
Nosocomial COVID-19 Infection in a Long-Term Hospital in Spain: Retrospective Observational Study

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
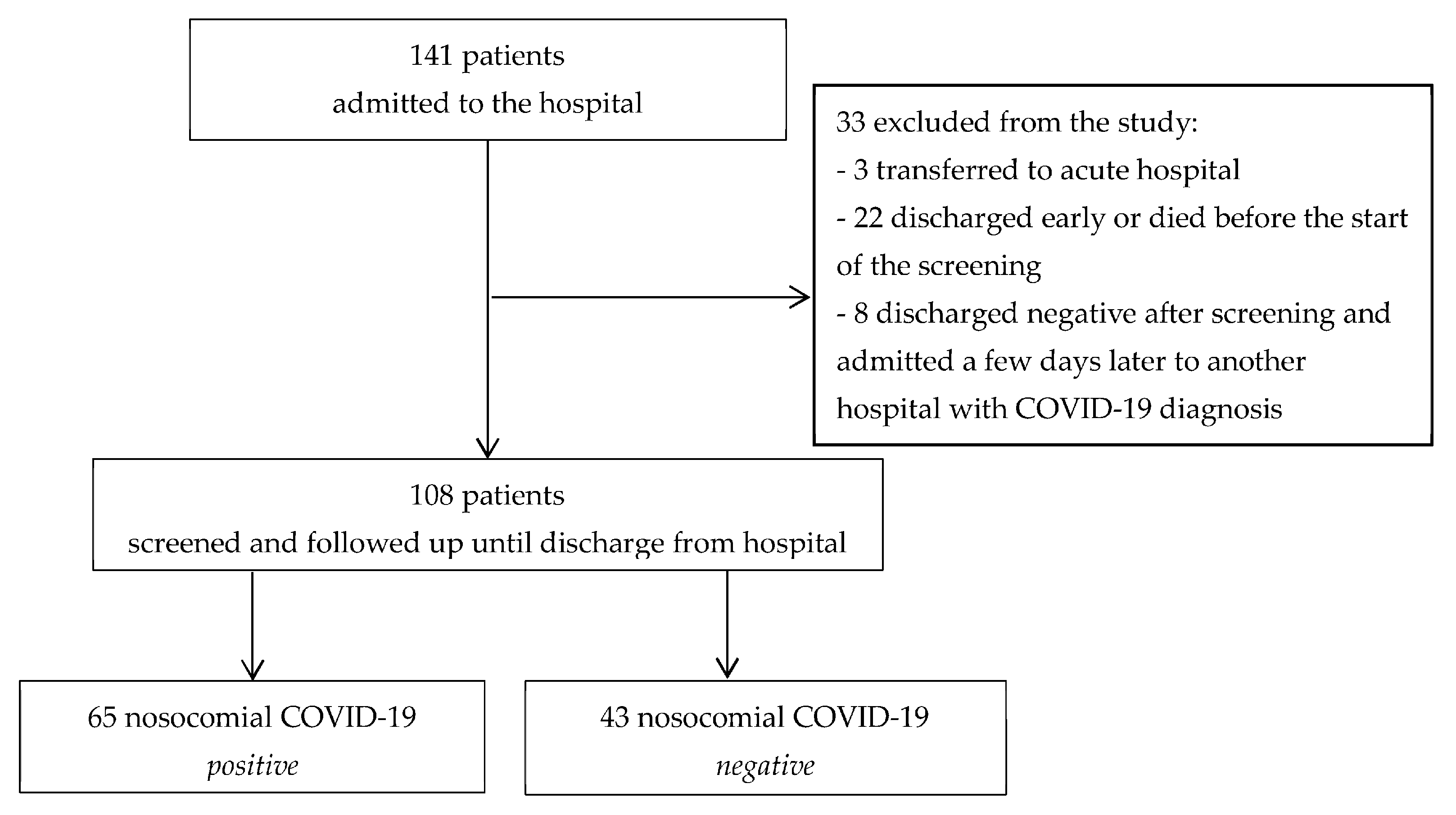
2.1. Design and Participants
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethical Aspects
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehra, M.R.; Desai, S.S.; Kuy, S.; Henry, T.D.; Patel, A.N. Cardiovascular disease, drug therapy, and mortality in COVID-19. N. Engl. J. Med. 2020, 382, e102. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report 105. 5 May 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200504-covid-19-sitrep-105.pdf?sfvrsn¼4cdda8af_2 (accessed on 5 May 2020).
- Johns Hopkins University center for Systems Science and Engineering. COVID-19 Global Cases. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 8 April 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Sum-mary of a report of 72,314 cases from the Chinese center for Dis-ease Control and Prevention. JAMA 2020, 323, 1239.e42. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Pfeiffer, E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Fuentelsaz, C. Validación de la escala EMINA©: Un instrumento de valoración del riesgo de desarrollar úlceras por presión en pacientes hospitalizados. Enferm. Clin. 2001, 11, 97–103. [Google Scholar] [CrossRef]
- Inouye, S.K.; van Dyck, C.H.; Alessi, C.A.; Balkin, S.; Siegal, A.P.; Horwitz, R.I. Clarifying confusion: The confusion assessment method. A new method for detection of delirium. Ann. Intern. Med. 1990, 113, 941–948. [Google Scholar] [CrossRef]
- Gómez-Batiste, X.; Martínez-Muñoz, M.; Blay, C.; Amblàs, J.; Vila, L.; Costa, X.; Espaulella, J.; Espinosa, J.; Figuerola, M. Proyecto NECPAL CCOMSICO©: Identification of people with chronic advanced diseases and need of palliative care in sociosanitary services: Elaboration of the NECPAL CCOMS-ICO© tool. Med. Clin. 2013, 140, 241–245. [Google Scholar] [CrossRef]
- Ulíbarri, J.I.; González-Madroño, A.; de Villar, N.G.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for Controlling Nutritional Status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Schwendimann, R.; De Geest, S.; Milisen, K. Evaluation of the Morse Fall Scale in hospitalised patients. Age Ageing 2006, 35, 311–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, D.; Kelly, D.; Goldstone, L.; Gammon, J. Examining the validity of pressure ulcer risk assessment scales: Developing and using illustrated patient simulations to collect the data. J. Clin. Nurs. 2001, 10, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061.e9. [Google Scholar] [CrossRef] [PubMed]
- Harding, L.; Campbell, D. Up to 20% of Hospital Patients with COVID-19 Caught It at Hospital. The Guardian. 17 May 2020. Available online: www.theguardian.com/world/2020/may/17/hospital-patients-england-coronavirus-covid-19 (accessed on 17 May 2020).
- Zhou, Q.; Gao, Y.; Wang, X.; Liu, R.; Du, P.; Wang, X.; COVID-19 Evidence and Recommendations Working Group. Nosocomial infections among patients with COVID-19, SARS and MERS: A rapid review and meta-analysis. Ann. Transl. Med. 2020, 8, 629. [Google Scholar] [CrossRef]
- Carter, B.; Collins, J.T.; Barlow-Pay, F.; Rickard, F.; Bruce, E.; Verduri, A.; Quinn, T.J.; Mitchell, E.; Price, A.; Vilches-Moraga, A.; et al. Nosocomial COVID-19 infection: Examining the risk of mortality. The COPE-Nosocomial Study (COVID in Older PEople). J. Hosp. Infect. 2020, 106, 376–384. [Google Scholar] [CrossRef]
- Ponsford, M.J.; Ward, T.J.; Stoneham, S.; Dallimore, C.M.; Sham, D.; Osman, K.; Barry, S.M.; Jolles, S.; Humphreys, I.R.; Farewell, D. A Systematic Review and Meta-Analysis of Inpatient Mortality Associated with Nosocomial and Community COVID-19 Exposes the Vulnerability of Immunosuppressed Adults. Front. Immunol. 2021, 12, 744696. [Google Scholar] [CrossRef]
- Wang, Q.; Davis, P.B.; Gurney, M.E.; Xu, R. COVID-19 and dementia: Analyses of risk, disparity, and outcomes from electronic health records in the US. Alzheimers Dement. 2021, 17, 1297–1306. [Google Scholar] [CrossRef]
- Ryg, J.; Engberg, H.; Mariadas, P.; Pedersen, S.G.H.; Jorgensen, M.G.; Vinding, K.L.; Andersen-Ranberg, K. Barthel Index at hospital admission is associated with mortality in geriatric patients: A Danish nationwide population-based cohort study. Clin. Epidemiol. 2018, 10, 1789–1800. [Google Scholar] [CrossRef] [Green Version]
- Kashani, K.B. Hypoxia in COVID-19: Sign of Severity or Cause for Poor Outcomes. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2020; Volume 95, pp. 1094–1096. [Google Scholar] [CrossRef]
- Xie, J.; Covassin, N.; Fan, Z.; Singh, P.; Gao, W.; Li, G.; Kara, T.; Somers, V.K. Association Between Hypoxemia and Mortality in Patients with COVID-19. In Mayo Clinic Proceedings; Elsevier: Amsterdam, The Netherlands, 2020; Volume 95, pp. 1138–1147. [Google Scholar] [CrossRef]
- Ramos-Rincon, J.M.; Buonaiuto, V.; Ricci, M.; Martín-Carmona, J.; Paredes-Ruíz, D.; Calderón-Moreno, M.; Rubio-Rivas, M.; Beato-Pérez, J.L.; Arnalich-Fernández, F.; Monge-Monge, D.; et al. Clinical Characteristics and Risk Factors for Mortality in Very Old Patients Hospitalized With COVID-19 in Spain. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, e28–e37. [Google Scholar] [CrossRef]
- Ramos-Rincón, J.M.; Bernabeu-Wittel, M.; Fiteni-Mera, I.; López-Sampalo, A.; López-Ríos, C.; García-Andreu, M.D.M.; Mancebo-Sevilla, J.J.; Jiménez-Juan, C.; Matía-Sanz, M.; López-Quirantes, P.; et al. SEMI-COVID-19 Network. Clinical features and risk factors for mortality among long-term care facility residents hospitalized due to COVID-19 in Spain. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 77, e138–e147. [Google Scholar] [CrossRef]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 infections and transmission in a skilled nursing facility. N. Engl. J. Med. 2020, 382, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Calsina-Berna, A.; Martinez-Muñoz, M.; Bardés Robles, I.; Beas Alba, E.; Madariaga Sánchez, R.; Gómez Batiste Alentorn, X. Intrahospital Mortality and Survival of Patients with Advanced Chronic Illnesses in a Tertiary Hospital Identified with the NECPAL CCOMS-ICO © Tool. J. Palliat. Med. 2018, 21, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Vilma, A.; Tripodoro, V.A.; Victoria Llanos, V.; Silvina De Lellis, S.; Cecilia Salazar Güemes, C.; Gabriel, G.; De Simone, G.G.; Xavier Gómez-Batiste, X. Prognostic factors in cancer patients with palliative needs identified by the NECPAL CCOMS-ICO© tool. Medicina 2019, 79, 95–103. [Google Scholar]
- Gómez-Batiste, X.; Pamela Turrillas, P.; Cristian Tebé, C.; Agnès Calsina-Berna, A.; Amblàs-Novellas, J. NECPAL tool prognostication in advanced chronic illness: A rapid review and expert consensus. BMJ Support. Palliat. Care 2020. [Google Scholar] [CrossRef] [PubMed]
- Girum, T.; Lentiro, K.; Geremew, M.; Migora, B.; Shewamare, S. Global strategies and effectiveness for COVID-19 prevention through contact tracing, screening, quarantine, and isolation: A systematic review. Trop. Med. Health 2020, 48, 91. [Google Scholar] [CrossRef]


{kind=link}
| COVID-19 (n = 65) | No COVID-19 (n = 43) | p Value | |
|---|---|---|---|
| Age, years, median (IQR) | 81 (70–89) | 73 (65–84) | 0.092 |
| Sex, n (%) | 0.12 | ||
| Female | 34 (52) | 27 (63) | |
| Male | 31 (48) | 16 (37) | |
| Hospitalization units, n (%) | 0.72 | ||
| Convalescence | 37 (57) | 28 (65) | |
| Long-stay | 15 (23) | 8 (19) | |
| Palliative care | 8 (12) | 3 (7) | |
| Brain injury | 5(8) | 4 (9) | |
| Charlson (score), median (IQR) | 6.0 (5–9) | 5 (3–7) | 0.028 |
| Comorbidities, n (%) | |||
| Hypertension | 50 (76.9) | 27 (62.8) | 0.11 |
| Cerebrovascular disease | 24 (36.9) | 10 (23.3) | 0.13 |
| Diabetes mellitus | 23 (35.4) | 15 (34.9) | 0.96 |
| Dementia | 22 (33.8) | 4 (9.3) | 0.003 |
| Lung disease | 20 (30.8) | 9 (20.9) | 0.26 |
| Heart disease | 17 (26.2) | 12 (27.9) | 0.84 |
| Kidney disease | 15 (23.1) | 11 (25.6) | 0.77 |
| Symptoms, n (%) | |||
| Cough | 49 (75.4) | 37 (86) | 0.18 |
| Hypoxemia * | 32 (97) | 1 (3) | <0.001 |
| Dyspnea | 23 (35.4) | 4 (9.3) | 0.002 |
| Confusion/disorientation | 21 (32.3) | 7 (16.3) | 0.063 |
| Asthenia | 18 (27.7) | 3 (7) | 0.008 |
| Fever | 4 (6.2) | 3 (7) | 0.87 |
| Constants in PCR screening | |||
| Baseline SatO2, median (IQR) | 96 (95–98) | 97 (96–98) | 0.11 |
| Heart rate, bpm, mean (SD) | 79 (16.60) | 78 (13.01) | 0.84 |
| Temperature, °C, mean (SD) | 36.53 (0.36) | 36.46 (0.51) | 0.44 |
| Systolic blood pressure, mmHg, mean (SD) | 122 (19.82) | 127 (15.84) | 0.10 |
| Diastolic blood pressure, mmHg, mean (SD) | 68 (11.97) | 72 (13.20) | 0.17 |
| Analytical results | |||
| Glomerular filtration rate, mL/min, median (IQR) | 80.9 (47.54–90) | 80.2 (18.17–90) | 0.86 |
| C-reactive protein, mg/L, median (IQR) | 3.75 (1–10.67) | 0.43 (1.61–7.32) | 0.33 |
| Lactate dehydrogenase, UI/L, median (IQR) | 258 (197–307) | 228 (194–285) | 0.94 |
| Lymphocytes, ×103, mean (IQR) | 1358 (801) | 1537 (710) | 0.24 |
| Ferritin, µg/L, mean (SD) | 997 (1726) | 563 (564) | 0.14 |
| Chest X-ray, n (%) | 0.21 | ||
| Normal | 25 (45.5) | 14 (56) | |
| Unilateral pneumonia | 14 (25.5) | 4 (16) | |
| Bilateral pneumonia | 9 (16.4) | 1 (4) | |
| Treatment, n (%) | |||
| Antibiotics | 32 (49.2) | 7 (16.3) | 0.001 |
| Corticosteroids | 38 (58.5) | 5 (11.6) | <0.001 |
| Ventilatory support | 45 (69.2) | 14 (33.3) | <0.001 |
| Oxygen therapy | 42 (93.3) | 14 (93.3) | 0.71 |
| Mortality, n (%) | 29 (44.6) | 7 (16.3) | 0.002 |
| COVID-19 (n = 65) | No COVID-19 (n= 43) | p Value | |
|---|---|---|---|
| NECPAL, median (IQR) | 6 (2–8.5) | 2 (0–4) | <0.001 |
| Barthel, median (IQR) | 10 (0–20) | 15 (5–52.5) | 0.011 |
| CAM, median (IQR) | 3.5 (0–7) | 0 (0–2) | 0.020 |
| Clinical Frailty Scale, median (IQR) | 7 (6.5–8) | 7 (5–8) | 0.064 |
| EMINA scale median (IQR) | 8 (7–10) | 7 (5–8) | 0.11 |
| CONUT, median (IQR) | 5 (4–7) | 5 (2–7) | 0.31 |
| VAS, median (IQR) | 0 (0–1) | 1 (0–1) | 0.46 |
| Pfeiffer, median (IQR) | 5 (1–9) | 6 (2–9) | 0.67 |
| Morse fall scale, median (IQR) | 50 (35–65) | 55 (35–75) | 0.88 |
| COVID-19 n = 29 (44.6%) n (%) | No COVID-19 n = 7 (16.2%) n (%) | p Value | |
|---|---|---|---|
| COVID-19 | 9 (31) | 0 (0) | 0.16 |
| Cardiovascular diseases | 5 (17.2) | 1 (14.3) | 1.00 |
| Neoplasm | 5 (17.2) | 2 (28.6) | 0.60 |
| Infectious disease other than COVID-19 | 4 (13.8) | 4 (57.1) | 0.027 |
| Advanced dementia | 3 (10.3) | 0 (0) | 1.00 |
| Severe obstructive lung disease | 1 (3.4) | 0 (0) | 1.00 |
| Chronic end-stage kidney disease | 1 (3.4) | 0 (0) | 1.00 |
| Cirrhosis | 1 (3.4) | 0 (0) | 1.00 |
| Died (n = 29) | Survived (n = 36) | Crude OR (95% CIs) | p Value | |
|---|---|---|---|---|
| Age, years | 82 (73–90) | 80.5 (64–86.5) | 0.98 (0.94–1.01) | 0.24 |
| Sex, n (%) | 0.36 | |||
| Female | 17 (59) | 17 (49) | 1 | |
| Male | 12 (41) | 19 (53) | 0.63 (0.23–1.70) | |
| Scales | ||||
| NECPAL, median (IQR) | 4.49 (4.4) | 3.2 (3.11) | 1.20 (1.05–1.39) | 0.009 |
| Symptoms, n (%) | ||||
| Hypoxemia * | 19 (65.5) | 13 (36.1) | 3.36 (1.21–9.36) | 0.018 |
| Dyspnea | 16 (55.2) | 7 (19.4) | 5.09 (1.69–15.37) | 0.003 |
| Confusion/disorientation | 15 (51.7) | 6 (16.7) | 5.36 (1.71–16.74) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caro-Martínez, E.; Abad-Collado, S.; Escrivá-Cerrudo, B.; García-Almarza, S.; García-Ródenas, M.d.M.; Gómez-Merino, E.; Serrano-Mateo, M.-I.; Ramos-Rincón, J.-M. Nosocomial COVID-19 Infection in a Long-Term Hospital in Spain: Retrospective Observational Study. Medicina 2022, 58, 566. https://doi.org/10.3390/medicina58050566
Caro-Martínez E, Abad-Collado S, Escrivá-Cerrudo B, García-Almarza S, García-Ródenas MdM, Gómez-Merino E, Serrano-Mateo M-I, Ramos-Rincón J-M. Nosocomial COVID-19 Infection in a Long-Term Hospital in Spain: Retrospective Observational Study. Medicina. 2022; 58(5):566. https://doi.org/10.3390/medicina58050566
Chicago/Turabian StyleCaro-Martínez, Elena, Susana Abad-Collado, Blanca Escrivá-Cerrudo, Shaila García-Almarza, María del Mar García-Ródenas, Elena Gómez-Merino, María-Isabel Serrano-Mateo, and Jose-Manuel Ramos-Rincón. 2022. "Nosocomial COVID-19 Infection in a Long-Term Hospital in Spain: Retrospective Observational Study" Medicina 58, no. 5: 566. https://doi.org/10.3390/medicina58050566