiness (Meletti et al., 2009), possibly as a result of ceiling effects due the expressions of happiness being recognized very accurately. For example, Ekman and Friesen (1976a) reported an average accuracy for happiness recognition of 99.2 % in typical participants. Possible ceiling effects for happy FER have also affected testing of the VM, which predicts that right-TLE patients should show impaired recognition of negative emotions, while left-TLE patients should show deficits in recognizing positive emotions. Similarly, reduction in the intensity of happy facial expressions through the use of morphing in the present experiment may make such an effect visible. Finally the approach–withdrawal model predicts specific deficits in disgust, fear, and sadness (avoidance emotions) in right-TLE patients, and in anger and happiness (approach emotions) in left-TLE patients, considering that emotion recognition is accomplished by both temporal and prefrontal regions and that this network might be interrupted by TLE.
Materials and method
Participants
A group of 66 patients diagnosed with drug-resistant TLE (ILAE, C.o.E.a.P., 1993) were selected for the study. Patients were recruited from the “Claudio Munari” Centre for Epilepsy Surgery, Niguarda Ca’ Granda Hospital, Milan, and from the Epilepsy Centre, Neurology II, San Paolo Hospital, University of Milan, Milan. The patients were candidate for surgical treatment of epilepsy on the basis of clinical evaluation, electroencephalographic (EEG) video monitoring, and neuroimaging results. All patients had normal or corrected-to-normal vision and gave informed consent for participating in the study. The experiment was conducted in accordance with the Declaration of Helsinki.
Before being recruited for the experiment, patients underwent a neuropsychological evaluation involving the assessment of language (token test, letter and category fluency test, Boston Naming Test), episodic memory (short-story recall), verbal and nonverbal short-term memory (digit span forward task, Corsi block-tapping task) and memory for faces (Camden Recognition Test), executive functions (trail-making test, attentive matrices), visuospatial processing (Benton Judgment of Line Orientation Test), abstract reasoning (Raven’s Coloured Progressive Matrices), and depression (Beck Depression Inventory [BDI]). Anxiety was assessed via a psychiatric clinical colloquium. Patients performing in the normal range at all of these tasks were recruited for the experiment, so as to avoid mixed results that could be due to cognitive impairments rather than emotional deficits. The inclusion criteria to participate in the study were (1) age between 16 and 70 years; (2) absence of mental deterioration, as confirmed by the neuropsychological testing; (3) preserved perceptual functioning and memory for faces, as evidenced by normal performance on the Benton Judgment of Line Orientation Test and the Camden Recognition Test; (4) preserved executive functions and abstract reasoning, as confirmed by trail-making test, attentive matrices, and Raven’s Coloured Progressive Matrices; (5) absence of dementia (according to the DSM-IV-TR diagnostic criteria for dementia; American Psychiatric Association, 2007), sensory or motor deficits, and psychiatric illness; and (6) absence of mood disorder or suspected depression, as highlighted by the BDI and by the psychiatric assessment. Antiepileptic drugs (AEDs) were not considered as an exclusion criterion, since our patients showed no cognitive side effects due to drug treatment. The patients were tested on average one month prior to surgery. Neuropsychological and FER tests were administered in separate sessions and not during neuroimaging or EEG examinations. Of the 66 patients recruited, ten were excluded due to pathological scores at the neuropsychological tests. Thus, the final sample was composed of 56 individuals (Table 1).
Of these patients, 32 had the focus epilepticus in the left hemisphere, and 24 were lateralized in the right hemisphere (Table 1). The left- and right-side patients did not differ with respect to age [t(54) = 0.945, p = .349], sex (χ 2 = 0.024, p = .876), educational levels (χ 2 = 3.905, p = .272), or Raven’s Coloured Progressive Matrices scores [t(54) = 0.757, p = .453]. Furthermore, we did not find any significant difference in the distributions of epilepsy onset between left- and right-TLE patients (χ 2 = 1.904, p = .593). A group of 54 age- and sex-matched control participants were also recruited from the subject pool of the University of Pavia. These controls were referred on the basis of an absence of previous history of mental illness and completed the Raven’s Coloured Progressive Matrices test to confirm preserved perceptual and executive functioning. As compared to the control group, both right- and left-TLE patients showed no significant differences in their distributions of gender and age (all ps > .05). However, the patient groups showed both fewer years of education (Kruskal–Wallis χ 2 = 42.447, p < .001) and lower scores on the Raven’s Coloured Progressive Matrices (Kruskal–Wallis χ 2 = 13.646, p = .001) than did the controls. Even though patients performed worse than controls on the Raven’s Coloured Progressive Matrices, their performance was still within the normal range, according to the Italian normative values (Caffarra, Vezzadini, Zonato, Copelli, & Venneri, 2003).
Apparatus and procedure
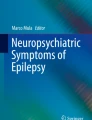
The Animated Full Facial Expression Test–Revised (AFFECT-R) is a computerized test created to investigate facial emotion recognition. The test was modeled on the FER task used by Gagliardi et al. (2003). In the AFFECT-R, five basic facial emotion expressions (fear, disgust, anger, sadness, and happiness), expressed by four individuals (two males and two females) from the Ekman and Friesen (1976b) series are displayed. In the present experiment, the five basic expressions of anger, disgust, fear, happiness, and sadness were displayed at four intensity levels: 35 %, 50 %, 75 %, and 100 % (Fig. 1). The intermediate levels (35 %, 50 %, and 75 %) were obtained using a morphing technique (Benson & Perrett, 1991; Tiddeman, Burt, & Perrett, 2001) that allows for changing (morphing) the neutral into the full-intensity (100 %) expression (software: Psychomorph; Tiddeman et al., 2001). The emotion of surprise was not used, as previous studies had reported that even unimpaired participants frequently mistake this emotion for fear (Rapcsak et al., 2000).

Examples of the AFFECT-R stimuli. From left to right, the different expression intensities for disgust are depicted by one of the male individuals. The first image displays the neutral face (0 % intensity), while the last depicts the full-blown intensity (100 %). The in-between images (35 %, 50 %, and 75 %) display intermediate intensities obtained using the morphing technique
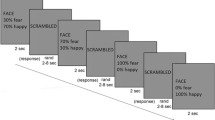
We presented the AFFECT-R on a 15-in. (30 × 23 cm) touch screen (VIDI LCD VL150 C/T, Model “comfort xp,” CA&G ELETTRONICA srl) with a screen resolution of 1,024 × 768 pixels. Pictures had a size of 14.7 cm high and 7.6 cm wide, covering a vertical visual angle of 16.72º. On each trial, one image was shown in the center of the screen, and five labels (corresponding to the emotions presented on the test) were shown below (Fig. 2). With their dominant hand, participants had the task of touching the onscreen label that best represented the emotion depicted. Participants were asked to answer as quickly and accurately as possible, but there was no time limit to complete a trial. The order of the emotion labels was randomized between participants. The participants did not receive any feedback on their performance during the experiment, and accuracy was collected for each trial.

Example of an AFFECT-R trial. The emotional expression is shown in the center of the screen, and the five answer labels (each one corresponding to one of the five emotions presented on the test) are shown below it. Participants had to press the label that best corresponded to the facial expression. Labels were randomized across the experiment
At the beginning of the experiment, participants were presented with five practice trials (one for each emotion) in a random order. During this practice, emotions were expressed at full intensity to familiarize participants with the task. After the practice trials, the participants started with the four experimental blocks of the AFFECT-R, in which they were shown a total of 80 stimuli (16 for each emotion, with four for every intensity level). Blocks were randomized between participants and included 20 stimuli each. The experiment took about 20 min to complete.
Statistics
The data were analyzed using the Statistical Package for Social Sciences (SPSS 13.0; IBM, Chicago, IL). Percentages of correct answers (accuracy; see Table S1 in the supplementary materials for average raw scores) were transformed into z scores in order to normalize the data. FER scores were analyzed using a repeated measures analysis of variance (ANOVA), with Expression (anger, fear, disgust, sadness, and happiness) and Stimulus Intensity (35 %, 50 %, 75 %, and 100 %) as within-subjects factors, and Group (controls and left- and right-TLE patients) as a between-subjects factor. The alpha level was set at .05. Further ANOVAs and post-hoc comparisons (Bonferroni corrected) were then performed according to the main effects and interactions that emerged from the previous analysis.
Finally, to test the “early-onset” hypothesis, we performed Spearman’s rank correlations between age at epilepsy onset (categorical variable) and FER accuracy.
Results
Between-group analysis
The repeated measures ANOVA performed on the percentages of correct answers (Fig. 3; see Table S1 in the supplementary materials for the average raw scores) revealed a significant three-way interaction between emotional category, stimulus intensity, and group [F(24, 1284) = 2,120, p = .001]. No other significant main effects or interactions were found. As the patients and controls had different levels of education, we ran this main analysis again, including education as covariate. This control did not change the results; the three-way interaction was still the only significant finding. Thus, we can conclude that the differences in FER were not due to differences in education.

Percentages of correct answers (accuracy) for each emotion, depicted as a function of display intensity. Bars represent standard errors of the means. Black lines = controls, dotted lines = left-TLE patients, dashed lines = right-TLE patients
To further explore the Emotional Category × Stimulus Intensity × Group interaction, we performed separate ANOVAs for each intensity level with the factors Emotional Category and Group.
We found a significant main effect of group [F(2, 107) = 4,480, p = .014] and no other effects or interactions in the 35 %-intensity display. Post hoc analysis (estimated marginal means comparisons) of the main effect revealed that right-TLE patients performed significantly worse with respect to controls (mean difference: –0.322, p = .014]. Interestingly, no differences between right and left TLE emerged, nor between left TLE and controls (all ps > .05).
At 50 % intensity, a main effect of group [F(2, 107) = 4,480, p = .014] and a strong trend toward significance for the Emotional Category × Group interaction [F(8, 428) = 4,480, p = .059] emerged. Post hoc analysis (estimated marginal means comparisons) of the main effect revealed significantly worse performance for right-TLE patients with respect to controls (mean difference −0.550 p = .003), but no differences between left and right TLE and left TLE and controls (all ps > .05). To explore the interaction between emotional category and group, we performed further ANOVAs for each emotion. These analyses revealed significant differences between groups for disgust [F(2, 107) = 4,179, p = .018], fear [F(2, 107) = 6,136, p = .003], and sadness [F(2, 107) = 6,230, p = .003] recognition. Post hoc comparisons showed that the difference in disgust recognition was driven by significantly worse performance for right-TLE patients as compared to controls (mean difference: –0.678, p = .016). Similarly, right-TLE patients were poorer than controls in recognizing sadness (mean difference: –0.773, p = .004). In contrast, for fear recognition, right-TLE patients differed not only from controls (mean difference: –0.815, p = .002), but also from left-TLE patients (mean difference: –0.649, p = .040), showing that the latter group were better at recognizing this emotion at this intensity.
A main effect of group [F(2, 107) = 11,008, p < .001] and no other effects or interactions were found at the 75 % intensity level. Post hoc analysis (estimated marginal means comparisons) of this effect revealed significantly worse performance of right-TLE patients with respect to controls (mean difference: –0.700, p < .001). Interestingly, here we also found a significant difference between right and left TLE (mean difference: –0.408, p = .046), with right-TLE patients performing worse than their left-TLE counterparts. No differences emerged between left TLE and controls (all ps > .05).
At 100 % intensity, neither group nor emotional category, nor the interaction between these factors, revealed any significant differences (all ps > .05).
In summary, our data clearly showed general compromise in the right-TLE patients, which manifested independent from emotional categories at 35 % and 75 % intensity. In contrast, at 50 % intensity, the difference seems to have also been related to the emotional category. Particularly, we highlighted greater compromise of fear recognition with right TLE as compared to both controls and left TLE. Generally, even with morphed stimuli, participants with left TLE did not show impairments in FER recognition. Finally, no differences were detected for 100 % displays of the stimuli.
Valence analysis
According to the VM, right-TLE patients should show an impairment in recognizing negative emotions, while those with left TLE should show impairment in recognizing positive emotions. The consideration of negative emotions separately in the previous analysis could have masked effects of valence. In an attempt to unmask these effects, we explored the data further by grouping emotional categories into positive (happiness) and negative (averaged answers for anger, fear, disgust, and sadness) emotions (valence). Then we applied a repeated measures ANOVA, with Group, Stimulus Intensity, and Valence as factors. We found a significant main effect of group [F(2, 107) = 5,985, p = .003], which post-hoc tests showed was due to worse performance for right TLE as compared to controls (mean difference: –.417, p = .005). Furthermore, the analysis revealed a significant three-way interaction between group, stimulus intensity, and valence [F(6, 321) = 2,246, p = .047]. Follow-up ANOVAs at each intensity level showed a significant interaction between valence and group only at 50 % intensity [F(2, 107) = 3,365, p = .038]. Further exploration of this interaction revealed that the effect was driven by a significant difference between the groups for negative emotions [F(2, 107) = 6,689, p = .002], explained by worse performance for right-TLE patients with respect to controls (mean difference: –0.636, p = .002).
In summary, the effect of valence emerged only for 50 %-intensity displays and indicated compromise in recognizing negative emotions only in the right-TLE patients.
Approach–withdrawal analysis
The approach–withdrawal model predicts that right-TLE patients should show an impairment in recognizing avoidance emotions, while left-TLE patients should be impaired in recognizing approach emotions. To explore these predictions, we further analyzed the data by grouping emotional categories into avoidance (averaged answers for fear, disgust, and sadness) and approach (averaged answers for anger and happiness) emotions. As in the other analyses, we applied a repeated measures ANOVA with Group, Stimulus Intensity, and Emotional State (approach, withdrawal) as factors.
We found a significant main effect of group [F(2, 107) = 9,484, p < .001], which post-hoc tests showed was due to worse performance for right TLE as compared to controls (mean difference: –0.654, p < .001). Furthermore, this analysis revealed a significant difference between left-TLE patients and controls (mean difference: –0.349, p = .045), but no differences between right- and left-TLE patients (p > .05).
Second, we found a significant two-way interaction between emotional state and group [F(2, 107) = 8,513, p = .001]. A follow-up ANOVA revealed a significant difference in avoidance emotion recognition between groups [F(2, 107) = 11,443, p < .001], driven by worse performance among right-TLE patients, as compared to both controls (mean difference: –1.007, p < .001) and left-TLE patients (mean difference: –0.596, p = .036). Furthermore, we also found a significant difference between groups for approach emotions [F(2, 107) = 3,466, p = .035]. In this case, the difference was driven by a trend toward significance between left-TLE patients and controls (mean difference: –0.287, p = .088).
Finally, the analysis revealed a three-way interaction between group, stimulus intensity, and emotional state [F(6, 321) = 2,950, p = .010]. Follow-up ANOVAs at each intensity level showed a significant interaction between emotional state and group at 50 % intensity [F(2, 107) = 5,810, p = .004], driven by a significant difference for avoidance emotions [F(2, 107) = 7,923, p = .001], explained by the worse performance of right-TLE patients with respect to controls (mean difference: –0.378, p < .001) and a trend toward a significance difference between left-TLE patients and controls (mean difference: –0.755, p = .053). At 75 % intensity, we also found a significant interaction between emotional state and group [F(2, 107) = 7,120, p = .001], explained by a difference between groups for avoidance emotions [F(2, 107) = 13,850, p < .001], with right-TLE patients performing less accurately than either controls (mean difference: –1.302, p < .001) or left-TLE patients (mean difference: –0.730, p = .028). Furthermore, at this intensity, the left-TLE group performed worse than controls when asked to recognize avoidance emotions (mean difference: –0.572, p = .040). Finally, at 100 % intensity, the analysis revealed a significant interaction between emotional state and group [F(2, 107) = 8.851, p < .001], driven by a significant difference between groups for avoidance emotion recognition [F(2, 107) = 10,205, p < .001], with right-TLE patients performing less accurately than controls (mean difference: –1.163, p < .001). Finally, at this intensity, left-TLE patients showed a trend toward a significance difference versus controls, performing worse for avoidance emotions (mean difference: –0.580, p = .052).
In summary, the analysis of the approach–withdrawal model predictions revealed that generally, both the left- and right-TLE groups performed worse than controls. Furthermore, when intensity was kept fixed, right-TLE patients appeared compromised in their avoidance emotion recognition, while left-TLE patients were compromised in approach emotion recognition. However, at 50 % and 100 % intensity, left-TLE patients were also worse than controls at recognizing avoidance emotions. This last finding is not in agreement with the model’s predictions.
Correlation with age at epilepsy onset
Finally, we investigated the correlations between FER and age at epilepsy onset.
We considered overall performance on the FER task, independently from the emotional category and stimulus intensity. No significant correlation emerged for left-TLE patients (n = 32, r = −.015, p > .05), while right-TLE patients showed a significant positive correlation between age at epilepsy onset and FER accuracy (n = 24, r = .610, p = .002). This last finding might indicate that, if age at onset is later in life, FER performance is better. It should be remarked that we did not find significant differences in the onset distributions between left- and right-TLE patients. Thus, our results are unlikely to be due to an influence of the different numbers of participants resulting in later disease onset among the left-TLE patients.
Taken together, our results confirm that age at onset influences right- but not left-TLE patients’ performance, in agreement with previous findings (Hlobil et al., 2008; Meletti, Benuzzi, Rubboli, et al., 2003b).
Discussion
Facial expression recognition has often been investigated in patients with temporal lobe epilepsy (Boucsein, Weniger, Mursch, Steinhoff, & Irle, 2001; Fowler et al., 2006; Golouboff et al., 2008; Hlobil et al., 2008; Meletti et al., 2009; Meletti, Benuzzi, Rubboli, et al., 2003b), but there has been no agreement as to whether FER impairments are greater only in right TLE (Benuzzi et al., 2004; Bonora et al., 2011; McClelland et al., 2006; Meletti et al., 2009; Meletti, Benuzzi, Nichelli, & Tassinari, 2003a; Meletti, Benuzzi, Rubboli, et al., 2003b), or whether left TLE is also characterized by FER deficits (Meletti et al., 2009; Reynders et al., 2005). Here, rather than use only full-intensity faces (Ekman & Friesen, 1976b), we displayed facial expressions of different intensities in order to clarify the role of epilepsy lateralization in FER. The anatomical lateralization in TLE is normally clear, making TLE a suitable model for exploring hemispheric dominance in emotional processing, which may in turn clarify whether emotional processing is predominantly associated with the right hemisphere (RHM; Borod et al., 1983; Heilman & Bowers, 1990; Wager et al., 2003), or whether bihemispheric contributions to emotion recognition depend on the stimulus valence (VM; Davidson, 1992; Gur et al., 1994; Silberman & Weingartner, 1986).
Through the use of more sensitive graded stimuli, we found that only right-TLE patients showed FER impairments that were independent of emotional category. Age at epilepsy onset was also found to impact FER, in right-TLE patients only, supporting the “early-onset” hypothesis, which suggests that right amygdala damage before 6 years of age results in permanent FER impairments (Hlobil et al., 2008; McClelland et al., 2006; Meletti et al., 2009; Meletti, Benuzzi, Nichelli, & Tassinari, 2003a), preventing functional cerebral reorganization and the development of an appropriate FER system (McClelland et al., 2006; Meletti et al., 2009). Even using stimuli of various intensities, we found that age at epilepsy onset seems to be associated with right-TLE patients’ performance only. These results are in agreement with the hypothesis that right temporal structures diffusely modulate different emotions (Adolphs, 2010; Fusar-Poli, Placentino, Carletti, Landi, et al., 2009b). Considering the RHM predictions, we confirmed that only right-TLE patients show impairment. Furthermore, this impairment concerns all emotional categories, congruent with the postulate that the right hemisphere is responsible for all emotions (Borod et al., 1983; Gainotti, 1983; Heilman & Bowers, 1990; Wager et al., 2003)
However, at 50 % intensity, we found greater compromise of fear recognition in right TLE with respect to both controls and left TLE, in agreement with previous studies that have highlighted an impairment of fear recognition (Adolphs et al., 1994; McClelland et al., 2006; Meletti, Benuzzi, Rubboli, et al., 2003). Furthermore, at this intensity, the observed deficit concerned only fear, sadness, and disgust. Considering also the analysis of valence, our results are partly in agreement with studies showing impaired recognition of negative emotions (i.e., anger, fear, disgust, and sadness) in TLE (Brierley et al., 2004; Meletti et al., 2009; Meletti, Benuzzi, Rubboli, et al., 2003), and generally more in agreement with the idea that right temporal structures have a special role for negative stimuli (Davidson, 1992; Gur et al., 1994; Silberman & Weingartner, 1986). These results partly confirm the VM, according to which right-TLE patients should show an impairment in recognizing negative emotions. However, even using more sensitive stimuli, we were not able to detect positive-emotion impairments in left TLE.
Furthermore, the results at 50 % intensity also offer partial support for the approach–withdrawal model, which postulates a specific deficit in disgust, fear, and sadness (avoidance emotions) in right-TLE patients. The separate analysis for this model’s predictions further confirmed its validity, with a clear impairment in avoidance emotion recognition when the right hemisphere was compromised, and an impairment for approach emotions when the left hemisphere was involved. However, the evidence for approach emotions and for the left hemisphere was generally less strong, as when we considered intensities separately, at 50 % and 75 % those with left TLE appeared to be impaired for avoidance emotions as well. This last finding contradicts the approach–withdrawal model, and does not fit with the other model predictions, either.
It should be noted that we employed only one positive emotion, in order to obtain results comparable to those from previous studies using the Ekman and Friesen series, but the use of only one positive emotion might put in question the generalizability of the results for positive emotions. Recent studies investigating happiness recognition have highlighted an advantage for happy faces as compared to other facial expressions (Calvo & Lundqvist, 2008; Calvo, Nummenma, & Avero, 2010). Furthermore, it seems possible that, at a basic level, there is only one positive emotion—happiness—making happiness recognition a simpler task than recognizing specific negative emotions (Adolphs et al., 1996). It should be considered that virtually all happy faces contain some variant of the stereotypic signal of this emotion, the smile (Adolphs et al., 1996). Nevertheless, other studies in TLE using happiness as the only positive emotion have been able to highlight effects (Hlobil et al., 2008), and our results, at least for low intensities, were not at ceiling. Thus, it seems unlikely that our findings are due to the use of happiness only.
Finally, the absence of significant differences for 100 % intensity is coherent with previous results showing a lack of differences based on the epileptogenic area lateralization (Benuzzi et al., 2004; Brierley et al., 2004). This result, in particular, might indicate that in some cases full displays of emotions are not sensitive enough to assess impairments, further corroborating the hypothesis that more difficult stimuli are needed.
A recent meta-analysis considered emotional face processing in unimpaired participants (Fusar-Poli, Placentino, Carletti, Allen, et al., 2009a). This work, performed on 105 studies that mainly used the Ekman and Friesen series, highlights that the brain networks for facial emotional processing might be far more complex than is indicated by the RHM, the VM, or the approach–withdrawal model, as the recognition of emotional faces seems to involve bilateral, widespread areas that include not only the limbic system, but also the prefrontal and visual cortex (Fusar-Poli, Placentino, Carletti, Allen, et al., 2009a). Moreover, these findings support the idea that the bilateral activation of some structures, such as the amygdala, might indicate multistep processing during the decoding of emotional expressions (Adolphs, 2002a; Fusar-Poli, Placentino, Carletti, Allen, et al., 2009a; Glascher, Tuscher, Weiller, & Buchel, 2004; Vuilleumier, Richardson, Armony, Driver, & Dolan, 2004). According to this hypothesis, the right amygdala might be activated automatically by arousing stimuli, in a relatively global emotional reaction, while the left amygdala could be involved in a more detailed and cognitive information-processing step aimed at decoding emotional valence and magnitude (Adolphs, 2002b; Glascher et al., 2004). Our results are partly in agreement with this hypothesis, as we found that more general impairment was restricted to right patients only. However, given the difficulty of the stimuli—for instance, at 35 % intensity—we could not confirm the role of the left amygdala in a more detailed, cognitive information-processing step. Rather, considering a multistep model, it might be that the impairment in right structures is enough to preclude even later steps in processing, preventing a compensation from the left structures and the activation of subsequent stations of the emotional network. Interestingly, the same voxel-based meta-analysis also showed that disgust recognition is processed in right subcortical and cortical structures (Fusar-Poli, Placentino, Carletti, Landi, et al., 2009b). This finding is in line with the compromising of this negative emotion that we found in right-TLE patients. Particularly, it has been pointed out in several studies that disgust is processed by the insula (Phillips et al., 1998; Phillips et al., 1997; Sprengelmeyer et al., 1996), and depth-electrode studies performed in epilepsy patients have further suggested that the crucial area of this structure is the ventral anterior part (Krolak-Salmon et al., 2003). Disgust is postulated to be different from other emotions, such as fear. A possible explanation for these differences, such as the later temporal responses found in event-related potential studies (Krolak-Salmon et al., 2003), is that disgust has a different evolutionary meaning, being characterized by a broader conceptual knowledge related to moral disgust (a more cognitive component), and not only by a primitive and arousing environmental reaction (Krolak-Salmon et al., 2003; Rozin & Fallon, 1987). Moreover, the insula has extensive anatomical connections with temporal areas, such as the amygdala and hippocampus, and several studies have pointed out its implication in TLE epileptic pathology (Schwartz, 2005). Even though still no data are available to precisely compare the roles of the right and the left insula (Krolak-Salmon et al., 2003), it seems from our results that the right insula might be more involved in disgust processing than is the left. However, our data should be considered cautiously, as we cannot establish the degree to which the insula may have been involved in the patient group used in our study, and further studies on TLE could directly address this hypothesis.
A different explanation proposed for the contributions of the two hemispheres to emotional processing is that conscious and unconscious aspects of emotional processing could be mediated differently by the two hemispheres, with the right hemisphere being more involved in unconscious and the left hemisphere in conscious emotional processing (Gainotti, 2012). However, our results, similarly to those of previous studies (Meletti, Benuzzi, Rubboli, et al., 2003b), seem to suggest that the right hemisphere also plays an important role in explicit emotional processing. Furthermore, as we adopted a task in which participants were required to choose the correct label for an emotion without time constraints, our results are not in agreement with the idea that the left hemisphere is concerned with categorization or cognitive tasks using emotional materials, whereas rapid-detection tasks would imply the right hemisphere (Gainotti, 2012). However, as we did not adopt both kinds of task, we cannot completely rule out the possibility of a difference between left- and right-hemisphere contributions based on the task. Further studies could directly compare tasks (categorization/detection) and types of processing (conscious/unconscious) in TLE, to clarify this alternative hypothesis on hemispheric specialization. Finally, as we modeled our FER task on the basis of previously used protocols (Meletti et al., 2009; Meletti, Benuzzi, Rubboli, et al., 2003b), we adopted a forced choice procedure in which participants did not have the possibility to choose a “neutral” answer. This might be an important task issue, as in other domains it has been demonstrated that differences in patients’ performance can arise from using different response criteria during clinical and forced choice tests (Azzopardi & Cowey, 1998). Future studies could explore whether using a different procedure—allowing participants to answer that they do not see any emotion—might produce diverse results.
Even though the evidence from our data seems to provide stronger support for the RHM, the partial support that we also found for the VM and the approach–withdrawal model suggests that to understand emotional lateralization and formulate exhaustive models, researchers should consider more widespread brain networks (Vuilleumier et al., 2004), evaluate both conscious and unconscious processing (Gainotti, 2012), and adopt stimuli of diverse arousals, valences, and difficulties (Demaree et al., 2005). In our study, which was not aimed at directly comparing emotional dimensions, we nevertheless were able to describe mixed results. Furthermore, the most interesting findings were derived from stimuli at 50 % intensity. Thus, a comprehensive model should also be able to explain the relationship between these different components of emotional processing, rather than considering them in isolation, and in order to reach this goal, the study of emotional processing in TLE, which has usually been performed to shed light on the issue of emotional lateralization, should make use of more sensitive experimental paradigms (Vuilleumier et al., 2004) that take into account new models of the hemispheric contributions to emotional processing. While previous studies mainly adopted full-intensity displays, in this experiment we used different stimulus intensities that have been demonstrated to be more effective. Morphed stimuli are more sensitive in detecting subtle impairments, gender differences. (Hoffmann et al., 2010; Law Smith et al., 2010). Future studies on FER in TLE could benefit from adopting more varied expressions. Particularly, our speculation is that TLE, instead of confirming the RHM or the VM, points toward the possibility of alternative and more comprehensive models of emotional lateralization that will also take into account the multistep nature of this function.
References
Adolphs, R. (2002a). Neural systems for recognizing emotion. Current Opinion in Neurobiology, 12, 169–177.
Adolphs, R. (2002b). Recognizing emotion from facial expressions: Psychological and neurological mechanisms. Behavioral and Cognitive Neuroscience Reviews, 1, 21–62. doi:10.1177/1534582302001001003
Adolphs, R. (2010). What does the amygdala contribute to social cognition? Annals of the New York Academy of Sciences, 1191, 42–61.
Adolphs, R., Damasio, H., Tranel, D., & Damasio, A. R. (1996). Cortical systems for the recognition of emotion in facial expressions. Journal of Neuroscience, 16, 7678–7687.
Adolphs, R., Tranel, D., Damasio, H., & Damasio, A. (1994). Impaired recognition of emotion in facial expressions following bilateral damage to the human amygdala. Nature, 372, 669–672.
American Psychiatric Association. (2007). DSM-IV-TR: Manuale diagnostico e statistico dei disturbi mentali. Text revision (4th ed.). Amsterdam, The Netherlands: Elsevier.
Anderson, I. M., Shippen, C., Juhasz, G., Chase, D., Thomas, E., Downey, D.,… Deakin, J. F. (2011). State-dependent alteration in face emotion recognition in depression. British Journal of Psychiatry, 198, 302–308.
Azzopardi, P., & Cowey, A. (1998). Blindsight and visual awareness. Consciousness and Cognition, 7, 292–311.
Beauchamp, M. S., Nath, A. R., & Pasalar, S. (2010). fMRI-guided transcranial magnetic stimulation reveals that the superior temporal sulcus is a cortical locus of the McGurk effect. Journal of Neuroscience, 30, 2414–2417.
Benowitz, L. I., Bear, D. M., Rosenthal, R., Mesulam, M. M., Zaidel, E., & Sperry, R. W. (1983). Hemispheric specialization in nonverbal communication. Cortex, 19, 5–11.
Benson, P. J., & Perrett, D. I. (1991). Computer averaging and manipulation of faces. In P. Wombell (Ed.), Photovideo: Photography in the age of the computer (pp. 32–38). London, UK: Rivers Oram Press.
Benuzzi, F., Meletti, S., Zamboni, G., Calandra-Buonaura, G., Serafini, M., Lui, F.,… Nichelli, P. (2004). Impaired fear processing in right mesial temporal sclerosis: A fMRI study. Brain Research Bulletin, 63, 269–281.
Bonora, A., Benuzzi, F., Monti, G., Mirandola, L., Pugnaghi, M., Nichelli, P., et al. (2011). Recognition of emotions from faces and voices in medial temporal lobe epilepsy. Epilepsy and Behaviour, 20, 648–654.
Borod, J. C., Cicero, B. A., Obler, L. K., Welkowitz, J., Erhan, H. M., Santschi, C.,… Whalen, J. R. (1998). Right hemisphere emotional perception: Evidence across multiple channels. Neuropsychology, 12, 446–458.
Borod, J. C., Koff, E., & Caron, H. (1983). Right hemispheric specialization for the expression and appreciation of emotion: A focus on the face. In E. Perecman (Ed.), Cognitive processing in the right hemisphere (pp. 83–110). New York, NY: Academic Press.
Boucsein, K., Weniger, G., Mursch, K., Steinhoff, B. J., & Irle, E. (2001). Amygdala lesion in temporal lobe epilepsy subjects impairs associative learning of emotional facial expressions. Neuropsychologia, 39, 231–236.
Brierley, B., Medford, N., Shaw, P., & David, A. S. (2004). Emotional memory and perception in temporal lobectomy patients with amygdala damage. Journal of Neurology, Neurosurgery & Psychiatry, 75, 593–599.
Caffarra, P., Vezzadini, G., Zonato, F., Copelli, S., & Venneri, A. (2003). A normative study of a shorter version of Raven’s Progressive Matrices 1938. Neurological Sciences, 24, 336–339.
Calvo, M. G., & Lundqvist, D. (2008). Facial expressions of emotion (KDEF): Identification under different display-duration conditions. Behavior Research Methods, 40, 109–115. doi:10.3758/BRM.40.1.109
Calvo, M. G., Nummenma, L., & Avero, P. (2010). Recognition advantage of happy faces in extrafoveal vision: Featural and affective processing. Visual Cognition, 18, 1274–1297.
Chemerinski, E., & Robinson, R. G. (2000). The neuropsychiatry of stroke. Psychosomatics, 41, 5–14.
Davidson, R. J. (1992). Anterior cerebral asymmetry and the nature of emotion. Brain and Cognition, 20, 125–151.
de Freitas, G. R. (2012). Aphasia and other language disorders. Frontiers in Neurology and Neuroscience, 30, 41–45.
Demaree, H. A., Everhart, D. E., Youngstrom, E. A., & Harrison, D. W. (2005). Brain lateralization of emotional processing: Historical roots and a future incorporating “dominance. Behavioral and Cognitive Neuroscience Reviews, 4, 3–20.
Ekman, P., & Friesen, W. (1976a). Measuring facial movements. Environmental Psychology and Nonverbal Behaviour, 1(1).
Ekman, P., & Friesen, W. V. (1976b). Pictures of facial affect. Palo Alto, CA: Consulting Psychologists Press.
Ferro, J. M. (2001). Hyperacute cognitive stroke syndromes. Journal of Neurology, 248, 841–849.
Fowler, H. L., Baker, G. A., Tipples, J., Hare, D. J., Keller, S., Chadwick, D. W., et al. (2006). Recognition of emotion with temporal lobe epilepsy and asymmetrical amygdala damage. Epilepsy and Behaviour, 9, 164–172.
Fusar-Poli, P., Placentino, A., Carletti, F., Allen, P., Landi, P., Abbamonte, M.,… Politi, P. L. (2009). Laterality effect on emotional faces processing: ALE meta-analysis of evidence. Neuroscience Letters, 452, 262–267. doi:10.1016/j.neulet.2009.01.065
Fusar-Poli, P., Placentino, A., Carletti, F., Landi, P., Allen, P., Surguladze, S.,… Politi, P. (2009). Functional atlas of emotional faces processing: A voxel-based meta-analysis of 105 functional magnetic resonance imaging studies. Journal of Psychiatry and Neuroscience, 34, 418–432.
Gagliardi, C., Frigerio, E., Burt, D. M., Cazzaniga, I., Perrett, D. I., & Borgatti, R. (2003). Facial expression recognition in Williams syndrome. Neuropsychologia, 41, 733–738.
Gainotti, G. (1983). Emotions and hemispheric lateralization: Review of the literature. Encephale, 9, 345–364.
Gainotti, G. (2012). Unconscious processing of emotions and the right hemisphere. Neuropsychologia, 50, 205–218. doi:10.1016/j.neuropsychologia.2011.12.005
Glascher, J., Tuscher, O., Weiller, C., & Buchel, C. (2004). Elevated responses to constant facial emotions in different faces in the human amygdala: An fMRI study of facial identity and expression. BMC Neuroscience, 5, 45.
Golouboff, N., Fiori, N., Delalande, O., Fohlen, M., Dellatolas, G., & Jambaque, I. (2008). Impaired facial expression recognition in children with temporal lobe epilepsy: Impact of early seizure onset on fear recognition. Neuropsychologia, 46, 1415–1428.
Gur, R. C., Skolnick, B. E., & Gur, R. E. (1994). Effects of emotional discrimination tasks on cerebral blood flow: Regional activation and its relation to performance. Brain and Cognition, 25, 271–286.
Haxby, J. V., Hoffman, E. A., & Gobbini, M. I. (2000). The distributed human neural system for face perception. Trends in Cognitive Sciences, 4, 223–233.
Heilman, K. M., & Bowers, D. (1990). Neuropsychological studies of emotional changes induced by right and left hemispheric lesions. In N. L. Stein, B. Leventhal, & T. Trabasso (Eds.), Psychological and biological approaches to emotion (pp. 97–114). Hillsdale, NJ: Erlbaum.
Hlobil, U., Rathore, C., Alexander, A., Sarma, S., & Radhakrishnan, K. (2008). Impaired facial emotion recognition in patients with mesial temporal lobe epilepsy associated with hippocampal sclerosis (MTLE-HS): Side and age at onset matters. Epilepsy Research, 80, 150–157.
Hoffmann, H., Kessler, H., Eppel, T., Rukavina, S., & Traue, H. C. (2010). Expression intensity, gender and facial emotion recognition: Women recognize only subtle facial emotions better than men. Acta Psychologica, 135, 278–283. doi:10.1016/j.actpsy.2010.07.012
Huang, J., Chan, R. C. K., Gollan, J. K., Liu, W., Ma, Z., Li, Z., et al. (2011). Perceptual bias of patients with schizophrenia in morphed facial expression. Psychiatry Research, 185, 60–65.
ILAE, C.o.E.a.P. (1993). Guidelines for epidemiologic studies on epilepsy. Epilepsia, 34, 592–596.
Krolak-Salmon, P., Henaff, M. A., Isnard, J., Tallon-Baudry, C., Guenot, M., Vighetto, A.,… Mauguiere, F. (2003). An attention modulated response to disgust in human ventral anterior insula. Annals of Neurology, 53, 446–453.
Landis, T., Assal, G., & Perret, E. (1979). Opposite cerebral hemispheric superiorities for visual associative processing of emotional facial expressions and objects. Nature, 278, 739–740.
Law Smith, M. J., Montagne, B., Perrett, D. I., Gill, M., & Gallagher, L. (2010). Detecting subtle facial emotion recognition deficits in high-functioning autism using dynamic stimuli of varying intensities. Neuropsychologia, 48, 2777–2781.
Levine, S. C., & Levy, J. (1986). Perceptual asymmetry for chimeric faces across the life span. Brain and Cognition, 5, 291–306.
McClelland, S., III, Garcia, R. E., Peraza, D. M., Shih, T. T., Hirsch, L. J., Hirsch, J., et al. (2006). Facial emotion recognition after curative nondominant temporal lobectomy in patients with mesial temporal sclerosis. Epilepsia, 47, 1337–1342.
Meletti, S., Benuzzi, F., Cantalupo, G., Rubboli, G., Tassinari, C. A., & Nichelli, P. (2009). Facial emotion recognition impairment in chronic temporal lobe epilepsy. Epilepsia, 50, 1547–1559.
Meletti, S., Benuzzi, F., Nichelli, P., & Tassinari, C. A. (2003a). Damage to the right hippocampal–amygdala formation during early infancy and recognition of fearful faces: Neuropsychological and fMRI evidence in subjects with temporal lobe epilepsy. Annals of the New York Academy of Sciences, 1000, 385–388.
Meletti, S., Benuzzi, F., Rubboli, G., Cantalupo, G., Stanzani Maserati, M., Nichelli, P., et al. (2003b). Impaired facial emotion recognition in early-onset right mesial temporal lobe epilepsy. Neurology, 60, 426–431.
Olson, I. R., Plotzker, A., & Ezzyat, Y. (2007). The enigmatic temporal pole: A review of findings on social and emotional processing. Brain, 130, 1718–1731.
Phillips, M. L., Young, A. W., Scott, S. K., Calder, A. J., Andrew, C., Giampietro, V.,… Gray, J. A. (1998). Neural responses to facial and vocal expressions of fear and disgust. Proceedings of the Royal Society B, 265, 1809–1817.
Phillips, M. L., Young, A. W., Senior, C., Brammer, M., Andrew, C., Calder, A. J.,… David, A. S. (1997). A specific neural substrate for perceiving facial expressions of disgust. Nature, 389, 495–498.
Rapcsak, S. Z., Galper, S. R., Comer, J. F., Reminger, S. L., Nielsen, L., Kaszniak, A. W.,… Cohen, R. A. (2000). Fear recognition deficits after focal brain damage: A cautionary note. Neurology, 54, 575–581.
Reuter-Lorenz, P. A., Givis, R. P., & Moscovitch, M. (1983). Hemispheric specialization and the perception of emotion: Evidence from right-handers and from inverted and non-inverted left-handers. Neuropsychologia, 21, 687–692.
Reynders, H. J., Broks, P., Dickson, J. M., Lee, C. E., & Turpin, G. (2005). Investigation of social and emotion information processing in temporal lobe epilepsy with ictal fear. Epilepsy and Behaviour, 7, 419–429.
Rozin, P., & Fallon, A. E. (1987). A perspective on disgust. Psychological Review, 94, 23–41.
Schwartz, T. H. (2005). Insular seizures: Have we been missing the boat? Epilepsy Currents, 5, 147–148.
Silberman, E. K., & Weingartner, H. (1986). Hemispheric lateralization of functions related to emotion. Brain and Cognition, 5, 322–353.
Spence, S., Shapiro, D., & Zaidel, E. (1996). The role of the right hemisphere in the physiological and cognitive components of emotional processing. Psychophysiology, 33, 112–122.
Spoletini, I., Marra, C., Di Iulio, F., Gianni, W., Sancesario, G., Giubilei, F.,… Spalletta, G. (2008). Facial emotion recognition deficit in amnestic mild cognitive impairment and Alzheimer disease. American Journal of Geriatric Psychiatry, 16, 389–398.
Sprengelmeyer, R., Young, A. W., Calder, A. J., Karnat, A., Lange, H., Homberg, V.,… Rowland, D. (1996). Loss of disgust. Perception of faces and emotions in Huntington’s disease. Brain, 119, 1647–1665.
Sprengelmeyer, R., Young, A. W., Mahn, K., Schroeder, U., Woitalla, D., Buttner, T.,… Przuntek, H. (2003). Facial expression recognition in people with medicated and unmedicated Parkinson’s disease. Neuropsychologia, 41, 1047–1057.
Tiddeman, B., Burt, D., & Perrett, D. (2001). Computer graphics in facial perception research. IEEE Computer Graphics and Applications, 21, 42–50.
Vuilleumier, P., Richardson, M. P., Armony, J. L., Driver, J., & Dolan, R. J. (2004). Distant influences of amygdala lesion on visual cortical activation during emotional face processing. Nature Neuroscience, 7, 1271–1278.
Wager, T. D., Phan, K. L., Liberzon, I., & Taylor, S. F. (2003). Valence, gender, and lateralization of functional brain anatomy in emotion: A meta-analysis of findings from neuroimaging. NeuroImage, 19, 513–531.
Walsh, V., & Cowey, A. (2000). Transcranial magnetic stimulation and cognitive neuroscience. Nature Reviews Neuroscience, 1, 73–79.
Author note
The first and second authors contributed equally to this work. A.S. was partially supported by QUALIA, the Associazione per la Ricerca Teorica e Applicata in Scienze Cognitive. None of the authors has any conflict of interest to disclose. We confirm that we have read the journal’s position on issues involved in ethical publication, and affirm that this report is consistent with those guidelines.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 77 kb)
Rights and permissions
About this article
Cite this article
Sedda, A., Rivolta, D., Scarpa, P. et al. Ambiguous emotion recognition in temporal lobe epilepsy: The role of expression intensity. Cogn Affect Behav Neurosci 13, 452–463 (2013). https://doi.org/10.3758/s13415-013-0153-y
Published:
Issue Date:
DOI: https://doi.org/10.3758/s13415-013-0153-y