Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies




Abstract
:1. Introduction
1.1. Overview of Parental Vaccine Hesitancy Towards Childhood Vaccines in the U.S.
1.2. Vaccines, Vaccination, and Immunization
1.3. Components of Vaccines
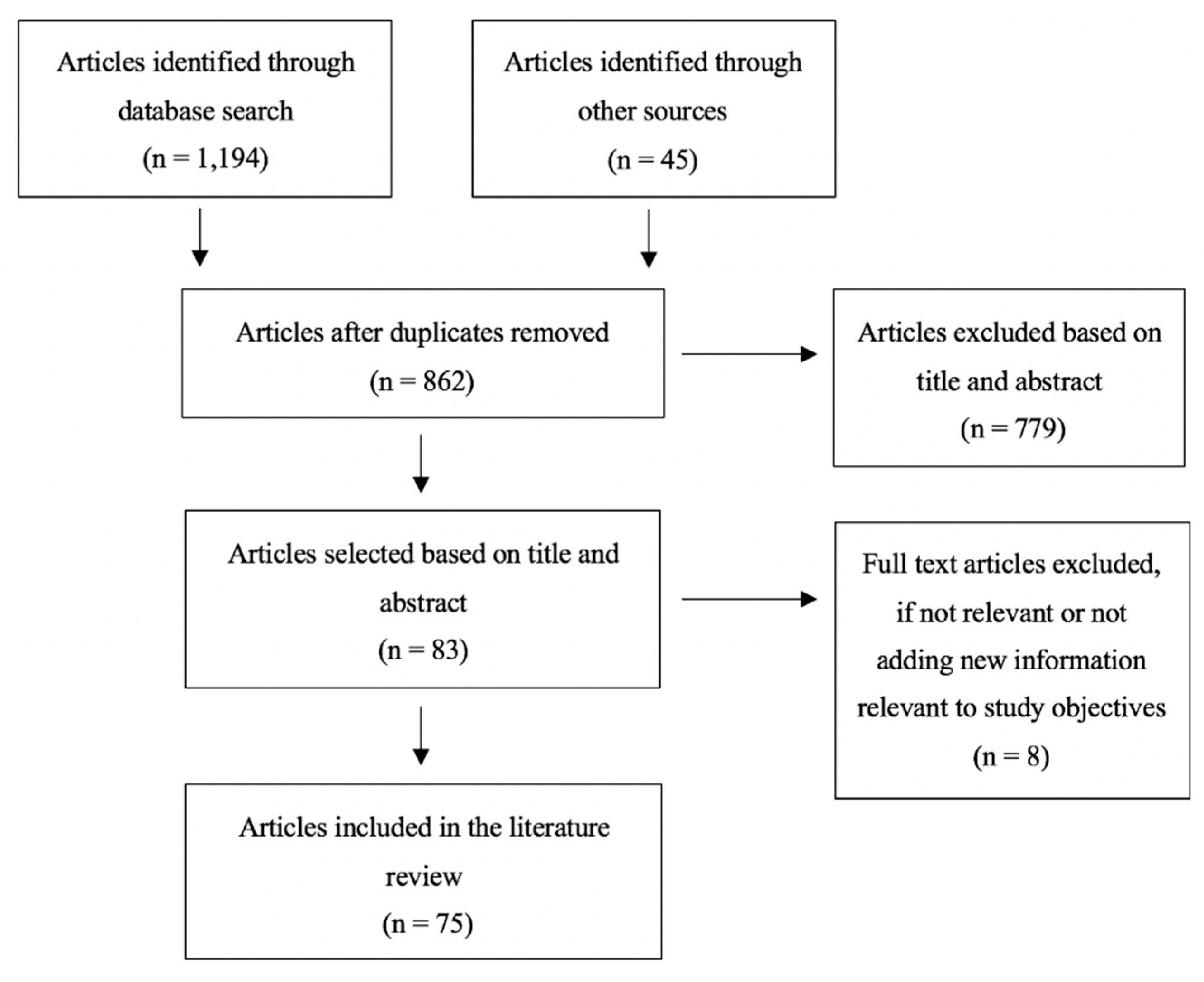
2. Materials and Methods
3. Results
3.1. Defining Vaccine Hesitancy
3.2. Key Determinants of Childhood Vaccine Hesitancy
3.3. Key Communication Interventions and Strategies That Address Vaccine Hesitancy
3.3.1. Inform and Educate
3.3.2. Remind or Recall
3.3.3. Enhance Community Ownership
3.3.4. Teach Skills
3.3.5. Provide Support
3.3.6. Facilitate Decision-Making
3.3.7. Enable Communication
3.4. Key Themes Identified in the Literature for Targeting Interventions
3.4.1. Audiences Targeted
3.4.2. Messenger of Vaccination Information
3.4.3. Timing of Vaccination Information
3.4.4. Amount of Vaccination Information
3.4.5. Content of Vaccination Information
3.4.6. Approaches to Vaccine Messaging
3.4.7. Vaccine Misinformation and Disinformation
3.4.8. Vaccine Literacy
3.4.9. Face-to-Face Communication Strategies
3.4.10. Technology-Based Communication Strategies
4. Discussion
4.1. Public Health Implications of the Findings
4.2. Interventions That Have Been Successful or Unsuccessful
5. Recommendations and Conclusions
5.1. Start Early and Build Trust with Parents
5.2. Tailor the Information to the Target Audience, Their Reasons for Hesitancy, and the Specific Context
5.3. Present Vaccination as the Default Approach
5.4. Develop Vaccine Education Materials Using Health Literacy Best Practices
5.5. Incorporate Dialogue-Based Communication Strategies and Provide Balanced Information about Vaccines
5.6. Tell Stories with Gists and Emotive Anecdotes
5.7. Choose the Messenger of Vaccine Information Carefully
5.8. Focus on Vaccine Messaging That Centers Both the Child and Community
5.9. Use Technology to Promote Vaccination
5.10. Use Caution When Addressing Vaccine Misinformation
5.11. Improve Parents’ Vaccine Literacy and Critical Thinking Skills
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control. Ten Great Public Health Achievements—United States, 1900–1999. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00056796.htm (accessed on 7 February 2020).
- Centers for Disease Control. Ten Great Public Health Achievements—United States, 2001–2010. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6019a5.htm (accessed on 7 February 2020).
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Kempe, A.; Saville, A.W.; Albertin, C.; Zimet, G.; Breck, A.; Helmkamp, L.; Vangala, S.; Dickinson, L.M.; Rand, C.; Humiston, S.; et al. Parental Hesitancy About Routine Childhood and Influenza Vaccinations: A National Survey. Pediatrics 2020, 146, e20193852. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). In Vaccination Coverage Among Children Aged 19–35 Months—United States; 2017. Available online: https://www.cdc.gov/mmwr/volumes/67/wr/mm6740a4.htm (accessed on 7 February 2020).
- Hargreaves, A.L.; Nowak, G.; Frew, P.; Hinman, A.R.; Orenstein, W.A.; Mendel, J.; Aikin, A.; Nadeau, J.A.; McNutt, L.-A.; Chamberlain, A.T.; et al. Adherence to Timely Vaccinations in the United States. Pediatrics 2020, 145, e20190783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olive, J.K.; Hotez, P.J.; Damania, A.; Nolan, M.S. The state of the antivaccine movement in the United States: A focused examination of nonmedical exemptions in states and counties. PLoS Med. 2018, 15, e1002578. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. U.S. Public Health Response to the Measles Outbreak. (2019, February 27). Available online: https://www.cdc.gov/washington/testimony/2019/t20190227.htm (accessed on 7 February 2020).
- Centers for Disease Control and Prevention. Measles Outbreak—California, December 2014–February 2015. (2015, February 20). Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6406a5.htm (accessed on 7 February 2020).
- Centers for Disease Control and Prevention. Measles Cases and Outbreaks. (2020, April 6). Available online: https://www.cdc.gov/measles/cases-outbreaks.html (accessed on 25 April 2020).
- Patel, M.; Lee, A.; Redd, S.; Clemmons, N.; McNaiill, R.; Cohn, A.; Gastanaduy, P. Increase in Measles Cases—United States, January 1–April 26. 2019. Available online: https://www.cdc.gov/mmwr/volumes/68/wr/mm6817e1.htm (accessed on 7 February 2020).
- Hussain, A.; Ali, S.; Ahmed, M.; Hussain, S. The Anti-vaccination Movement: A Regression in Modern Medicine. Cureus 2018, 10, 2919. [Google Scholar] [CrossRef] [Green Version]
- Rosselli, R.; Martini, M.; Bragazzi, N. The old and the new: Vaccine hesitancy in the era of the Web 2.0. Challenges and opportunities. J. Prev. Med. Hyg. 2016, 57, E47–E50. [Google Scholar]
- Stahl, J.-P.; Cohen, R.; Denis, F.; Gaudelus, J.; Martinot, A.; Lery, T.; Lepetit, H. The impact of the web and social networks on vaccination. New challenges and opportunities offered to fight against vaccine hesitancy. Med. Mal. Infect. 2016, 46, 117–122. [Google Scholar] [CrossRef]
- Macdonald, N.E.; Dubé, E. Promoting immunization resiliency in the digital information age. Can. Commun. Dis. Rep. 2020, 46, 20–24. [Google Scholar] [CrossRef]
- Burki, T. Vaccine misinformation and social media. Lancet Digit. Health 2019, 1, e258–e259. [Google Scholar] [CrossRef] [Green Version]
- Pluviano, S.; Watt, C.; Della Sala, S. Misinformation lingers in memory: Failure of three pro-vaccination strategies. PLoS ONE 2017, 12, e0181640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, H.J.; Cooper, L.Z.; Eskola, J.; Katz, S.L.; Ratzan, S. Addressing the vaccine confidence gap. Lancet 2011, 378, 526–535. [Google Scholar] [CrossRef]
- Godlee, F.; Smith, J.; Marcovitch, H. Wakefield’s article linking MMR vaccine and autism was fraudulent. BMJ 2011, 342, c7452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrix, K.S.; Finnell, S.M.E.; Zimet, G.D.; Sturm, L.A.; Lane, K.A.; Downs, S.M. Vaccine Message Framing and Parents’ Intent to Immunize Their Infants for MMR. Pediatrics 2014, 134, e675–e683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, P.J.; Humiston, S.G.; Marcuse, E.K.; Zhao, Z.; Dorell, C.G.; Howes, C.; Hibbs, B. Parental Delay or Refusal of Vaccine Doses, Childhood Vaccination Coverage at 24 Months of Age, and the Health Belief Model. Public Health Rep. 2011, 126, 135–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edwards, K.M.; Hackell, J.M. Countering Vaccine Hesitancy. Pediatrics 2016, 138, 20162146. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Vivion, M.; E MacDonald, N. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: Influence, impact and implications. Expert Rev. Vaccines 2014, 14, 99–117. [Google Scholar] [CrossRef]
- Glanz, J.; Kraus, C.R.; Daley, M.F. Addressing Parental Vaccine Concerns: Engagement, Balance, and Timing. PLoS Biol. 2015, 13, e1002227. [Google Scholar] [CrossRef] [Green Version]
- Salmon, A.D.; Dudley, M.Z.; Glanz, J.M.; Omer, S.B. Vaccine hesitancy. Vaccine 2015, 33, D66–D71. [Google Scholar] [CrossRef]
- Williams, E.S. What are the factors that contribute to parental vaccine-hesitancy and what can we do about it? Hum. Vaccines Immunother. 2014, 10, 2584–2596. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ten threats to global health in 2019. 2019. Available online: https://www.who.int/news-room/feature-stories/ten-threats-to-global-health-in-2019 (accessed on 7 February 2020).
- World Health Organization. Report of the SAGE Working Group on Vaccine Hesitancy. (2014, November 12). Available online: https://www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf?ua=1 (accessed on 7 February 2020).
- Kumar, D.; Chandra, R.; Mathur, N.; Samdariya, S.; Kapoor, N. Vaccine hesitancy: Understanding better to address better. Isr. J. Health Policy Res. 2016, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.; Dubey, V. Addressing vaccine hesitancy: Clinical guidance for primary care physicians working with parents. Can. Fam. Physician Med. Fam. Can. 2019, 65, 175–181. [Google Scholar]
- Sadaf, A.; Richards, J.L.; Glanz, J.; A Salmon, D.; Omer, S.B. A systematic review of interventions for reducing parental vaccine refusal and vaccine hesitancy. Vaccine 2013, 31, 4293–4304. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arede, M.; Bravo-Araya, M.; Bouchard, É.; Gill, G.S.; Plajer, V.; Shehraj, A.; Shuaib, Y.A. Combating Vaccine Hesitancy: Teaching the next Generation to Navigate through the Post Truth Era. Front. Public Health 2019, 6, 381. [Google Scholar] [CrossRef] [Green Version]
- Penţa, M.A.; Băban, A. Message Framing in Vaccine Communication: A Systematic Review of Published Literature. Health Commun. 2017, 33, 1–16. [Google Scholar] [CrossRef]
- Larson, H.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef]
- Betsch, C.; Brewer, N.T.; Brocard, P.; Davies, P.; Gaissmaier, W.; Haase, N.; Leask, J.; Renkewitz, F.; Renner, B.; Reyna, V.F.; et al. Opportunities and challenges of Web 2.0 for vaccination decisions. Vaccine 2012, 30, 3727–3733. [Google Scholar] [CrossRef] [Green Version]
- Vetter, V.; Denizer, G.; Friedland, L.R.; Krishnan, J.; Shapiro, M. Understanding modern-day vaccines: What you need to know. Ann. Med. 2017, 50, 110–120. [Google Scholar] [CrossRef]
- Murphy, K.; Weaver, C. Janeway’s Immunobiology. Available online: http://www.garlandscience.com/product/isbn/9780815345053 (accessed on 28 September 2020).
- Office of Disease Prevention and Health Promotion. Immunization and Infectious Diseases (2020, August 08). Available online: https://www.healthypeople.gov/2020/topics-objectives/topic/immunization-and-infectious-diseases (accessed on 23 August 2020).
- World Health Organization. Vaccination greatly reduces disease, disability, death and inequity worldwide. (2008, February). Available online: https://www.who.int/bulletin/volumes/86/2/07-040089/en/ (accessed on 7 February 2020).
- Centers for Disease Control. 14 Diseases You Almost Forgot About (Thanks to Vaccines). (2020, January 03). Available online: https://www.cdc.gov/vaccines/parents/diseases/forgot-14-diseases.html (accessed on 7 February 2020).
- Wack, A.; Rappuoli, R. Vaccinology at the beginning of the 21st century. Curr. Opin. Immunol. 2005, 17, 411–418. [Google Scholar] [CrossRef] [PubMed]
- O’Hagan, D.T.; Rappuoli, R. The safety of vaccines. Drug Discov. Today 2004, 9, 846–854. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Vaccines: Vac-Gen/Additives in Vaccines Fact Sheet. (2019, August 5). Available online: https://www.cdc.gov/vaccines/vac-gen/additives.htm (accessed on 7 February 2020).
- Centers for Disease Control and Prevention. Who Sets the Immunization Schedule? (2012, March 8). Available online: https://www.cdc.gov/vaccines/parents/schedules/sets-schedule.html (accessed on 7 February 2020).
- Centers for Disease Control and Prevention. Easy-to-read Immunization Schedule by Vaccine for Ages Birth-6 Years. (2020, February 3). Available online: https://www.cdc.gov/vaccines/schedules/easy-to-read/child-easyread.html (accessed on 7 February 2020).
- Leask, J.; Kinnersley, P.; Jackson, C.; Cheater, F.; Bedford, H.; Rowles, G. Communicating with parents about vaccination: A framework for health professionals. BMC Pediatr. 2012, 12, 154. [Google Scholar] [CrossRef] [PubMed]
- Oduwole, O.E.; Pienaar, E.D.; Mahomed, H.; Iwu, C.J. Current tools available for investigating vaccine hesitancy: A scoping review protocol. BMJ Open 2019, 9, e033245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larson, H.J.; Schulz, W.S.; Tucker, J.D.; Smith, D.M.D. Measuring Vaccine Confidence: Introducing a Global Vaccine Confidence Index. PLoS Curr. 2015, 7, e033245. [Google Scholar] [CrossRef]
- Gilkey, M.B.; Magnus, B.E.; Reiter, P.L.; McRee, A.-L.; Dempsey, A.F.; Brewer, N.T. The Vaccination Confidence Scale: A brief measure of parents’ vaccination beliefs. Vaccine 2014, 32, 6259–6265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, G.K.; Tatar, O.; Dubé, E.; Amsel, R.; Knäuper, B.; Naz, A.; Perez, S.; Rosberger, Z. The vaccine hesitancy scale: Psychometric properties and validation. Vaccine 2018, 36, 660–667. [Google Scholar] [CrossRef]
- Opel, D.J.; Mangione-Smith, R.; Taylor, J.A.; Korfiatis, C.; Wiese, C.; Catz, S.; Martin, D.P. Development of a survey to identify vaccine-hesitant parents. Hum. Vaccines 2011, 7, 419–425. [Google Scholar] [CrossRef] [Green Version]
- Opel, D.J.; Taylor, J.A.; Zhou, C.; Catz, S.; Myaing, M.; Mangione-Smith, R. The Relationship between Parent Attitudes About Childhood Vaccines Survey Scores and Future Child Immunization Status. JAMA Pediatr. 2013, 167, 1065. [Google Scholar] [CrossRef] [Green Version]
- Cunningham, R.M.; Minard, C.G.; Guffey, D.; Swaim, L.S.; Opel, D.J.; Boom, J.A. Prevalence of Vaccine Hesitancy Among Expectant Mothers in Houston, Texas. Acad. Pediatr. 2018, 18, 154–160. [Google Scholar] [CrossRef]
- Glanz, J.M.; Wagner, N.M.; Narwaney, K.J.; Kraus, C.R.; Shoup, J.A.; Xu, S.; O’Leary, S.T.; Omer, S.B.; Gleason, K.S.; Daley, M.F. Web-based Social Media Intervention to Increase Vaccine Acceptance: A Randomized Controlled Trial. Pediatrics 2017, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henrikson, N.B.; Opel, D.J.; Grothaus, L.; Nelson, J.; Scrol, A.; Dunn, J.; Faubion, T.; Roberts, M.; Marcuse, E.K.; Grossman, D.C. Physician Communication Training and Parental Vaccine Hesitancy: A Randomized Trial. Pediatrics 2015, 136, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Williams, S.E.; Rothman, R.L.; Offit, P.A.; Barnett, E.; Sullivan, M.; Edwards, K.M. A Randomized Trial to Increase Acceptance of Childhood Vaccines by Vaccine-Hesitant Parents: A Pilot Study. Acad. Pediatr. 2013, 13, 475–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leask, J. Improving communication about vaccination. (2015, May 12). Available online: https://julieleask.wordpress.com/2015/05/12/improving-communication-about-vaccination-sarah/ (accessed on 2 November 2019).
- Leask, J.; Willaby, H.W.; Kaufman, J. The big picture in addressing vaccine hesitancy. Hum. Vaccines Immunother. 2014, 10, 2600–2602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, A.; Robinson, K.; Vallée-Tourangeau, G. The 5As: A practical taxonomy for the determinants of vaccine uptake. Vaccine 2016, 34, 1018–1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomson, A.; Vallée-Tourangeau, G.; Suggs, L.S. Strategies to increase vaccine acceptance and uptake: From behavioral insights to context-specific, culturally-appropriate, evidence-based communications and interventions. Vaccine 2018, 36, 6457–6458. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.; Ames, H.; Bosch-Capblanch, X.; Cartier, Y.; Cliff, J.; Glenton, C.; Lewin, S.; Muloliwa, A.M.; Oku, A.; Oyo-Ita, A.; et al. The comprehensive ‘Communicate to Vaccinate’ taxonomy of communication interventions for childhood vaccination in routine and campaign contexts. BMC Public Health 2017, 17, 423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gowda, C.; Schaffer, S.E.; Kopec, K.; Markel, A.; Dempsey, A.F. A pilot study on the effects of individually tailored education for MMR vaccine-hesitant parents on MMR vaccination intention. Hum. Vaccines Immunother. 2013, 9, 437–445. [Google Scholar] [CrossRef]
- Jolley, D.; Douglas, K.M. Prevention is better than cure: Addressing anti-vaccine conspiracy theories. J. Appl. Soc. Psychol. 2017, 47, 459–469. [Google Scholar] [CrossRef]
- Frew, P.M.; Lutz, C.S. Interventions to increase pediatric vaccine uptake: An overview of recent findings. Hum. Vaccines Immunother. 2017, 13, 2503–2511. [Google Scholar] [CrossRef] [Green Version]
- Schoeppe, J.; Melton, M.; Faubion, T.; Miller, C.; Matthys, J.; Hsu, C.; Cheadle, A. The Immunity Community: A Community Engagement Strategy for Reducing Vaccine Hesitancy. Health Promot. Pract. 2017, 18, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Attwell, K.; Freeman, M. I Immunise: An evaluation of a values-based campaign to change attitudes and beliefs. Vaccine 2015, 33, 6235–6240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daley, M.F.; Narwaney, K.; Shoup, J.A.; Wagner, N.M.; Glanz, J.M. Addressing Parents’ Vaccine Concerns: A Randomized Trial of a Social Media Intervention. Am. J. Prev. Med. 2018, 55, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Gagneur, A.; Lemaître, T.; Gosselin, V.; Farrands, A.; Carrier, N.; Petit, G.; Valiquette, L.; De Wals, P. A postpartum vaccination promotion intervention using motivational interviewing techniques improves short-term vaccine coverage: PromoVac study. BMC Public Health 2018, 18, 811. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.C.; Fredrickson, D.D.; Bocchini, C.; Arnold, C.L.; Green, K.W.; Humiston, S.G.; Wilder, E.; Bocchini, J.A. Improving vaccine risk/benefit communication with an immunization education package: A pilot study. Ambul. Pediatr. 2002, 2, 193–200. [Google Scholar] [CrossRef]
- Berry, N.; Danchin, M.; Trevena, L.; Witteman, H.; Kinnersley, P.; Snelling, T.; Robinson, P.; Leask, J. Sharing knowledge about immunization (SKAI): An exploration of parents’ communication needs to inform development of a clinical communication support intervention. Vaccine 2018, 36, 6480–6490. [Google Scholar] [CrossRef] [PubMed]
- Salmon, A.D.; Limaye, R.J.; Dudley, M.Z.; Oloko, O.K.; Church-Balin, C.; Ellingson, M.K.; Spina, C.I.; Brewer, S.E.; Orenstein, W.A.; Halsey, N.A.; et al. MomsTalkShots: An individually tailored educational application for maternal and infant vaccines. Vaccine 2019, 37, 6478–6485. [Google Scholar] [CrossRef]
- Sowers, C. Influencing Parental Intent to Immunize through Prenatal Education. Doctoral Dissertation, Catholic University of America, Washington, DC, USA, 2017. [Google Scholar]
- Wang, E.; Baras, Y.; Buttenheim, A. “Everybody just wants to do what’s best for their child”: Understanding how pro-vaccine parents can support a culture of vaccine hesitancy. Vaccine 2015, 33, 6703–6709. [Google Scholar] [CrossRef] [Green Version]
- Ames, H.M.; Glenton, C.; Lewin, S. Parents’ and informal caregivers’ views and experiences of communication about routine childhood vaccination: A synthesis of qualitative evidence. Cochrane Database Syst. Rev. 2017, 2, CD011787. [Google Scholar] [CrossRef] [Green Version]
- Bedford, H. Pro-vaccine messages may be counterproductive among vaccine-hesitant parents. Evid. Based Med. 2014, 19, 219. [Google Scholar] [CrossRef]
- Healy, C.M.; Pickering, L.K. How to Communicate With Vaccine-Hesitant Parents. Pediatrics 2011, 127, S127–S133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nour, R. A Systematic Review of Methods to Improve Attitudes Towards Childhood Vaccinations. Cureus 2019, 11, e5067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tafuri, S.; Gallone, M.; Cappelli, M.; Martinelli, D.; Prato, R.; Germinario, C. Addressing the anti-vaccination movement and the role of HCWs. Vaccine 2014, 32, 4860–4865. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.; Dubé, E.; Driedger, M. Vaccine Hesitancy: In Search of the Risk Communication Comfort Zone. PLoS Curr. 2017, 9. [Google Scholar] [CrossRef]
- Lwembe, S.; Green, S.A.; Tanna, N.; Connor, J.; Valler, C.; Barnes, R. A qualitative evaluation to explore the suitability, feasibility and acceptability of using a ’celebration card’ intervention in primary care to improve the uptake of childhood vaccinations. BMC Fam. Pract. 2016, 17, 101. [Google Scholar] [CrossRef] [Green Version]
- Kempe, A.; Daley, M.F.; McCauley, M.M.; Crane, L.A.; Suh, C.A.; Kennedy, A.M.; Basket, M.M.; Stokley, S.K.; Dong, F.; Babbel, C.I.; et al. Prevalence of Parental Concerns About Childhood Vaccines. Am. J. Prev. Med. 2011, 40, 548–555. [Google Scholar] [CrossRef]
- Dubé, E.; Vivion, M.; Sauvageau, C.; Gagneur, A.; Gagnon, R.; Guay, M. Nature Does Things Well, Why Should We Interfere? Qual. Health Res. 2015, 26, 411–425. [Google Scholar] [CrossRef]
- Stevens, J.C. The C.A.S.E. Approach (Corroboration, about Me, Science, Explain/Advise): Improving Communication with Vaccine-Hesitant Parents. Doctoral Dissertation, The University of Arizona, Tucson, AZ, USA, 2016. [Google Scholar]
- Broniatowski, D.A.; Hilyard, K.M.; Dredze, M. Effective vaccine communication during the disneyland measles outbreak. Vaccine 2016, 34, 3225–3228. [Google Scholar] [CrossRef] [Green Version]
- Meppelink, C.S.; Smit, E.G.; Fransen, M.L.; Diviani, N. “I was Right about Vaccination”: Confirmation Bias and Health Literacy in Online Health Information Seeking. J. Health Commun. 2019, 24, 129–140. [Google Scholar] [CrossRef] [Green Version]
- Moran, M.B.; Lucas, M.; Everhart, K.; Morgan, A.; Prickett, E. What makes anti-vaccine websites persuasive? A content analysis of techniques used by anti-vaccine websites to engender anti-vaccine sentiment. J. Commun. Health 2016, 9, 151–163. [Google Scholar] [CrossRef]
- Reyna, V.F. Risk perception and communication in vaccination decisions: A fuzzy-trace theory approach. Vaccine 2012, 30, 3790–3797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attwell, K.; Smith, D.T. Parenting as politics: Social identity theory and vaccine hesitant communities. Int. J. Health Gov. 2017, 22, 183–198. [Google Scholar] [CrossRef]
- Brunson, E.K. The impact of social networks on parents’ vaccination decisions. Pediatrics 2013, 131, e1397–e1404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weigmann, K. An injection of confidence: Scientists explore new and old methods to counter anti-vaccine propaganda and overcome vaccine hesitancy so as to increase vaccination rates. EMBO Rep. 2017, 18, 21–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [Green Version]
- Goldstein, S.; Macdonald, N.E.; Guirguis, S. Health communication and vaccine hesitancy. Vaccine 2015, 33, 4212–4214. [Google Scholar] [CrossRef] [Green Version]
- Dubé, E.; Gagnon, D.; Macdonald, N.E. Strategies intended to address vaccine hesitancy: Review of published reviews. Vaccine 2015, 33, 4191–4203. [Google Scholar] [CrossRef] [Green Version]
- Harvey, H.; Reissland, N.; Mason, J. Parental reminder, recall and educational interventions to improve early childhood immunisation uptake: A systematic review and meta-analysis. Vaccine 2015, 33, 2862–2880. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.F.; Kroll, J.S.; Hudson, M.J.; Ramsay, M.; Green, J.; Long, S.J.; Vincent, C.J.; Fraser, G.; Sevdalis, N. Factors underlying parental decisions about combination childhood vaccinations including MMR: A systematic review. Vaccine 2010, 28, 4235–4248. [Google Scholar] [CrossRef]
- McKee, C.; Bohannon, K. Exploring the Reasons Behind Parental Refusal of Vaccines. J. Pediatr. Pharmacol. Ther. 2016, 21, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Fadda, M.; Galimberti, E.; Fiordelli, M.; Romanò, L.; Zanetti, A.; Schulz, P.J. Effectiveness of a smartphone app to increase parents’ knowledge and empowerment in the MMR vaccination decision: A randomized controlled trial. Hum. Vaccines Immunother. 2017, 13, 2512–2521. [Google Scholar] [CrossRef]
- Shelby, A.; Ernst, K. Story and science: How providers and parents can utilize storytelling to combat anti-vaccine misinformation. Hum. Vaccines Immunother. 2013, 9, 1795–1801. [Google Scholar] [CrossRef] [Green Version]
- Shoup, J.A.; Wagner, N.M.; Kraus, C.R.; Narwaney, K.J.; Goddard, K.S.; Glanz, J.M. Development of an Interactive Social Media Tool for Parents With Concerns About Vaccines. Health Educ. Behav. 2014, 42, 302–312. [Google Scholar] [CrossRef]
- Dempsey, A.F.; Wagner, N.; Narwaney, K.; Pyrzanowski, J.; Kwan, B.M.; Kraus, C.; Gleason, K.; Resnicow, K.; Sevick, C.; Cataldi, J.; et al. ‘Reducing Delays In Vaccination’ (REDIVAC) trial: A protocol for a randomised controlled trial of a web-based, individually tailored, educational intervention to improve timeliness of infant vaccination. BMJ Open 2019, 9, e027968. [Google Scholar] [CrossRef] [PubMed]
- Sadique, Z.; Devlin, N.; Edmunds, W.J.; Parkin, D. The Effect of Perceived Risks on the Demand for Vaccination: Results from a Discrete Choice Experiment. PLoS ONE 2013, 8, e54149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seeber, L.; Conrad, T.; Hoppe, C.; Obermeier, P.; Chen, X.; Karsch, K.; Muehlhans, S.; Tief, F.; Böttcher, S.; Diedrich, S.; et al. Educating parents about the vaccination status of their children: A user-centered mobile application. Prev. Med. Rep. 2017, 5, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Wagner, N.M. Assessing the Value of the Vaccine Social Media Intervention through the Re-aim Framework Implementation Dimension. Doctoral Dissertation, University of Colorado, Boulder, CO, USA, 2019. [Google Scholar]
- Moyer-Gusé, E.; Robinson, M.J.; McKnight, J. The Role of Humor in Messaging about the MMR Vaccine. J. Health Commun. 2018, 23, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Haydarov, R.; Gordon, J.C. Effect of combining attribute and goal framing within messages to change vaccination behavior. J. Commun. Health 2015, 8, 45–54. [Google Scholar] [CrossRef]
- Kennedy, A.; Glasser, J.; Covello, V.; Gust, D. Development of Vaccine Risk Communication Messages Using Risk Comparisons and Mathematical Modeling. J. Health Commun. 2008, 13, 793–807. [Google Scholar] [CrossRef]
- O’Keefe, D.J.; Nan, X. The Relative Persuasiveness of Gain- and Loss-Framed Messages for Promoting Vaccination: A Meta-Analytic Review. Health Commun. 2012, 27, 776–783. [Google Scholar] [CrossRef]
- Nyhan, B.; Reifler, J.; Richey, S.; Freed, G.L. Effective Messages in Vaccine Promotion: A Randomized Trial. Pediatrics 2014, 133, e835–e842. [Google Scholar] [CrossRef] [Green Version]
- Amin, A.B.; Bednarczyk, R.A.; Ray, C.E.; Melchiori, K.J.; Graham, J.; Huntsinger, J.R.; Omer, S.B. Association of moral values with vaccine hesitancy. Nat. Hum. Behav. 2017, 1, 873–880. [Google Scholar] [CrossRef]
- Lorini, C.; Santomauro, F.; Donzellini, M.; Capecchi, L.; Bechini, A.; Boccalini, S.; Bonanni, P.; Bonaccorsi, G. Health literacy and vaccination: A systematic review. Hum. Vaccines Immunother. 2017, 14, 478–488. [Google Scholar] [CrossRef] [Green Version]
- Ratzan, S.C. Vaccine Literacy: A New Shot for Advancing Health. J. Health Commun. 2011, 16, 227–229. [Google Scholar] [CrossRef]
- Nowak, G.J.; Gellin, B.G.; Macdonald, N.E.; Butler, R. Addressing vaccine hesitancy: The potential value of commercial and social marketing principles and practices. Vaccine 2015, 33, 4204–4211. [Google Scholar] [CrossRef] [Green Version]
- Stockwell, M.S.; Fiks, A.G. Utilizing health information technology to improve vaccine communication and coverage. Hum. Vaccines Immunother. 2013, 9, 1802–1811. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Type of Ingredient | Example(s) | Purpose |
|---|---|---|
| Preservatives | Thimerosal (only in multi-dose vials of flu vaccine) | To prevent contamination |
| Adjuvants | Aluminum salts * | To help boost the body’s response to the vaccine |
| Stabilizers | Sugars, gelatin | To keep the vaccine effective after manufacture |
| Residual cell culture materials | Egg protein | To grow enough of the virus or bacteria to make the vaccine |
| Residual inactivating ingredients | Formaldehyde | To kill viruses or inactivate toxins during the manufacturing process |
| Residual antibiotics | Neomycin | To prevent contamination by bacteria during the vaccine manufacturing process |
| Birth | 1 Month | 2 Months | 4 Months | 6 Months | 12 Months | 15 Months | 18 Months | 19–23 Months | 2–3 Years | 4–6 Years |
|---|---|---|---|---|---|---|---|---|---|---|
| HepB | HepB | - | HepB | - | - | - | ||||
| - | - | RV | RV | RV | - | - | - | - | - | - |
| - | - | DTaP | DTaP | DTaP | - | DTaP | - | - | DTaP | |
| - | - | Hib | Hib | Hib | Hib | - | - | - | - | |
| - | - | PCV13 | PCV13 | PCV13 | PCV13 | - | - | - | - | |
| - | - | IPV | IPV | IPV | - | - | IPV | |||
| - | - | - | - | Influenza (Yearly) * | ||||||
| - | - | - | - | - | MMR | - | - | - | - | MMR |
| - | - | - | - | - | Varicella | - | - | - | - | Varicella |
| - | - | - | - | - | HepA | - | - | |||
| Target Population | Children and Parents |
|---|---|
| Vaccine hesitancy | Parental vaccine concerns, vaccine refusal and delay, childhood vaccines, alternative vaccine schedules |
| Determinants of vaccine hesitancy | Vaccine attitudes, vaccine behaviors, vaccine decisions vaccine risk perceptions |
| Addressing vaccine hesitancy | Vaccine confidence, vaccine acceptability, vaccine promotion, vaccine communication, addressing/preventing vaccine hesitancy, intervention strategies, pro-vaccine messages |
| CONTEXTUAL INFLUENCES Influences arising due to historic, socio-cultural, environmental, health system/institutional, economic, or political factors |
|
| INDIVIDUAL AND GROUP INFLUENCES Influences arising from personal perception of the vaccine or influences of the social/peer environment |
|
| VACCINE/VACCINATION-SPECIFIC ISSUES Directly related to vaccine or vaccination |
|
| Messenger | Evidence from the Literature |
|---|---|
| Health Care Professionals | Health care professionals (HCP) are cited as the most important source for receiving vaccination information for parents. They are seen as trustworthy, informative, and a reliable source for answering questions and concerns parents have about childhood vaccines. HCP’s communication styles with parents are important. Poor communication and negative relationships with HCP can heavily impact parents’ vaccination decisions. Furthermore, HCP’s behavior and opinions about vaccination influence parents’ acceptance of vaccination. HCP may not always be best equipped or have the time to address the emerging issue of parental vaccine hesitancy. This is especially true when parental questions and concerns arise from very persuasive misinformation found on the Internet and from their social network, which has proven difficult to counter and correct based on numerous studies. The literature suggests that if HCP refuse parents’ requests to delay vaccines, be selective with vaccines, or alter the recommended childhood vaccine schedule, parents will continue to search for other HCP or alternative health professionals. However, literature also suggests that if vaccination is presented as the default approach and HCP engage in open discussion with parents about vaccines early and often, parents are more likely to vaccinate their children [4,14,15,23,25,27,34,58,59,61,63,73,77,78,79,80,81,82,83,84,85,86]. |
| Internet and Social Media (Web 2.0) | Parents often cite that the Internet and social media are trusted sources of vaccination information. In one study, up to 72% of American internet users trusted health information obtained on the Internet, and 75% evaluated the source of information only sometimes or never. This poses a tremendous threat and opportunity for individuals to be influenced by false or misleading information about vaccines [38,59,70,76,80,87,88,89,90]. |
| Family and Friends | A parent’s social network plays an important role in their attitudes and beliefs about vaccines and their intention to vaccinate their child. A parent’s social network can include family, friends, colleagues, neighbors, and other personal relationships. It is found in the literature that a parent’s social network can even be more predictive of a parent’s decision to vaccinate their child than any other variable, including the parent’s own perceptions of vaccination. When vaccination is viewed as the social norm in that parent’s social network, social pressure and responsibility act as a powerful driver of vaccine uptake [4,15,59,61,76,91,92,93,94]. |
| Religious and Community Leaders | Religious and community leaders have proven to be effective messengers for motivating parents to vaccinate or not vaccinate their child. Vaccine refusal has been linked to moral convictions and philosophical beliefs such as a preference for natural over artificial medicines. Therefore, for specific populations, it may be important to identify religious and community influences in order to successfully deliver vaccination information and tailor specific interventions [4,19,27,75,95]. |
| Health Authorities and Government Authorities | Health authorities and government authorities are cited as one of the most common barriers to vaccine acceptance for some vaccine-hesitant populations. This is due to a lack of trust in the messenger due to many reasons including political, social, historical, etc. However, during outbreaks of vaccine-preventable diseases, traditional media and government websites are often used, despite the widely held belief that social media is replacing these legacy news organizations/authorities [4,19,24,26,82,86,93]. |
| Vaccine Topic | Evidence from the Literature |
|---|---|
| Science of Vaccines | Parents want up-to-date information on current scientific information, research, and statistics related to past and current vaccines [35,63,77,82,89,101]. |
| Vaccine Safety | Parents want to be informed about the safety of vaccines. This includes information about common vaccine side-effects and their severity. Furthermore, parents want vaccine information to be balanced; they want information about both the benefits and the risks of vaccines. Parents report that they are overwhelmingly informed about the benefits and under-informed about the risks, which leads them to be skeptical. Parents also want information about how to mitigate the pain that is inflicted on their child when receiving a vaccine. There are clinically based guidelines that have been developed to reduce vaccination-associated pain. Parents want to be educated about pain management for vaccine injection before or on the day of vaccination [14,19,25,26,27,32,77,81,82,93,102]. |
| Vaccine Ingredients | Parents want information about the ingredients in vaccines. In particular, they want to know the purpose of each ingredient and if those ingredients are toxic and unsafe [23,26,32,77,79]. |
| Combined versus Single Vaccines | Parents want information about vaccine dosage and the differences between combined and single vaccines [25,26,27,65,77]. |
| The Childhood Vaccine Schedule | Parents want information about the reasons behind the childhood vaccine schedule: clarification on the quantity and timing of vaccines [25,27,73,75,76,77,85,103]. |
| The Diseases that Vaccines Prevent | Parents may lack knowledge about how vaccinations work and the diseases they prevent. Today’s generation of parents may not have first-hand knowledge of once-deadly infectious diseases that are now prevented by vaccines [19,23,65,77,79]. |
| Technical Information on Vaccine Production and Delivery | Parents want more information about the names of vaccines, how vaccines have been tested, the proper storage of vaccines, the country of manufacture, and the quality control/evaluation measures for production and delivery [35,77]. |
| Vaccine Policies, Recommendations, and Costs | Parents want to know the reasons behind why some policies and recommendations differ for different communities, school districts, etc. [35,77]. |
| Alternatives to Vaccines | Some parents are exploring alternatives to vaccines such as homeopathic treatments. Parents want information about the effectiveness and safety of vaccines compared to other alternatives [4,35,49,76,85,89,93]. |
| Myths about Vaccines | Parents are concerned when faced with myths and controversies about childhood vaccines. Examples of major vaccine myths circulating today include the ideas that vaccines cause autism, and mercury in vaccines act as a neurotoxin. Parents want clarification about why these myths exist and scientific evidence and expert advice on how to recognize vaccine misinformation [18,26,82,89,93,97]. |
| Message-Framing Technique | Evidence from the Literature |
|---|---|
| Storytelling | Storytelling and the use of personal narratives when communicating vaccination information is a powerful messaging tool. It has more famously been used in anti-vaccination messaging to spread fear about childhood vaccinations. Two examples of pro-vaccine studies that have utilized storytelling include the Seattle Mama Doc and Moms Who Vax [25,27,38,63,78,80,89,93,101,104,105]. |
| Gists | Gists or the bottom-line meaning of messaging is critical in storytelling messaging. Stories without gists may not be as effective. Examples of gists used in vaccine messaging include “there is no chance that mercury in vaccines can cause autism, since it is not in vaccines anymore” or “if you do not vaccinate your child, there is a real chance that they could get sick”. Messages about vaccines that express a clear gist are arguably more compelling compared to messages without gists. In general, gists are also more likely to be shared on Facebook and other social media platforms than verbatim statistics [38,63,87,90,97,102,105,106]. |
| Emotive Anecdotes and Emotive Imagery | Emotive anecdotes and emotive imagery in messaging are cited as one of the most persuasive and effective message-framing strategies to communicate vaccine information. An anecdote is a short amusing or interesting story about a real incident or person that has a point to make. The emotive anecdote is the use of emotive language and images to have a greater emotional impact on the audience [18,24,38,79,80,84,86,87,89,90,100,101,102]. |
| Gamified Messaging | Offering parents a gamified learning experience can significantly contribute to knowledge gain in the context of vaccination. This is a new and developing message-framing technique being used in this field with promising initial results [100]. |
| Tone | Compared to more serious messaging, satirical messaging and humor has been shown to reduce psychological reactance, leading to greater perceptions of disease severity and less vaccine hesitancy. While humor can reduce psychological reactance, it is not an effective strategy among parents who already hold favorable beliefs about vaccination. Among parents who are not vaccine hesitant, the use of humor in messaging is less effective and can even be counter effective in positively influencing parents’ attitudes, beliefs, and intentions towards childhood vaccinations. In addition to the use of humor, the use of enthusiasm in the messenger’s tone when delivering vaccine communication is often received more positively among parents compared to unenthusiastic communication. This has been shown in the motivational interviewing techniques used in interventions aimed at new mothers [71,81,107,108]. |
| Gain versus Loss Goal Framing | Gain versus loss goal framing is well studied in the literature as an important health communication message-framing technique. For vaccination messaging, the hypothesis is that loss-framed messages that present the negative consequences of not performing a behavior are more persuasive for disease-detection behaviors, and gain-framed messages, which present the positive consequences of performing a behavior, are more persuasive for preventive behaviors. It is argued that because vaccination may be considered risky given the possibility of side effects, loss-framed messages might be more effective. There is mixed evidence that loss-framed messaging is more effective than gain-framed messaging for vaccination information. Some studies affirm that loss-framed messages have the greatest impact, other studies find that a combination of gain- and loss-framed messaging is most effective, and other studies find no overall difference between loss- and gain-framed messaging [27,35,36,67,108,109,110]. |
| Fear-Based Messaging | Fear-based messaging is more often than not viewed as counterproductive in reducing vaccine hesitancy by several studies. By contrast, fear-based messaging has been extremely effective in anti-vaccination messaging [18,24,80,86,93,97,111]. |
| Co-Promoted Behavioral Messaging | Co-promoted behavioral messaging is effective in framing vaccines as part of a holistic health plan for the child. Pairing pro-vaccine messages with messages such as breastfeeding and healthy eating has been shown to be effective. Furthermore, research has shown that it is advantageous to appeal to the target audiences’ values in order to change behaviors. Vaccine decisions are value-based decisions, and the goal should be not to change values but to change behaviors [69,89,91,96,102,112]. |
| Statistical Information | Statistical information and (“verbatim”) statements on probabilities about vaccines are not as effective on their own and are not found to be as powerful as using anecdotes and emotion-based messaging techniques. The use of statistical information and probabilistic information is most often used by medical and public health authorities in their communication about vaccines. This message-framing technique is also more commonly used in the knowledge-deficit approach to address vaccine hesitancy [4,18,24,38,63,86,87,93,101,104]. |
| Science-Based Messaging | Messaging with references to scientific studies and references to the science of vaccines is cited with a high level of support from parents. However, parents have reported high levels of support for science-based messaging but not when science-based jargon is used. Parents want to be able to understand the science of vaccines in plain language [35,82,89,101]. |
| Expert Opinion | Expert opinion (i.e., an article written by a “doctor” or “scientist”) messaging has been shown to be powerful. Some interventions show that messaging including quotes from doctors and individuals seen as experts in the field of vaccines is very persuasive [89,102]. |
| Misconceptions about Childhood Vaccination | Evidence from the Literature |
|---|---|
| Natural Immunity is Better than Vaccine-Acquired Immunity | Some vaccine-hesitant parents claim that natural immunity is better than immunity induced by vaccines, which they believe are “toxins”. Other vaccine-hesitant parents claim that most vaccine-preventable diseases are harmless to most children in the U.S. today, and natural exposure provides more long-lasting immunity [19,22,25,76,84,95,105]. |
| Too Many Immunizations Overload the Immune System | Some vaccine-hesitant parents claim that vaccines “overwhelm” the immune system and that the childhood vaccine schedule involves too many vaccines, too soon. There is a belief that in following the recommended vaccine schedule for children, the immune system becomes “overwhelmed” and this leads to autism and an assortment of chronic health conditions [19,22,25,49,65,79,84,85,91,105]. |
| Vaccines Contain Harmful Ingredients and Cause Serious Side Effects | Some vaccine-hesitant parents often state that vaccines are more dangerous than the infectious diseases that vaccines prevent. Vaccine-hesitant parents believe strongly that the toxins in vaccines can lead to an assortment of chronic health conditions that are more dangerous than vaccine-preventable diseases such as measles, mumps, and rubella (MMR) [23,25,26,77]. |
| Many of the Vaccine-Preventable Diseases Are Uncommon in the United States Now | Until recently with the 2020 COVID-19 pandemic in the U.S., most parents today never had first-hand experience with infectious disease outbreaks. Therefore, it has been cited that either the side effects of the vaccines themselves appear more concerning than the diseases that the vaccines prevent, or parents believe vaccines are not needed [19,23,85]. |
| There Are Alternatives to Vaccines | Some vaccine-hesitant parents believe that there are alternative to vaccines that are more effective and safer than vaccines for protecting children’s health. Vaccine-hesitant parents may seek counseling and information from alternative medicine practitioners such as homeopaths and naturopaths to justify alternative to vaccines [49,69,76,85,91]. |
| Pharmaceutical Companies and Medical Science are not Trustworthy | Some vaccine-hesitant parents believe that pharmaceutical companies are using vaccines as a tool to profit without consideration of the harm to children. Some parents also have distrust in the medical science behind vaccines and believe that the research on vaccines is outdated and inaccurate and vaccines have not been tested properly and therefore are not safe [22,24,27,82,86]. |
| Vaccines Cause Autism | A significant number of vaccine-hesitant parents believe, or are uncertain, about the scientifically unproven link between vaccines and autism. [18,26,82,89,93,97]. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olson, O.; Berry, C.; Kumar, N. Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies. Vaccines 2020, 8, 590. https://doi.org/10.3390/vaccines8040590
Olson O, Berry C, Kumar N. Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies. Vaccines. 2020; 8(4):590. https://doi.org/10.3390/vaccines8040590
Chicago/Turabian StyleOlson, Olivia, Corinne Berry, and Nirbhay Kumar. 2020. "Addressing Parental Vaccine Hesitancy towards Childhood Vaccines in the United States: A Systematic Literature Review of Communication Interventions and Strategies" Vaccines 8, no. 4: 590. https://doi.org/10.3390/vaccines8040590