Application of a Perception Neuron® System in Simulation-Based Surgical Training

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
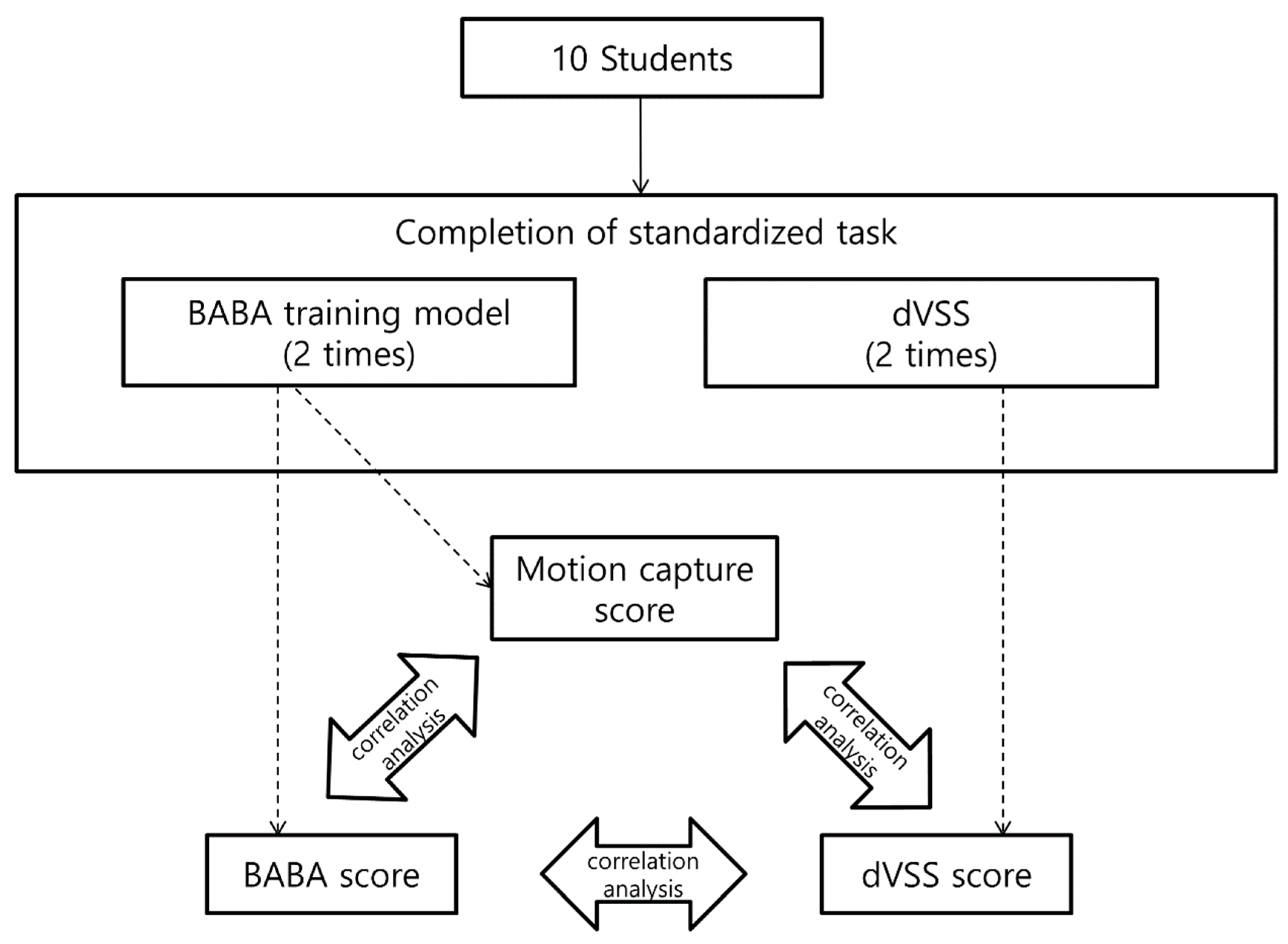
2.1. Participants and Study Design
2.2. BABA Training Model and Standardized Tasks
2.3. Use of the Motion Capture System to Capture the Movements of the Participants during BABA Training
2.4. dVSS® and Standardized Tasks
2.5. Calculate Participants’ Proficiency (MC Score)
2.6. Statistical Analysis
3. Results
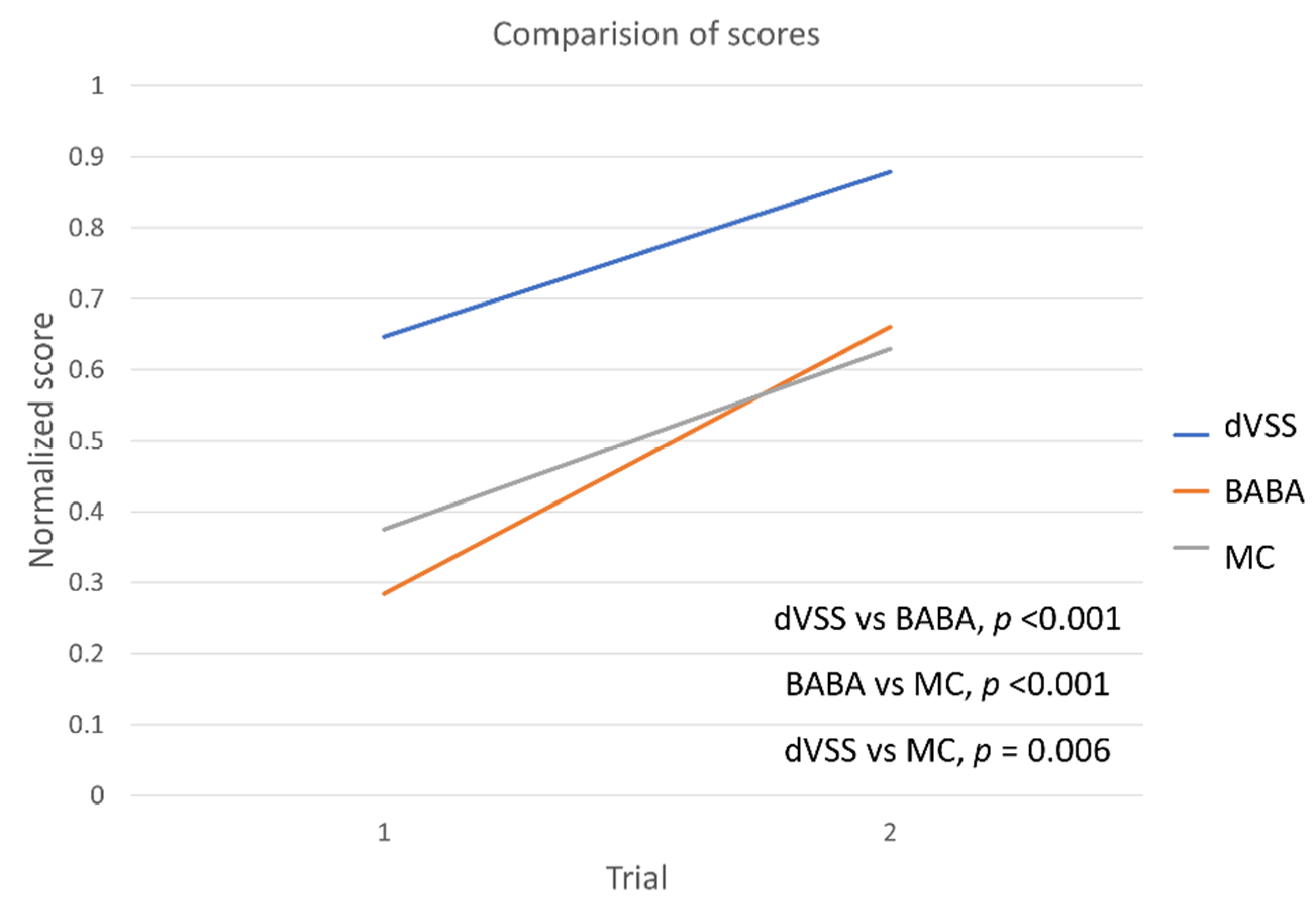
3.1. Comparison of Scores for dVSS, BABA, and MC Scores
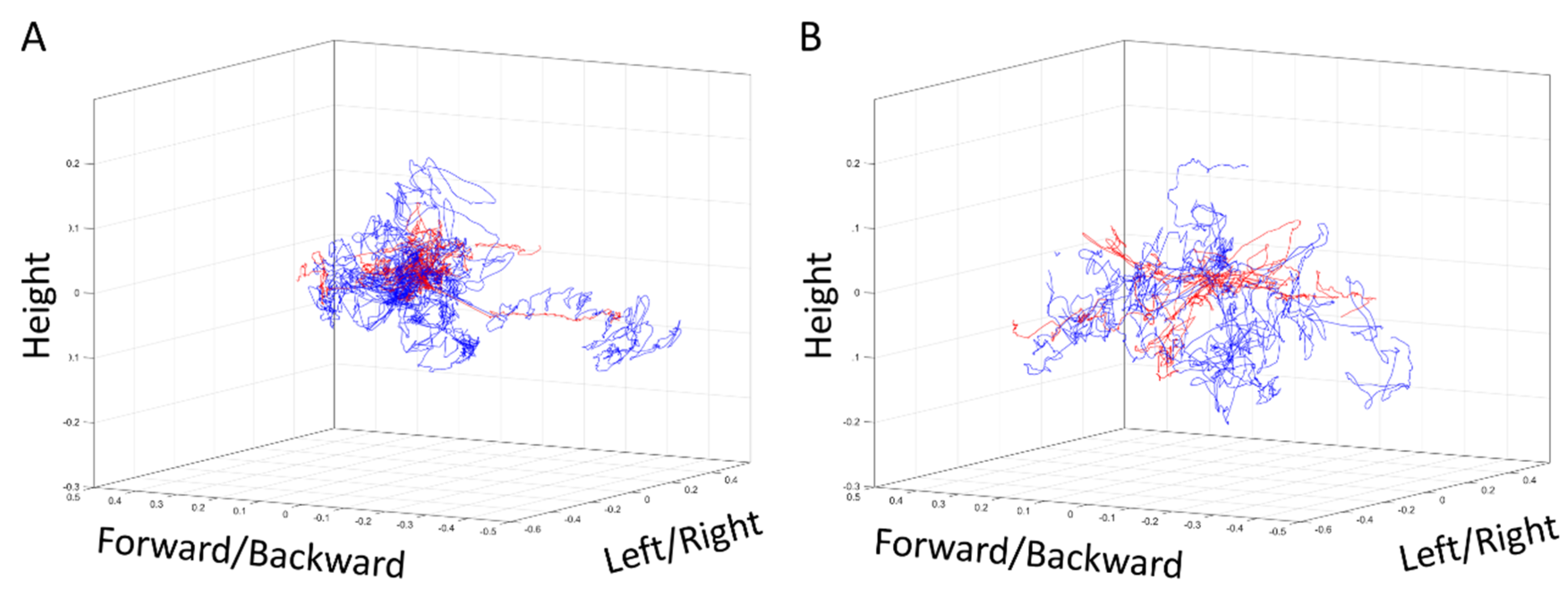
3.2. Differences in Actual Body Movements between Low and High Scores
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Evgeniou, E.; Loizou, P. Simulation-based surgical education. ANZ J. Surg. 2013, 83, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Sedlack, R.E.; Cook, D.A. Effects of simulation-based training in gastrointestinal endoscopy: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 1611–1623. [Google Scholar] [CrossRef] [PubMed]
- Kneebone, R.L. Practice, rehearsal, and performance: An approach for simulation-based surgical and procedure training. JAMA 2009, 302, 1336–1338. [Google Scholar] [CrossRef] [PubMed]
- Jiam, N.T.; Cooper, M.A.; Lyu, H.G.; Hirose, K.; Makary, M.A. Surgical malpractice claims in the United States. J. Healthc. Risk Manag. 2014, 33, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.A.; Choudhry, A.J.; Ray-Zack, M.D.; Lindor, R.A.; Bergquist, J.R.; Habermann, E.B.; Zielinski, M.D. Medical Malpractice Lawsuits Involving Surgical Residents. JAMA Surg. 2017, 153, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Kainer, F. Simulation-based training in obstetrics. Arch. Gynecol. Obstet. 2014, 289, 703–704. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Aydin, A.; Khan, M.S.; Dasgupta, P.; Ahmed, K. Simulation-based training for prostate surgery. BJU Int. 2014, 116, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Bjerrum, F.; Strandbygaard, J.; Rosthøj, S.; Grantcharov, T.; Ottesen, B.; Sorensen, J.L. Evaluation of Procedural Simulation as a Training and Assessment Tool in General Surgery—Simulating a Laparoscopic Appendectomy. J. Surg. Educ. 2016, 74, 243–250. [Google Scholar] [CrossRef]
- Kordowicz, A.G.; Gough, M.J. The challenges of implementing a simulation-based surgical training curriculum. Br. J. Surg. 2014, 101, 441–443. [Google Scholar] [CrossRef]
- Kiely, D.J.; Gotlieb, W.H.; Lau, S.; Zeng, X.; Samouelian, V.; Ramanakumar, A.V.; Zakrzewski, H.; Brin, S.; Fraser, S.A.; Korsieporn, P.; et al. Virtual reality robotic surgery simulation curriculum to teach robotic suturing: A randomized controlled trial. J. Robot. Surg. 2015, 9, 179–186. [Google Scholar] [CrossRef]
- De Win, G.; Van Bruwaene, S.; Kulkarni, J.; Van Calster, B.; Aggarwal, R.; Allen, C.; Lissens, A.; De Ridder, D.; Miserez, M. An evidence based laparoscopic simulation curriculum shortens the clinical learning curve and reduces surgical adverse events. Adv. Med. Educ. Pract. 2016, 7, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Gravante, G.; Venditti, D. A systematic review on low-cost box models to achieve basic and advanced laparoscopic skills during modern surgical training. Surg. Laparosc. Endosc. Percutan. Tech. 2013, 23, 109–120. [Google Scholar] [CrossRef] [PubMed]
- Bareeq, R.A.; Jayaraman, S.; Kiaii, B.; Schlachta, C.; Denstedt, J.D.; Pautler, S.E. The role of surgical simulation and the learning curve in robot-assisted surgery. J. Robot. Surg. 2008, 2, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Farcas, M.A.; Trudeau, M.O.; Nasr, A.; Gerstle, J.T.; Carrillo, B.; Azzie, G. Analysis of motion in laparoscopy: The deconstruction of an intra-corporeal suturing task. Surg. Endosc. 2017, 31, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Takayasu, K.; Yoshida, K.; Mishima, T.; Watanabe, M.; Matsuda, T.; Kinoshita, H. Analysis of the posture pattern during robotic simulator tasks using an optical motion capture system. Surg. Endosc. 2018, 32, 183–190. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.E.; Kim, E.; Koo, D.H.; Choi, J.Y.; Kim, K.H.; Youn, Y.K. Robotic thyroidectomy by bilateral axillo-breast approach: Review of 1026 cases and surgical completeness. Surg. Endosc. 2013, 27, 2955–2962. [Google Scholar] [CrossRef]
- Yu, H.W.; Yi, J.W.; Seong, C.Y.; Kim, J.K.; Bae, I.E.; Kwon, H.; Chai, Y.J.; Kim, S.J.; Choi, J.Y.; Lee, K.E. Development of a surgical training model for bilateral axillo-breast approach robotic thyroidectomy. Surg. Endosc. 2018, 32, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Walliczek, U.; Förtsch, A.; Dworschak, P.; Teymoortash, A.; Mandapathil, M.; Werner, J.; Güldner, C. Effect of training frequency on the learning curve on the da Vinci Skills Simulator. Head Neck 2016, 38 (Suppl. 1), E1762–E1769. [Google Scholar] [CrossRef]
- Jimbo, T.; Ieiri, S.; Obata, S.; Uemura, M.; Souzaki, R.; Matsuoka, N.; Katayama, T.; Masumoto, K.; Hashizume, M.; Taguchi, T. A new innovative laparoscopic fundoplication training simulator with a surgical skill validation system. Surg. Endosc. 2017, 31, 1688–1696. [Google Scholar] [CrossRef]
- Tergas, A.I.; Sheth, S.B.; Green, I.C.; Giuntoli, R.L.; Winder, A.D.; Fader, A.N. A pilot study of surgical training using a virtual robotic surgery simulator. JSLS 2013, 17, 219–226. [Google Scholar] [CrossRef]
- Brown, K.; Mosley, N.; Tierney, J. Battle of the bots: A comparison of the standard da Vinci and the da Vinci Surgical Skills Simulator in surgical skills acquisition. J. Robot. Surg. 2017, 11, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Supe, A.; Dalvi, A.; Prabhu, R.; Kantharia, C.; Bhuiyan, P. Cadaver as a model for laparoscopic training. Indian J. Gastroenterol. 2005, 24, 111–113. [Google Scholar] [PubMed]
- Pérez-Duarte, F.J.; Lucas-Hernández, M.; Matos-Azevedo, A.; Sánchez-Margallo, J.A.; Díaz-Güemes, I.; Sánchez-Margallo, F.M. Objective analysis of surgeons’ ergonomy during laparoendoscopic single-site surgery through the use of surface electromyography and a motion capture data glove. Surg. Endosc. 2014, 28, 1314–1320. [Google Scholar] [CrossRef] [PubMed]
- Bae, D.S.; Suh, B.J.; Park, J.K.; Koo, D.H. Technical, Oncological, and Functional Safety of Bilateral Axillo-Breast Approach ( BABA ) Robotic Total Thyroidectomy. Surg. Laparosc. Endosc. Percutan. Tech. 2016, 26, 253–258. [Google Scholar] [CrossRef]
- Lee, K.E.; Koo, D.H.; Im, H.J.; Park, S.K.; Choi, J.Y.; Paeng, J.C.; Chung, J.K.; Oh, S.K.; Youn, Y.K. Surgical completeness of bilateral axillo-breast approach robotic thyroidectomy: Comparison with conventional open thyroidectomy after propensity score matching. Surgery 2011, 150, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- Chai, Y.J.; Suh, H.; Woo, J.W.; Yu, H.W.; Song, R.Y.; Kwon, H.; Lee, K.E. Surgical safety and oncological completeness of robotic thyroidectomy for thyroid carcinoma larger than 2 cm. Surg. Endosc. 2017, 31, 1235–1240. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.W.; Jung, J.H.; Park, H.Y. The Learning Curve for Robotic Thyroidectomy Using a Bilateral Axillo-Breast Approach From the 100 Cases. Surg. Laparosc. Endosc. Percutan. Tech. 2015, 25, 412–416. [Google Scholar] [CrossRef]
- Yu, D.; Dural, C.; Morrow, M.M.; Yang, L.; Collins, J.W.; Hallbeck, S.; Kjellman, M.; Forsman, M. Intraoperative workload in robotic surgery assessed by wearable motion tracking sensors and questionnaires. Surg. Endosc. 2017, 31, 877–886. [Google Scholar] [CrossRef]
- Gritsenko, V.; Dailey, E.; Kyle, N.; Taylor, M.; Whittacre, S.; Swisher, A.K. Feasibility of using low-cost motion capture for automated screening of shoulder motion limitation after breast cancer surgery. PLoS ONE 2015, 10, e0128809. [Google Scholar] [CrossRef]
- Wijewickrema, S.; Copson, B.; Zhou, Y.; Ma, X.; Briggs, R.; Bailey, J.; Kennedy, G.; O’Leary, S. Design and Evaluation of a Virtual Reality Simulation Module for Training Advanced Temporal Bone Surgery. In Proceedings of the 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22 June 2017; pp. 7–12. [Google Scholar] [CrossRef]
- Ma, X.; Wijewickrema, S.; Zhou, Y.; Zhou, S.; O’Leary, S.; Bailey, J. Providing Effective Real-time Feedback in Simulation-based Surgical Training. MICCAI 2017, 566–574. [Google Scholar] [CrossRef]
- Ma, X.; Wijewickrema, S.; Zhou, Y.; Copson, B.; Bailey, J.; Kennedy, G.; O’Leary, S. Simulation for Training Cochlear Implant Electrode Insertion. In Proceedings of the 2017 IEEE 30th International Symposium on Computer-Based Medical Systems (CBMS), Thessaloniki, Greece, 22 June 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Lee, D.; Yi, J.W.; Hong, J.; Chai, Y.J.; Kim, H.C.; Kong, H.-J. Augmented Reality to Localize Individual Organ in Surgical Procedure. Healthc Inform Res. 2018, 24, 394–401. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | BABA Score | MC Score | dVSS Score | |||
|---|---|---|---|---|---|---|
| First Cycle | Second Cycle | First Cycle | Second Cycle | First Cycle | Second Cycle | |
| 1 | 26 | 35 | 39.3 | 85.7 | 80 | 91 |
| 2 | 18 | 36 | 33.0 | 89.9 | 57 | 82 |
| 3 | 19 | 23 | 69.8 | 39.3 | 64 | 73 |
| 4 | 15 | 32 | 28.9 | 60.0 | 62 | 87 |
| 5 | 20 | 28 | 45.2 | 56.8 | 64 | 84 |
| 6 | 11 | 18 | 16.4 | 20.3 | 1 | 55 |
| 7 | 20 | 24 | 58.8 | 77.7 | 56 | 89 |
| 8 | 13 | 25 | 35.3 | 52.6 | 61 | 80 |
| 9 | 17 | 25 | 55.6 | 64.7 | 80 | 89 |
| 10 | 22 | 29 | 57.5 | 79.6 | 67 | 71 |
| Average | 18.1 ± 4.4 | 27.5 ± 5.6 | 44.0 ± 16.4 | 62.7 ± 21.8 | 59.2 ± 22.1 | 80.1 ± 11.1 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.S.; Hong, N.; Kim, M.; Yoon, S.G.; Yu, H.W.; Kong, H.-J.; Kim, S.-J.; Chai, Y.J.; Choi, H.J.; Choi, J.Y.; et al. Application of a Perception Neuron® System in Simulation-Based Surgical Training. J. Clin. Med. 2019, 8, 124. https://doi.org/10.3390/jcm8010124
Kim HS, Hong N, Kim M, Yoon SG, Yu HW, Kong H-J, Kim S-J, Chai YJ, Choi HJ, Choi JY, et al. Application of a Perception Neuron® System in Simulation-Based Surgical Training. Journal of Clinical Medicine. 2019; 8(1):124. https://doi.org/10.3390/jcm8010124
Chicago/Turabian StyleKim, Hyun Soo, Nhayoung Hong, Myungjoon Kim, Sang Gab Yoon, Hyeong Won Yu, Hyoun-Joong Kong, Su-Jin Kim, Young Jun Chai, Hyung Jin Choi, June Young Choi, and et al. 2019. "Application of a Perception Neuron® System in Simulation-Based Surgical Training" Journal of Clinical Medicine 8, no. 1: 124. https://doi.org/10.3390/jcm8010124