
Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study—The COViNEPH Project

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
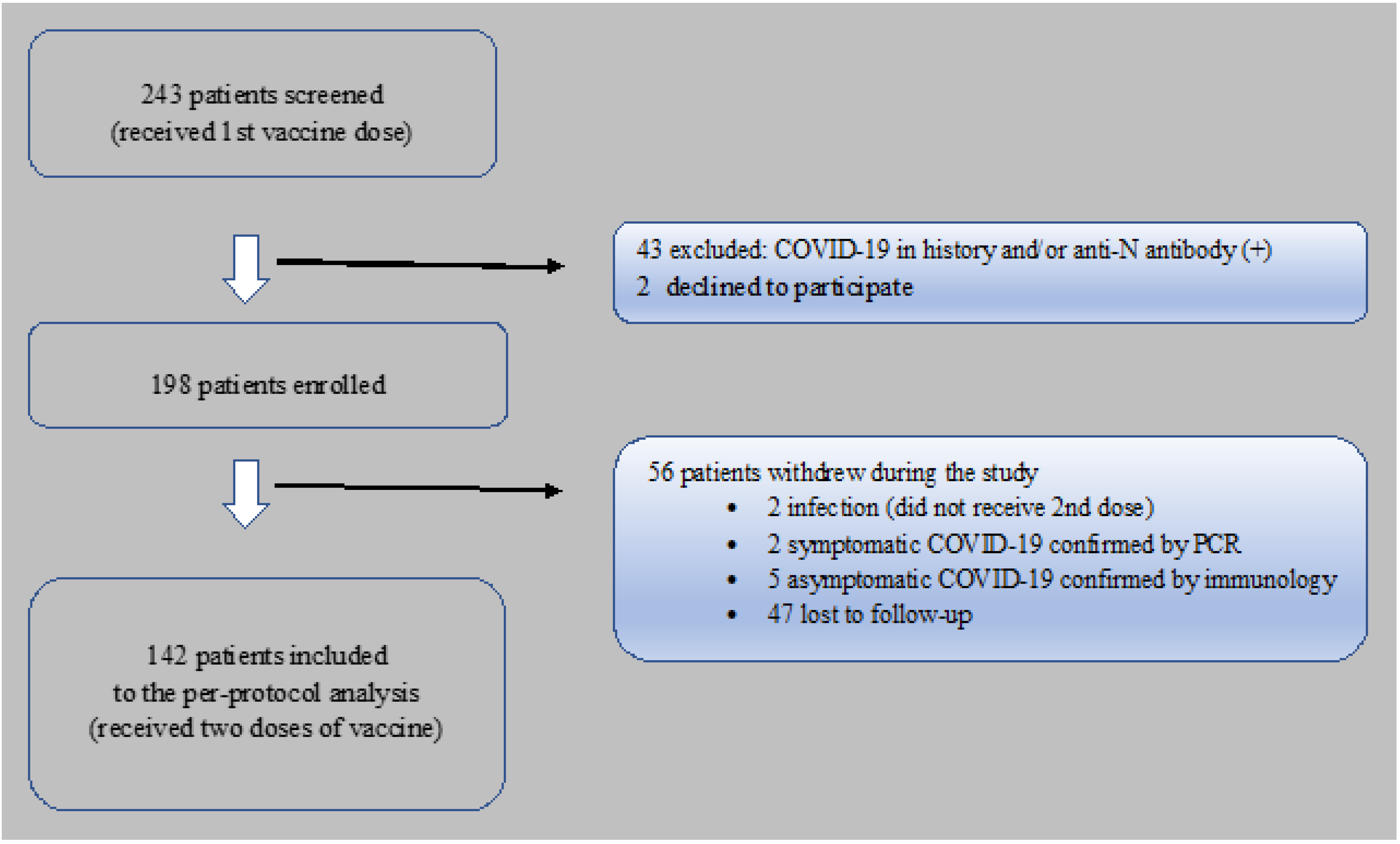
2.1. Study Design
2.2. Anti-SARS-CoV-2 Antibodies Measurement
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristic
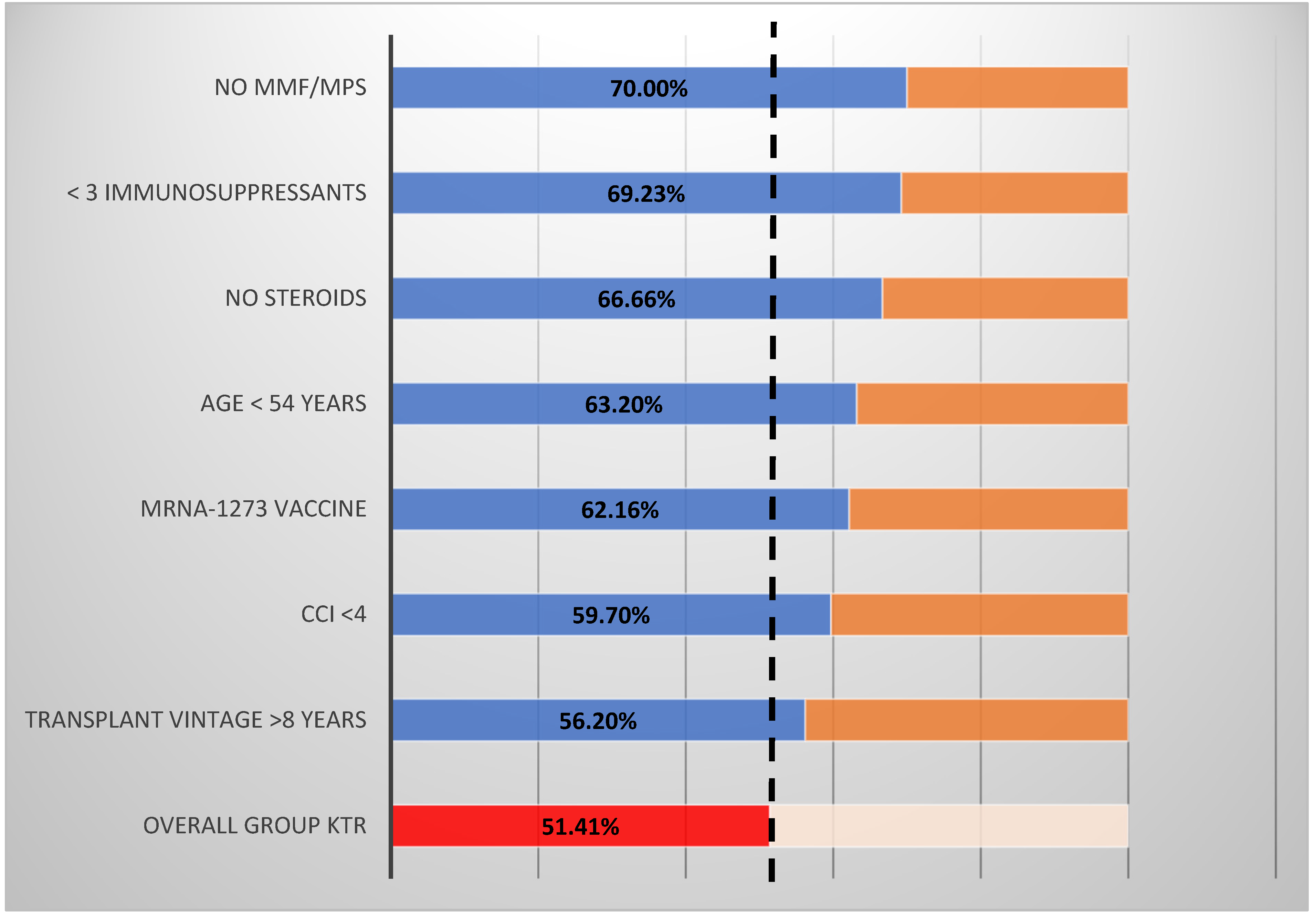
3.2. Seroconversion in Anti-s IgG Antibodies
3.3. Determinants of The Seroconversion in Anti-s IgG Antibodies in KTR
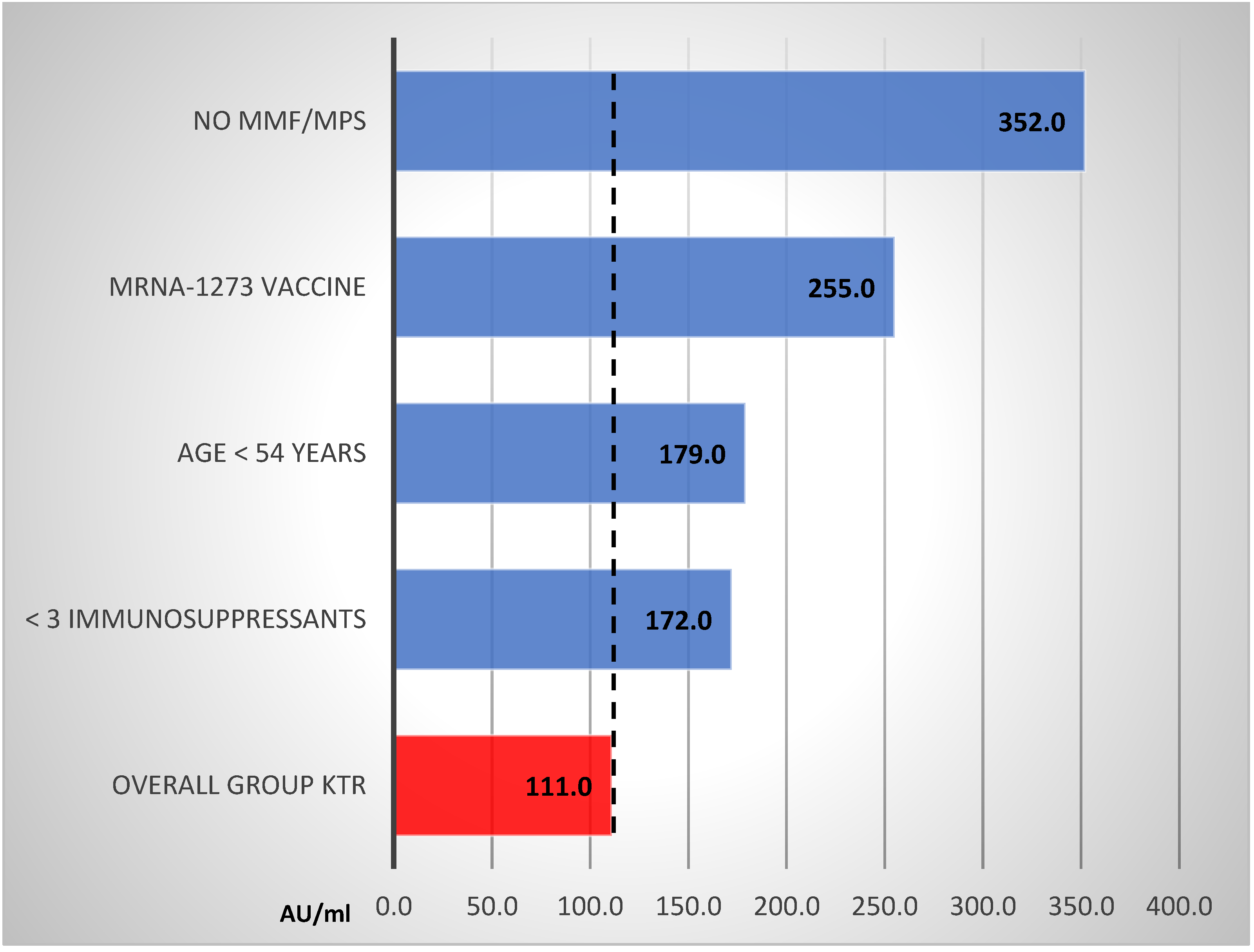
3.4. Determinants of Anti-s IgG Titer Magnitude in KTR Responders
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Azzi, Y.; Bartash, R.; Scalea, J.; Loarte-Campos, P.; Akalin, E. COVID-19 and Solid Organ Transplantation: A Review Article. Transplantation 2021, 105, 37–55. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Tylicki, L.; Biedunkiewicz, B.; Dąbrowska, M.; Ślizień, W.; Tylicki, P.; Polewska, K.; Rosenberg, I.; Rodak, S.; Dębska-Ślizień, A. Humoral response to SARS-CoV-2 vaccination promises to improve the catastrophic prognosis of hemodialysis patients as a result of COVID-19. The COViNEPH Project. Pol. Arch. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Tylicki, L.; Piotrowska, M.; Biedunkiewicz, B.; Zieliński, M.; Dąbrowska, M.; Tylicki, P.; Polewska, K.; Trzonkowski, P.; Lichodziejewska-Niemierko, M.; Dębska-Ślizień, A. Humoral response to the vaccination against COVID-19 in peritoneal dialysis patients. The COViNEPH Project. Pol. Arch. Intern. Med. 2021. [Google Scholar] [CrossRef]
- Benotmane, I.; Gautier-Vargas, G.; Cognard, N.; Olagne, J.; Heibel, F.; Braun-Parvez, L.; Martzloff, J.; Perrin, P.; Moulin, B.; Fafi-Kremer, S.; et al. Low immunization rates among kidney transplant recipients who received 2 doses of the mRNA-1273 SARS-CoV-2 vaccine. Kidney Int. 2021, 99, 1498–1500. [Google Scholar] [CrossRef]
- Grupper, A.; Katchman, H. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus: Not alarming, but should be taken gravely. Am. J. Transplant 2021. [Google Scholar] [CrossRef]
- Hou, Y.C.; Lu, K.C.; Kuo, K.L. The Efficacy of COVID-19 Vaccines in Chronic Kidney Disease and Kidney Transplantation Patients: A Narrative Review. Vaccines 2021, 9, 885. [Google Scholar] [CrossRef]
- Aslam, S.; Danziger-Isakov, L.; Mehra, M.R. COVID-19 vaccination immune paresis in heart and lung transplantation. J. Heart Lung Transpl. 2021, 40, 763–766. [Google Scholar] [CrossRef]
- Narasimhan, M.; Mahimainathan, L.; Clark, A.E.; Usmani, A.; Cao, J.; Araj, E.; Torres, F.; Sarode, R.; Kaza, V.; Lacelle, C.; et al. Serological Response in Lung Transplant Recipients after Two Doses of SARS-CoV-2 mRNA Vaccines. Vaccines 2021, 9, 708. [Google Scholar] [CrossRef]
- Rashidi-Alavijeh, J.; Frey, A.; Passenberg, M.; Korth, J.; Zmudzinski, J.; Anastasiou, O.E.; Saner, F.H.; Jahn, M.; Lange, C.M.; Willuweit, K. Humoral Response to SARS-CoV-2 Vaccination in Liver Transplant Recipients-A Single-Center Experience. Vaccines 2021, 9, 738. [Google Scholar] [CrossRef]
- Stumpf, J.; Siepmann, T.; Lindner, T.; Karger, C.; Schwobel, J.; Anders, L.; Faulhaber-Walter, R.; Schewe, J.; Martin, H.; Schirutschke, H.; et al. Humoral and cellular immunity to SARS-CoV-2 vaccination in renal transplant versus dialysis patients: A prospective, multicenter observational study using mRNA-1273 or BNT162b2 mRNA vaccine. Lancet. Reg. Health Eur. 2021, 100178. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Immunogenicity of a Single Dose of SARS-CoV-2 Messenger RNA Vaccine in Solid Organ Transplant Recipients. JAMA 2021, 325, 1784–1786. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Campbell, P.; Hoschler, K.; Hidalgo, L.; Al-Dabbagh, M.; Wilson, L.; Humar, A. Randomized Controlled Trial of Adjuvanted Versus Nonadjuvanted Influenza Vaccine in Kidney Transplant Recipients. Transplantation 2016, 100, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Chadban, S.J.; Ahn, C.; Axelrod, D.A.; Foster, B.J.; Kasiske, B.L.; Kher, V.; Kumar, D.; Oberbauer, R.; Pascual, J.; Pilmore, H.L.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Management of Candidates for Kidney Transplantation. Transplantation 2020, 104, S11–S103. [Google Scholar] [CrossRef]
- Stock, P.G.; Henrich, T.J.; Segev, D.L.; Werbel, W.A. Interpreting and addressing suboptimal immune responses after COVID-19 vaccination in solid-organ transplant recipients. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Firket, L.; Descy, J.; Seidel, L.; Bonvoisin, C.; Bouquegneau, A.; Grosch, S.; Jouret, F.; Weekers, L. Serological response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients depends on prior exposure to SARS-CoV-2. Am. J. Transpl. 2021. [Google Scholar] [CrossRef]
- Heldman, M.R.; Limaye, A.P. SARS-CoV-2 Vaccines in Kidney Transplant Recipients: Will They Be Safe and Effective and How Will We Know? J. Am. Soc. Nephrol. 2021, 32, 1021–1024. [Google Scholar] [CrossRef]
- Lazarus, R.; Taucher, C.; Duncan, C.; Faust, S.; Green, C.A.; Finn, A. Immunogenicity and safety of inactivated whole virion Coronavirus vaccine with CpG (VLA2001) in healthy adults aged 18 to 55: A randomised phase 1/2 clinical trial. medRxiv 2001. [Google Scholar] [CrossRef]
- Sette, A.; Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 2021, 184, 861–880. [Google Scholar] [CrossRef]
- Cheng, L.; Zhang, X.; Chen, Y.; Wang, D.; Zhang, D.; Yan, S.; Wang, H.; Xiao, M.; Liang, T.; Li, H.; et al. Dynamic landscape mapping of humoral immunity to SARS-CoV-2 identifies non-structural protein antibodies associated with the survival of critical COVID-19 patients. Signal Transduct. Target Ther. 2021, 6, 304. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.; Chiu, Y.; Huang, E.; Chen, M.; Wang, J.; Lai, I.; Singh, S.; Shaw, R.; MacCoss, M.; Yee, C. Immunogenic SARS-CoV2 Epitopes Defined by Mass Spectrometry. BioRxiv 2021. [Google Scholar] [CrossRef]
- Uttamrao, P.P.; Sathyaseelan, C.; Patro, L.P.P.; Rathinavelan, T. Revelation of Potent Epitopes Present in Unannotated ORF Antigens of SARS-CoV-2 for Epitope-Based Polyvalent Vaccine Design Using Immunoinformatics Approach. Front. Immunol. 2021, 12, 692937. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA COVID-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Deming, M.E.; Lyke, K.E. A ‘mix and match’ approach to SARS-CoV-2 vaccination. Nat. Med. 2021. [Google Scholar] [CrossRef]
- Powell, A.A.; Power, L.; Westrop, S.; McOwat, K.; Campbell, H.; Simmons, R.; Ramsay, M.E.; Brown, K.; Ladhani, S.N.; Amirthalingam, G. Real-world data shows increased reactogenicity in adults after heterologous compared to homologous prime-boost COVID-19 vaccination, March-June 2021, England. Eurosurveillance 2021, 26. [Google Scholar] [CrossRef]
- Shaw, R.H.; Stuart, A.; Greenland, M.; Liu, X.; Nguyen Van-Tam, J.S.; Snape, M.D.; Com, C.O.V.S.G. Heterologous prime-boost COVID-19 vaccination: Initial reactogenicity data. Lancet 2021, 397, 2043–2046. [Google Scholar] [CrossRef]
- Konstantinidis, T.G.; Zisaki, S.; Mitroulis, I.; Konstantinidou, E.; Kontekaki, E.G.; Romanidou, G.; Karvelas, A.; Nanousi, I.; Lazidis, L.; Cassimos, D.; et al. Levels of Produced Antibodies after Vaccination with mRNA Vaccine; Effect of Previous Infection with SARS-CoV-2. J. Clin. Med. 2021, 10, 2842. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Group n = 142 | Control Group n = 36 | p-Value | |
|---|---|---|---|
| Age years median (IQR) | 54 (43–63) | 48 (45–62) | ns |
| Sex male n (%) | 83 (58.45) | 21 (58.3) | ns |
| CCI median (IQR) | 4 (2–5) | 0.5 (0–1) | <0.001 |
| Serum creatinine mg/dl median (IQR) | 1.35 (1.12–1.7) | ||
| BMI kg/m2 median (IQR) | 25 (22.55–28.37) | ||
| Primary nephropathy n (%) Unknown Glomerulonephritis ADPKD Other | 36 (25.35) 36 (25.35) 21 (14.79) 35 (24.65) | ||
| Transplant vintage years median (IQR) | 8 (3.5–15) | ||
| Deceased donor n (%) | 133 (93.7) | ||
| Immunosuppression protocol n (%) Protocol without steroids Protocol without MMF/MPS Protocol with induction | 12 (8.5) 30 (21.13) 37 (26.06) | ||
| mRNA-1273 vaccination n (%) | 37 (26.06) | 0 (0) | 0.002 |
| mRNA BNT162b2 vaccination n (%) | 105 (73.94) | 36 (100) | 0.002 |
| Responders n = 73 | Nonresponders n = 69 | p-Value | |
|---|---|---|---|
| Age years median (IQR) | 48.0 (40–61) | 58.0 (50–66) | 0.002 |
| Sex male n (%) | 44 (60.3) | 39 (56.5) | 0.65 |
| BMI kg/m2 median (IQR) | 25.01 (23.11–28.37) | 25.35 (22.49–28.41) | 0.33 |
| CCI median (IQR) | 3 (2–5) | 4 (3–6) | 0.079 |
| Diabetes n (%) | 16 (21.92) | 20 (28.98) | 0.33 |
| Transplant vintage years median (IQR) | 10.0 (6–19) | 7.0 (2.5–12) | 0.002 |
| Deceased donor n (%) | 69 (94.52) | 64 (92.75) | 0.67 |
| Serum creatinine mg/dl median (IQR) | 1.31 (1.03–1.58) | 1.39 (1.14–1.77) | 0.13 |
| Induction in history n (%) | 16 (21.9) | 23 (33.3) | 0.13 |
| >2 drugs immunosuppression n (%) | 46 (65.83) | 57 (82.61) | 0.009 |
| Corticosteroids n (%) | 65 (89.04) | 65 (94.2) | 0.27 |
| MMF/MPS n (%) | 52 (71.2) | 60 (86.9) | 0.02 |
| mRNA-1273 vaccine n (%) | 23 (31.5) | 14 (20.3) | 0.13 |
| Coefficient | p-Value | OR (95% CI) | |
|---|---|---|---|
| Age | −0.059 | <0.001 | 0.94 (0.91–0.97) |
| Transplant vintage | 0.081 | <0.003 | 1.08 (1.03–1.14) |
| >2 drug immunosuppression | −1.136 | <0.01 | 0.32 (0.13–0.77) |
| Coefficient | Standard Error | p-Value | |
|---|---|---|---|
| Age | −5.42 | 1.86 | 0.005 |
| >2 immunosuppressants | −193.38 | 47.19 | 0.001 |
| mRNA-1273 vaccine | 91.55 | 47.33 | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dębska-Ślizień, A.; Ślizień, Z.; Muchlado, M.; Kubanek, A.; Piotrowska, M.; Dąbrowska, M.; Tarasewicz, A.; Chamienia, A.; Biedunkiewicz, B.; Renke, M.; et al. Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study—The COViNEPH Project. Vaccines 2021, 9, 1165. https://doi.org/10.3390/vaccines9101165
Dębska-Ślizień A, Ślizień Z, Muchlado M, Kubanek A, Piotrowska M, Dąbrowska M, Tarasewicz A, Chamienia A, Biedunkiewicz B, Renke M, et al. Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study—The COViNEPH Project. Vaccines. 2021; 9(10):1165. https://doi.org/10.3390/vaccines9101165
Chicago/Turabian StyleDębska-Ślizień, Alicja, Zuzanna Ślizień, Marta Muchlado, Alicja Kubanek, Magdalena Piotrowska, Małgorzata Dąbrowska, Agnieszka Tarasewicz, Andrzej Chamienia, Bogdan Biedunkiewicz, Marcin Renke, and et al. 2021. "Predictors of Humoral Response to mRNA COVID19 Vaccines in Kidney Transplant Recipients: A Longitudinal Study—The COViNEPH Project" Vaccines 9, no. 10: 1165. https://doi.org/10.3390/vaccines9101165