
The Safety of mRNA-1273, BNT162b2 and JNJ-78436735 COVID-19 Vaccines: Safety Monitoring for Adverse Events Using Real-World Data

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
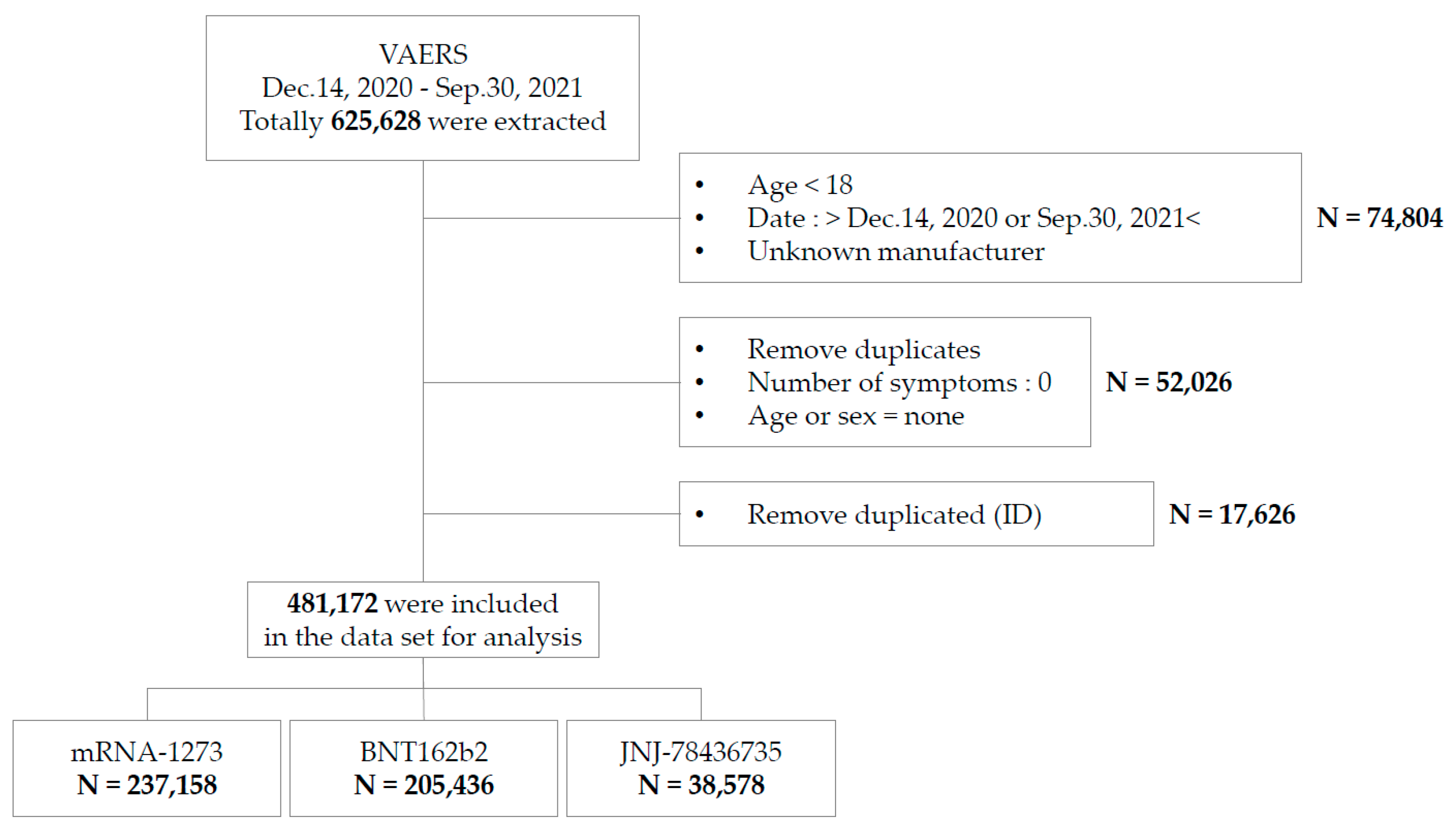
2.2. Setting and Study Population
2.3. Chosen Severe AEs
2.4. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Common AEs
3.3. Severe AEs
3.3.1. Central Nervous Disorders
3.3.2. Respiratory Disorders
3.3.3. Cardiac Disorders
3.3.4. Gastrointestinal Disorders
3.3.5. Hematologic Disorders
3.3.6. Correlation Analysis between Death and Severe AEs
3.4. Serious Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nassar, A.; Ibrahim, I.M.; Amin, F.G.; Magdy, M.; Elgharib, A.M.; Azzam, E.B.; Nasser, F.; Yousry, K.; Shamkh, I.M.; Mahdy, S.M.; et al. A Review of Human Coronaviruses’ Receptors: The Host-Cell Targets for the Crown Bearing Viruses. Molecules 2021, 26, 6455. [Google Scholar] [CrossRef] [PubMed]
- Klein, N.P.; Lewis, N.; Goddard, K.; Fireman, B.; Zerbo, O.; Hanson, K.E.; Donahue, J.G.; Kharbanda, E.O.; Naleway, A.; Nelson, J.C.; et al. Surveillance for adverse events after COVID-19 mRNA vaccination. JAMA 2021, 326, 1390–1399. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; et al. Comparative effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) vaccines in preventing COVID-19 hospitalizations among adults without immunocompromising conditions—United States, March–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Nguyen, M.; Martin, D.; DeStefano, F. Safety monitoring in the vaccine adverse event reporting system (VAERS). Vaccine 2015, 33, 4398–4405. [Google Scholar] [CrossRef] [Green Version]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernan, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 vaccine in a nationwide setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Singh, A.; Khillan, R.; Mishra, Y.; Khurana, S. The Safety profile of COVID-19 vaccinations in the United States. Am. J. Infect. Control 2022, 50, 15–19. [Google Scholar] [CrossRef]
- Liu, C.; Lee, J.; Ta, C.; Soroush, A.; Rogers, J.R.; Kim, J.H.; Natarajan, K.; Zucker, J.; Weng, C. A Retrospective Analysis of COVID-19 mRNA Vaccine Breakthrough Infections-Risk Factors and Vaccine Effectiveness. medRxiv, 2021; Prepint. [Google Scholar] [CrossRef]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef]
- Cari, L.; Alhosseini, M.N.; Fiore, P.; Pierno, S.; Pacor, S.; Bergamo, A.; Sava, G.; Nocentini, G. Cardiovascular, neurological, and pulmonary events following vaccination with the BNT162b2, ChAdOx1 nCoV-19, and Ad26.COV2.S vaccines: An analysis of European data. J. Autoimmun. 2021, 125, 102742. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Lee, J.Y.; Yi, S.Y. Axillary Lymphadenopathy on Ultrasound after COVID-19 Vaccination and Its Influencing Factors: A Single-Center Study. J. Clin. Med. 2022, 11, 238. [Google Scholar] [CrossRef] [PubMed]
- Patone, M.; Mei, X.W.; Handunnetthi, L.; Dixon, S.; Zaccardi, F.; Shankar-Hari, M.; Watkinson, P.; Khunti, K.; Harnden, A.; Coupland, C.A.C.; et al. Risks of myocarditis, pericarditis, and cardiac arrhythmias associated with COVID-19 vaccination or SARS-CoV-2 infection. Nat. Med. 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Albalawi, O.M.; Alomran, M.I.; Alsagri, G.M.; Althunian, T.A.; Alshammari, T.M. Analyzing the U.S. Post-marketing safety surveillance of COVID-19 vaccines. Saudi Pharm. J. 2022, 30, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Beatty, A.L.; Peyser, N.D.; Butcher, X.E.; Cocohoba, J.M.; Lin, F.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Analysis of COVID-19 Vaccine Type and Adverse Effects Following Vaccination. JAMA Netw. Open 2021, 4, e2140364. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. Influenza; Data Are for the U.S. 2021. Available online: https://www.cdc.gov/nchs/fastats/flu.htm (accessed on 19 December 2021).
- Somiya, M.; Mine, S.; Yasukawa, K.; Ikeda, S. Sex differences in the incidence of anaphylaxis to LNP-mRNA COVID-19 vaccines. Vaccine 2021, 39, 3313–3314. [Google Scholar] [CrossRef]
- McNeil, M.M.; Weintraub, E.S.; Duffy, J.; Sukumaran, L.; Jacobsen, S.; Klein, N.P.; Hambidge, S.J.; Lee, G.M.; Jackson, L.A.; Irving, S.A.; et al. Risk of anaphylaxis after vaccination in children and adults. J. Allergy Clin. Immunol. 2016, 137, 868–878. [Google Scholar] [CrossRef] [Green Version]
- Iskander, J.; Broder, K. Monitoring the safety of annual and pandemic influenza vaccines: Lessons from the US experience. Expert Rev. Vaccines 2008, 7, 75–82. [Google Scholar] [CrossRef]
- Gálvez, L.A.; Abadía, L.A.R.; Guevara, C.A.D.L.R.; Orozco, J.F.H. Guillain-Barre syndrome after vaccination for COVID-19. The first report in Latin America. Neurol. Perspect. 2021, 1, 236–238. [Google Scholar] [CrossRef]
- Fact Sheet for Healthcare Providers Administering Vaccine. Janssen COVID-19 Vaccine. 2021. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/janssen-covid-19-vaccine (accessed on 19 December 2021).
- Garg, R.K.; Paliwal, V.K. Spectrum of neurological complications following COVID-19 vaccination. Neurol. Sci. 2022, 43, 3–40. [Google Scholar] [CrossRef]
- Rosenblum, H.G.; Hadler, S.C.; Moulia, D.; Shimabukuro, T.T.; Su, J.R.; Tepper, N.K.; Ess, K.C.; Woo, E.J.; Mba-Jonas, A.; Alimchandani, M.; et al. Use of COVID-19 vaccines after reports of adverse events among adult recipients of Janssen (Johnson & Johnson) and mRNA COVID-19 vaccines (Pfizer-BioNTech and Moderna): Update from the Advisory Committee on Immunization Practices—United States, July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1094–1099. [Google Scholar]
- Yamaguchi, Y.; Kimihira, L.; Nagasawa, H.; Seo, K.; Wada, M. Cerebral Venous Sinus Thrombosis After BNT162b2 mRNA COVID-19 Vaccination. Cureus 2021, 13, e18775. [Google Scholar] [CrossRef] [PubMed]
- Syed, K.; Chaudhary, H.; Donato, A. Central Venous Sinus Thrombosis with Subarachnoid Hemorrhage Following an mRNA COVID-19 Vaccination: Are These Reports Merely Co-Incidental? Am. J. Case Rep. 2021, 22, e933397. [Google Scholar] [CrossRef] [PubMed]
- Schulz, J.B.; Berlit, P.; Diener, H.C.; Gerloff, C.; Greinacher, A.; Klein, C.; Petzold, G.C.; Piccininni, M.; Poli, S.; Röhrig, R.; et al. COVID-19 Vaccine-Associated Cerebral Venous Thrombosis in Germany. Ann. Neurol. 2021, 90, 627–639. [Google Scholar] [CrossRef] [PubMed]
- Hajjo, R.; Sabbah, D.A.; Bardaweel, S.K.; Tropsha, A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines 2021, 9, 1186. [Google Scholar] [CrossRef]


{kind=link}
| Severe AEs | Common AEs | |||||||
|---|---|---|---|---|---|---|---|---|
| mRNA-1273 | BNT162b2 | JNJ-78436735 | Sum | mRNA-1273 | BNT162b2 | JNJ-78436735 | Sum | |
| Female | ||||||||
| 18–24 | 454 | 565 | 118 | 1137 | 16,802 | 15,772 | 5908 | 38,482 |
| 25–39 | 2492 | 2983 | 378 | 5853 | 88,919 | 75,605 | 19,045 | 183,569 |
| 40–49 | 1914 | 2445 | 316 | 4675 | 69,034 | 56,110 | 12,668 | 137,812 |
| 50–64 | 2596 | 2762 | 509 | 5867 | 106,474 | 75,185 | 17,454 | 199,113 |
| 65–74 | 1388 | 1231 | 216 | 2835 | 65,980 | 29,710 | 3602 | 99,292 |
| ≥75 | 1196 | 1017 | 208 | 2421 | 28,884 | 12,201 | 980 | 42,065 |
| Sum (sex ratio, %) | 10,040 (51.8) | 11,003 (49.5) | 1745 (51.7) | 22,788 | 376,093 (51.2) | 264,583 (47.6) | 59,657 (43.8) | 700,333 |
| Male | ||||||||
| 18–24 | 418 | 591 | 128 | 1137 | 5409 | 5929 | 3957 | 15,295 |
| 25–39 | 966 | 1244 | 316 | 2526 | 21,342 | 21,565 | 8934 | 51,841 |
| 40–49 | 657 | 827 | 255 | 1739 | 14,487 | 14,012 | 4417 | 32,916 |
| 50–64 | 1249 | 1385 | 497 | 3131 | 26,787 | 19,985 | 6580 | 53,352 |
| 65–74 | 1033 | 928 | 191 | 2152 | 19,358 | 10,922 | 1541 | 31,821 |
| ≥75 | 1075 | 940 | 131 | 2146 | 10,866 | 5917 | 548 | 17,331 |
| Sum (sex ratio, %) | 5398 (55.8) | 5915 (52.5) | 1518 (50.6) | 12,831 | 98,249 (52.9) | 78,330 (48.7) | 25,977 (41.8) | 202,556 |
| Total * (per 100,000 people) | 15,438 (10.191) | 16,918 (7.485) | 3263 (21.753) | 35,619 (9.075) | 474,342 (313.135) | 342,913 (151.709) | 85,634 (570.881) | 902,889 † (230.026) |
| mRNA-1273 | BNT162b2 | JNJ-78436735 | ||||
|---|---|---|---|---|---|---|
| Symptom | Number | Incidence of Events (Onset Day-Median) | Number | Incidence of Events (Onset Day-median) | Number | Incidence of Events (Onset Day-Median) |
| Bell’s palsy | 1093 | 0.72 (8) | 1234 | 0.55 (7) | 204 | 1.36 (16) |
| Stroke, hemorrhagic | 77 | 0.05 (7) | 82 | 0.04 (7) | 36 | 0.24 (5) |
| Stroke, ischemic | 302 | 0.20 (7) | 334 | 0.15 (5) | 100 | 0.67 (10) |
| Encephalitis/myelitis/encephalomyelitis | 30 | 0.02 (6) | 33 | 0.01 (10.5) | 6 | 0.04 (9) |
| Cerebral venous sinus thrombosis | 44 | 0.03 (16.5) | 47 | 0.02 (16.5) | 46 | 0.31 (10.5) |
| Convulsions/seizures | 1479 | 0.98 (0) | 1664 | 0.74 (0) | 574 | 3.83 (0) |
| Guillain–Barré syndrome | 13 | 0.01 (8) | 15 | 0.01 (14.5) | 145 | 0.97 (14) |
| Transverse myelitis | 53 | 0.03 (12) | 57 | 0.03 (8) | 20 | 0.13 (13) |
| Acute disseminated encephalomyelitis | 6 | 0.00 (12.5) | 13 | 0.01 (3.5) | 4 | 0.03 (11.5) |
| Narcolepsy/cataplexy | 12 | 0.01 (1) | 14 | 0.01 (1) | 2 | 0.01 (0) |
| Pulmonary embolism | 857 | 0.57 (9) | 843 | 0.37 (10) | 428 | 2.85 (13) |
| Acute respiratory distress syndrome | 42 | 0.03 (12.5) | 45 | 0.02 (43) | 17 | 0.11 (24.5) |
| Acute myocardial infarction | 230 | 0.15 (5) | 287 | 0.13 (8) | 43 | 0.29 (10) |
| Myocarditis/pericarditis | 791 | 0.52 (3) | 1 072 | 0.47 (3) | 93 | 0.62 (8) |
| Appendicitis | 160 | 0.11 (3) | 291 | 0.13 (5.5) | 38 | 0.25 (4) |
| Anemia | 37 | 0.02 (11) | 39 | 0.02 (6) | 7 | 0.05 (16) |
| Lymphadenopathy | 6761 | 4.46 (1) | 7847 | 3.47 (1) | 420 | 2.80 (1) |
| Lymphopenia | 13 | 0.01 (16.5) | 17 | 0.01 (4) | 3 | 0.02 (8) |
| Neutropenia | 18 | 0.01 (3) | 31 | 0.01 (10.5) | 6 | 0.04 (1.5) |
| Other thrombosis | 354 | 0.23 (11) | 358 | 0.16 (9) | 202 | 1.35 (13) |
| Thrombocytopenia | 261 | 0.17 (10.5) | 302 | 0.13 (10.5) | 114 | 0.76 (13) |
| Deep vein thrombosis | 643 | 0.42 (10) | 716 | 0.32 (8) | 448 | 2.99 (12) |
| Anaphylaxis | 79 | 0.05 (0) | 79 | 0.03 (0) | 13 | 0.09 (0) |
| Multisystem inflammatory syndrome in children/adults | 1 | 0.00 (6) | 2 | 0.00 (4) | 1 | 0.01 (0) |
| Death | 2286 | 1.51 (5) | 2005 | 0.89 (5) | 447 | 2.98 (10) |
| Young People (18–64 Years) | Older People (≥65 Years) | Total | ||||
|---|---|---|---|---|---|---|
| Symptom | Number | Incidence † of Events | Number | Incidence † of Events | Number | Incidence † of Events |
| Bell’s palsy ** | 1889 | 0.707 | 616 | 0.622 | 2505 | 0.684 |
| Stroke, hemorrhagic *** | 96 | 0.036 | 84 | 0.085 | 180 | 0.049 |
| Stroke, ischemic *** | 338 | 0.126 | 364 | 0.368 | 702 | 0.192 |
| Encephalitis/myelitis/encephalomyelitis | 49 | 0.018 | 25 | 0.025 | 74 | 0.020 |
| Cerebral venous sinus thrombosis | 106 | 0.040 | 27 | 0.027 | 133 | 0.036 |
| Convulsions/seizures *** | 3287 | 1.229 | 574 | 0.58 | 3861 | 1.054 |
| Guillain–Barré syndrome | 355 | 0.133 | 155 | 0.157 | 510 | 0.139 |
| Transverse myelitis | 90 | 0.034 | 35 | 0.035 | 125 | 0.034 |
| Acute disseminated encephalomyelitis | 17 | 0.006 | 5 | 0.005 | 22 | 0.006 |
| Narcolepsy/cataplexy | 18 | 0.007 | 7 | 0.007 | 25 | 0.007 |
| Pulmonary embolism *** | 1242 | 0.465 | 804 | 0.812 | 2046 | 0.559 |
| Acute respiratory distress syndrome *** | 36 | 0.013 | 56 | 0.057 | 92 | 0.025 |
| Acute myocardial infarction *** | 240 | 0.090 | 254 | 0.257 | 494 | 0.135 |
| Myocarditis/pericarditis *** | 1573 | 0.588 | 193 | 0.195 | 1766 | 0.482 |
| Appendicitis *** | 389 | 0.145 | 64 | 0.065 | 453 | 0.124 |
| Anemia *** | 43 | 0.016 | 34 | 0.034 | 77 | 0.021 |
| Lymphadenopathy *** | 13,337 | 4.988 | 1681 | 1.699 | 15,018 | 4.100 |
| Lymphopenia * | 14 | 0.005 | 13 | 0.013 | 27 | 0.007 |
| Neutropenia ** | 25 | 0.009 | 22 | 0.022 | 47 | 0.013 |
| Other thrombosis *** | 519 | 0.194 | 335 | 0.339 | 854 | 0.233 |
| Thrombocytopenia *** | 347 | 0.130 | 252 | 0.255 | 599 | 0.164 |
| Deep vein thrombosis *** | 1141 | 0.427 | 592 | 0.598 | 1733 | 0.473 |
| Anaphylaxis *** | 1401 | 0.524 | 209 | 0.211 | 1610 | 0.439 |
| Multisystem inflammatory syndrome in children/adults *** | 62 | 0.023 | 48 | 0.049 | 110 | 0.030 |
| Death *** | 1176 | 0.440 | 3413 | 3.449 | 4589 | 1.253 |
| Severe AEs | Correlation with Death (r *) | p Value * | OR (CI) † | p Value † |
|---|---|---|---|---|
| Bell’s palsy | −0.007 | <0.001 | - | 0.859 |
| Hemorrhagic stroke | 0.032 | <0.001 | 9.965 (6.406–15.499) | <0.001 |
| Ischemic stroke | 0.005 | <0.001 | 0.899 (0.541–1.496) | 0.683 |
| Encephalitis/myelitis/encephalomyelitis | 0.002 | 0.122 | 1.565 (0.365–6.717) | 0.547 |
| Cerebral venous sinus thrombosis | 0.001 | 0.514 | 1.537 (0.368–6.423) | 0.556 |
| Convulsions seizures | 0.007 | <0.001 | 2.437 (1.877–3.164) | <0.001 |
| Guillain Barre syndrome | 0.001 | 0.605 | 0.743 (0.328–1.683) | 0.476 |
| Transverse myelitis | −0.002 | 0.273 | - | 0.887 |
| Acute disseminated encephalomyelitis | −0.001 | 0.645 | - | 0.903 |
| Narcolepsy cataplexy | −0.001 | 0.624 | - | 0.887 |
| Pulmonary embolism | 0.023 | <0.001 | 2.363 (1.885–2.961) | <0.001 |
| Acute respiratory distress syndrome | 0.053 | <0.001 | 20.510 (12.620–33.332) | <0.001 |
| Acute myocardial infarction | 0.028 | <0.001 | 3.872 (2.794–5.366) | <0.001 |
| Myocarditis/pericarditis | −0.001 | 0.651 | 1.453 (0.863–2.448) | 0.160 |
| Appendicitis | −0.002 | 0.108 | 0.333 (0.046–2.406) | 0.276 |
| Anemia | 0.006 | <0.001 | 3.797 (1.330–10.839) | 0.013 |
| Lymphadenopathy | −0.017 | <0.001 | 0.149 (0.078–0.287) | <0.001 |
| Neutropenia | 0.006 | <0.001 | 3.622 (1.069–12.273) | 0.039 |
| Other thrombosis | 0.011 | <0.001 | 1.910 (1.297–2.812) | 0.001 |
| Thrombocytopenia | 0.014 | <0.001 | 2.141 (1.427–3.213) | <0.001 |
| Deep vein thrombosis | 0.003 | 0.064 | 0.641 (0.417–0.985) | 0.042 |
| Anaphylaxis | −0.005 | 0.002 | 0.388 (0.124–1.211) | 0.103 |
| Multisystem inflammatory syndrome | 0.006 | <0.001 | 2.053 (0.775–5.439) | 0.148 |
| Number of Outcomes | mRNA-1273(%) | BNT162b2 (%) | JNJ-78436735(%) | Sum |
|---|---|---|---|---|
| 1~5 | 174,347 (73.52%) | 151,908 (73.94%) | 25,407 (65.86%) | 351,662 (73.08%) |
| 6~10 | 51,026 (21.52%) | 41,618 (20.26%) | 9924 (25.72%) | 102,568 (21.32%) |
| 11~15 | 8700 (3.67%) | 8380 (4.08%) | 2293 (5.94%) | 19,373 (4.03%) |
| 16~20 | 1921 (0.81%) | 2124 (1.03%) | 581 (1.51%) | 4626 (0.96%) |
| ≥21 | 1164 (0.49%) | 1406 (0.68%) | 373 (0.97%) | 2943 (0.61%) |
| Sum | 237,158 | 205,436 | 38,578 | 481,172 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sa, S.; Lee, C.W.; Shim, S.R.; Yoo, H.; Choi, J.; Kim, J.H.; Lee, K.; Hong, M.; Han, H.W. The Safety of mRNA-1273, BNT162b2 and JNJ-78436735 COVID-19 Vaccines: Safety Monitoring for Adverse Events Using Real-World Data. Vaccines 2022, 10, 320. https://doi.org/10.3390/vaccines10020320
Sa S, Lee CW, Shim SR, Yoo H, Choi J, Kim JH, Lee K, Hong M, Han HW. The Safety of mRNA-1273, BNT162b2 and JNJ-78436735 COVID-19 Vaccines: Safety Monitoring for Adverse Events Using Real-World Data. Vaccines. 2022; 10(2):320. https://doi.org/10.3390/vaccines10020320
Chicago/Turabian StyleSa, Soonok, Chae Won Lee, Sung Ryul Shim, Hyounggyoon Yoo, Jinwha Choi, Ju Hee Kim, Kiwon Lee, Myunghee Hong, and Hyun Wook Han. 2022. "The Safety of mRNA-1273, BNT162b2 and JNJ-78436735 COVID-19 Vaccines: Safety Monitoring for Adverse Events Using Real-World Data" Vaccines 10, no. 2: 320. https://doi.org/10.3390/vaccines10020320