Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Objectives
- Interventions to promote early and exclusive breastfeeding;
- Interventions to promote continued breastfeeding;
- Interventions to promote appropriate complementary feeding (education or provision of complementary food) during infancy and childhood;
- Effectiveness of community-based interventions to prevent moderate and severe acute malnutrition.
2.1.1. Types of Studies and Participants
2.1.2. Types of Participants
2.1.3. Types of Interventions
- Interventions designed to promote early initiation, exclusive and continued breastfeeding, such as education and support of early and exclusive breastfeeding practices.
- Interventions to promote dietary diversification and appropriate complementary feeding. These will be divided in interventions that provide only education and interventions in which the provision of complementary food for healthy individuals takes place regardless of education.
- Interventions to prevent moderate and severe acute malnutrition, such as educative interventions and supplementary food for children suffering from MAM or SAM.
2.1.4. Types of Outcome Measures
2.2. Literature Search
2.3. Data Collection and Analysis
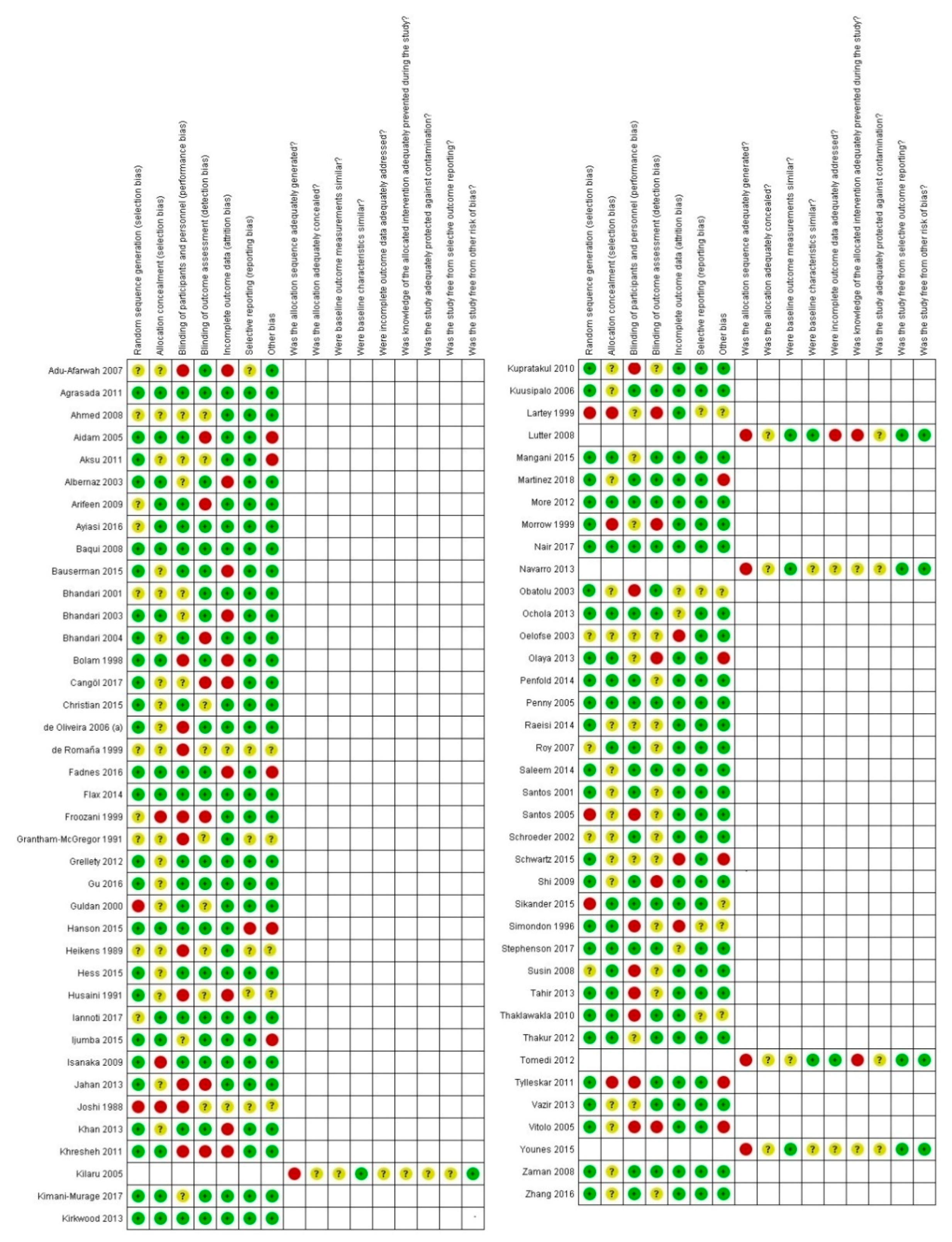
2.3.1. Assessment of Risk of Bias in Included Studies
2.3.2. Assessment of Quality Evidence
2.3.3. Subgroup Analysis, Investigation of Heterogeneity and Sensitivity Analysis
3. Results
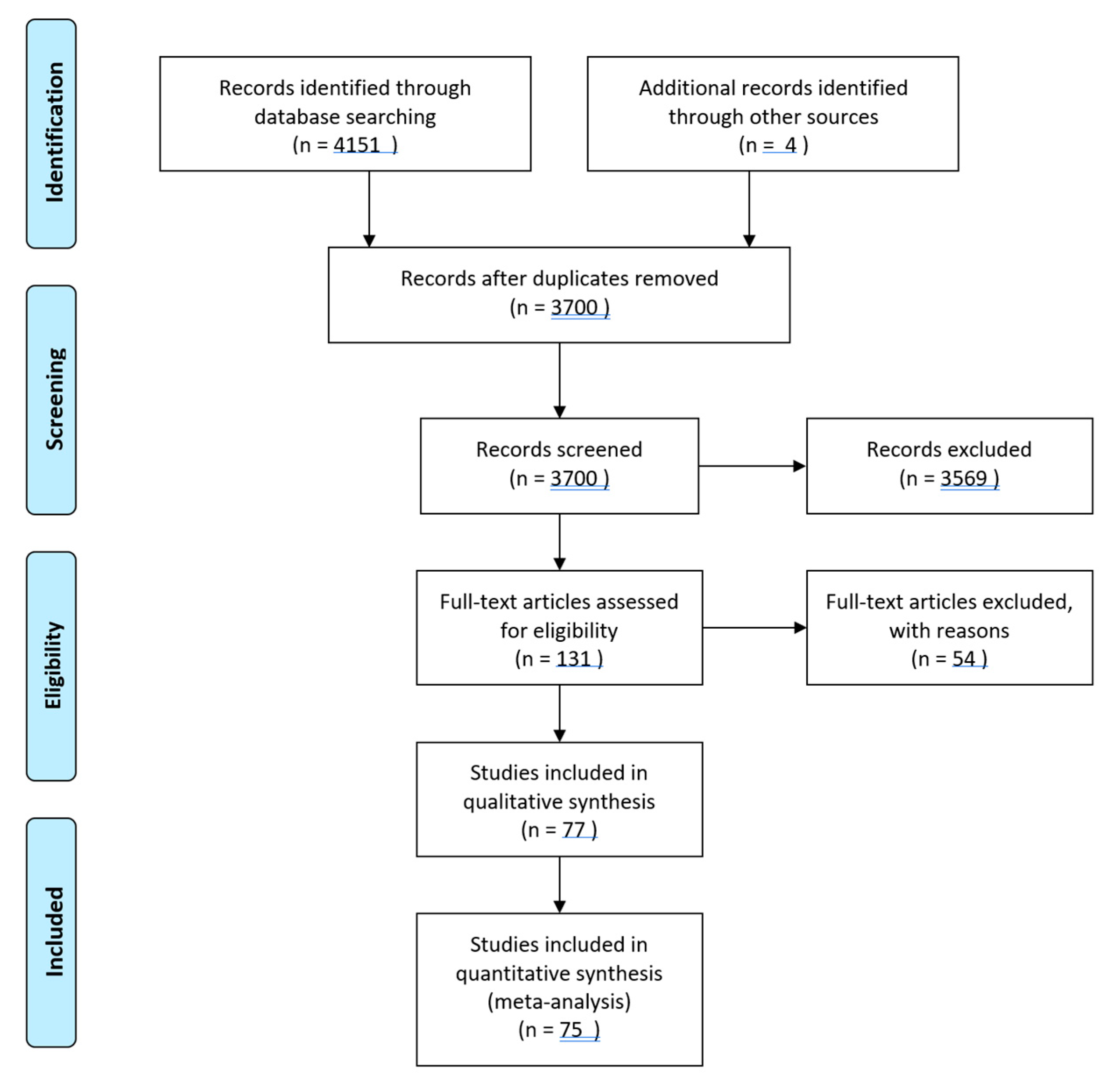
3.1. Study Selection
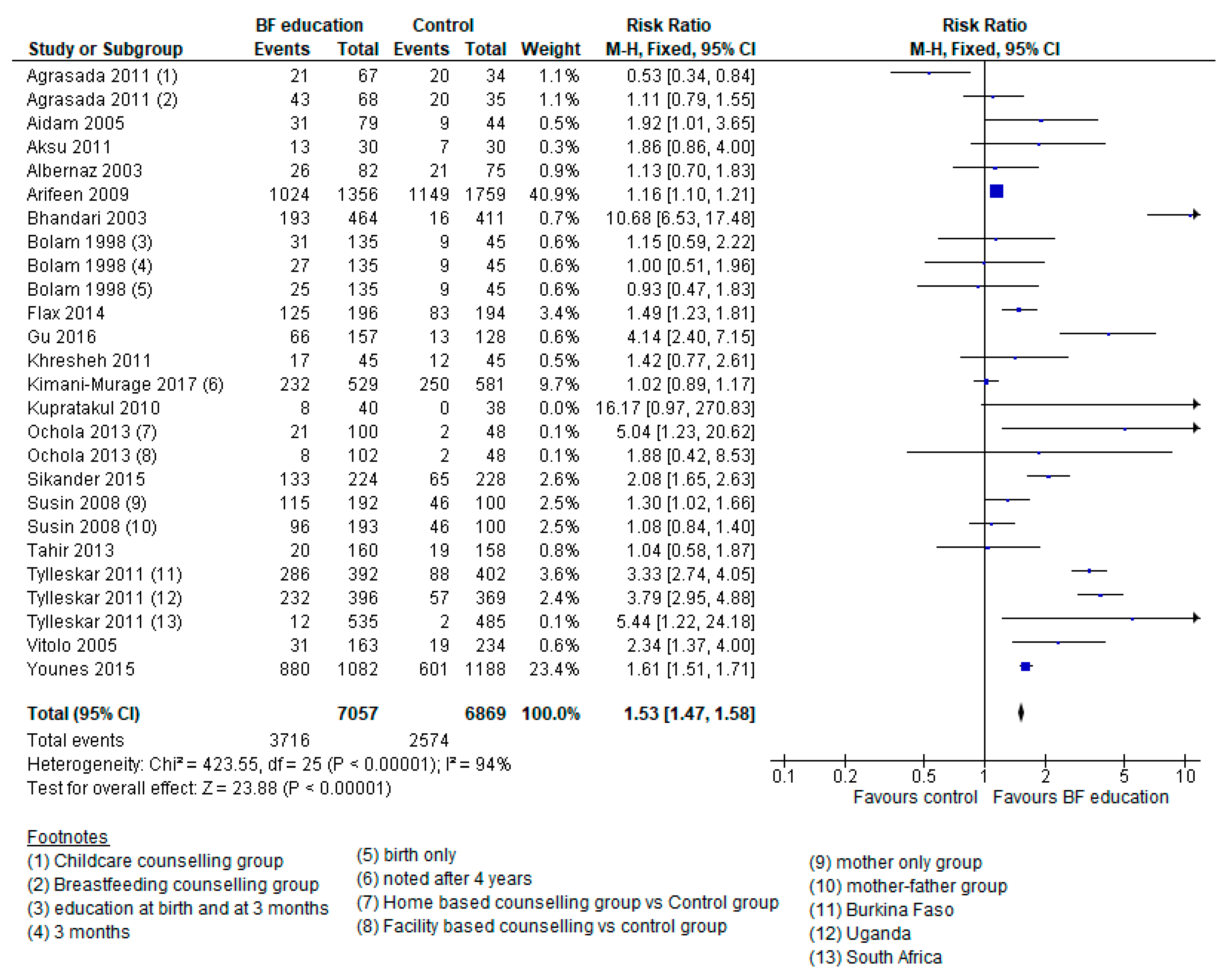
3.2. Comparison 1: Breastfeeding Education Interventions vs. Control
3.3. Comparison 2a: Complementary Feeding Education
3.4. Comparison 2b: Complementary Feeding Provision with or without Education vs. Control
3.5. Comparison 3: Supplementary Feeding Programs vs. Control
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- UNICEF; WHO. Levels and Trends in Child Malnutrition in UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates Key Findings of the 2016 Edition; UNICE: New York, NY, USA, 2017. [Google Scholar]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- UNICEF. Undernutrition Contributes to Nearly Half of All Deaths in Children under 5 and is Widespread in Asia and Africa; UNICEF: New York, NY, USA, 2016. [Google Scholar]
- Olofin, I.; McDonald, C.M.; Ezzati, M.; Flaxman, S.; Black, R.E.; Fawzi, W.W.; Caulfield, L.E.; Danaei, G. Study NIM Associations of suboptimal growth with all-cause and cause-specific mortality in children under five years: A pooled analysis of ten prospective studies. PLoS ONE 2013, 8, e64636. [Google Scholar] [CrossRef] [Green Version]
- Menon, P.; Stoltzfus, R.J. Building Convergence in Science, Programs, and Policy Actions on Child Undernutrition: Symposium Rationale and Overview12. Adv. Nutr. 2012, 3, 224–226. [Google Scholar] [CrossRef] [Green Version]
- James, P.; Sadler, K.; Wondafrash, M.; Argaw, A.; Luo, H.; Geleta, B.; Kedir, K.; Getnet, Y.; Belachew, T.; Bahwere, P. Children with Moderate Acute Malnutrition with No Access to Supplementary Feeding Programmes Experience High Rates of Deterioration and No Improvement: Results from a Prospective Cohort Study in Rural Ethiopia. PLoS ONE 2016, 11, e0153530. [Google Scholar] [CrossRef]
- UNICEF WW. Levels and Trends in Child Malnutrition: UNICEF- WHO-World Bank joint Child Malnutrition Estimates; UNICEF: New York, NY, USA, 2012. [Google Scholar]
- Michels, K.; Ghassabian, A.; Mumford, S.L.; Sundaram, R.; Bell, E.M.; Bello, S.C.; Yeung, E. Breastfeeding and motor development in term and preterm infants in a longitudinal US cohort. Am. J. Clin. Nutr. 2017, 106, 1456–1462. [Google Scholar]
- Kramer, M.S.; Kakuma, R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst. Rev. 2012, CD003517. [Google Scholar]
- Zivkovic, A.M.; German, J.B.; Lebrilla, C.B.; Mills, D.A. Human milk glycobiome and its impact on the infant gastrointestinal microbiota. Proc. Natl. Acad. Sci. USA 2010, 108, 4653–4658. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, R.; Sinha, B.; Sankar, M.J.; Taneja, S.; Bhandari, N.; Rollins, N.; Bahl, R.; Martines, J. Breastfeeding and maternal health outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 96–113. [Google Scholar]
- Jordan, S.; Siskind, V.; Green, A.; Whiteman, D.C.; Webb, P. Breastfeeding and risk of epithelial ovarian cancer. Cancer Causes Control. 2009, 21, 109–116. [Google Scholar]
- Dewey, K. Guiding Principles for Complementary Feeding of the Breastfed Child; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- White, J.M.; Bégin, F.; Kumapley, R.; Murray, C.; Krasevec, J.; Aguayo, V.M. Complementary feeding practices: Current global and regional estimates. Matern. Child Nutr. 2017, 13, e12505. [Google Scholar]
- Campbell, R.K.; Hurley, K.M.; Shamim, A.A.; Shaikh, S.; Chowdhury, Z.T.; Mehra, S.; De Pee, S.; Ahmed, T.; West, K.P.; Christian, P. Effect of complementary food supplementation on breastfeeding and home diet in rural Bangladeshi children. Am. J. Clin. Nutr. 2016, 104, 1450–1458. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Irfan, O.; Hadi, R.; Das, J.K.; Bhutta, Z.A. PROTOCOL: Effects of interventions for infant and young child feeding (IYCF) promotion on optimal IYCF practices, nutrition, growth and health in low- and middle-income countries: A systematic review. Campbell Syst. Rev. 2018, 14, 1–26. [Google Scholar] [CrossRef]
- Higgins, J.; Altman, U.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; Debeer, H. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiology 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Adu-Afarwuah, S.; Lartey, A.; Brown, K.H.; Zlotkin, S.; Briend, A.; Dewey, K.G. Randomized comparison of 3 types of micronutrient supplements for home fortification of complementary foods in Ghana: Effects on growth and motor development. Am. J. Clin. Nutr. 2007, 86, 412–420. [Google Scholar] [CrossRef] [Green Version]
- Agrasada, G.V.; Ewald, U.; Kylberg, E.; Gustafsson, J. Exclusive breastfeeding of low birth weight infants for the first six months: Infant morbidity and maternal and infant anthropometry. Asia Pac. J. Clin. Nutr. 2011, 20. [Google Scholar]
- Ahmed, A.H. Breastfeeding preterm infants: An educational program to support mothers of preterm infants in Cairo, Egypt. Pediatr. Nurs. 2008, 34, 125–130. [Google Scholar]
- Aidam, B.A.; Pérez-Escamilla, R.; Lartey, A. Lactation Counseling Increases Exclusive Breast-Feeding Rates in Ghana. J. Nutr. 2005, 135, 1691–1695. [Google Scholar] [CrossRef] [Green Version]
- Aksu, H.; Kucuk, M.; Düzgün, G. The effect of postnatal breastfeeding education/support offered at home 3 days after delivery on breastfeeding duration and knowledge: A randomized trial. J. Matern. Neonatal Med. 2010, 24, 354–361. [Google Scholar] [CrossRef]
- Albernaz, E.; Victora, C.G.; Haisma, H.; Wright, A.; Coward, W.A. Lactation Counseling Increases Breast-Feeding Duration but Not Breast Milk Intake as Measured by Isotopic Methods. J. Nutr. 2003, 133, 205–210. [Google Scholar] [CrossRef]
- Arifeen, S.; Hoque, D.M.E.; Akter, T.; Rahman, M.; Hoque, M.E.; Begum, K.; Chowdhury, E.; Khan, R.; Blum, L.S.; Ahmed, S.; et al. Effect of the Integrated Management of Childhood Illness strategy on childhood mortality and nutrition in a rural area in Bangladesh: A cluster randomised trial. Lancet 2009, 374, 393–403. [Google Scholar] [CrossRef]
- Baqui, A.H.; Arifeen, S.; Darmstadt, G.L.; Ahmed, S.; Williams, E.K.; Seraji, H.R.; Mannan, I.; Rahman, S.M.; Shah, R.; Saha, S.K.; et al. Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: A cluster-randomised controlled trial. Lancet 2008, 371, 1936–1944. [Google Scholar] [CrossRef]
- Bauserman, M.; Lokangaka, A.; Gado, J.; Close, K.; Wallace, D.; Kodondi, K.-K.; Tshefu, A.; Bose, C. A cluster-randomized trial determining the efficacy of caterpillar cereal as a locally available and sustainable complementary food to prevent stunting and anaemia. Public Health Nutr. 2015, 18, 1785–1792. [Google Scholar] [CrossRef] [Green Version]
- Bhandari, N.; Bahl, R.; Mazumdar, S.; Martines, J.; Black, R.E.; Bhan, M.K. Effect of community-based promotion of exclusive breastfeeding on diarrhoeal illness and growth: A cluster randomised controlled trial. Lancet 2003, 361, 1418–1423. [Google Scholar] [CrossRef]
- Bhandari, N.; Bahl, R.; Nayyar, B.; Khokhar, P.; Rohde, J.E.; Bhan, M.K. Food supplementation with encouragement to feed it to infants from 4 to 12 months of age has a small impact on weight gain. J. Nutr. 2001, 131, 1946–1951. [Google Scholar] [CrossRef] [Green Version]
- Infant Feeding Study Group; Bhandari, N.; Martines, J.; Black, R.E.; Bhan, M.K.; Mazumder, S.; Bahl, R. An Educational Intervention to Promote Appropriate Complementary Feeding Practices and Physical Growth in Infants and Young Children in Rural Haryana, India. J. Nutr. 2004, 134, 2342–2348. [Google Scholar] [CrossRef]
- Bolam, A.; Manandhar, D.S.; Shrestha, P.; Ellis, M.; Costello, A.M.D.L. The effects of postnatal health education for mothers on infant care and family planning practices in Nepal: A randomised controlled trial. BMJ 1998, 316, 805–811. [Google Scholar] [CrossRef] [Green Version]
- Cangöl, E.; Şahin, N.H. The Effect of a Breastfeeding Motivation Program Maintained During Pregnancy on Supporting Breastfeeding: A Randomized Controlled Trial. Breastfeed. Med. 2017, 12, 218–226. [Google Scholar] [CrossRef]
- Christian, P.; Shaikh, S.; Shamim, A.A.; Mehra, S.; Wu, L.; Mitra, M.; Ali, H.; Merrill, R.D.; Choudhury, N.; Parveen, M.; et al. Effect of fortified complementary food supplementation on child growth in rural Bangladesh: A cluster-randomized trial. Int. J. Epidemiology 2015, 44, 1862–1876. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, L.D.; Giugliani, E.; Santo, L.C.D.E.; França, M.C.T.; Weigert, E.M.L.; Kohler, C.V.F.; Bonilha, A.L.D.L. Effect of Intervention to Improve Breastfeeding Technique on the Frequency of Exclusive Breastfeeding and Lactation-Related Problems. J. Hum. Lact. 2006, 22, 315–321. [Google Scholar] [CrossRef]
- De Romaña, G.L.J.F.; Bulletin, N. Experience with complementary feeding in the FONCODES project. Food Nutr. Bull. 2000, 21, 43–48. [Google Scholar] [CrossRef]
- Fadnes, L.T.; Nankabirwa, V.; Engebretsen, I.M.; Sommerfelt, H.; Birungi, N.; Lombard, C.; Swanevelder, S.; Van den Broeck, J.; Tylleskär, T.; Tumwine, J.K. Effects of an exclusive breastfeeding intervention for six months on growth patterns of 4–5 year old children in Uganda: The cluster-randomised PROMISE EBF trial. BMC Public Health 2016, 16, 555. [Google Scholar] [CrossRef] [Green Version]
- Flax, V.L.; Negerie, M.; Ibrahim, A.U.; Leatherman, S.; Daza, E.J.; Bentley, M.E. Integrating Group Counseling, Cell Phone Messaging, and Participant-Generated Songs and Dramas into a Microcredit Program Increases Nigerian Women’s Adherence to International Breastfeeding Recommendations–3. J. Nutr. 2014, 144, 1120–1124. [Google Scholar] [CrossRef]
- Froozani, M.D.; Permehzadeh, K.; Motlagh, A.R.; Golestan, B. Effect of breastfeeding education on the feeding pattern and health of infants in their first 4 months in the Islamic Republic of Iran. Bull. World Heal. Organ. 1999, 77, 381–385. [Google Scholar]
- Gardner, J.M.; Grantham-McGregor, S.M.; Himes, J.; Chang, S. Behaviour and development of stunted and nonstunted Jamaican children. J. Child Psychol. Psychiatry Allied Discip. 1999, 40, 819–827. [Google Scholar] [CrossRef]
- Grellety, E.; Shepherd, S.; Roederer, T.; Manzo, M.L.; Doyon, S.; Ategbo, E.A.; Grais, R.F. Effect of mass supplementation with ready-to-use supplementary food during an anticipated nutritional emergency. PLoS ONE 2012, 7, e44549. [Google Scholar] [CrossRef] [Green Version]
- Gu, Y.; Zhu, Y.; Zhang, Z.; Wan, H. Effectiveness of a theory-based breastfeeding promotion intervention on exclusive breastfeeding in China: A randomised controlled trial. Midwifery 2016, 42, 93–99. [Google Scholar] [CrossRef]
- Guldan, G.S.; Fan, H.-C.; Ma, X.; Ni, Z.-Z.; Xiang, X.; Tang, M.-Z. Culturally appropriate nutrition education improves infant feeding and growth in rural Sichuan, China. J. Nutr. 2000, 130, 1204–1211. [Google Scholar] [CrossRef] [Green Version]
- Hanson, C.; Manzi, F.; Mkumbo, E.; Shirima, K.; Penfold, S.; Hill, Z.; Shamba, D.; Jaribu, J.; Hamisi, Y.; Soremekun, S.; et al. Effectiveness of a Home-Based Counselling Strategy on Neonatal Care and Survival: A Cluster-Randomised Trial in Six Districts of Rural Southern Tanzania. PLoS Med. 2015, 12, e1001881. [Google Scholar] [CrossRef] [Green Version]
- Heikens, G.T.; Schofield, W.N.; Dawson, S.; Grantham-McGregor, S. The Kingston project. I. Growth of malnourished children during rehabilitation in the community, given a high energy supplement. Eur. J. Clin. Nutr. 1989, 43, 145–160. [Google Scholar]
- Hess, S.Y.; Bado, L.; Aaron, G.J.; Ouédraogo, J.B.; Zeilani, M.; Brown, K.H. Acceptability of zinc-fortified, lipid-based nutrient supplements (LNS) prepared for young children in Burkina Faso. Maternal Child Nutr. 2011, 7, 357–367. [Google Scholar] [CrossRef]
- Husaini, M.A.; Karyadi, L.; Husaini, Y.K.; Sandjaja; Karyadi, D.; Pollitt, E. Developmental effects of short-term supplementary feeding in nutritionally-at-risk Indonesian infants. Am. J. Clin. Nutr. 1991, 54, 799–804. [Google Scholar] [CrossRef]
- Iannotti, L.L.; Lutter, C.K.; Stewart, C.P.; Riofrío, C.A.G.; Malo, C.; Reinhart, G.; Palacios, A.; Karp, C.; Chapnick, M.; Cox, K.; et al. Eggs in Early Complementary Feeding and Child Growth: A Randomized Controlled Trial. Pediatrics 2017, 140, e20163495. [Google Scholar] [CrossRef] [Green Version]
- Ijumba, P.; Doherty, T.; Jackson, D.; Tomlinson, M.; Sanders, D.; Swanevelder, S.; Persson, L.-Å. Effect of an integrated community-based package for maternal and newborn care on feeding patterns during the first 12 weeks of life: A cluster-randomized trial in a South African township. Public Heal. Nutr. 2015, 18, 2660–2668. [Google Scholar] [CrossRef] [Green Version]
- Isanaka, S.; Nombela, N.; Djibo, A.; Poupard, M.; Van Beckhoven, D.; Gaboulaud, V.; Guerin, P.; Grais, R.F. Effect of Preventive Supplementation with Ready-to-Use Therapeutic Food on the Nutritional Status, Mortality, and Morbidity of Children Aged 6 to 60 Months in Niger. JAMA 2009, 301, 277–285. [Google Scholar] [CrossRef]
- Jahan, K.; Roy, S.; Israt, S.; Ferdouse, K.; Salam, S. Impact of nutrition education on pregnancy weight gain and birth outcome. Ann. Nutr. Metab. 2013, 63, 756. [Google Scholar]
- Joshi, S.; Rao, S. Assessing supplementary feeding programmes in selected Balwadies. Eur. J. Clin. Nutr. 1988, 42, 779–785. [Google Scholar]
- Khan, A.I.; Hawkesworth, S.; Ekström, E.C.; Arifeen, S.; Moore, S.E.; Frongillo, E.A.; Yunus, M.; Persson, L.Å.; Kabir, I. Effects of exclusive breastfeeding intervention on child growth and body composition: The MINIMat trial, Bangladesh. Acta Paediatr. 2013, 102, 815–823. [Google Scholar] [CrossRef]
- Khresheh, R.M.; Suhaimat, A.; Jalamdeh, F.; Barclay, L. The effect of a postnatal education and support program on breastfeeding among primiparous women: A randomized controlled trial. Int. J. Nurs. Stud. 2011, 48, 1058–1065. [Google Scholar] [CrossRef]
- Kilaru, A.; Griffiths, P.L.; Ganapathy, S.; Shanti, G. Community-based nutrition education forimproving infant growth in rural Karnataka. Indian Pediatr. 2005, 42, 425. [Google Scholar]
- Kimani, E.; Griffiths, P.; Wekesah, F.M.; Wanjohi, M.; Muhia, N.; Muriuki, P.; Egondi, T.; Kyobutungi, C.; Ezeh, A.; McGarvey, S.T.; et al. Effectiveness of home-based nutritional counselling and support on exclusive breastfeeding in urban poor settings in Nairobi: A cluster randomized controlled trial. Glob. Health 2017, 13, 90. [Google Scholar] [CrossRef] [Green Version]
- Kirkwood, B.; Manu, A.A.; Asbroek, A.H.T.; Soremekun, S.; Weobong, B.; Gyan, T.; Danso, S.; Amenga-Etego, S.; Tawiah, C.; Owusu-Agyei, S.; et al. Effect of the Newhints home-visits intervention on neonatal mortality rate and care practices in Ghana: A cluster randomised controlled trial. Lancet 2013, 381, 2184–2192. [Google Scholar] [CrossRef]
- Kupratakul, J.; Taneepanichskul, S.; Voramongkol, N.; Phupong, V. A randomized controlled trial of knowledge sharing practice with empowerment strategies in pregnant women to improve exclusive breastfeeding during the first six months postpartum. J. Med Assoc. Thail. = Chotmaihet Thangphaet 2010, 93, 1009–1018. [Google Scholar]
- Kuusipalo, H.; Maleta, K.; Briend, A.; Manary, M.; Ashorn, P.; Maleta, K. Growth and Change in Blood Haemoglobin Concentration Among Underweight Malawian Infants Receiving Fortified Spreads for 12 Weeks. J. Pediatr. Gastroenterol. Nutr. 2006, 43, 525–532. [Google Scholar] [CrossRef]
- Lartey, A.; Manu, A.; Brown, K.H.; Peerson, J.M.; Dewey, K.G. A randomized, community-based trial of the effects of improved, centrally processed complementary foods on growth and micronutrient status of Ghanaian infants from 6 to 12 mo of age. Am. J. Clin. Nutr. 1999, 70, 391–404. [Google Scholar] [CrossRef] [Green Version]
- Lutter, C.K.; Rodríguez, A.; Fuenmayor, G.; Avila, L.; Sempertegui, F.; Escobar, J. Growth and Micronutrient Status in Children Receiving a Fortified Complementary Food. J. Nutr. 2008, 138, 379–388. [Google Scholar] [CrossRef]
- Mangani, C.; Maleta, K.; Phuka, J.; Cheung, Y.B.; Thakwalakwa, C.; Dewey, K.; Manary, M.; Puumalainen, T.; Ashorn, P.; Maleta, K. Effect of complementary feeding with lipid-based nutrient supplements and corn-soy blend on the incidence of stunting and linear growth among 6- to 18-month-old infants and children in rural Malawi. Matern. Child Nutr. 2015, 11, 132–143. [Google Scholar] [CrossRef] [Green Version]
- Ayiasi, R.M.; Kolsteren, P.; Batwala, V.; Criel, B.; Orach, C.G. Effect of Village Health Team Home Visits and Mobile Phone Consultations on Maternal and Newborn Care Practices in Masindi and Kiryandongo, Uganda: A Community-Intervention Trial. PLoS ONE 2016, 11, e0153051. [Google Scholar]
- Martinez, B.; Webb, M.F.; Gonzalez, A.; Douglas, K.; Grazioso, M.D.P.; Rohloff, P. Complementary feeding intervention on stunted Guatemalan children: A randomised controlled trial. BMJ Paediatr. Open 2018, 2, e000213. [Google Scholar] [CrossRef]
- More, N.S.; Bapat, U.; Das, S.; Alcock, G.; Patil, S.; Porel, M.; Vaidya, L.; Fernandez, A.; Joshi, W.; Osrin, D. Community Mobilization in Mumbai Slums to Improve Perinatal Care and Outcomes: A Cluster Randomized Controlled Trial. PLoS Med. 2012, 9, e1001257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrow, A.L.; Guerrero, M.L.; Shults, J.; Calva, J.; Lutter, C.; Bravo, J.; Ruiz-Palacios, G.; Morrow, R.C.; Butterfoss, F.D. Efficacy of home-based peer counselling to promote exclusive breastfeeding: A randomised controlled trial. Lancet 1999, 353, 1226–1231. [Google Scholar] [CrossRef]
- Nair, N.; Tripathy, P.; Sachdev, H.S.; Pradhan, H.; Bhattacharyya, S.; Gope, R.; Gagrai, S.; Rath, S.; Rath, S.; Sinha, R.; et al. Effect of participatory women’s groups and counselling through home visits on children’s linear growth in rural eastern India (CARING trial): A cluster-randomised controlled trial. Lancet Global Health 2017, 5, e1004–e1016. [Google Scholar] [CrossRef] [Green Version]
- Navarro, J.I.; Sigulem, D.M.; Ferraro, A.; Polanco, J.J.; De Barros, A.J.D. The double task of preventing malnutrition and overweight: A quasi-experimental community-based trial. BMC Public Heal. 2013, 13, 212. [Google Scholar] [CrossRef]
- Obatolu, V.A. Growth pattern of infants fed with a mixture of extruded malted maize and cowpea. Nutrients 2003, 19, 174–178. [Google Scholar] [CrossRef]
- Ochola, S.; Labadarios, D.; Nduati, R.W. Impact of counselling on exclusive breast-feeding practices in a poor urban setting in Kenya: A randomized controlled trial. Public Health Nutr. 2012, 16, 1732–1740. [Google Scholar] [CrossRef] [Green Version]
- Oelofse, A.; Van Raaij, J.; Benadé, A.; Dhansay, M.; Tolboom, J.; Hautvast, J. The effect of a micronutrient-fortified complementary food on micronutrient status, growth and development of 6- to 12-month-old disadvantaged urban South African infants. Int. J. Food Sci. Nutr. 2003, 54, 399–407. [Google Scholar] [CrossRef]
- Olaya, G.A.; Lawson, M.; Fewtrell, M.S. Efficacy and safety of new complementary feeding guidelines with an emphasis on red meat consumption: A randomized trial in Bogota, Colombia. Am. J. Clin. Nutr. 2013, 98, 983–993. [Google Scholar] [CrossRef] [Green Version]
- Penfold, S.; Manzi, F.; Mkumbo, E.; Temu, S.; Jaribu, J.; Shamba, D.; Mshinda, H.; Cousens, S.; Marchant, T.; Tanner, M.; et al. Effect of home-based counselling on newborn care practices in southern Tanzania one year after implementation: A cluster-randomised controlled trial. BMC Pediatr. 2014, 14, 187. [Google Scholar] [CrossRef] [Green Version]
- Penny, M.; Creed-Kanashiro, H.; Robert, R.C.; Narro, M.R.; Caulfield, L.E.; Black, R.E. Effectiveness of an educational intervention delivered through the health services to improve nutrition in young children: A cluster-randomised controlled trial. Lancet 2005, 365, 1863–1872. [Google Scholar] [CrossRef]
- Raeisi, K.; Shariat, M.; Nayeri, F.; Raji, F.; Dalili, H. A single center study of the effects of trained fathers’ participation in constant breastfeeding. Acta medica Iran. 2014, 52, 694–696. [Google Scholar]
- Roy, S.; Jolly, S.P.; Shafique, S.; Fuchs, G.J.; Mahmud, Z.; Chakraborty, B.; Roy, S. Prevention of Malnutrition among Young Children in Rural Bangladesh by a Food-Health-Care Educational Intervention: A Randomized, Controlled Trial. Food Nutr. Bull. 2007, 28, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Saleem, A.F.; Mahmud, S.; Baig-Ansari, N.; Zaidi, A.K. Impact of Maternal Education about Complementary Feeding on Their Infants’ Nutritional Outcomes in Low- and Middle-income Households: A Community-based Randomized Interventional Study in Karachi, Pakistan. J. Heal. Popul. Nutr. 2014, 32, 623–633. [Google Scholar]
- Santos, I.S.; Gigante, D.P.; Coitinho, D.C.; Haisma, H.; Valle, N.C.J.; Valente, G. Evaluation of the impact of a nutritional program for undernourished children in Brazil. Cadernos de Saúde Pública 2005, 21, 776–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, I.S.; Victora, C.G.; Martines, J.; Gonçalves, H.; Gigante, D.P.; Valle, N.J.; Pelto, G. Nutrition counseling increases weight gain among Brazilian children. J. Nutr. 2001, 131, 2866–2873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroeder, D.G.; Pachón, H.; Dearden, K.A.; Ha, T.T.; Lang, T.T.; Marsh, D.R. An integrated child nutrition intervention improved growth of younger, more malnourished children in northern Vietnam. Food Nutr. Bull. 2002, 23, 50–58. [Google Scholar] [CrossRef]
- Schwartz, R.; Vigo, Á.; De Oliveira, L.D.; Giugliani, E.R.J. The Effect of a Pro-Breastfeeding and Healthy Complementary Feeding Intervention Targeting Adolescent Mothers and Grandmothers on Growth and Prevalence of Overweight of Preschool Children. PLoS ONE 2015, 10, e0131884. [Google Scholar] [CrossRef]
- Shi, L.; Zhang, J.; Wang, Y.; Caulfield, L.E.; Guyer, B. Effectiveness of an educational intervention on complementary feeding practices and growth in rural China: A cluster randomised controlled trial. Public Heal. Nutr. 2009, 13, 556–565. [Google Scholar] [CrossRef] [Green Version]
- Sikander, S.; Maselko, J.; Zafar, S.; Haq, Z.; Ahmad, I.; Ahmad, M.; Hafeez, A.; Rahman, A. Cognitive-Behavioral Counseling for Exclusive Breastfeeding in Rural Pediatrics: A Cluster RCT. Pediatrics 2015, 135, e424–e431. [Google Scholar] [CrossRef] [Green Version]
- Simondon, K.B.; Gartner, A.; Berger, J.; Cornu, A.; Massamba, J.P.; Miguel, J.L.S.; Ly, C.; Missotte, I.; Simondon, F.; Traissac, P.; et al. Effect of early, short-term supplementation on weight and linear growth of 4–7-mo-old infants in developing countries: A four-country randomized trial. Am. J. Clin. Nutr. 1996, 64, 537–545. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, K.B.; Agapova, S.E.; Divala, O.; Kaimila, Y.; Maleta, K.M.; Thakwalakwa, C.; Ordiz, M.I.; Trehan, I.; Manary, M. Complementary feeding with cowpea reduces growth faltering in rural Malawian infants: A blind, randomized controlled clinical trial. Am. J. Clin. Nutr. 2017, 106, 1500–1507. [Google Scholar] [CrossRef] [Green Version]
- Susin, L.R.O.; Giugliani, E.R.J. Inclusion of Fathers in an Intervention to Promote Breastfeeding: Impact on Breastfeeding Rates. J. Hum. Lact. 2008, 24, 386–392. [Google Scholar] [CrossRef]
- Tahir, N.M.; Al-Sadat, N. Does telephone lactation counselling improve breastfeeding practices?: A randomised controlled trial. Int. J. Nurs. Stud. 2013, 50, 16–25. [Google Scholar] [CrossRef]
- Thakur, S.K.; Roy, S.K.; Paul, K.; Khanam, M.; Khatun, W.; Sarker, D. Effect of nutrition education on exclusive breastfeeding for nutritional outcome of low birth weight babies. Eur. J. Clin. Nutr. 2011, 66, 376–381. [Google Scholar] [CrossRef]
- Thakwalakwa, C.; Ashorn, P.; Phuka, J.; Cheung, Y.B.; Briend, A.; Puumalainen, T.; Maleta, K. A Lipid-Based Nutrient Supplement but Not Corn-Soy Blend Modestly Increases Weight Gain among 6- to 18-Month-Old Moderately Underweight Children in Rural Malawi. J. Nutr. 2010, 140, 2008–2013. [Google Scholar] [CrossRef]
- Tomedi, A.; Rohan-Minjares, F.; McCalmont, K.; Ashton, R.; Opiyo, R.; Mwanthi, M. Feasibility and effectiveness of supplementation with locally available foods in prevention of child malnutrition in Kenya. Public Heal. Nutr. 2011, 15, 749–756. [Google Scholar] [CrossRef] [Green Version]
- Tylleskar, T.; Jackson, D.; Meda, N.; Engebretsen, I.M.S.; Chopra, M.; Diallo, A.H.; Doherty, T.; Ekström, E.-C.; Fadnes, L.T.; Goga, A.; et al. Exclusive breastfeeding promotion by peer counsellors in sub-Saharan Africa (PROMISE-EBF): A cluster-randomised trial. Lancet 2011, 378, 420–427. [Google Scholar] [CrossRef] [Green Version]
- Vazir, S.; Engle, P.; Balakrishna, N.; Griffiths, P.L.; Johnson, S.L.; Creed-Kanashiro, H.; Rao, S.F.; Shroff, M.R.; Bentley, M.E. Cluster-randomized trial on complementary and responsive feeding education to caregivers found improved dietary intake, growth and development among rural Indian toddlers. Matern. Child Nutr. 2012, 9, 99–117. [Google Scholar] [CrossRef] [Green Version]
- Vitolo, M.R.; Bortolini, G.A.; Feldens, C.; Drachler, M.D.L. Impacts of the 10 Steps to Healthy Feeding in Infants: A randomized field trial. Cadernos de Saúde Pública 2005, 21, 1448–1457. [Google Scholar] [CrossRef] [Green Version]
- Younes, L.; Houweling, T.A.; Azad, K.; Kuddus, A.; Shaha, S.; Haq, B.; Nahar, T.; Hossen, M.; Beard, J.; Copas, A.; et al. The effect of participatory women’s groups on infant feeding and child health knowledge, behaviour and outcomes in rural Bangladesh: A controlled before-and-after study. J. Epidemiol. Community Health 2015, 69, 374–381. [Google Scholar] [CrossRef] [Green Version]
- Zaman, S.; Ashraf, R.N.; Martines, J. Training in Complementary Feeding Counselling of Healthcare Workers and Its Influence on Maternal Behaviours and Child Growth: A Cluster-randomized Controlled Trial in Lahore, Pakistan. J. Heal. Popul. Nutr. 2008, 26, 210–222. [Google Scholar]
- Zhang, Y.; Wu, Q.; Wang, W.; van Velthoven, M.H.; Chang, S.; Han, H.; Xing, M.; Chen, L.; Scherpbier, R.W. Effectiveness of complementary food supplements and dietary counselling on anaemia and stunting in children aged 6–23 months in poor areas of Qinghai Province, China: A controlled interventional study. BMJ Open 2016, 6, e011234. [Google Scholar] [CrossRef]
- Kim, S.K.; Park, S.; Oh, J.; Kim, J.; Ahn, S. Interventions promoting exclusive breastfeeding up to six months after birth: A systematic review and meta-analysis of randomized controlled trials. Int. J. Nurs. Stud. 2018, 80, 94–105. [Google Scholar] [CrossRef]
- Rollins, N.C.; Bhandari, N.; Hajeebhoy, N.; Horton, S.; Lutter, C.K.; Martines, J.C.; Piwoz, E.G.; Richter, L.M.; Victora, C.G. Why invest, and what it will take to improve breastfeeding practices? Lancet 2016, 387, 491–504. [Google Scholar] [CrossRef]
- Balogun, O.O.; O’Sullivan, E.J.; McFadden, A.; Ota, E.; Gavine, A.; Garner, C.D.; Renfrew, M.J.; MacGillivray, S. Interventions for promoting the initiation of breastfeeding. Cochrane Database Syst. Rev. 2016, 2016, CD001688. [Google Scholar] [CrossRef] [Green Version]
- Sinha, B.; Chowdhury, R.; Upadhyay, R.P.; Taneja, S.; Martines, J.; Bahl, R.; Sankar, M.J. Integrated Interventions Delivered in Health Systems, Home, and Community Have the Highest Impact on Breastfeeding Outcomes in Low- and Middle-Income Countries. J. Nutr. 2017, 147, 2179S–2187S. [Google Scholar] [CrossRef]
- Sinha, B.; Chowdhury, R.; Sankar, M.J.; Martines, J.; Taneja, S.; Mazumder, S.; Rollins, N.; Bahl, R.; Bhandari, N. Interventions to improve breastfeeding outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 114–134. [Google Scholar] [CrossRef] [Green Version]
- Arikpo, D.; Edet, E.S.; Chibuzor, M.T.; Odey, F.; Caldwell, D.M. Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database Syst. Rev. 2018, 5, Cd011768. [Google Scholar] [CrossRef] [Green Version]
- Lassi, Z.S.; Das, J.K.; Zahid, G.-E.-S.; Imdad, A.; Bhutta, Z.A. Impact of education and provision of complementary feeding on growth and morbidity in children less than 2 years of age in developing countries: A systematic review. BMC Public Health 2013, 13, S13. [Google Scholar] [CrossRef] [Green Version]
- Kristjansson, E.; Francis, D.K.; Liberato, S.; Jandu, M.B.; Welch, V.; Batal, M.; Greenhalgh, T.; Rader, T.; Noonan, E.; Shea, B.; et al. Food supplementation for improving the physical and psychosocial health of socio-economically disadvantaged children aged three months to five years. Cochrane Database Syst. Rev. 2015, 11, Cd009924. [Google Scholar] [CrossRef]
- Beaton, G.H.; Ghassemi, H. Supplementary feeding programs for young children in developing countries. Am. J. Clin. Nutr. 1982, 35, 864–916. [Google Scholar] [CrossRef]
- Pollitt, E.; Gorman, K.S.; Engle, P.L.; Martorell, R.; Rivera, J.; Wachs, T.D.; Scrimshaw, N.S. Early Supplementary Feeding and Cognition: Effects over Two Decades. Monogr. Soc. Res. Child Dev. 1993, 58, i-118. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Outcomes | MD | RR | 95% CI | n | No. of Studies | GRADE | p-Value |
|---|---|---|---|---|---|---|---|
| Breastfeeding Education Interventions | |||||||
| Early initiation of breastfeeding | 1.20 | 1.12 to 1.28 | 84092 | 14 | LOW | <0.001 | |
| EBF @ 3 months | 2.02 | 1.88 to 2.17 | 4063 | 6 | VERY-LOW | <0.001 | |
| EBF @ 6 months | 1.53 | 1.47 to 1.58 | 13926 | 19 | VERY-LOW | <0.001 | |
| HAZ | 0.10 | −0.04 to 0.25 | 5620 | 6 | - | 0.17 | |
| WAZ | −0.04 | −0.12 to 0.05 | 4565 | 3 | - | 0.42 | |
| WHZ | 0.01 | −0.07 to 0.09 | 4514 | 3 | - | 0.83 | |
| stunting | 1.00 | 0.88 to 1.14 | 6518 | 6 | - | 0.99 | |
| Underweight | 1.31 | 0.79 to 2.16 | 3448 | 3 | - | 0.30 | |
| WAWasting | 0.94 | 0.86 to 1.03 | 3925 | 2 | - | 0.19 | |
| Neonatal mortality (%) | 1.10 | 0.90 to 1.24 | 22752 | 2 | - | 0.35 | |
| Infant mortality (%) | 0.86 | 0.73 to 1.02 | 35943 | 2 | - | 0.08 | |
| Diarrheal disease | 0.76 | 0.67 to 0.85 | 4585 | 8 | - | <0.001 | |
| Incidence of infection | 1.96 | 0.65 to 5.93 | 1831 | 3 | - | 0.23 | |
| Complementary Feeding Education—Food Secure Settings | |||||||
| WAZ | 0.41 | 0.07 to 0.75 | 1562 | F4 | HIGH | 0.02 | |
| HAZ | 0.29 | 0.04 to 0.54 | 1560 | 4 | MODERATE | 0.03 | |
| WHZ | 0.22 | −0.03 to 0.47 | 1065 | 3 | MODERATE | 0.08 | |
| Stunting | 0.50 | 0.18 to 1.40 | 1006 | 3 | LOW | 0.19 | |
| Wasting | 0.19 | 0.03 to 1.18 | 665 | 2 | MODERATE | 0.07 | |
| Weight gain (kg) | 0.12 | −0.12 to 0.37 | 894 | 2 | MODERATE | 0.33 | |
| Height gain (cm) | 0.33 | −0.46 to 1.12 | 894 | 2 | LOW | 0.42 | |
| Complementary Feeding Education—Food Insecure Settings | |||||||
| WAZ | 0.47 | 0.35 to 0.59 | 572 | 1 | LOW | <0.001 | |
| HAZ | 0.25 | 0.09 to 0.41 | 572 | 1 | HIGH | 0.002 | |
| WHZ | 0.50 | 0.35 to 0.65 | 572 | 1 | HIGH | <0.001 | |
| Stunting | 0.65 | 0.42 to 1.01 | 1476 | 3 | LOW | 0.05 | |
| Wasting | 1.05 | 0.15 to 7.26 | 178 | 1 | MODERATE | 0.07 | |
| Weight gain (kg) | 0.01 | −0.07 to 0.08 | 1213 | 2 | LOW | 0.33 | |
| Height gain (cm) | −0.09 | −0.30 to 0.12 | 1214 | 2 | LOW | 0.42 | |
| Complementary Feed Provision Interventions—Food Secure Settings | |||||||
| WAZ | −0.09 | −0.34 to 0.16 | 172 | 1 | LOW | 0.48 | |
| HAZ | −0.12 | −0.46 to 0.22 | 172 | 1 | LOW | 0.49 | |
| WHZ | −0.03 | −0.28 to 0.22 | 172 | 1 | LOW | 0.81 | |
| Stunting | 0.47 | 0.37 to 0.59 | 2896 | 1 | HIGH | <0.001 | |
| Weight gain (kg) | −0.01 | −0.24 to 0.22 | 172 | 1 | LOW | 0.93 | |
| Height gain (cm) | −0.23 | −1.11 to 0.65 | 172 | 1 | LOW | 0.61 | |
| Complementary Feed Provision Interventions—Food Insecure Settings | |||||||
| WAZ | 0.34 | −0.35 to 1.03 | 3570 | 10 | VERY-LOW | 0.33 | |
| HAZ | 0.14 | 0.04 to 0.24 | 8996 | 12 | LOW | 0.005 | |
| WHZ | 0.01 | −0.01 to 0.03 | 8197 | 10 | LOW | 0.27 | |
| Stunting | 0.64 | 0.44 to 0.92 | 7894 | 7 | LOW | 0.02 | |
| Wasting | 0.87 | 0.74 to 1.01 | 7081 | 6 | MODERATE | 0.07 | |
| Weight gain (kg) | 0.62 | −0.02 to 1.26 | 986 | 3 | VERY-LOW | 0.06 | |
| Height gain (cm) | 0.17 | −0.11 to 0.44 | 924 | 3 | MODERATE | 0.24 | |
| Supplementary Feeding Interventions | |||||||
| HAZ | 0.11 | −0.03 to 0.24 | 3724 | 6 | LOW | 0.13 | |
| WAZ | 0.20 | −0.12 to 0.52 | 711 | 5 | VERY-LOW | 0.23 | |
| WHZ | 0.15 | 0.08 to 0.22 | 3664 | 6 | MODERATE | <10−5 | |
| Stunting | 1.31 | 0.95 to 1.81 | 1512 | 4 | LOW | 0.10 | |
| Wasting | 0.80 | 0.55 to 1.17 | 4299 | 4 | LOW | 0.25 | |
| Infant mortality (%) | 0.61 | 0.38 to 0.97 | 4757 | 2 | HIGH | 0.04 | |
| Weight gain (kg) | 0.06 | −0.01 to 0.12 | 845 | 5 | LOW | 0.08 | |
| Height gain (cm) | 0.13 | −0.03 to 0.35 | 832 | 5 | LOW | 0.11 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lassi, Z.S.; Rind, F.; Irfan, O.; Hadi, R.; Das, J.K.; Bhutta, Z.A. Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: Systematic Review. Nutrients 2020, 12, 722. https://doi.org/10.3390/nu12030722
Lassi ZS, Rind F, Irfan O, Hadi R, Das JK, Bhutta ZA. Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: Systematic Review. Nutrients. 2020; 12(3):722. https://doi.org/10.3390/nu12030722
Chicago/Turabian StyleLassi, Zohra S., Fahad Rind, Omar Irfan, Rabia Hadi, Jai K. Das, and Zulfiqar A. Bhutta. 2020. "Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: Systematic Review" Nutrients 12, no. 3: 722. https://doi.org/10.3390/nu12030722