Acute Respiratory Tract Infection and 25-Hydroxyvitamin D Concentration: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search and Screening Strategy
2.2. Inclusion/Exclusion Criteria
2.3. Definition of Outcome
2.4. Quality Assessment
2.5. Statistical Analysis Methods
- A measure of association between 25(OH)D concentration and ARTI risk or severity (odds ratio (OR), relative risk (RR), hazard ratio (HR), mean difference (MD)) and their 95% confidence interval (CI) or standard deviation (SD); or
- Sufficient data to derive two by two tables of ARTI risk, comparing the lowest versus the highest 25(OH)D category.
2.6. Assessment of Heterogeneity and Publication Bias
3. Results
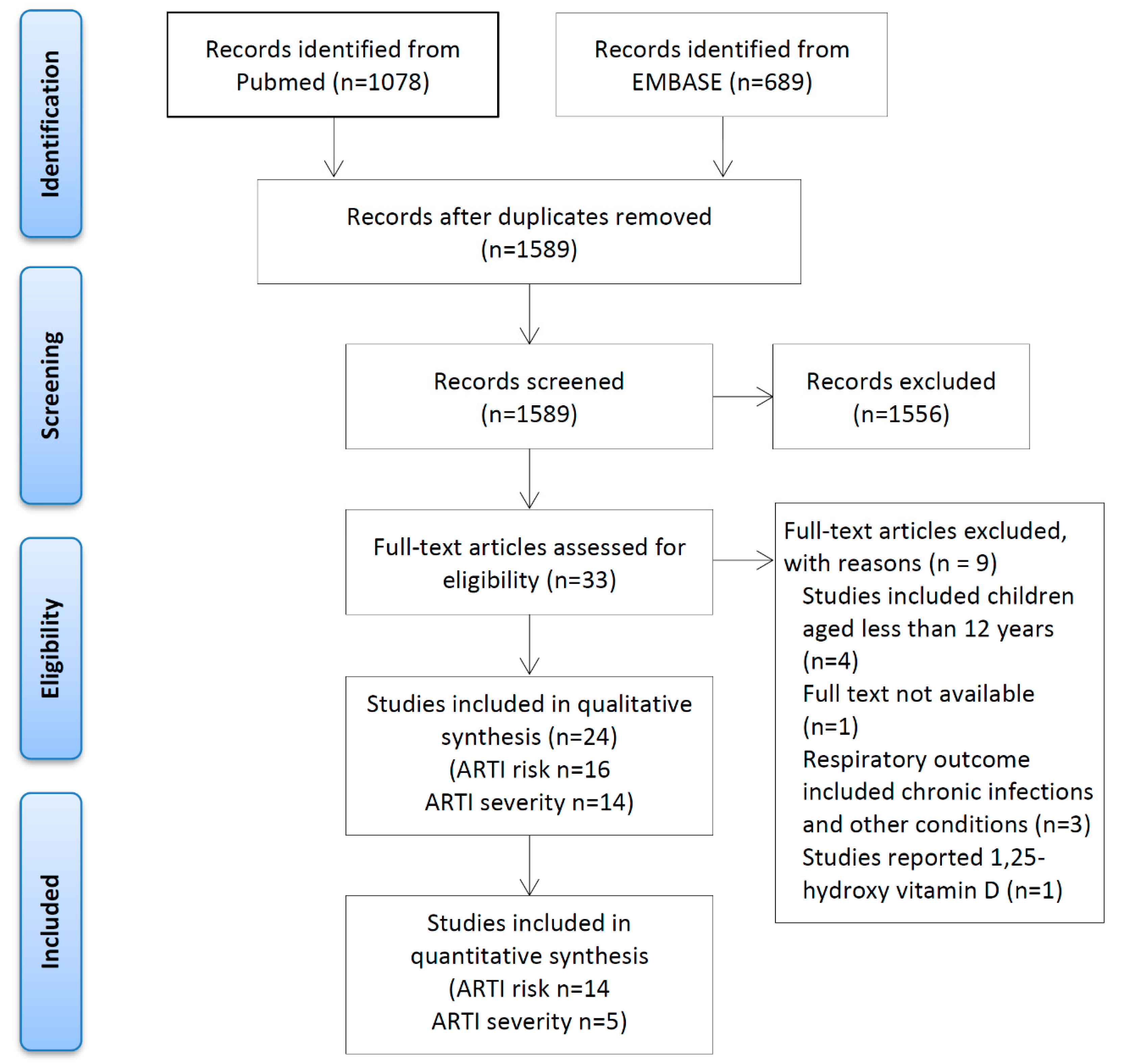
3.1. Identification and Selection of Studies
3.2. Study Characteristics
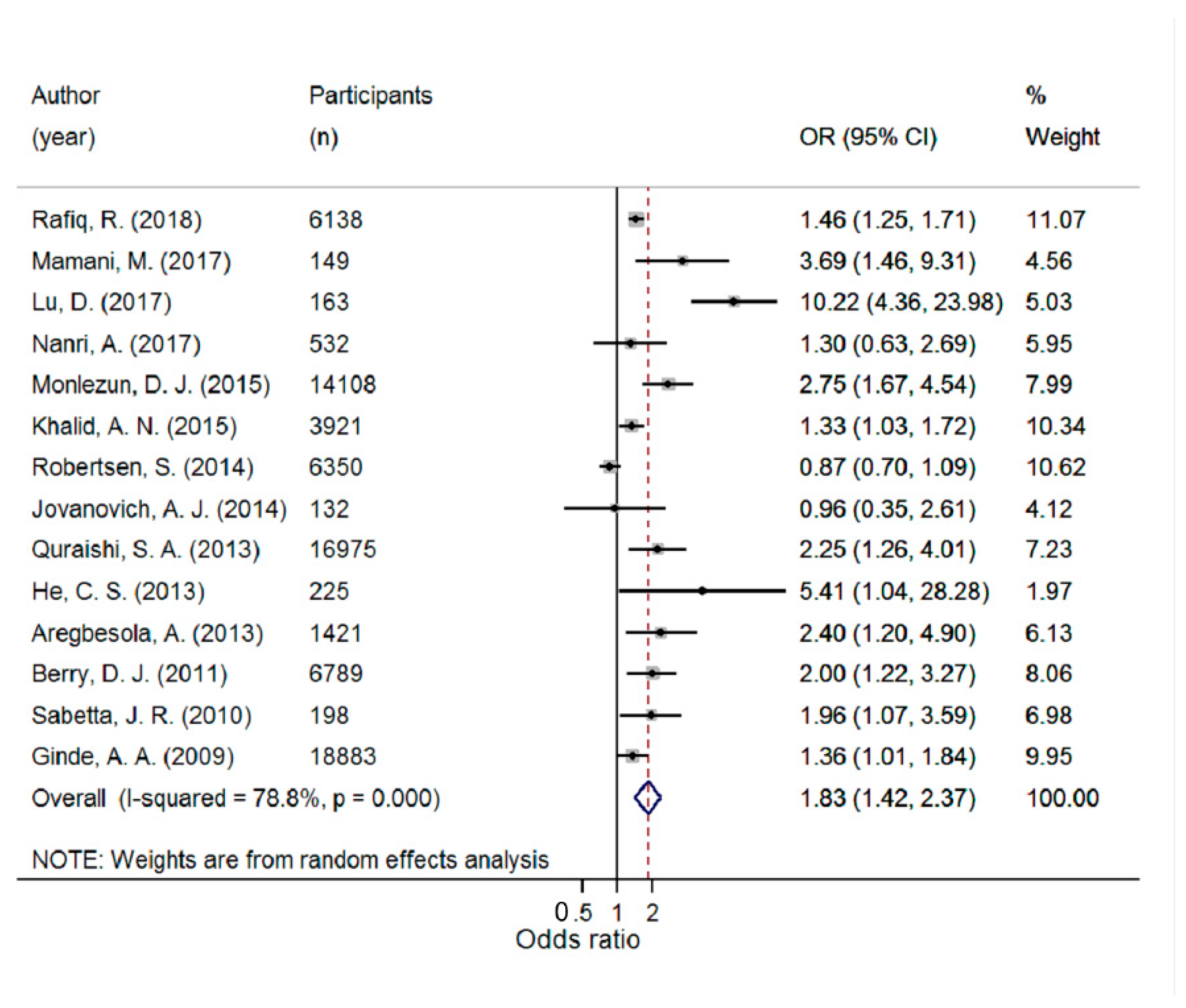
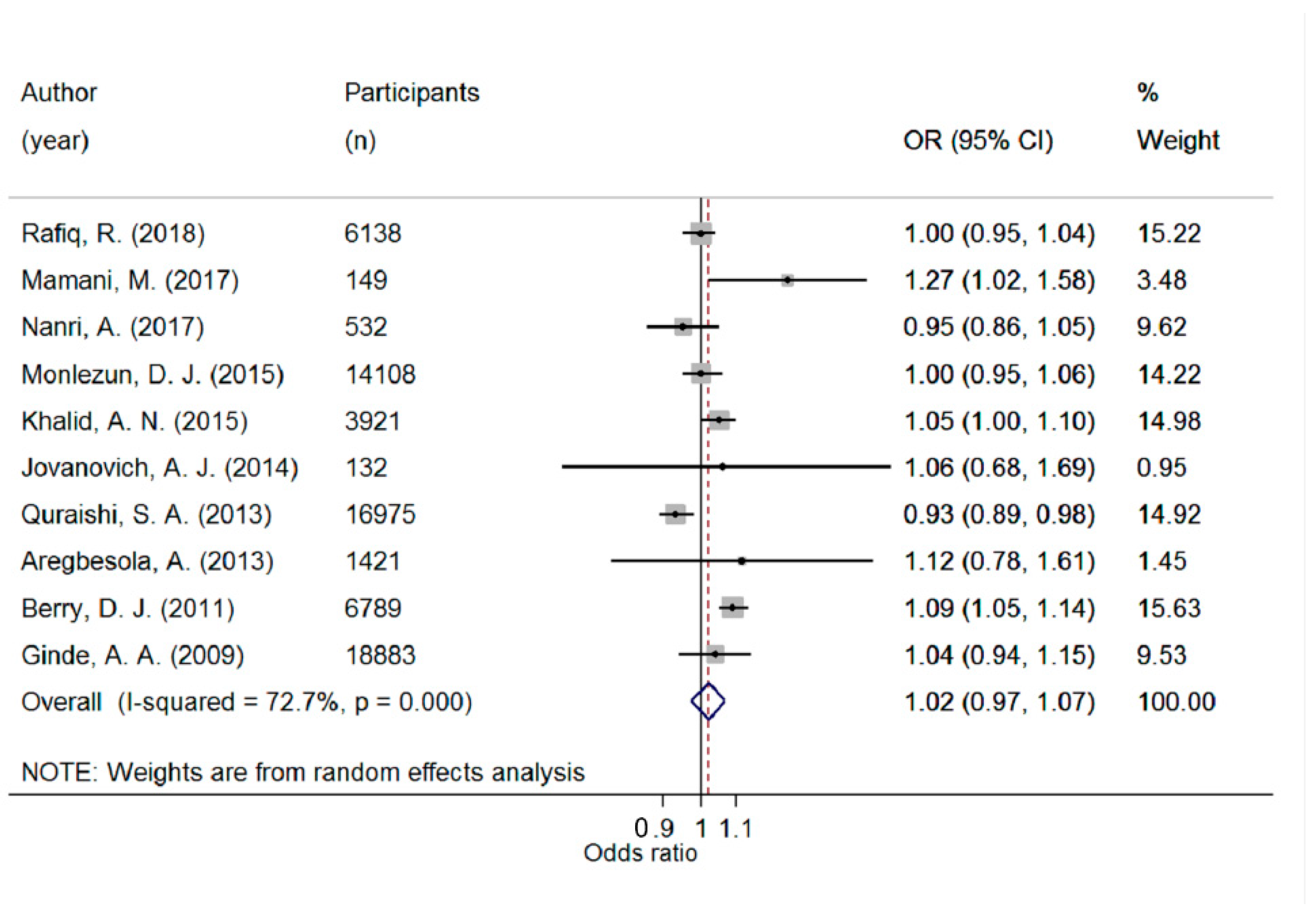
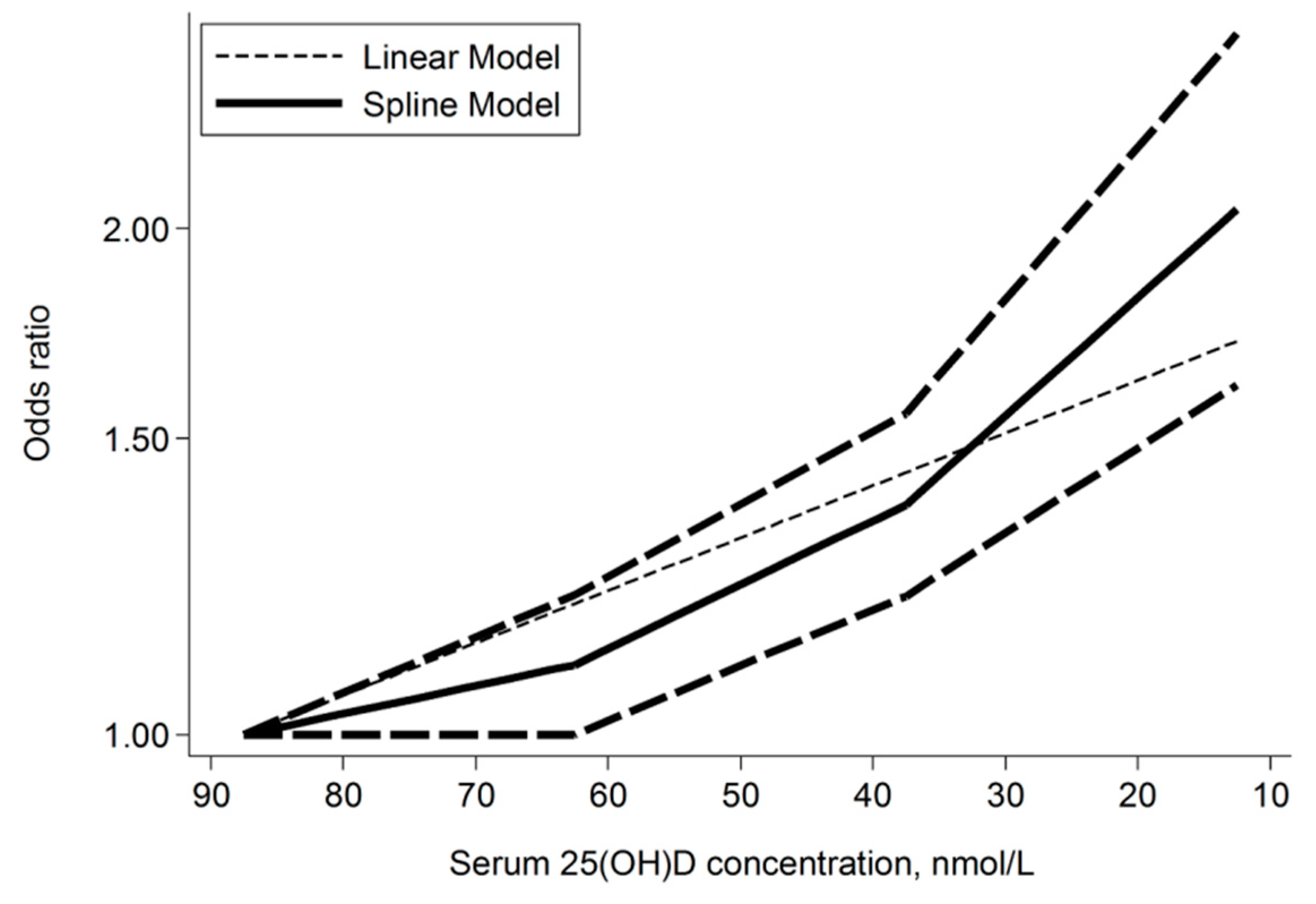
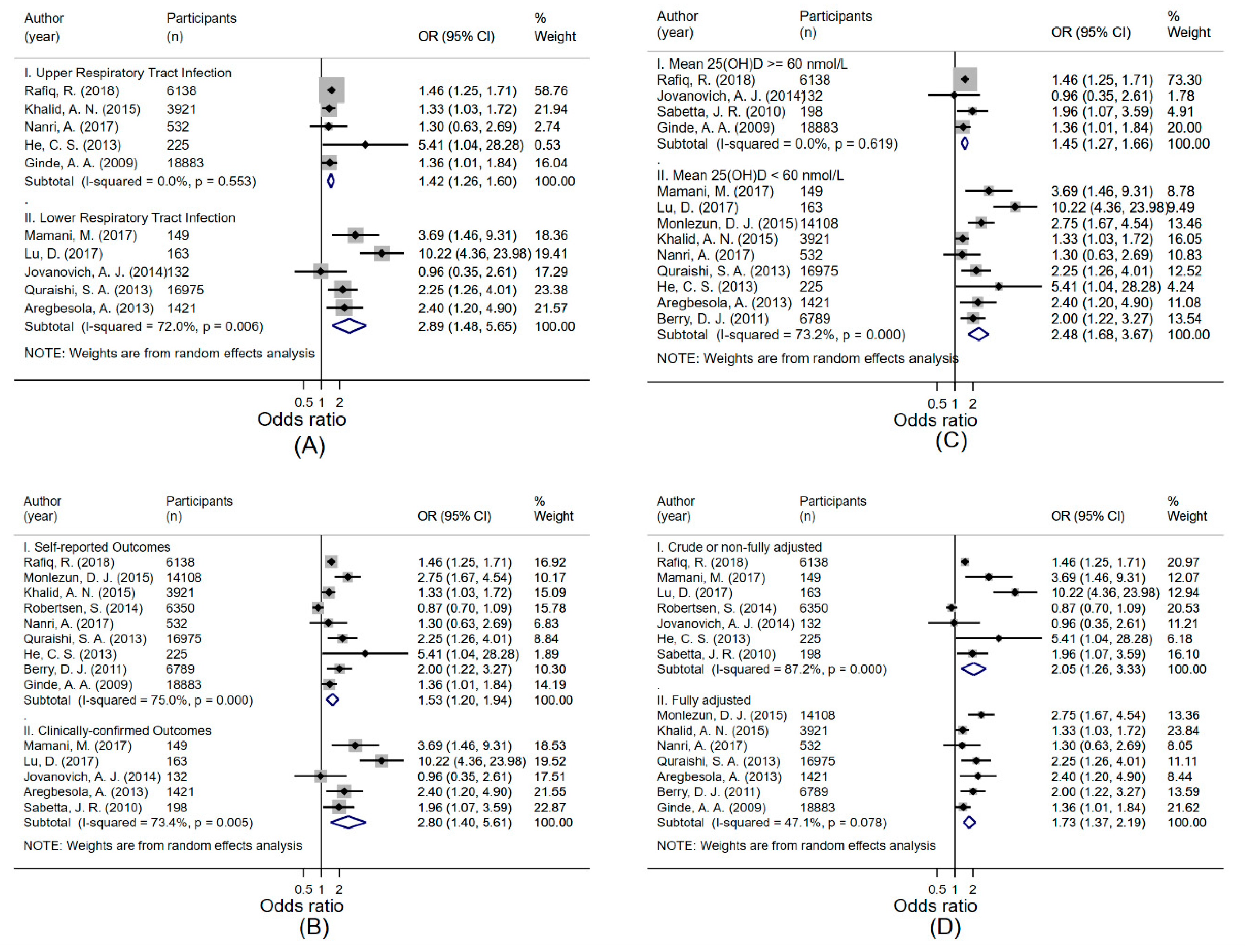
3.3. Association between 25(OH)D Concentration and Risk of ARTI
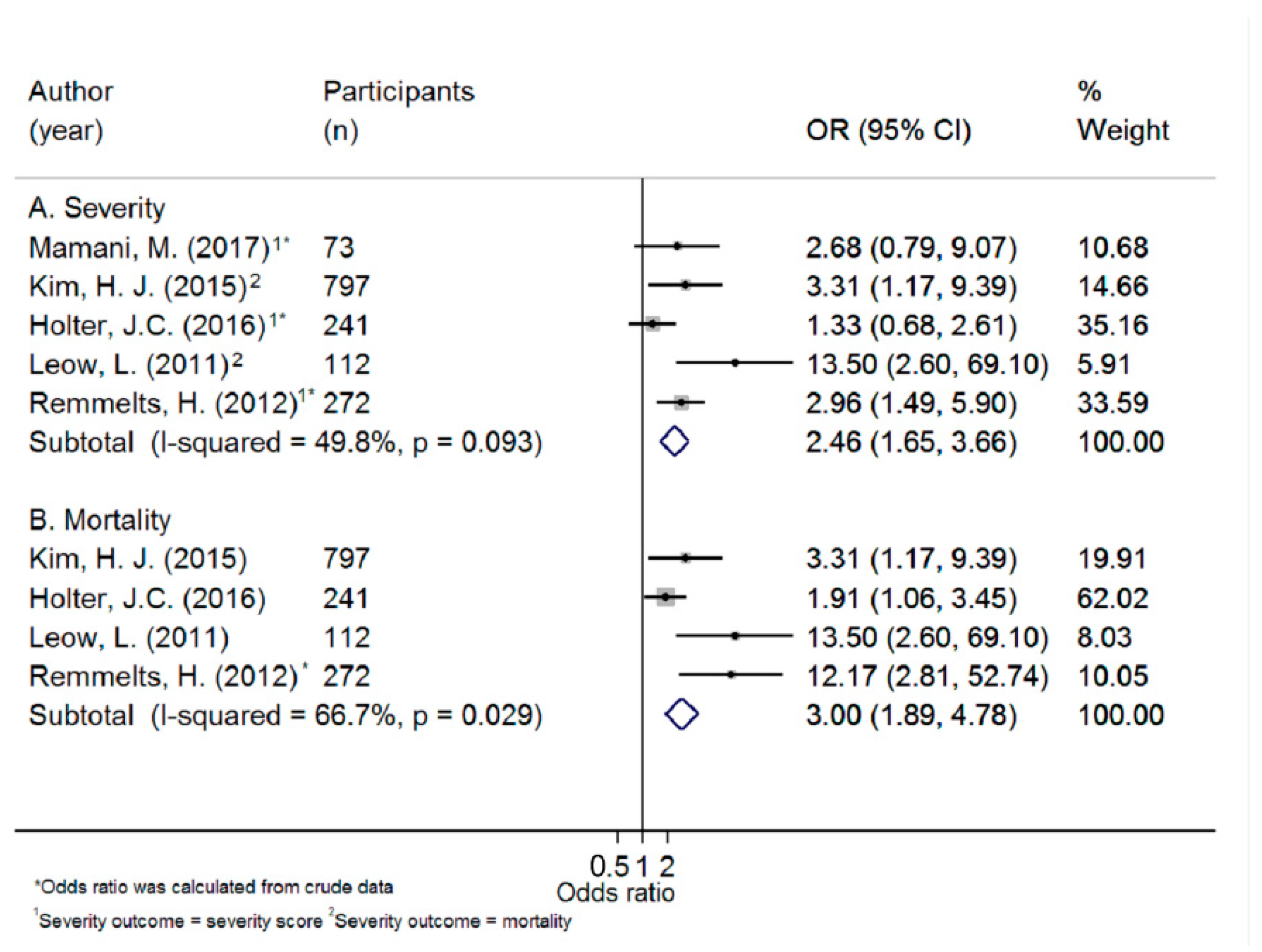
3.4. Association between 25(OH)D Concentration and Severity of ARTI
3.5. Studies Excluded from the Meta-Analysis
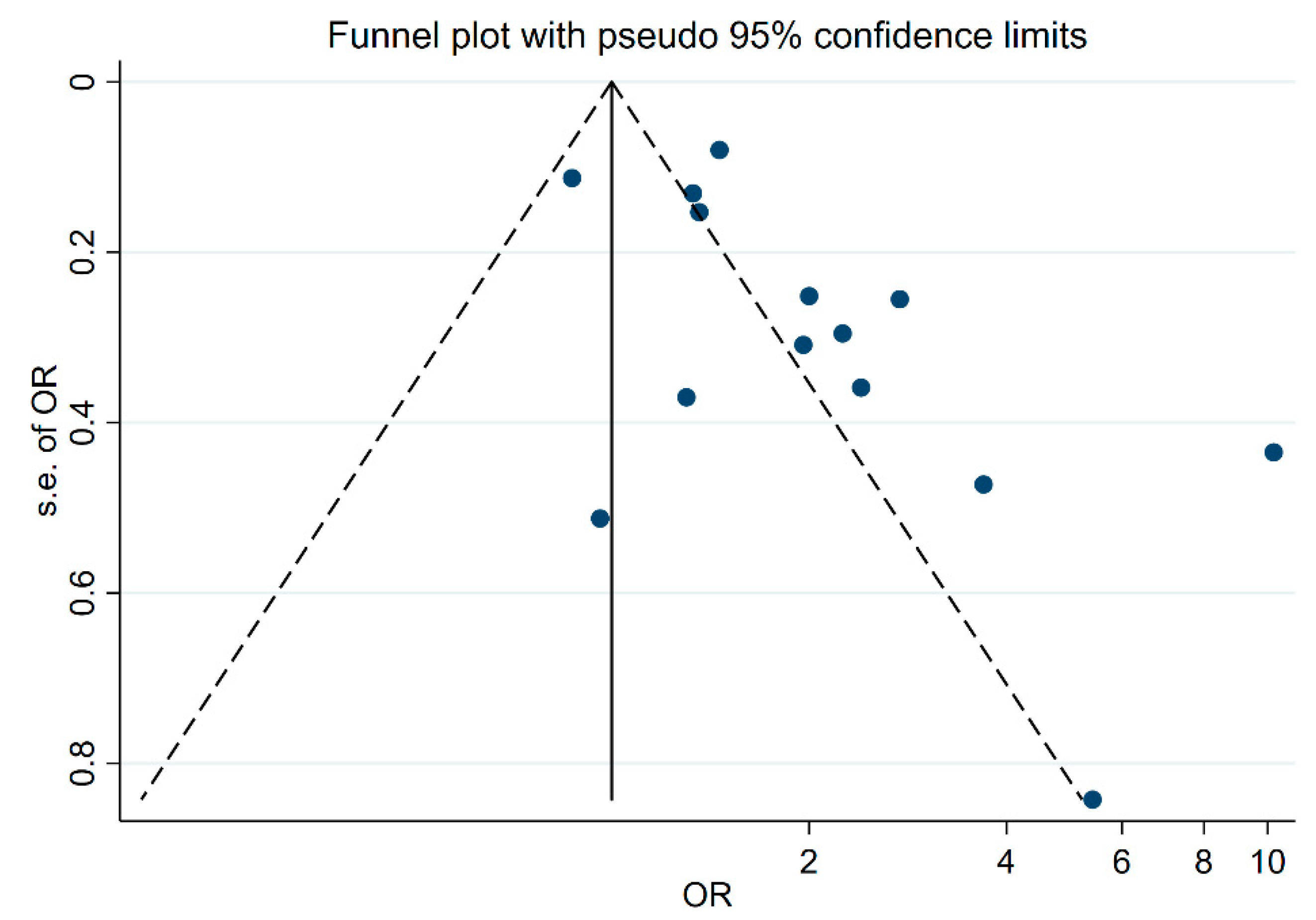
3.6. Subgroup Analysis and Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Heikkinen, T.; Jarvinen, A. The common cold. Lancet 2003, 361, 51–59. [Google Scholar] [CrossRef]
- WHO. Review of global influenza activity, October 2016–October 2017. Wkly. Epidemiol. Rec. 2017, 92, 761–779. [Google Scholar]
- LRICollaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef]
- Australian Government, Department of Health. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/ozflu-surveil-2017-final.htm#current (accessed on 26 April 2019).
- Telcian, A.G.; Zdrenghea, M.T.; Edwards, M.R.; Laza-Stanca, V.; Mallia, P.; Johnston, S.L.; Stanciu, L.A. Vitamin D increases the antiviral activity of bronchial epithelial cells in vitro. Antivir. Res. 2017, 137, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Zdrenghea, M.T.; Makrinioti, H.; Bagacean, C.; Bush, A.; Johnston, S.L.; Stanciu, L.A. Vitamin D modulation of innate immune responses to respiratory viral infections. Rev. Med. Virol. 2017, 27. [Google Scholar] [CrossRef]
- Assa, A.; Vong, L.; Pinnell, L.J.; Avitzur, N.; Johnson-Henry, K.C.; Sherman, P.M. Vitamin D deficiency promotes epithelial barrier dysfunction and intestinal inflammation. J. Infect. Dis 2014, 210, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Bartley, J. Vitamin D, innate immunity and upper respiratory tract infection. J. Laryngol. Otol. 2010, 124, 465–469. [Google Scholar] [CrossRef]
- Jat, K.R. Vitamin D deficiency and lower respiratory tract infections in children: A systematic review and meta-analysis of observational studies. Trop. Doct. 2017, 47, 77–84. [Google Scholar] [CrossRef] [PubMed]
- García-Marcos, L.; Morales, E.; Pacheco-Gonzalez, R.M. Prenatal vitamin D status and respiratory and allergic outcomes in childhood: A meta-analysis of observational studies. Pediatr. Allergy Immunol. 2018, 29, 243–253. [Google Scholar]
- Furlong, K.; Omand, J.; Pitino, M.; Science, M.; O’Connor, D.; Maguire, J.; Tran, D. Vitamin D Status and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Observational Evidence. FASEB J. 2015, 29, 252–255. [Google Scholar]
- Jolliffe, D.A.; Griffiths, C.J.; Martineau, A.R. Vitamin D in the prevention of acute respiratory infection: Systematic review of clinical studies. J. Steroid Biochem. Mol. Boil. 2013, 136, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Zhang, J.; Ma, C.; Yue, Y.; Zou, Z.; Yu, C.; Yin, F. Link between community-acquired pneumonia and vitamin D levels in older patients. Z. Gerontol. Geriatr. 2017, 51, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Pletz, M.W.; Terkamp, C.; Schumacher, U.; Rohde, G.; Schütte, H.; Welte, T.; Bals, R. Vitamin D deficiency in community-acquired pneumonia: Low levels of 1,25(OH)2 D are associated with disease severity. Respir. Res. 2014, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- He, C.-S.; Handzlik, M.; Fraser, W.D.; Muhamad, A.; Preston, H.; Richardson, A.; Gleeson, M. Influence of vitamin D status on respiratory infection incidence and immune function during 4 months of winter training in endurance sport athletes. Exerc. Immunol. Rev. 2013, 19, 86–101. [Google Scholar] [PubMed]
- Laaksi, I.; Ruohola, J.-P.; Tuohimaa, P.; Auvinen, A.; Haataja, R.; Pihlajamäki, H.; Ylikomi, T. An association of serum vitamin D concentrations < 40 nmol/L with acute respiratory tract infection in young Finnish men. Am. J. Clin. Nutr. 2007, 86, 714–717. [Google Scholar] [PubMed]
- Bergman, P.; Lindh, A.U.; Björkhem-Bergman, L.; Lindh, J.D. Vitamin D and Respiratory Tract Infections: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2013, 8, e65835. [Google Scholar] [CrossRef] [PubMed]
- Charan, J.; Goyal, J.P.; Saxena, D.; Yadav, P. Vitamin D for prevention of respiratory tract infections: A systematic review and meta-analysis. J. Pharmacol. Pharm. 2012, 3, 300–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, S.; Huang, S. Vitamin D supplementation and risk of respiratory tract infections: A meta-analysis of randomized controlled trials. Scand. J. Infect. Dis. 2013, 45, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Gysin, D.V.; Dao, D.; Lytvyn, L.; Loeb, M. Effect of Vitamin D3 Supplementation on Respiratory Tract Infections in Healthy Individuals: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2016, 11, 0162996. [Google Scholar]
- Xiao, L.; Xing, C.; Yang, Z.; Xu, S.; Wang, M.; Du, H.; Liu, K.; Huang, Z. Vitamin D supplementation for the prevention of childhood acute respiratory infections: A systematic review of randomised controlled trials. Br. J. Nutr. 2015, 114, 1026–1034. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Dubnov-Raz, G.; Esposito, S.; Ganmaa, D.; Ginde, A.A.; et al. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef]
- PROSPERO. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=94987/ (accessed on 1 May 2019).
- Wells, G.; Shea, B.J.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Non-Randomized Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 16 July 2019).
- Aregbesola, A.; Voutilainen, S.; Nurmi, T.; Virtanen, J.; Ronkainen, K.; Tuomainen, T.-P. Serum 25-hydroxyvitamin D3 and the risk of pneumonia in an ageing general population. J. Epidemiol. Commun. Heal. 2013, 67, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Sabetta, J.R.; DePetrillo, P.; Cipriani, R.J.; Smardin, J.; Burns, L.A.; Landry, M.L. Serum 25-Hydroxyvitamin D and the Incidence of Acute Viral Respiratory Tract Infections in Healthy Adults. PLoS ONE 2010, 5, e11088. [Google Scholar] [CrossRef] [PubMed]
- Greenland, S.; Longnecker, M.P. Methods for Trend Estimation from Summarized Dose-Response Data, with Applications to Meta-Analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized Least Squares for Trend Estimation of Summarized Dose–response Data. Stata J. Promot. Commun. Stat. Stata 2006, 6, 40–57. [Google Scholar] [CrossRef]
- Ginde, A.A.; Mansbach, J.M.; Camargo, C.A. Association between serum 25-hydroxyvitamin D level and upper respiratory tract infection in the Third National Health and Nutrition Examination Survey. Arch. Intern. Med. 2009, 169, 384–390. [Google Scholar] [CrossRef]
- Touvier, M.; Chan, D.S.; Lau, R.; Aune, D.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Riboli, E.; Hercberg, S.; Norat, T. Meta-Analyses of Vitamin D Intake, 25-Hydroxyvitamin D Status, Vitamin D Receptor Polymorphisms, and Colorectal Cancer Risk. Cancer Epidemiol. Biomark. Prev. 2011, 20, 1003–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, D.J.; Hesketh, K.; Power, C.; Hyppönen, E. Vitamin D status has a linear association with seasonal infections and lung function in British adults. Br. J. Nutr. 2011, 106, 1433–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jovanovich, A.J.; Ginde, A.A.; Holmen, J.; Jablonski, K.; Allyn, R.L.; Kendrick, J.; Chonchol, M. Vitamin D Level and Risk of Community-Acquired Pneumonia and Sepsis. Nutrients 2014, 6, 2196–2205. [Google Scholar] [CrossRef] [Green Version]
- Khalid, A.N.; Ladha, K.S.; Luong, A.U.; Quraishi, S.A. Association of Vitamin D Status and Acute Rhinosinusitis: Results From the United States National Health and Nutrition Examination Survey 2001–2006. Medicine 2015, 94, e1447. [Google Scholar] [CrossRef]
- Monlezun, D.J.; Bittner, E.A.; Christopher, K.B.; Camargo, C.A.; Quraishi, S.A. Vitamin D Status and Acute Respiratory Infection: Cross Sectional Results from the United States National Health and Nutrition Examination Survey, 2001–2006. Nutrients 2015, 7, 1933–1944. [Google Scholar] [CrossRef] [PubMed]
- Nanri, A.; Nakamoto, K.; Sakamoto, N.; Imai, T.; Akter, S.; Nonaka, D.; Mizoue, T. Association of serum 25-hydroxyvitamin D with influenza in case-control study nested in a cohort of Japanese employees. Clin. Nutr. 2017, 36, 1288–1293. [Google Scholar] [CrossRef] [PubMed]
- Porojnicu, A.C.; Moroti-Constantinescu, R.; Laslau, A.; Lagunova, Z.; Dahlback, A.; Hristea, A.; Moan, J. Vitamin D status in healthy Romanian caregivers and risk of respiratory infections. Public Heal. Nutr. 2012, 15, 2157–2162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quraishi, S.A.; Bittner, E.A.; Christopher, K.B.; Camargo, C.A. Vitamin D Status and Community-Acquired Pneumonia: Results from the Third National Health and Nutrition Examination Survey. PLoS ONE 2013, 8, e81120. [Google Scholar] [CrossRef] [PubMed]
- Rafiq, R.; Thijs, W.; Prein, R.; De Jongh, R.T.; Taube, C.; Hiemstra, P.S.; De Mutsert, R.; Heijer, M.D. Associations of Serum 25(OH)D Concentrations with Lung Function, Airway Inflammation and Common Cold in the General Population. Nutrients 2018, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Brance, M.L.; Miljevic, J.N.; Tizziani, R.; Taberna, M.E.; Grossi, G.P.; Toni, P.; Valentini, E.; Trepat, A.; Zaccardi, J.; Moro, J.; et al. Serum 25-hydroxyvitamin D levels in hospitalized adults with community-acquired pneumonia. J. Bone Min. Res. 2017, 32, S258. [Google Scholar] [CrossRef] [PubMed]
- Holter, J.C.; Ueland, T.; Norseth, J.; Brunborg, C.; Frøland, S.S.; Husebye, E.; Aukrust, P.; Heggelund, L. Vitamin D Status and Long-Term Mortality in Community-Acquired Pneumonia: Secondary Data Analysis from a Prospective Cohort. PLoS ONE 2016, 11, e0158536. [Google Scholar] [CrossRef]
- Kim, H.J.; Jang, J.G.; Hong, K.S.; Park, J.-K.; Choi, E.-Y. Relationship between serum vitamin D concentrations and clinical outcome of community-acquired pneumonia. Int. J. Tuberc. Lung Dis. 2015, 19, 729–734. [Google Scholar] [CrossRef]
- Leow, L.; Simpson, T.; Cursons, R.; Karalus, N.; Hancox, R.J. Vitamin D, innate immunity and outcomes in community acquired pneumonia. Respirology (Carlton Vic.) 2011, 16, 611–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remmelts, H.; van de Garde, E.; Meijvis, S.; Peelen, E.; Damoiseaux, J.; Grutters, J.; Biesma, D.; Bos, W.J.; Rijkers, G. Vitamin D level predicts clinical outcome in community-acquired pneumonia. Eur. Respir. J. 2012, 40, 1361. [Google Scholar]
- Yaghoobi, M.H.; Taher, A.; Seifrabie, M.A.; Sabahi, M.; Rahimi-Bashar, F. Serum vitamin D level was not associated with severity of ventilator associated pneumonia. Romanian J. Intern. Med. 2019, 57, 55–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamani, M.; Muceli, N.; Basir, H.R.G.; Vasheghani, M.; Poorolajal, J. Association between serum concentration of 25-hydroxyvitamin D and community-acquired pneumonia: A case-control study. Int. J. Gen. Med. 2017, 10, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Robertsen, S.; Grimnes, G.; Melbye, H. Association between serum 25-hydroxyvitamin D concentration and symptoms of respiratory tract infection in a Norwegian population: The Tromso Study. Public Health Nutr. 2014, 17, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Scullion, L.; Baker, D.; Healey, P.; Edwards, A.; Love, T.; Black, K. No Association between Vitamin D and Acute Respiratory Tract Infections Amongst Elite New Zealand Rugby Players and Rowers. Int. J. Vitam. Nutr. Res. 2018, 88, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Blatchford, P.; Breese, K.; Zarrabi, L.; Linnebur, S.A.; Wallace, J.I.; Schwartz, R.S. High-Dose Monthly Vitamin D for Prevention of Acute Respiratory Infection in Older Long-Term Care Residents: A Randomized Clinical Trial. J. Am. Geriatr. Soc. 2017, 65, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Majak, P.; Olszowiec-Chlebna, M.; Smejda, K.; Stelmach, I. Vitamin D supplementation in children may prevent asthma exacerbation triggered by acute respiratory infection. J. Allergy Clin. Immunol. 2011, 127, 1294–1296. [Google Scholar] [CrossRef] [PubMed]
- Urashima, M.; Segawa, T.; Okazaki, M.; Kurihara, M.; Wada, Y.; Ida, H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Am. J. Clin. Nutr. 2010, 91, 1255–1260. [Google Scholar] [CrossRef] [Green Version]
- Jorde, R.; Witham, M.; Janssens, W.; Rolighed, L.; Borchhardt, K.; de Boer, I.H.; Grimnes, G.; Hutchinson MSVitamin, D. Vitamin D supplementation did not prevent influenza-like illness as diagnosed retrospectively by questionnaires in subjects participating in randomized clinical trials. Scand. J. Infect. Dis 2012, 44, 126–132. [Google Scholar] [CrossRef]
- Mattila, V.; Ylikomi, T.; Laaksi, I.; Ruohola, J.-P.; Auvinen, A.; Pihlajamäki, H. Vitamin D supplementation for the prevention of acute respiratory tract infection: A randomized, double-blinded trial among young Finnish men. J. Infect. Dis. 2010, 202, 809–814. [Google Scholar]
- Li-Ng, M.; Aloia, J.F.; Pollack, S.; Cunha, B.A.; Mikhail, M.; Yeh, J.; Berbari, N. A randomized controlled trial of vitamin D3 supplementation for the prevention of symptomatic upper respiratory tract infections. Epidemiol. Infect. 2009, 137, 1396–1404. [Google Scholar] [CrossRef] [PubMed]
- Manaseki-Holland, S.; Maroof, Z.; Bruce, J.; Mughal, M.Z.; Masher, M.I.; Bhutta, Z.A.; Walraven, G.; Chandramohan, D. Effect on the incidence of pneumonia of vitamin D supplementation by quarterly bolus dose to infants in Kabul: A randomised controlled superiority trial. Lancet 2012, 379, 1419–1427. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Publication Year) | Year of Study | Follow-Up Time | Outcome | Participants | Age (Mean ± SD)/Sex (% Female) | Sample Size | Outcome Measurement | Mean (SD)/Median (Q1–Q3) 25(OH)D (nmol/L) | Lowest 25(OH)D Category (nmol/L) | Highest 25(OH)D Category (nmol/L) | 25(OH)D Measurement Method |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case-Control Studies | |||||||||||
| Jovanovich, A. J. (2014) [32] | 2008–2010 | Pneumonia | Cases: patients with CAP Controls: patients without CAP | Age: 60 ± 17 Sex: 71% F | 132 | Laboratory or x-ray confirmed | Cases: 70.1 (62.2–79.6) Controls: 79.3 (71.1–88.1) | 50 | ≥50 | INCSTAR RIA | |
| Nanri, A. (2017) [35] | 2011 | Influenza | Cases: employees with influenza Controls: employees without influenza | Age: 38 ± 12 Sex: 17% F | 532 | Self-reported (past 6 months) | Cases: 56.1 (12.8) Controls: 55.9 (13.0) | 50 | ≥75 | CBP assay | |
| Mamani, M. (2017) [45] | NA | Pneumonia | Cases: patients with CAP Controls: patients’ companions | Age: >18 Sex: 30% F | 149 | Laboratory or x-ray confirmed | Cases: 54.7 (61.9) Controls: 48.1 (27.8) | 25 | >50 | Diarosin CLIA | |
| Cross-Sectional Studies | |||||||||||
| Ginde, A.A. (2009) [29] | 1988–1994 | URTI | NHANES III (1988–1994) | Age: ≥12 Sex: 53% F | 18,883 | Self-reported (past few days) | 72.2 (52.3–92.1) | 25 | ≥75 | Diasorin RIA | |
| Quraishi, S.A. (2013) [37] | 1988–1994 | Pneumonia | NHANES III (1988–1994) | Age: ≥17 Sex: 53% F | 16,975 | Self-reported (past 12 months) | 59.8 (44.8–79.7) | 25 | ≥75 | Diasorin RIA | |
| Khalid, A.N. (2015) [33] | 2001–2006 | Acute rhinosinusitis | NHANES 2001–2006 | Age: ≥17 Sex: 51% F | 3921 | Self-reported (past 24 h) | 54.8 (39.8–69.7) | 50 | ≥50 | Diasorin RIA | |
| Monlezun, D.J. (2015) [34] | 2001–2006 | ARTI | NHANES 2001–2006 | Age: ≥17 Sex: 51% F | 14,108 | Self-reported (past 1 month) | 52.3 (37.4–67.2) | 25 | ≥75 | Diasorin RIA | |
| Berry, D.J. (2011) [31] | 2002–2004 | ARTI | Birth cohort born 1958 | Age: 45 Sex: 50% F | 6789 | Self-reported (past 3 weeks) | 52.2 | 25 | ≥100 | IDS OCTEIA | |
| Robertsen, S. (2014) [46] | 2007–2008 | ARTI | Tromsø population-based study | Age: ≥40 Sex: 57% F | 6350 | Self-reported (past 7 days) | NA | NA | Roche CLIA | ||
| Rafiq, R. (2018) [38] | 2008–2012 | Common cold | NEO study, BMI ≥ 27 kg/m2 | Age: 45–65 Sex: 56% F | 6138 | Self-reported (past 1 month) | 71.3 | 50 | ≥75 | Diasorin RIA, IDS CLIA, Roche CLIA | |
| Lu, D. (2017) [13] | 2011–2012 | Pneumonia | Hospitalised patients | Age: 60–94 Sex: 31% F | 163 | Clinically diagnosed | 30.0 (11.2) | 25 | ≥25 | IDS ELISA | |
| Scullion, L. (2018) [47] | NA | ARTI | Elite rugby players and rowers | Age: 23 ± 3 Sex: 25% F | 54 | Self-reported (past 6 months) | Summer 108.9 (102.8–115.4) Winter 86.8 (81.8–92.1) | NA | NA | Crystal Chem enzymatic assay | |
| Prospective Cohort Studies | |||||||||||
| Aregbesola, A. (2013) [25] | 1998–2011 | 10 years | Pneumonia | KIHD study: middle age and aging people | Age: 53–73 Sex: 49% F | 1421 | Clinically diagnosed | 43.5 (17.8) | tertile 1: 8.9–33.8 | tertile 3: 50.8–112.8 | HPLC |
| Porojnicu, A. C. (2012) [36] | 2007 | winter season | ARTI | Medical employees from a hospital | Age: 20–57 Sex: 94% F | 105 | Laboratory or x-ray confirmed | NA | NA | HPLC | |
| Sabetta, J.R. (2010) [26] | 2009–2010 | 5 months | Viral ARTI | Healthy adults | Age: 20–88 Sex: 57% F | 198 | Clinically diagnosed Laboratory confirmed | 71.0 (2.0) | 95 | ≥95 | Diasorin CLIA |
| He, C-S. (2013) [15] | 2011 | 4 months | URTI | Young athletes | Age: 18–40 Sex: 30% F | 225 | Self-reported (4 month diaries) | 53.0 (40.0–66.0) | 12–30 | >120 | HPLC |
| First Author (Publication Year) | Year of Study | Follow-Up Time | Outcome | Participants | Age (Mean ± SD)/Sex (% Female) | Sample Size | Severity Measurement | Mean (SD)/Median (IQR) 25(OH)D (nmol/L) | Lowest 25(OH)D Category (nmol/L) | Highest 25(OH)D Category (nmol/L) | 25(OH)D Measure ment Method |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cross-Sectional Studies | |||||||||||
| Mamani, M. (2017) [45] | NA | Pneumonia severity | Hospitalised patients with CAP | Age: 68 ± 10 Sex: 29% F | 73 | CURB-65 > 2 ICU admission Death | Severe: 52.8 (77.5) Non-severe: 56.5 (48.0) Yes: 59.8 (88.4) No: 52.8 (47.6) Yes: 64.6 (91.8) No: 53.0 (55.4) | <25 | ≥75 | Diasorin CLIA | |
| Pletz, M. W. (2014) [14] | 2002–2008 | Pneumonia severity | Participants with pneumonia | Age: ≥18 Sex: 43% F | 300 | Hospitalisation | Severe: 32.0 (19.5) Non-severe: 40.5 (25.0) | NA | NA | Diasorin CLIA | |
| Robertsen, S. (2014) [46] | 2007–2008 | ARTI | Tromsø population-based study | Age: ≥40 Sex: % F | 791 | Duration of the illness | NA | NA | Roche CLIA | ||
| Lu, D. (2017) [13] | 2011 | Pneumonia severity | Patients with pneumonia | Age: 60–94 Sex: 31% F | 49 | Duration of hospitalisation | <25 | ≥25 | IDS ELISA | ||
| Kim, H.J. (2015) [41] | 2012–2014 | Pneumonia severity | Hospitalised patients with CAP | Age: 18–96 Sex: 34% F | 797 | 28-day all-cause mortality Need for mechanical ventilator | <50 | ≥50 | CLIA | ||
| Brance, M. (2018) [39] | 2015–2016 | Pneumonia severity | Hospitalised patients with CAP | Age: >18 Sex: 59% F | 167 | CURB-65 ≥ 2 | Severe: 29.0 (18.3) Non-severe: 29.8 (18.8) | <25 | >50 | Siemens CLIA | |
| Yaghoobi, M.H. (2019) [44] | 2015 | Ventilator-associated pneumonia | Hospitalised patients with ventilator-associated pneumonia | Age: 18–82 Sex: 37% F | 84 | Mortality in 28 days Blood culture Duration of ventilation SOFA score | Yes: 61.5 (23.7) No: 61.9 (20.8) Positive: 53.4 (12.3) Negative: 62.7 (22.3) | <75 | ≥75 | NA | |
| Scullion, L. (2018) [47] | NA | ARTI | Elite rugby players and rowers | Age: 23 ± 3 Sex: 25%F | 53 | Duration of the illness | Summer: 4.8 (3.0) Winter: 6.9 (4.3) | NA | NA | Crystal Chem enzymatic assay | |
| Prospective Cohort Studies | |||||||||||
| Laaksi, I. (2007) [16] | 2002 | 6 months | ARTI severity | Young military men | Age: ≥18 Sex: 0% F | 652 | Number of days absence from duty due to ARTI | <40 | ≥40 | IDS OCTEIA | |
| Remmelts, H.F. (2012) [43] | 2007–2010 | 30 days | Pneumonia severity | Hospitalised patients with CAP | Age: ≥18 Sex: 44% F | 272 | ICU admission 30-day mortality PSI > 3 | ICU: 34.9 (23.8–46.3) No ICU: 48.3 (30.8–68.4) Yes: 25.8 (19.8–40.1) No: 48.8 (32.4–68.9) | <50 | >75 | Diasorin CLIA |
| Holter, J.C. (2016) [40] | 2008–2014 | 6 years | Pneumonia severity | Hospitalised patients with CAP | Age: ≥18 Sex: 49% F | 241 | CURB-65 ≥ 3 ICU admission Long-term all-cause mortality | <30 | ≥50 | Siemens CLIA | |
| Leow, L. (2011) [42] | 2008 | 4 months | Pneumonia severity | Hospitalised patients with CAP | Age: 16–97 Sex: NA | 112 | 30-day mortality | <30 | >50 | Roche CLIA | |
| Sabetta, J.R. (2010) [26] | 2009–2010 | 5 months | Viral ARTI severity | Healthy adults | Age: 20–88 Sex: 57% F | 198 | Duration of the illness | <95 | ≥95 | Diasorin CLIA | |
| He, C-S. (2013) [15] | 2011 | 4 months | URTI severity | Young athletes | Age: 18–40 Sex: 31% F | 103 | Duration of the illness SSC | 12–30 | >120 | HPLC | |
| First Author (Published Year) | Duration of Illness Mean (SD)/Median (IQR) (Days) | p-Value | |
|---|---|---|---|
| Lowest 25(OH)D Category | Highest 25(OH)D Category | ||
| Mamani, M. (2017) 1 | 11.03 (7.5) | 9.47 (6.1) | |
| Lu, D. (2017) 1 | 26.2 (15.6) | 15.5 (11.1) | 0.014 |
| He, C-S. (2013) 2 | 13 (10–17) | 5 (5–7) | ≤0.05 |
| Sabetta, J.R. (2010) 2 | 6 (2–8) | 6 (2–27) | |
| Laaksi, I. (2007) 3 | 4 (2–6) | 2 (0–4) | 0.004 |
| Kim, H.J. (2015) 1 | 12.5 (15.4) | 10.3 (11.0) | 0.570 |
| Robertsen, S. (2014) 2 | 14 | 13 | |
| Yaghoobi, M.H. (2019) 4 | 13.4 (6.1) | 13.7 (9.8) | 0.880 |
| Holter, J.C. (2016) 2 | 4 (2–6) | 5 (3–10) | |
| Scullion, L. (2018) 2,a | 6.9 (4.3) | 4.8 (3.0) | 0.044 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pham, H.; Rahman, A.; Majidi, A.; Waterhouse, M.; Neale, R.E. Acute Respiratory Tract Infection and 25-Hydroxyvitamin D Concentration: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3020. https://doi.org/10.3390/ijerph16173020
Pham H, Rahman A, Majidi A, Waterhouse M, Neale RE. Acute Respiratory Tract Infection and 25-Hydroxyvitamin D Concentration: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(17):3020. https://doi.org/10.3390/ijerph16173020
Chicago/Turabian StylePham, Hai, Aninda Rahman, Azam Majidi, Mary Waterhouse, and Rachel E. Neale. 2019. "Acute Respiratory Tract Infection and 25-Hydroxyvitamin D Concentration: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 17: 3020. https://doi.org/10.3390/ijerph16173020