Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Data Collection
2.2. Measurements
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographical Characteristics of the Sample
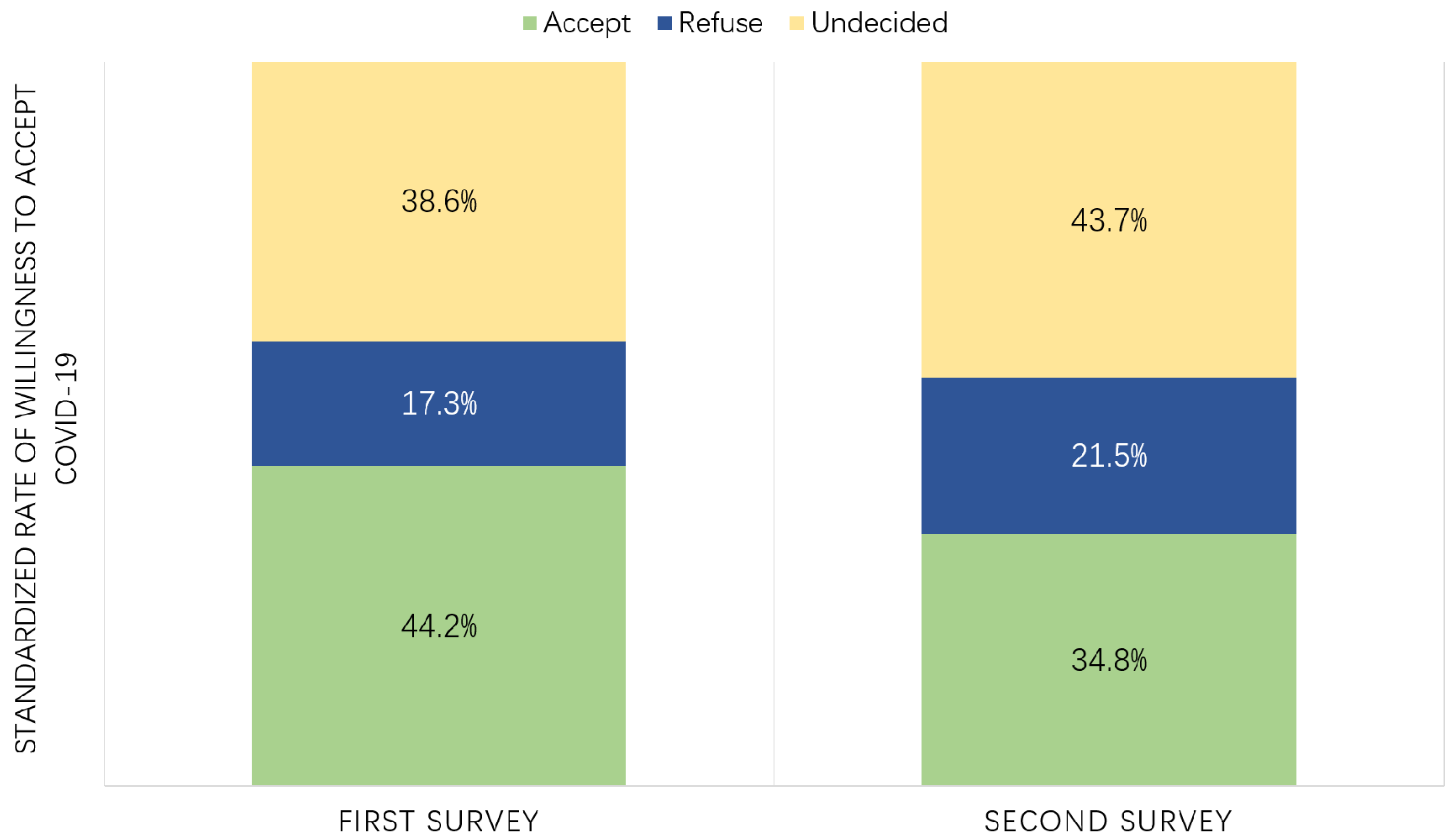
3.2. Willingness to Accept the COVID-19 Vaccine
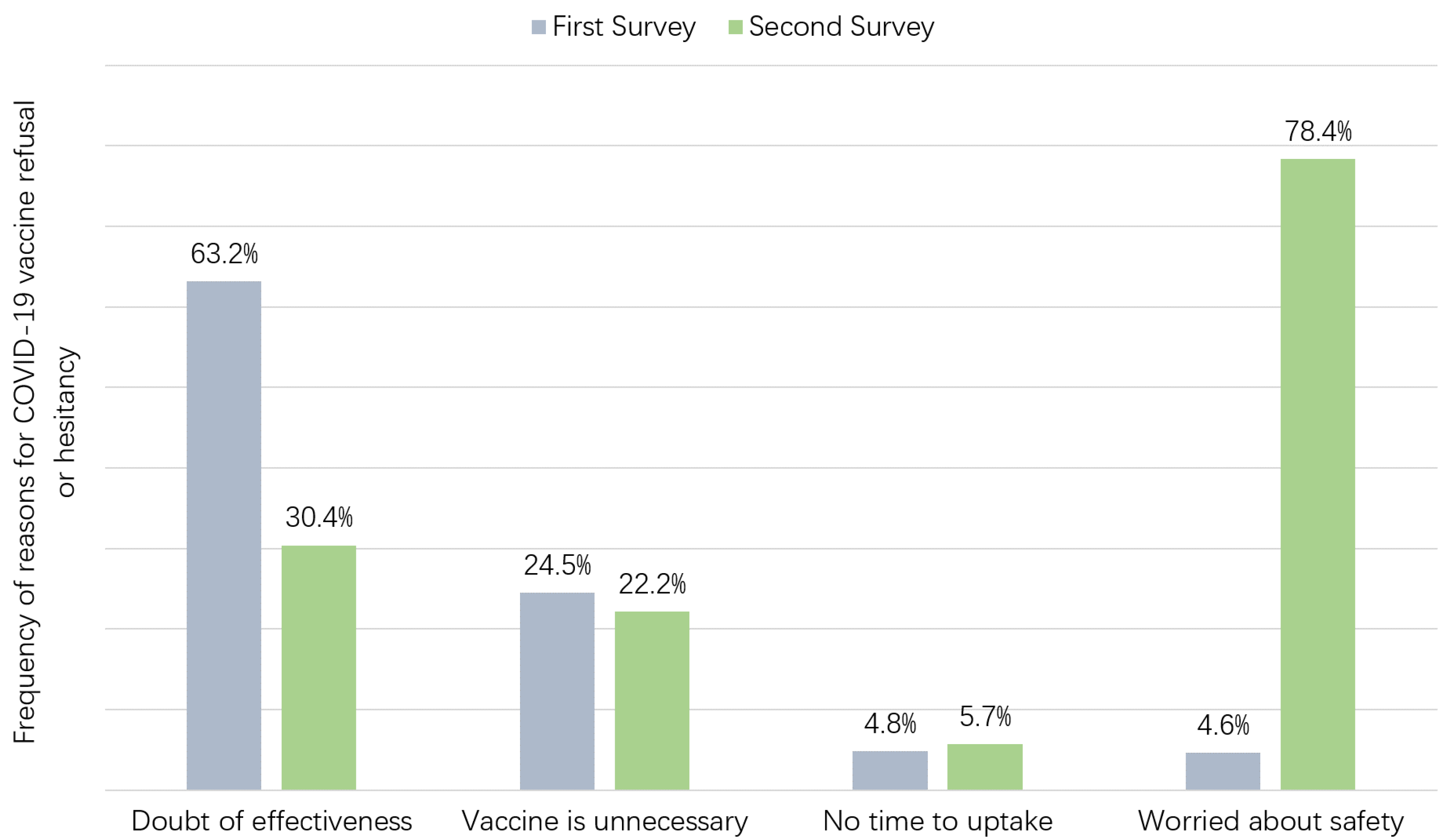
3.3. Participant Reasons for COVID-19 Vaccine Refusal or Hesitancy
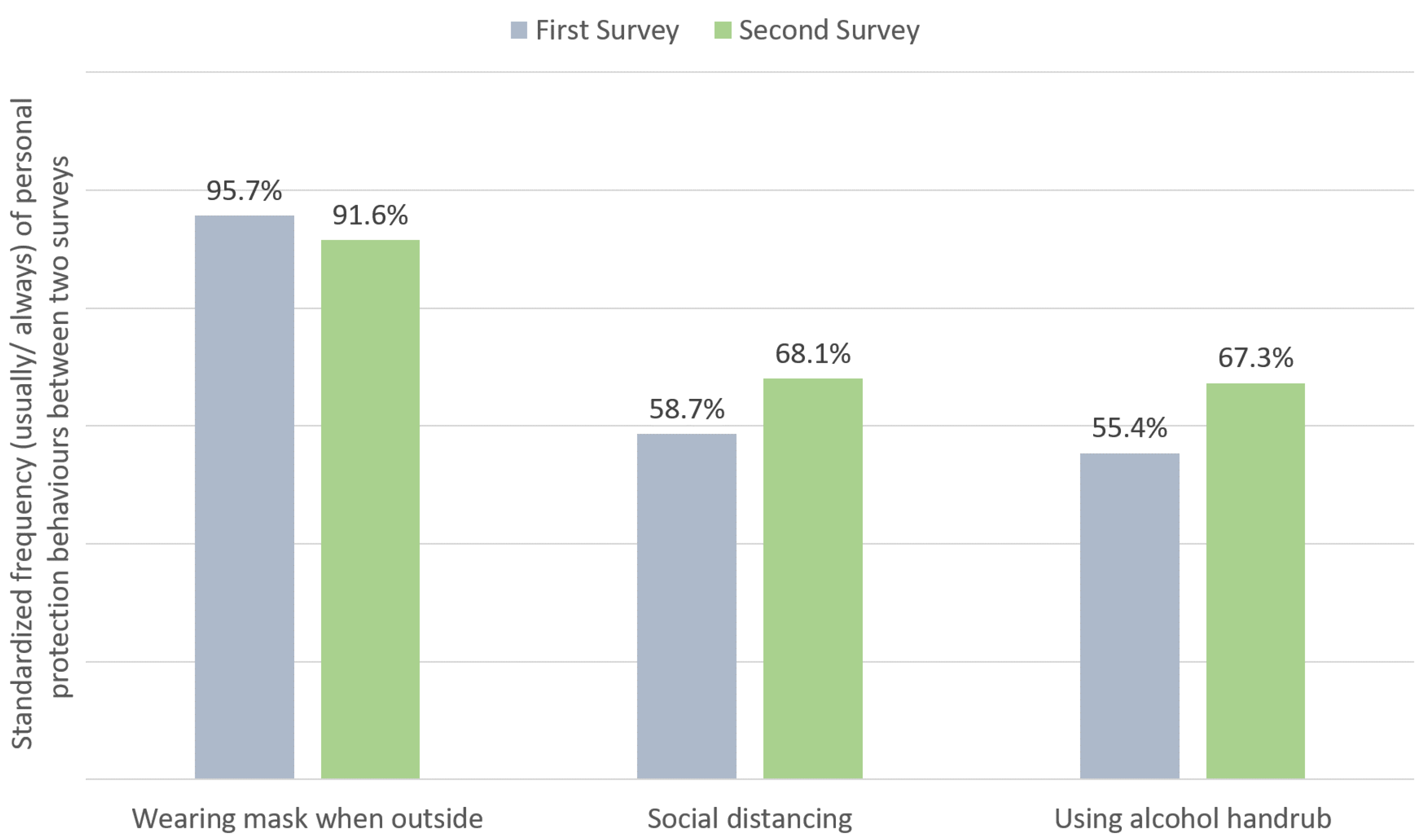
3.4. Personal Protection Behaviours to Prevent Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- John Hopkins University. Coronavirus Resource Center. 2020. Available online: https://coronavirus.jhu.edu/map.html (accessed on 12 November 2020).
- Alwan, N.A. Surveillance is underestimating the burden of the COVID-19 pandemic. Lancet 2020, 396, e24. [Google Scholar] [CrossRef]
- Pan, H.; Peto, R.; Karim, Q.A.; Alejandria, M.; Restrepo, A.M.H.; García, C.H.; Kieny, M.P.; Malekzadeh, R.; Murthy, S.; Preziosi, M.-P. Repurposed antiviral drugs for COVID-19; interim WHO SOLIDARITY trial results. medRxiv 2020. [Google Scholar] [CrossRef]
- Gao, Q.; Bao, L.; Mao, H.; Wang, L.; Xu, K.; Yang, M.; Li, Y.; Zhu, L.; Wang, N.; Lv, Z.; et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Kennedy, R.B. SARS-CoV-2 immunity: Review and applications to phase 3 vaccine candidates. Lancet 2020, 396, 1595–1606. [Google Scholar] [CrossRef]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2020, in press. [Google Scholar] [CrossRef]
- Utazi, C.E.; Thorley, J.; Alegana, V.A.; Ferrari, M.J.; Takahashi, S.; Metcalf, C.J.E.; Lessler, J.; Cutts, F.T.; Tatem, A.J. Mapping vaccination coverage to explore the effects of delivery mechanisms and inform vaccination strategies. Nat. Commun. 2019, 10, 1633. [Google Scholar] [CrossRef] [PubMed]
- Lahariya, C. Vaccine epidemiology: A review. J. Fam. Med. Prim. Care 2016, 5, 7. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Johnstone, J.; Loeb, M. Vaccine herd effect. Scand. J. Infect. Dis. 2011, 43, 683–689. [Google Scholar] [CrossRef] [Green Version]
- Trogen, B.; Oshinsky, D.; Caplan, A. Adverse Consequences of Rushing a SARS-CoV-2 Vaccine: Implications for Public Trust. JAMA 2020, 323, 2460–2461. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J.; the SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [Green Version]
- Sadaf, A.; Richards, J.L.; Glanz, J.; Salmon, D.A.; Omer, S.B. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine 2013, 31, 4293–4304. [Google Scholar] [CrossRef] [PubMed]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.A.; McFadden, S.M.; Elharake, J.; Omer, S.B. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine 2020, 26, 100495. [Google Scholar] [CrossRef] [PubMed]
- Frank, K.; Arim, R. Canadians’ Willingness to Get a COVID-19 Vaccine: Group Differences and Reasons for Vaccine Hesitancy 2020. Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00073-eng.htm (accessed on 12 November 2020).
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J.; Ayre, J.; Batcup, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccin. Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Graham, M.S.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Warner, E.T.; Sikavi, D.R.; Lo, C.-H.; et al. Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Lan, F.-Y.; Suharlim, C.; Kales, S.N.; Yang, J. Association between SARS-CoV-2 infection, exposure risk and mental health among a cohort of essential retail workers in the USA. Occup. Environ. Med. 2020. [Google Scholar] [CrossRef]
- Marinaccio, A.; Boccuni, F.; Rondinone, B.M.; Brusco, A.; D’Amario, S.; Iavicoli, S. Occupational factors in the COVID-19 pandemic in Italy: Compensation claims applications support establishing an occupational surveillance system. Occup. Environ. Med. 2020, 77, 818–821. [Google Scholar] [CrossRef]
- Lan, F.Y.; Wei, C.F.; Hsu, Y.T.; Christiani, D.C.; Kales, S.N. Work-related COVID-19 transmission in six Asian countries/areas: A follow-up study. PLoS ONE 2020, 15, e0233588. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 November 2020).
- Centre for Health Protection. COVID-19 Thematic Website Hong Kong. 2020. Available online: https://www.coronavirus.gov.hk/eng/index.html (accessed on 12 November 2020).
- Hong Kong SAR Government. Press Releases—Government Extends Social Distancing Measures Hong Kong. 2020. Available online: https://www.info.gov.hk/gia/general/202008/17/P2020081700445.htm (accessed on 12 November 2020).
- Census and Statistics Department. 2019 Report on Annual Earnings and Hours Survey Hong Kong. 2020. Available online: https://www.statistics.gov.hk/pub/B10500142019AN19B0100.pdf (accessed on 12 November 2020).
- Raab, M.; Pfadenhauer, L.M.; Millimouno, T.J.; Hoelscher, M.; Froeschl, G. Knowledge, attitudes and practices towards viral haemorrhagic fevers amongst healthcare workers in urban and rural public healthcare facilities in the N’zerekore prefecture, Guinea: A cross-sectional study. BMC Public Health 2020, 20, 296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Getting Your Workplace Ready for COVID-19. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/getting-workplace-ready-for-covid-19.pdf (accessed on 1 November 2020).
- Naing, N.N. Easy way to learn standardization: Direct and indirect methods. Malays. J. Med. Sci. 2000, 7, 10. [Google Scholar] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Chor, J.S.; Ngai, K.L.; Goggins, W.B.; Wong, M.C.; Wong, S.Y.; Lee, N.; Leung, T.F.; Rainer, T.H.; Griffiths, S.; Chan, P.K. Willingness of Hong Kong healthcare workers to accept pre-pandemic influenza vaccination at different WHO alert levels: Two questionnaire surveys. BMJ 2009, 339, b3391. [Google Scholar] [CrossRef] [Green Version]
- Hotez, P. America and Europe’s new normal: The return of vaccine-preventable diseases. Pediatr. Res. 2019, 85, 912–914. [Google Scholar] [CrossRef]
- Jolley, D.; Douglas, K.M. The effects of anti-vaccine conspiracy theories on vaccination intentions. PLoS ONE 2014, 9, e89177. [Google Scholar] [CrossRef]
- Burki, T. The online anti-vaccine movement in the age of COVID-19. Lancet Digit. Health 2020, 2, e504–e505. [Google Scholar] [CrossRef]
- Johnson, N.F.; Velasquez, N.; Restrepo, N.J.; Leahy, R.; Gabriel, N.; El Oud, S.; Zheng, M.; Manrique, P.; Wuchty, S.; Lupu, Y. The online competition between pro- and anti-vaccination views. Nature 2020, 582, 230–233. [Google Scholar] [CrossRef]
- Zhang, M.; Zhou, M.; Tang, F.; Wang, Y.; Nie, H.; Zhang, L.; You, G. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J. Hosp. Infect. 2020, 105, 183–187. [Google Scholar] [CrossRef]
- Alrubaiee, G.G.; Al-Qalah, T.A.H.; Al-Aawar, M.S.A. Knowledge, attitudes, anxiety, and preventive behaviours towards COVID-19 among health care providers in Yemen: An online cross-sectional survey. BMC Public Health 2020, 20, 1541. [Google Scholar] [CrossRef] [PubMed]
- Manuel, D.; Henry, B.; Hockin, J.; Naus, M. Health behavior associated with influenza vaccination among healthcare workers in long-term-care facilities. Infect. Control Hosp. Epidemiol. 2002, 23, 609–614. [Google Scholar] [CrossRef] [PubMed]
- Whibley, A. Global surge in measles and major international survey reinforce the need for greater awareness and uptake of all vaccinations. Acta Paediatr. 2020, 109, 1706–1708. [Google Scholar] [CrossRef] [PubMed]
- Loskutova, N.Y.; Smail, C.; Callen, E.; Staton, E.W.; Nazir, N.; Webster, B.; Pace, W.D. Effects of multicomponent primary care-based intervention on immunization rates and missed opportunities to vaccinate adults. BMC Fam. Pract. 2020, 21, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gudi, S.K.; Chhabra, M.; Undela, K.; Venkataraman, R.; Mateti, U.V.; Tiwari, K.K.; Nyamagoud, S. Knowledge and beliefs towards universal safety precautions during the coronavirus disease (COVID-19) pandemic among the Indian public: A web-based cross-sectional survey. Drugs Ther. Perspect. 2020, 36, 413–420. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, A.C.; Lu, P.-J.; Williams, W.W.; Schumacher, P.; Sussell, A.; Birdsey, J.; Boal, W.L.; Sweeney, M.H.; Luckhaupt, S.E.; Black, C.L. Influenza vaccination among workers—21 US states, 2013. Am. J. Infect. Control 2017, 45, 410–416. [Google Scholar] [CrossRef] [Green Version]
- Centre for Health Protection. Recommendations on Seasonal Influenza Vaccination for the 2020–2021 Season in Hong Kong. 2020. Available online: https://www.chp.gov.hk/files/pdf/recommendations_on_siv_for_2020-21.pdf (accessed on 12 November 2020).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2020, 1–4. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | First Survey: Willingness to Accept COVID-19 Vaccine | Second Survey: Willingness to Accept COVID-19 Vaccine | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Accept | Refuse | Undecided | p Value 1 | Total | Accept | Refuse | Undecided | p Value 1 | Total | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | |||
| Age | ||||||||||||||||||
| 18–29 | 110 | 26.0 | 20 | 9.6 | 87 | 20.9 | <0.001 * | 217 | 20.7 | 53 | 15.2 | 27 | 12.6 | 81 | 18.5 | 0.063 | 161 | 16.1 |
| 30–39 | 125 | 29.6 | 55 | 26.4 | 114 | 27.4 | 294 | 28.1 | 82 | 23.6 | 53 | 24.7 | 90 | 20.6 | 225 | 22.5 | ||
| 40–49 | 125 | 29.6 | 82 | 39.4 | 138 | 33.2 | 345 | 33.0 | 80 | 23.0 | 66 | 30.7 | 101 | 23.1 | 247 | 24.7 | ||
| 50–59 | 49 | 11.6 | 44 | 21.2 | 69 | 16.6 | 162 | 15.5 | 79 | 22.7 | 48 | 22.3 | 116 | 26.5 | 243 | 24.3 | ||
| 60+ | 14 | 3.3 | 7 | 3.4 | 8 | 1.9 | 29 | 2.8 | 54 | 15.5 | 21 | 9.8 | 49 | 11.2 | 124 | 12.4 | ||
| Sex | ||||||||||||||||||
| Male | 168 | 39.7 | 65 | 31.3 | 103 | 24.8 | <0.001 * | 336 | 32.1 | 205 | 58.9 | 108 | 50.2 | 226 | 51.7 | 0.063 | 539 | 53.9 |
| Female | 255 | 60.3 | 143 | 68.8 | 313 | 75.2 | 711 | 67.9 | 143 | 41.1 | 107 | 49.8 | 211 | 48.3 | 461 | 46.1 | ||
| Education | ||||||||||||||||||
| Below high school | 2 | 0.5 | 3 | 1.4 | 5 | 1.2 | 0.170 | 10 | 1.0 | 14 | 4.0 | 8 | 3.7 | 23 | 5.3 | 0.279 | 45 | 4.5 |
| High school | 35 | 8.3 | 27 | 13.0 | 41 | 9.9 | 103 | 9.8 | 87 | 25.0 | 68 | 31.6 | 100 | 22.9 | 255 | 25.5 | ||
| Preparatory | 51 | 12.1 | 30 | 14.4 | 67 | 16.1 | 148 | 14.1 | 81 | 23.3 | 51 | 23.7 | 114 | 26.1 | 246 | 24.6 | ||
| University or above | 335 | 79.2 | 148 | 71.2 | 303 | 72.8 | 786 | 75.1 | 166 | 47.7 | 88 | 40.9 | 200 | 45.8 | 454 | 45.4 | ||
| Marriage | ||||||||||||||||||
| Unmarried | 201 | 47.5 | 94 | 45.2 | 196 | 47.1 | 0.854 | 491 | 46.9 | 117 | 33.6 | 101 | 47.0 | 210 | 48.1 | <0.001 * | 428 | 42.8 |
| Married/cohabit | 222 | 52.5 | 114 | 54.8 | 220 | 52.9 | 556 | 53.1 | 231 | 66.4 | 114 | 53.0 | 227 | 52.0 | 572 | 57.2 | ||
| Occupation | ||||||||||||||||||
| Professionals | 173 | 40.9 | 99 | 47.6 | 168 | 40.4 | 0.298 | 440 | 42.0 | 50 | 14.4 | 17 | 7.9 | 36 | 8.2 | 0.044 * | 103 | 10.3 |
| Manager/administrator | 75 | 17.7 | 38 | 18.3 | 70 | 16.8 | 183 | 17.5 | 48 | 13.8 | 24 | 11.2 | 54 | 12.4 | 126 | 12.6 | ||
| Associate professional | 115 | 27.2 | 40 | 19.2 | 100 | 24.0 | 255 | 24.4 | 80 | 23.0 | 58 | 27.0 | 117 | 26.8 | 255 | 25.5 | ||
| Clerical/service/sales worker | 55 | 13.0 | 30 | 14.4 | 72 | 17.3 | 157 | 15.0 | 88 | 25.3 | 72 | 33.5 | 141 | 32.3 | 301 | 30.1 | ||
| Blue-collar worker | 5 | 1.2 | 1 | 0.5 | 6 | 1.4 | 12 | 1.2 | 82 | 23.6 | 44 | 20.5 | 89 | 20.4 | 215 | 21.5 | ||
| Chronic disease | ||||||||||||||||||
| No | 363 | 85.8 | 179 | 86.1 | 354 | 85.1 | 0.934 | 896 | 85.6 | 298 | 85.6 | 194 | 90.2 | 400 | 91.5 | 0.026 * | 892 | 89.2 |
| Yes | 60 | 14.2 | 29 | 13.9 | 62 | 14.9 | 151 | 14.4 | 50 | 14.4 | 21 | 9.8 | 37 | 8.5 | 108 | 10.8 | ||
| Influenza vaccine uptake last year | ||||||||||||||||||
| No | 309 | 73.1 | 190 | 91.4 | 355 | 85.3 | <0.001 * | 854 | 81.6 | 253 | 72.7 | 199 | 92.6 | 371 | 84.9 | <0.001 * | 823 | 82.3 |
| Yes | 114 | 27.0 | 18 | 8.7 | 61 | 14.7 | 193 | 18.4 | 95 | 27.3 | 16 | 7.4 | 66 | 15.1 | 177 | 17.7 | ||
| Total | 423 | 100.0 | 208 | 100.0 | 416 | 100.0 | 1047 | 100.0 | 348 | 100.0 | 215 | 100.0 | 437 | 100.0 | 1000 | 100 | ||
| Acceptance of Vaccination/Behaviours | First Survey | Second Survey | p Value 2 | |||
|---|---|---|---|---|---|---|
| N | Unstandardized % | Standardized % 1 | N | Standardized % 1 | ||
| Willingness to accept COVID-19 vaccine | ||||||
| Accept | 423 | 40.4 | 44.2 | 348 | 34.8 | <0.001 |
| Refuse | 208 | 19.9 | 17.3 | 215 | 21.5 | |
| Undecided | 416 | 39.7 | 38.6 | 437 | 43.7 | |
| Wearing mask when outside | ||||||
| Never/sometimes | 48 | 4.6 | 4.3 | 84 | 8.4 | <0.001 |
| Usually/always | 999 | 95.4 | 95.7 | 916 | 91.6 | |
| Social distancing | ||||||
| Never/sometimes | 343 | 32.8 | 41.3 | 319 | 31.9 | 0.001 |
| Usually/always | 704 | 67.2 | 58.7 | 681 | 68.1 | |
| Using alcohol hand rub | ||||||
| Never/sometimes | 457 | 43.7 | 44.5 | 327 | 32.7 | <0.001 |
| Usually/always | 590 | 56.4 | 55.6 | 673 | 67.3 | |
| Total | 1047 | 100.0 | 100.0 | 1000 | 100.0 | |
| Characteristics | COVID-19 Vaccine Acceptance (Undecided as Reference) 1 | Usually/Always Wear Mask When Outside1 | Usually/Always Maintain Social Distance 1 | Usually/Always Use Alcohol Hand Rub When Outside 1 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Accept | Refuse | |||||||||
| AOR 2 | 95%CI 2 | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Age | ||||||||||
| 18–29 | (reference) | (reference) | (reference) | (reference) | (reference) | |||||
| 30–39 | 0.67 * | (0.48, 0.93) | 1.76 * | (1.10, 2.82) | 0.81 | (0.44, 1.49) | 1.08 | (0.79, 1.47) | 0.91 | (0.67, 1.25) |
| 40–49 | 0.56 * | (0.39, 0.80) | 3.04 * | (1.88, 4.91) | 1.28 | (0.64, 2.55) | 0.87 | (0.62, 1.21) | 0.58 * | (0.42, 0.81) |
| 50–59 | 0.37 * | (0.26, 0.53) | 2.20 * | (1.36, 3.56) | 1.26 | (0.63, 2.51) | 0.78 | (0.56, 1.08) | 0.41 * | (0.29, 0.57) |
| 60+ | 0.70 | (0.46, 1.08) | 2.74 * | (1.55, 4.82) | 0.66 | (0.32, 1.36) | 0.95 | (0.64, 1.41) | 0.58 * | (0.39, 0.85) |
| Sex | ||||||||||
| Male | (reference) | (reference) | (reference) | (reference) | (reference) | |||||
| Female | 0.71 * | (0.57, 0.89) | 1.04 | (0.80, 1.35) | 1.40 | (0.94, 2.09) | 1.37 * | (1.11, 1.67) | 1.60 * | (1.31, 1.97) |
| Marriage | ||||||||||
| Unmarried | (reference) | (reference) | (reference) | (reference) | (reference) | |||||
| Married/cohabit | 1.69 * | (1.33, 2.14) | 0.75 * | (0.58, 0.98) | 0.80 | (0.52, 1.22) | 1.49 * | (1.21, 1.85) | 1.63 * | (1.32, 2.02) |
| Chronic disease | ||||||||||
| No | (reference) | (reference) | (reference) | (reference) | (reference) | |||||
| Yes | 1.07 | (0.80, 1.44) | 1.17 | (0.82, 1.67) | 0.56* | (0.35, 0.89) | 0.88 | (0.67, 1.14) | 0.93 | (0.72, 1.21) |
| Influenza vaccine uptake last year | ||||||||||
| No | (reference) | (reference) | - | - | - | |||||
| Yes | 2.25 * | (1.74, 2.93) | 0.42 * | (0.27, 0.66) | - | - | - | |||
| Occupation | ||||||||||
| Professionals | (reference) | (reference) | (reference) | (reference) | (reference) | |||||
| Manager/administrator | 0.81 | (0.53, 1.25) | 0.70 | (0.42, 1.16) | 0.79 | (0.35, 1.81) | 1.01 | (0.68, 1.51) | 2.08 * | (1.41, 3.07) |
| Associate professional | 0.77 | (0.53, 1.12) | 0.82 | (0.52, 1.29) | 0.67 | (0.33, 1.37) | 0.95 | (0.67, 1.34) | 1.27 | (0.91, 1.77) |
| Clerical/service/sales worker | 0.62 * | (0.43, 0.91) | 0.68 | (0.44, 1.06) | 0.70 | (0.34, 1.44) | 0.93 | (0.66, 1.32) | 1.36 | (0.97, 1.89) |
| Blue-collar worker | 0.76 | (0.52, 1.13) | 0.52 * | (0.32, 0.86) | 0.69 | (0.33, 1.45) | 0.54 * | (0.37, 0.77) | 1.47 * | (1.03, 2.10) |
| Wave of local epidemic | ||||||||||
| First wave (first survey) | (reference) | (reference) | (reference) | (reference) | (reference) | |||||
| Third wave (second survey) | 0.68 * | (0.56, 0.84) | 1.12 | (0.88, 1.44) | 0.47 * | (0.32, 0.69) | 1.54 * | (1.27, 1.86) | 1.67 * | (1.39, 2.02) |
| Occupations | Doubt of Effectiveness | Vaccine Is Unnecessary | No Time to Uptake | Worried About Safety | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | No | Yes | ||
| First survey (standardized N (%)) 1 | |||||||||
| Professional | 25 (40.3) | 37 (59.7) | 43 (69.1) | 19 (30.9) | 56 (91.6) | 5 (8.4) | 59 (96.1) | 2 (3.9) | 62 (100) |
| Manager/administrator | 35 (46.4) | 41 (53.6) | 50 (65.8) | 26 (34.2) | 76 (99.2) | 1 (0.8) | 69 (90.1) | 8 (9.9) | 76 (100) |
| Associate professional | 44 (34.3) | 85 (65.7) | 95 (73.7) | 34 (26.3) | 123 (95.3) | 6 (4.7) | 120 (93.1) | 9 (6.9) | 129 (100) |
| Clerical/service/sale worker | 79 (38.8) | 125 (61.2) | 147 (71.7) | 58 (28.4) | 189 (92.6) | 15 (7.4) | 198 (96.7) | 7 (3.3) | 205 (100) |
| Blue-collar worker | 22 (25) | 66 (75.1) | 88 (100) | 0 (0) | 88 (100) | 0 (0) | 88 (100) | 0 (0) | 88 (100) |
| p value 2 | 0.058 | 0.031 *,3 | 0.300 3 | 0.012 *,3 | |||||
| Total | 206 (36.8) | 354 (63.2) | 423 (75.5) | 137 (24.5) | 533 (95.2) | 27 (4.8) | 534 (95.4) | 26 (4.6) | 560 (100) |
| Second survey (N (%)) | |||||||||
| Professional | 38 (71.7) | 15 (28.3) | 43 (81.1) | 10 (18.9) | 50 (94.3) | 3 (5.7) | 11 (20.8) | 42 (79.3) | 53 (100.0) |
| Manager/administrator | 50 (64.1) | 28 (35.9) | 68 (87.2) | 10 (12.8) | 73 (93.6) | 5 (6.4) | 15 (19.2) | 63 (80.8) | 78 (100.0) |
| Associate professional | 118 (67.4) | 57 (32.6) | 143 (81.7) | 32 (18.3) | 169 (96.6) | 6 (3.4) | 29 (16.6) | 146 (83.4) | 175 (100.0) |
| Clerical/service/sale worker | 150 (70.4) | 63 (29.6) | 155 (72.8) | 58 (27.2) | 206 (96.7) | 7 (3.3) | 53 (24.9) | 160 (75.1) | 213 (100.0) |
| Blue-collar worker | 98 (73.7) | 35 (26.3) | 98 (73.7) | 35 (26.3) | 117 (88) | 16 (12) | 33 (24.8) | 100 (75.2) | 133 (100.0) |
| p value 2 | 0.604 | 0.036 * | 0.007 * | 0.282 | |||||
| Total | 454 (69.6) | 198 (30.4) | 507 (77.8) | 145 (22.2) | 615 (94.3) | 37 (5.7) | 141 (21.6) | 511 (78.4) | 652 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, K.; Wong, E.L.-Y.; Ho, K.-F.; Cheung, A.W.-L.; Yau, P.S.-Y.; Dong, D.; Wong, S.Y.-S.; Yeoh, E.-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. https://doi.org/10.3390/vaccines9010062
Wang K, Wong EL-Y, Ho K-F, Cheung AW-L, Yau PS-Y, Dong D, Wong SY-S, Yeoh E-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines. 2021; 9(1):62. https://doi.org/10.3390/vaccines9010062
Chicago/Turabian StyleWang, Kailu, Eliza Lai-Yi Wong, Kin-Fai Ho, Annie Wai-Ling Cheung, Peter Sen-Yung Yau, Dong Dong, Samuel Yeung-Shan Wong, and Eng-Kiong Yeoh. 2021. "Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys" Vaccines 9, no. 1: 62. https://doi.org/10.3390/vaccines9010062