Implementation of a Renal Precision Medicine Program: Clinician Attitudes and Acceptance

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Implementation
2.2. Demographics
2.3. The Survey
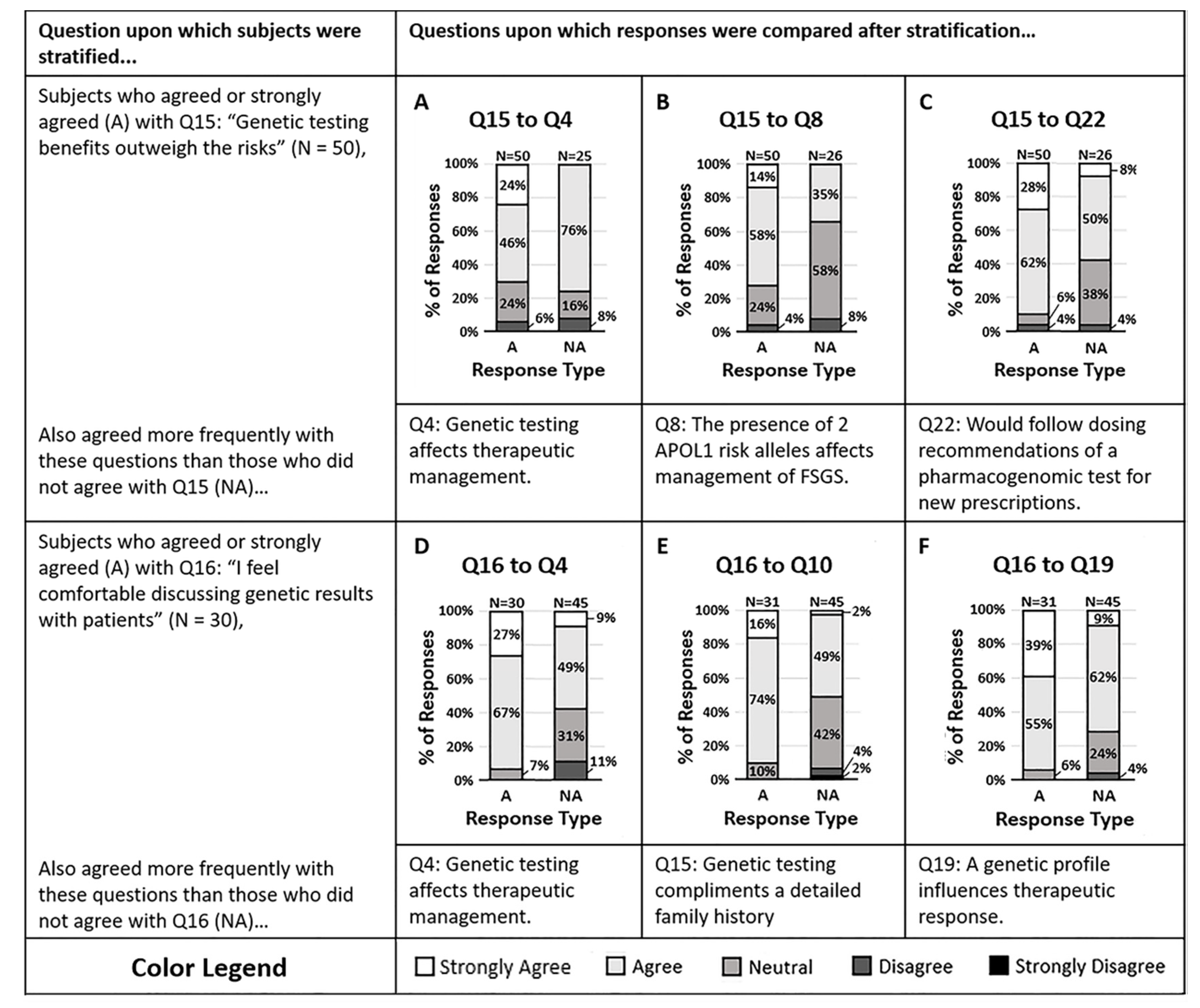
2.4. General Knowledge and Attitude Toward Genetics
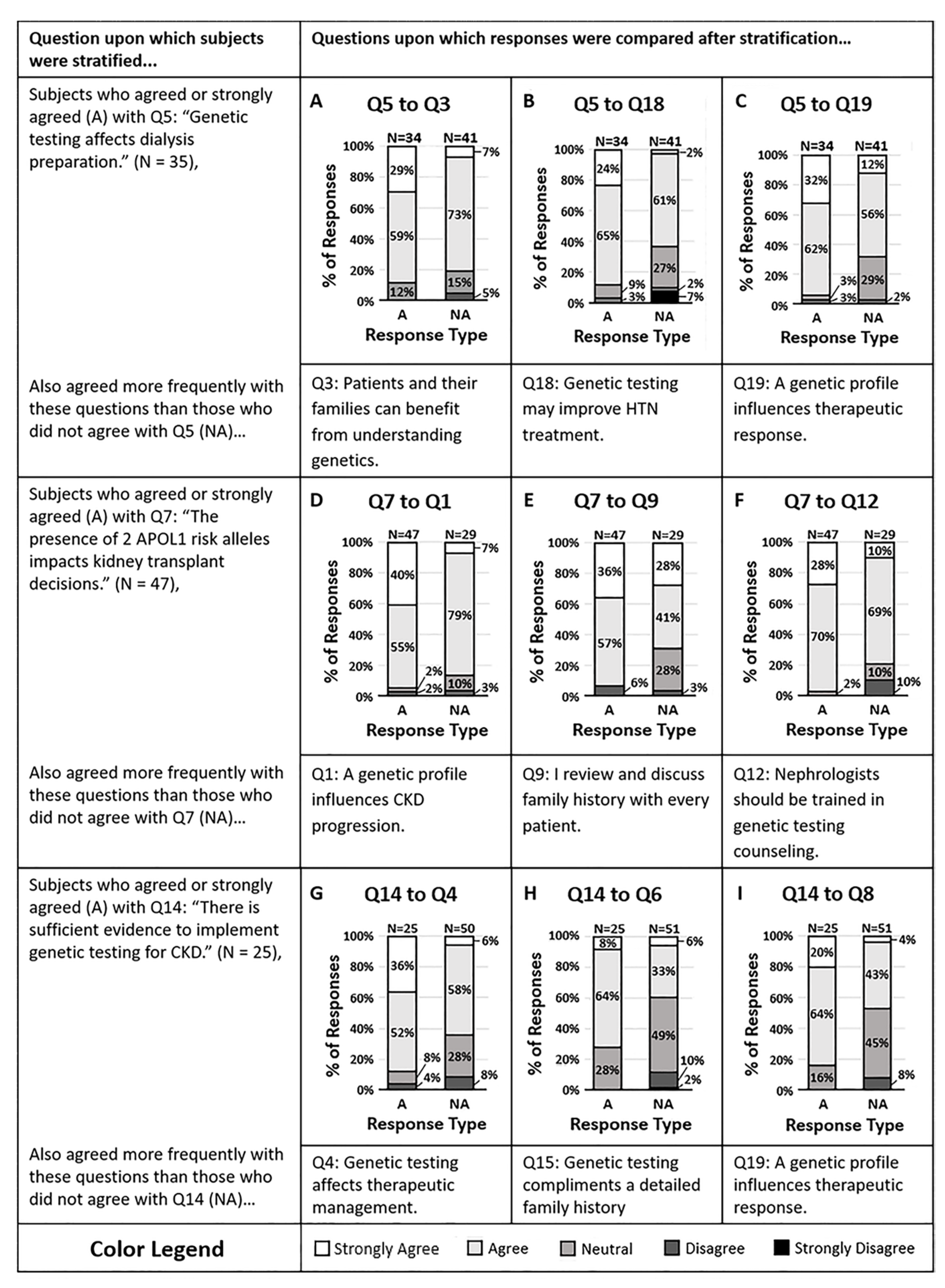
2.5. Genetics Predictors of Chronic Kidney Disease Progression
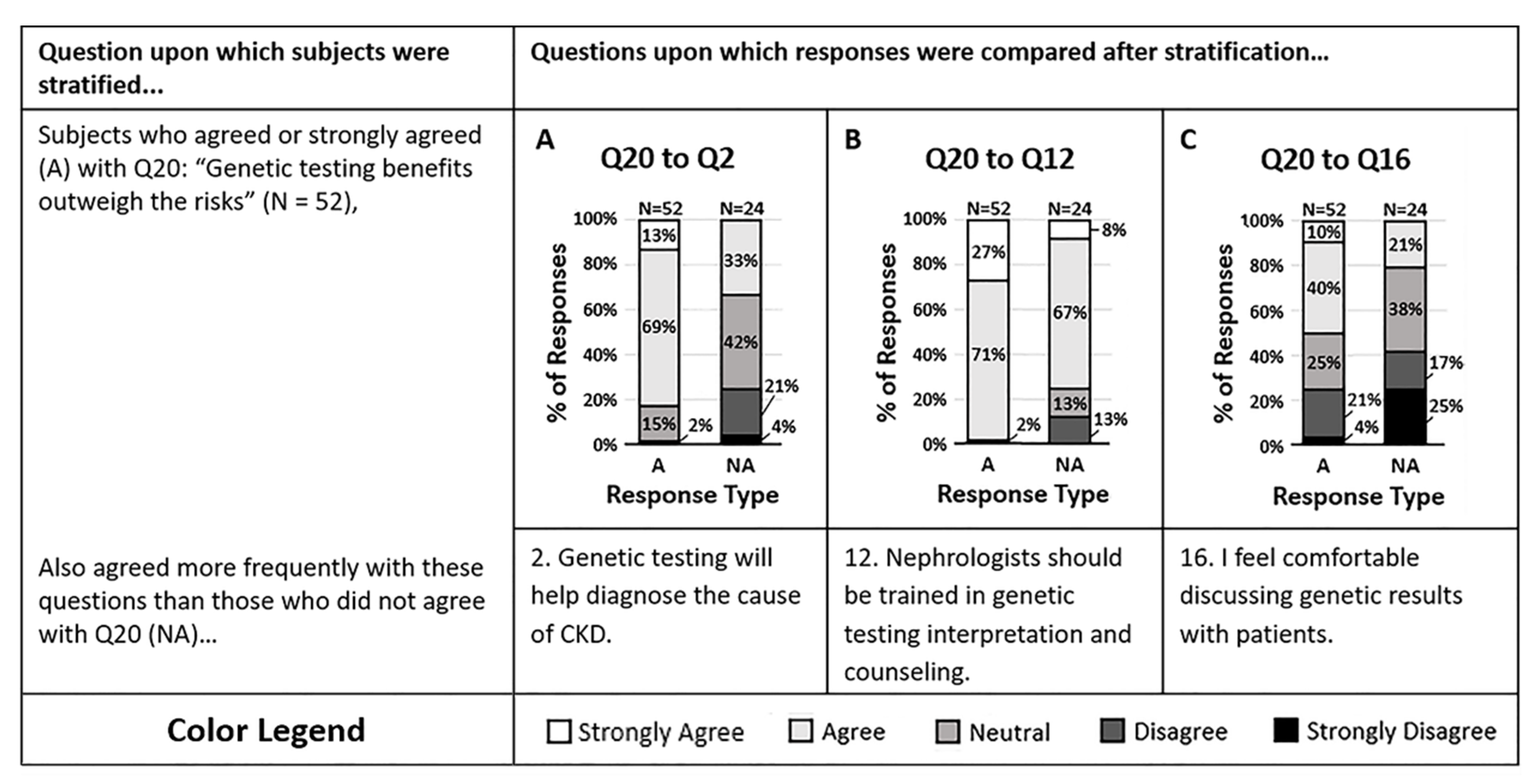
2.6. Genetics Predicting Antihypertensive Response
3. Materials and Methods
3.1. Participants
3.2. The Survey
4. Analysis
5. Statistics
6. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Liu, C.T.; Garnaas, M.K.; Tin, A.; Kottgen, A.; Franceschini, N.; Peralta, C.A.; de Boer, I.H.; Lu, X.; Atkinson, E.; Ding, J.; et al. Genetic association for renal traits among participants of African ancestry reveals new loci for renal function. PLoS Genet. 2011, 7, e1002264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fryar, C.D.; Ostchega, Y.; Hales, C.M.; Zhang, G.; Kruszon-Moran, D. Hypertension prevalence and control among adults: United states, 2015–2016. NCHS Data Brief. 2017, 289, 1–8. [Google Scholar]
- Parsa, A.; Kanetsky, P.A.; Xiao, R.; Gupta, J.; Mitra, N.; Limou, S.; Xie, D.; Xu, H.; Anderson, A.H.; Ojo, A.; et al. Genome-Wide Association of CKD progression: The chronic renal insufficiency cohort study. J. Am. Soc. Nephrol. 2017, 28, 923–934. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Li, Y.; Tang, J.T.; An, Y.F.; Luo, L.M.; Dai, B.; Shi, Y.Y.; Wang, L.L. The influence of living donor SHROOM3 and ABCB1 genetic variants on renal function after kidney transplantation. Pharm. Genom. 2017, 27, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Boger, C.A.; Gorski, M.; Li, M.; Hoffmann, M.M.; Huang, C.; Yang, Q.; Teumer, A.; Krane, V.; O’Seaghdha, C.M.; Kutalik, Z.; et al. Association of eGFR-Related Loci Identified by GWAS with Incident CKD and ESRD. PLoS Genet. 2011, 7, e1002292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Wang, Q.; Li, G.; Wang, L. A single nucleotide polymorphism in the UMOD promoter is associated with end stage renal disease. BMC Med. Genet. 2016, 17, 95. [Google Scholar] [CrossRef] [Green Version]
- Parsa, A.; Kao, W.H.; Xie, D.; Astor, B.C.; Li, M.; Hsu, C.Y.; Feldman, H.I.; Parekh, R.S.; Kusek, J.W.; Greene, T.H.; et al. APOL1 risk variants, race, and progression of chronic kidney disease. N. Engl. J. Med. 2013, 369, 2183–2196. [Google Scholar] [CrossRef] [Green Version]
- Kottgen, A.; Pattaro, C.; Boger, C.A.; Fuchsberger, C.; Olden, M.; Glazer, N.L.; Parsa, A.; Gao, X.; Yang, Q.; Smith, A.V.; et al. New loci associated with kidney function and chronic kidney disease. Nat. Genet. 2010, 42, 376–384. [Google Scholar] [CrossRef] [Green Version]
- Alwi, Z.B. The use of SNPs in pharmacogenomics studies. Malays. J. Med. Sci. 2005, 12, 4–12. [Google Scholar]
- Mancinelli, L.; Cronin, M.; Sadee, W. Pharmacogenomics: The promise of personalized medicine. AAPS PharmSci 2000, 2, E4. [Google Scholar] [CrossRef]
- Eadon, M.T.; Chapman, A.B. A physiologic approach to the pharmacogenomics of hypertension. Adv. Chronic Kidney Dis. 2016, 23, 91–105. [Google Scholar] [CrossRef] [Green Version]
- Relling, M.V.; Klein, T.E.; Gammal, R.S.; Whirl-Carrillo, M.; Hoffman, J.M.; Caudle, K.E. The clinical pharmacogenetics implementation consortium: 10 years later. Clin. Pharmacol. Ther. 2020, 107, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Swen, J.J.; Nijenhuis, M.; de Boer, A.; Grandia, L.; Maitland-van der Zee, A.H.; Mulder, H.; Rongen, G.A.; van Schaik, R.H.; Schalekamp, T.; Touw, D.J.; et al. Pharmacogenetics: From bench to byte--An update of guidelines. Clin. Pharmacol. Ther. 2011, 89, 662–673. [Google Scholar] [CrossRef]
- Eadon, M.T.; Desta, Z.; Levy, K.D.; Decker, B.S.; Pierson, R.C.; Pratt, V.M.; Callaghan, J.T.; Rosenman, M.B.; Carpenter, J.S.; Holmes, A.M.; et al. Implementation of a pharmacogenomics consult service to support the INGENIOUS trial. Clin. Pharmacol. Ther. 2016, 100, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Collins, K.S.; Pratt, V.M.; Stansberry, W.M.; Medeiros, E.B.; Kannegolla, K.; Swart, M.; Skaar, T.C.; Chapman, A.B.; Decker, B.S.; Moorthi, R.N.; et al. Analytical validity of a genotyping assay for use with personalized antihypertensive and chronic kidney disease therapy. Pharm. Genom. 2019, 29, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Lovelace, M.; Brickman, P. Best practices for measuring students’ attitudes toward learning science. CBE Life Sci. Educ. 2013, 12, 606–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eadon, M.T.; Kanuri, S.H.; Chapman, A.B. Pharmacogenomic studies of hypertension: Paving the way for personalized antihypertensive treatment. Expert Rev. Precis. Med. Drug Dev. 2018, 3, 33–47. [Google Scholar] [CrossRef]
- Ponto, J. Understanding and evaluating survey research. J. Adv. Pract. Oncol. 2015, 6, 168–171. [Google Scholar]
- Clason, D.L.; Dormody, T.J. Analyzing data measured by individual likert-type items. J. Agric. Ed. 1994, 35, 4. [Google Scholar] [CrossRef]
- Sisson, D.A.; Stocker, H.R. Analyzing and interpreting likert-type survey data. Delta Pi Epsil. J. 1989, 31, 81–85. [Google Scholar]
- Nadkarni, G.N.; Horowitz, C.R. Genomics in CKD: Is this the path forward? Adv. Chronic Kidney Dis. 2016, 23, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Nestor, J.G.; Groopman, E.E.; Gharavi, A.G. Towards precision nephrology: The opportunities and challenges of genomic medicine. J. Nephrol. 2018, 31, 47–60. [Google Scholar] [CrossRef] [PubMed]
- McPherson, E. Genetic diagnosis and testing in clinical practice. Clin. Med. Res. 2006, 4, 123–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.H.; Min, B.J.; Kim, J.H. Personal genome testing on physicians improves attitudes on pharmacogenomic approaches. PLoS ONE 2019, 14, e0213860. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, G.R.; Sinkunas, V.; Liguori, G.R.; Auler-Junior, J.O.C. Precision medicine: Changing the way we think about healthcare. Clinics (Sao Paulo) 2018, 73, e723. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, G.S.; Phillips, K.A. Precision medicine: From science to value. Health Aff. (Millwood) 2018, 37, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Alzu’bi, A.A.; Zhou, L.; Watzlaf, V.J.M. Genetic variations and precision medicine. Perspect. Health Inf. Manag. 2019, 16, 1a. [Google Scholar]
- Chen, W.; Xu, L.; Wang, Z.Y.; Xue, L.J.; Xue, F.L.; Jiang, M.J.; Wang, Q.P.; Zheng, H.L. Haplotype analysis of the XRCC1 gene and laryngeal cancer. Genet. Test. Mol. Biomark. 2014, 18, 525–529. [Google Scholar] [CrossRef] [Green Version]
- Reinhard, J.; Drepper, C.; Weber, H.; Schiele, M.A.; Kneer, K.; Mittermeier, A.; Frey, L.; Reif, A.; Pauli, P.; Domschke, K.; et al. Anxiety risk SNPs on chromosome 2 modulate arousal in children in a fear generalization paradigm. Eur. Child Adolesc. Psychiatry 2019. [Google Scholar] [CrossRef] [Green Version]
- Kensler, T.W.; Spira, A.; Garber, J.E.; Szabo, E.; Lee, J.J.; Dong, Z.; Dannenberg, A.J.; Hait, W.N.; Blackburn, E.; Davidson, N.E.; et al. Transforming Cancer Prevention through Precision Medicine and Immune-oncology. Cancer Prev. Res. (Phila.) 2016, 9, 2–10. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, P.H.; Wadhwa, N.; Danahey, K.; Borden, B.A.; Lee, S.M.; Hall, J.P.; Klammer, C.; Hussain, S.; Siegler, M.; Sorrentino, M.J.; et al. Pharmacogenomics-Based Point-of-Care Clinical Decision Support Significantly Alters Drug Prescribing. Clin. Pharmacol. Ther. 2017, 102, 859–869. [Google Scholar] [CrossRef] [PubMed]
- Just, K.S.; Steffens, M.; Swen, J.J.; Patrinos, G.P.; Guchelaar, H.J.; Stingl, J.C. Medical education in pharmacogenomics-results from a survey on pharmacogenetic knowledge in healthcare professionals within the European pharmacogenomics clinical implementation project Ubiquitous Pharmacogenomics (U-PGx). Eur. J. Clin. Pharmacol. 2017, 73, 1247–1252. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gene | Variants Tested | Relevant Phenotype |
|---|---|---|
| ADRB1 | rs1801252, rs1801253 | Beta-Blocker Efficacy |
| APOL1 | rs73885319, rs60910145, rs71785313 | Risk of CKD |
| CYP2C19 | rs4244285, rs4986893, rs28399504, rs72552267, rs41291556, rs6413438, rs12248560 | Clopidogrel Efficacy |
| CYP2C9 | rs1799853, rs1057910, rs28371686, rs9332131, rs7900194, rs28371685 | Losartan Efficacy |
| CYP2D6 | rs16947, rs1135840, rs35742686, rs3892097, rs1065852, rs5030655, rs5030867, rs5030865(A), rs5030656, rs1065852, rs1135840, rs5030865(T), rs28371706, rs61736512, rs59421388, rs1135840, rs28371725 | Metoprolol Efficacy |
| CYP3A4 | rs55785340, rs35599367 | Tacrolimus Dosing |
| CYP3A5 | rs776746, rs10264272, rs41303343 | Tacrolimus Dosing |
| F7 | rs6046 | Amlodipine Efficacy |
| FGF5/SH2B3/EBF1 | rs1458038, rs3184504, rs4551053 | Thiazide Efficacy |
| GRK4 | rs2960306, rs1024323 | Beta-Blocker Efficacy |
| LINC00923 | rs653747 | Risk of CKD |
| LOC105369332 | rs2282538 | Risk of CKD |
| NAT2 | rs1801279, rs1801280, rs1799930, rs1799931 | Hydralazine Efficacy |
| NEDD4L | rs4149601 | Diuretic Efficacy |
| NPHS1 | rs3814995 | Angiotensin receptor blocker efficacy |
| SLC3A2 | rs489381 | Risk of CKD |
| SLCO1B1 | rs4149056, rs4149015 | Simvastatin Dosing |
| SHROOM3 | rs17319721, rs4371638, rs13146355 | Risk of CKD |
| TPMT | rs1800462, rs1800460 and rs1142345, rs1800460, rs1142345, rs1800584 | Azathioprine Dosing |
| UMOD/PDILT | rs4293393, rs12917707, rs11864909 | Risk of CKD |
| VASP | rs10995 | Thiazide Efficacy |
| VKORC1 | rs9923231 | Warfarin Sensitivity |
| YEATS4 | rs7297610 | Thiazide Efficacy |
| Demographic | Respondents (%) |
|---|---|
| Total N | 76 (-) |
| Gender | |
| Female | 27 (35.5) |
| Male | 47 (61.8) |
| Other or prefer not to answer | 1 (1.3) |
| No response | 1 (1.3) |
| Race | |
| Black or African American | 1 (1.3) |
| American Indian or Alaska Native | 1 (1.3) |
| Asian | 23 (30.3) |
| Hispanic or Latino | 1 (1.3) |
| Native Hawaiian or Pacific Islander | 0 (0) |
| White or Caucasian | 42 (55.3) |
| Other or prefer not to answer | 5 (6.6) |
| No response | 3 (3.9) |
| Training | |
| Trainee | 37 (48.7) |
| Nephrologist | 39 (51.3) |
| Other | 0 (0) |
| Health System | |
| County Safety Net Hospital | 9 (11.8) |
| University Hospital | 32 (42.1) |
| Affiliated University Hospital with private practice model | 17 (22.4) |
| Pediatric Hospital | 3 (3.9) |
| Veteran Affairs Hospital | 7 (9.2) |
| Unknown | 8 (10.5) |
| Question | Condition | Discipline | Mean (SD) Agreement |
|---|---|---|---|
| 1. A patient’s genetic profile can influence their risk of CKD progression | CKD | Knowledge | 4.2 (0.6) |
| 2. Genetic testing will help me to better diagnose the cause of my patient’s CKD | CKD | Action | 3.6 (0.8) |
| 3. Patients and their families can benefit from understanding genetic contributors to their CKD. | CKD | Attitude | 4.0 (0.6) |
| 4. Genetic testing of my CKD patients provides information that may change my therapeutic management of patients. | CKD | Action | 3.8 (0.8) |
| 5. Genetic testing of my CKD patients provides information that changes dialysis preparation strategies in my patients. | CKD | Action | 3.3 (0.9) |
| 6. Genetic testing for CKD provides information that will help me delay or halt the progression of CKD in my patients. | CKD | Action | 3.5 (0.8) |
| 7. The presence of 2 APOL1 risk alleles in a potential donor would impact the decision to donate a kidney for transplantion. | CKD | Action | 3.8 (0.8) |
| 8. The presence of 2 APOL1 risk alleles in a patient would impact my management of Focal Segmental Glomerulosclerosis (FSGS). | CKD | Action | 3.6 (0.7) |
| 9. I personally review and discuss a family history (taken by myself or a physician-in-training/nurse/physician extender) for every patient I meet in the hospital or in a clinic. | General | Attitude | 4.1 (0.8) |
| 10. Genetic testing is a valuable complement to a detailed family history. | General | Knowledge | 3.7 (0.7) |
| 11. Discussing genetic testing results with patients will lead to increased patient anxiety. | General | Attitude | 3.1 (1.1) |
| 12. Nephrologists should be trained to interpret and counsel patients on genetic variants that contribute to CKD. | CKD | Attitude | 4.1 (0.6) |
| 13. Genetic counselors should be trained to interpret and counsel patients on genetic variants that contribute to CKD. | CKD | Attitude | 4.2 (0.6) |
| 14. There is sufficient evidence to implement genetic testing in patients with CKD. | CKD | Knowledge | 3.2 (0.9) |
| 15. The benefits of genetic testing outweigh the risks to patients. | General | Knowledge | 3.8 (0.7) |
| 16. I feel comfortable discussing genetic test results with patients. | General | Attitude | 3.1 (1.1) |
| 17. A discussion of genetic test results is too time-consuming for a clinic encounter. | General | Attitude | 3.3 (1.0) |
| 18. Genetic testing may help me better treat my patient’s hypertension. | HTN | Knowledge | 3.8 (0.8) |
| 19. A patient’s genetic profile can influence their therapeutic response to antihypertensives. | HTN | Knowledge | 4.0 (0.7) |
| 20. Genetic testing of my HTN patients provides information that may change the antihypertensives that I prescribe. | HTN | Action | 3.8 (0.9) |
| 21. Genetic testing of my HTN patients provides information that may help me better achieve the recommended blood pressure goals. | HTN | Action | 3.7 (0.8) |
| 22. Provided no contraindications exist, I would follow the dosing suggestions of a pharmacogenomic test for a NEW prescription if the test indicated an alternate medication or dose was appropriate. | HTN | Action | 4.0 (0.7) |
| 23. Provided no contraindications exist, I would change an EXISTING prescription, one in which the patient had a stable response, in order to follow the dosing suggestions of a pharmacogenomic test if the test indicated an alternate medication or dose was appropriate. | HTN | Action | 3.4 (0.9) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spiech, K.M.; Tripathy, P.R.; Woodcock, A.M.; Sheth, N.A.; Collins, K.S.; Kannegolla, K.; Sinha, A.D.; Sharfuddin, A.A.; Pratt, V.M.; Khalid, M.; et al. Implementation of a Renal Precision Medicine Program: Clinician Attitudes and Acceptance. Life 2020, 10, 32. https://doi.org/10.3390/life10040032
Spiech KM, Tripathy PR, Woodcock AM, Sheth NA, Collins KS, Kannegolla K, Sinha AD, Sharfuddin AA, Pratt VM, Khalid M, et al. Implementation of a Renal Precision Medicine Program: Clinician Attitudes and Acceptance. Life. 2020; 10(4):32. https://doi.org/10.3390/life10040032
Chicago/Turabian StyleSpiech, Katherine M., Purnima R. Tripathy, Alex M. Woodcock, Nehal A. Sheth, Kimberly S. Collins, Karthik Kannegolla, Arjun D. Sinha, Asif A. Sharfuddin, Victoria M. Pratt, Myda Khalid, and et al. 2020. "Implementation of a Renal Precision Medicine Program: Clinician Attitudes and Acceptance" Life 10, no. 4: 32. https://doi.org/10.3390/life10040032