Effect of Comorbidity Assessed by the Charlson Comorbidity Index on the Length of Stay, Costs and Mortality among Older Adults Hospitalised for Acute Stroke

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Outcomes
2.3. Covariates
3. Statistical Analyses
4. Ethics Approval
5. Results
5.1. Cohort Characteristics
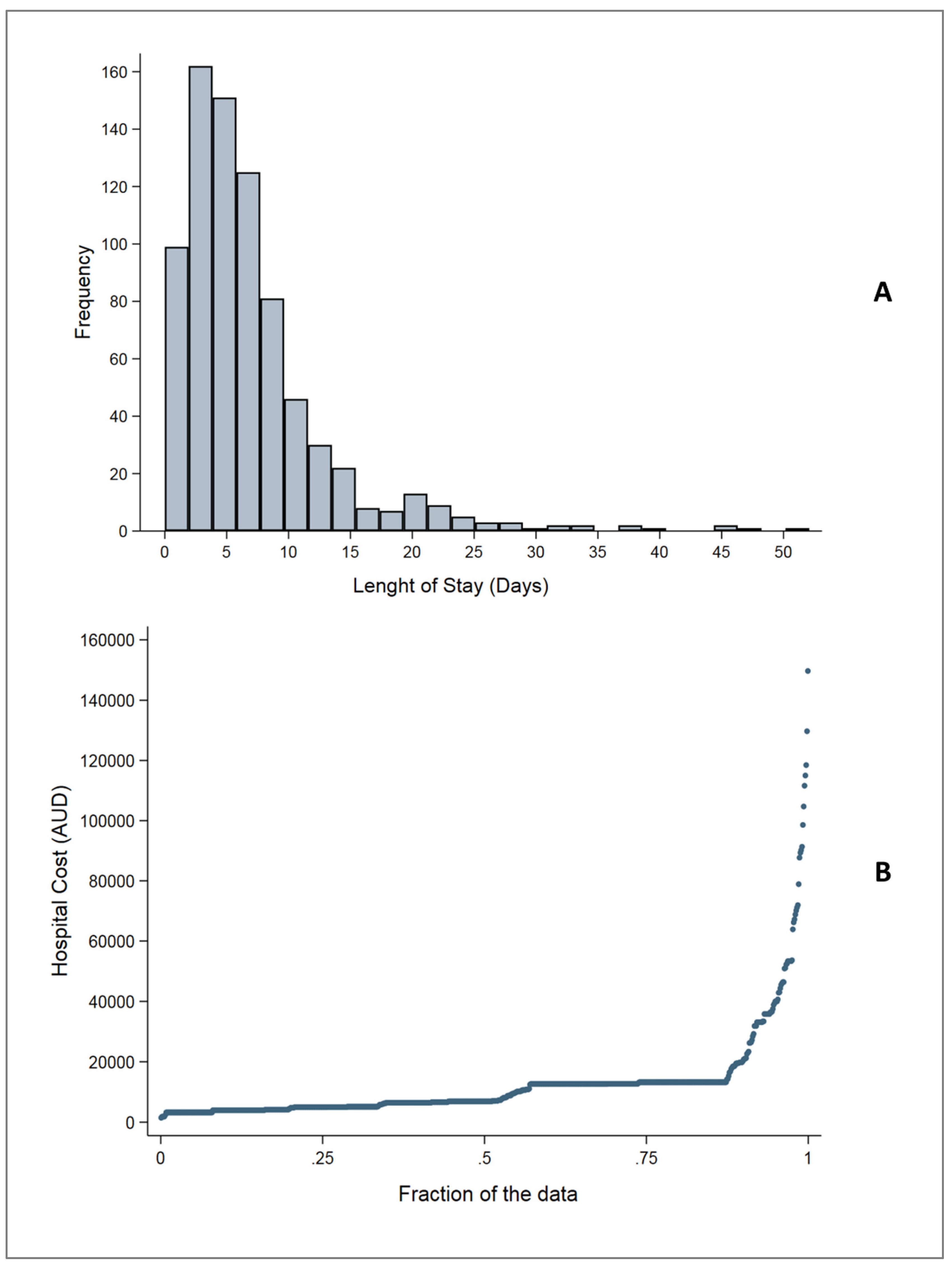
5.2. Length of Stay
5.3. Costs
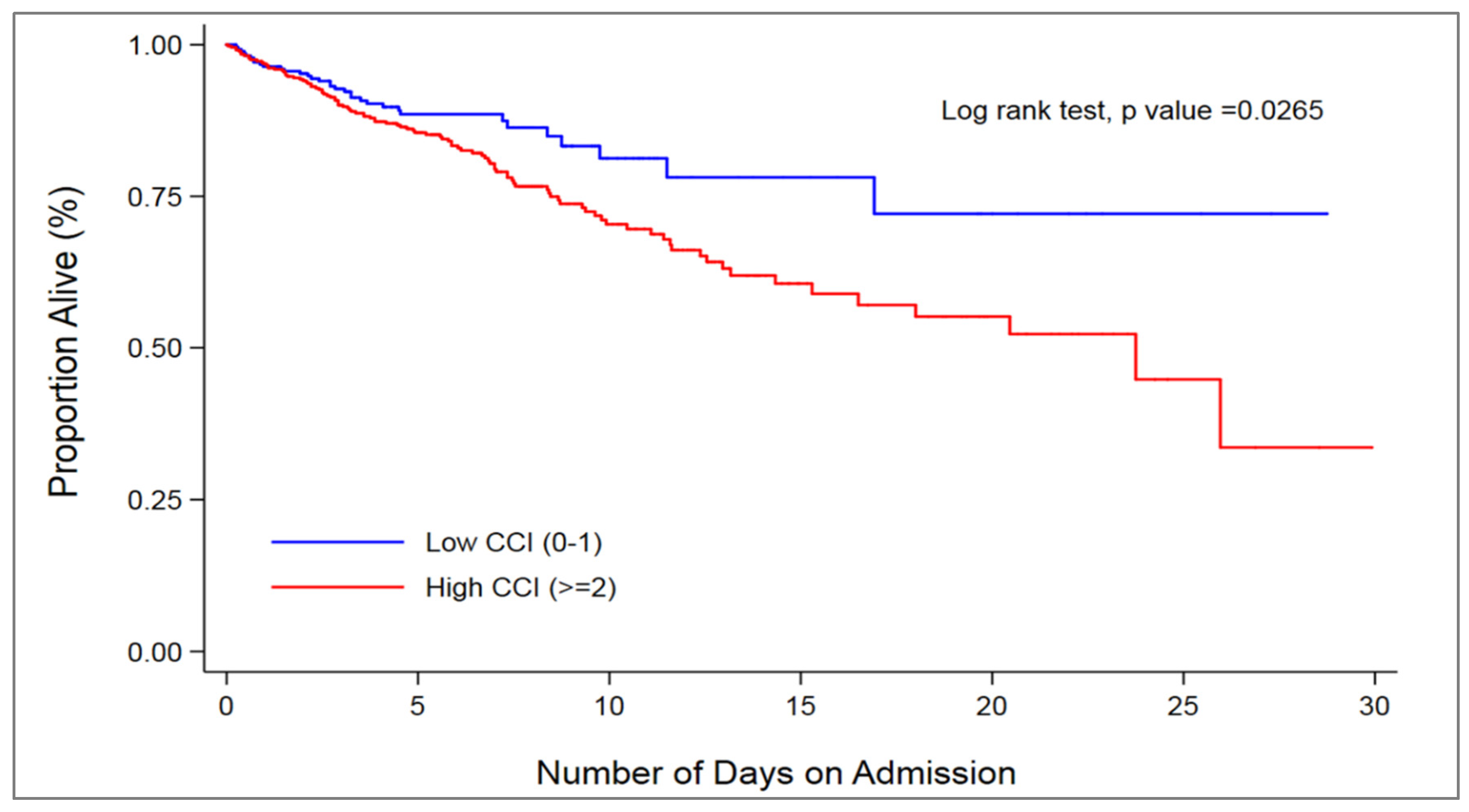
5.4. Mortality
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kennedy, B.K.; Berger, S.L.; Brunet, A.; Campisi, J.; Cuervo, A.M.; Epel, E.S.; Franceschi, C.; Lithgow, G.J.; Morimoto, R.I.; Pessin, J.E.; et al. Geroscience: Linking aging to chronic disease. Cell 2014, 159, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Ofori-Asenso, R.; Chin, K.L.; Curtis, A.J.; Zomer, E.; Zoungas, S.; Liew, D. Recent Patterns of Multimorbidity Among Older Adults in High-Income Countries. Popul. Health Manag. 2018. [Google Scholar] [CrossRef] [PubMed]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Wallace, E.; Salisbury, C.; Guthrie, B.; Lewis, C.; Fahey, T.; Smith, S.M. Managing patients with multimorbidity in primary care. BMJ 2015, 350, h176. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Stroke and Its Management in Australia: An Update; Cardiovascular Disease Series No. 37. Cat. No. CVD 61; AIHW: Canberra, Australia, 2013.
- Stroke Foundation. No Postcode Untouched: Stroke in Australia 2017. Available online: https://strokefoundation.org.au/What-we-do/Research/No-postcode-untouched (accessed on 13 May 2018).
- Phillips, M.C.; Leyden, J.M.; Chong, W.K.; Kleinig, T.; Czapran, P.; Lee, A.; Koblar, S.A.; Jannes, J. Ischaemic stroke among young people aged 15 to 50 years in Adelaide, South Australia. Med. J. Aust. 2011, 195, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Deloitte Access Economics. The Economic Impact of Stroke in Australia: Scoping Cost Effective Prevention. Available online: https://www2.deloitte.com/au/en/pages/economics/articles/economic-impact-stroke-australia.html (accessed on 13 May 2018).
- Gallacher, K.I.; Batty, G.D.; McLean, G.; Mercer, S.W.; Guthrie, B.; May, C.R.; Langhorne, P.; Mair, F.S. Stroke, multimorbidity and polypharmacy in a nationally representative sample of 1,424,378 patients in Scotland: Implications for treatment burden. BMC Med. 2014, 12, 151. [Google Scholar] [CrossRef] [PubMed]
- Tran, J.; Norton, R.; Conrad, N.; Rahimian, F.; Canoy, D.; Nazarzadeh, M.; Rahimi, K. Patterns and temporal trends of comorbidity among adult patients with incident cardiovascular disease in the UK between 2000 and 2014: A population-based cohort study. PLoS Med. 2018, 15, e1002513. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.D.; Kamal, N.; Jeerakathil, T. Bridging the Evidence-to-Practice Gap in Stroke Care. JAMA 2018. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, K.; Morrison, D.; Jani, B.; Macdonald, S.; May, C.R.; Montori, V.M.; Erwin, P.J.; Batty, G.D.; Eton, D.T.; Langhorne, P.; et al. Uncovering treatment burden as a key concept for stroke care: A systematic review of qualitative research. PLoS Med. 2013, 10, e1001473. [Google Scholar] [CrossRef] [PubMed]
- Falsetti, L.; Viticchi, G.; Tarquinio, N.; Silvestrini, M.; Capeci, W.; Catozzo, V.; Fioranelli, A.; Buratti, L.; Pellegrini, F. Charlson comorbidity index as a predictor of in-hospital death in acute ischemic stroke among very old patients: A single-cohort perspective study. Neurol. Sci. 2016, 37, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Pettinari, L.; Capeci, W.; Falsetti, L.; Tarquinio, N.; Kafyeke, A.; Fioranelli, A.; Catozzo, V.; Viticchi, G.; Gentile, A.; Pellegrini, F. Prevalence of the most common comorbidities in a cohort of elderly patients affected by acute ischemic stroke. Ital. J. Med. 2015, 9, 80. [Google Scholar] [CrossRef]
- Caballero, P.E.J.; Espuela, F.L.; Cuenca, J.C.P.; Moreno, J.M.R.; Zamorano, J.D.P.; Naranjo, I.C. Charlson Comorbidity Index in Ischemic Stroke and Intracerebral Hemorrhage as Predictor of Mortality and Functional Outcome after 6 Months. J. Stroke Cerebrovasc. Dis. 2013, 22, E214–E218. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Kwok, C.S.; Gale, C.P.; Doherty, P.; Olier, I.; Sperrin, M.; Kontopantelis, E.; Peat, G.; Mamas, M.A. Impact of co-morbid burden on mortality in patients with coronary heart disease, heart failure, and cerebrovascular accident: A systematic review and meta-analysis. Eur. Heart J. Qual. Care Clin. Outcomes 2017, 3, 20–36. [Google Scholar] [CrossRef] [PubMed]
- Yurkovich, M.; Avina-Zubieta, J.A.; Thomas, J.; Gorenchtein, M.; Lacaille, D. A systematic review identifies valid comorbidity indices derived from administrative health data. J. Clin. Epidemiol. 2015, 68, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, L.B.; Samsa, G.P.; Matchar, D.B.; Horner, R.D. Charlson Index comorbidity adjustment for ischemic stroke outcome studies. Stroke 2004, 35, 1941–1945. [Google Scholar] [CrossRef] [PubMed]
- Australian Consortium for Classification Development. ICD-10-AM/ACHI/ACS. Available online: https://www.accd.net.au/Icd10.aspx (accessed on 14 May 2018).
- Victoria State Government. Casemix Funding. Available online: https://www2.health.vic.gov.au/hospitals-and-health-services/funding-performance-accountability/activity-based-funding/casemix-funding (accessed on 11 July 2018).
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Bradburn, M.J.; Clark, T.G.; Love, S.B.; Altman, D.G. Survival analysis part II: Multivariate data analysis—An introduction to concepts and methods. Br. J. Cancer 2003, 89, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Thumboo, J.; Earnest, A.; Yong, S.L.; Fong, K.Y. The effect of comorbidity on hospital mortality in patients with SLE from an Asian tertiary hospital. Lupus 2014, 23, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Beyerlein, A. Quantile regression-opportunities and challenges from a user’s perspective. Am. J. Epidemiol. 2014, 180, 330–331. [Google Scholar] [CrossRef] [PubMed]
- Grube, M.M.; Koennecke, H.C.; Walter, G.; Meisel, A.; Sobesky, J.; Nolte, C.H.; Wellwood, I.; Heuschmann, P.U.; Berlin Stroke, R. Influence of acute complications on outcome 3 months after ischemic stroke. PLoS ONE 2013, 8, e75719. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.E.; Shobha, N.; Dai, D.; Olson, D.M.; Reeves, M.J.; Saver, J.L.; Hernandez, A.F.; Peterson, E.D.; Fonarow, G.C.; Schwamm, L.H. Risk score for in-hospital ischemic stroke mortality derived and validated within the Get With the Guidelines-Stroke Program. Circulation 2010, 122, 1496–1504. [Google Scholar] [CrossRef] [PubMed]
- Ovbiagele, B. Nationwide trends in in-hospital mortality among patients with stroke. Stroke 2010, 41, 1748–1754. [Google Scholar] [CrossRef] [PubMed]
- Cadilhac, D.A.; Kilkenny, M.F.; Levi, C.R.; Lannin, N.A.; Thrift, A.G.; Kim, J.; Grabsch, B.; Churilov, L.; Dewey, H.M.; Hill, K.; et al. Risk-adjusted hospital mortality rates for stroke: Evidence from the Australian Stroke Clinical Registry (AuSCR). Med. J. Aust. 2017, 206, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.T.; Sung, S.F.; Wong, Y.S.; Wu, C.S.; Hsu, Y.C.; Su, Y.H.; Li, C.H.; Hung, L.C. Risk Factors for In-Hospital Mortality among Ischemic Stroke Patients in Southern Taiwan. Int. J. Gerontol. 2016, 10, 86–90. [Google Scholar] [CrossRef]
- Alhazzani, A.A.; Mahfouz, A.A.; Abolyazid, A.Y.; Awadalla, N.J.; Katramiz, K.; Faraheen, A.; Khalil, S.N.; Aftab, R. In Hospital Stroke Mortality: Rates and Determinants in Southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Saposnik, G.; Cote, R.; Phillips, S.; Gubitz, G.; Bayer, N.; Minuk, J.; Black, S. Stroke outcome in those over 80: A multicenter cohort study across Canada. Stroke 2008, 39, 2310–2317. [Google Scholar] [CrossRef] [PubMed]
- Dogan, N.O.; Akinci, E.; Gumus, H.; Akilli, N.B.; Aksel, G. Predictors of Inhospital Mortality in Geriatric Patients Presenting to the Emergency Department With Ischemic Stroke. Clin. Appl. Thromb./Hemost. Off. J. Int. Acad. Clin. Appl. Thromb./Hemost. 2016, 22, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.K.; Olsen, T.S.; Dehlendorff, C.; Kammersgaard, L.P. Hemorrhagic and ischemic strokes compared: Stroke severity, mortality, and risk factors. Stroke 2009, 40, 2068–2072. [Google Scholar] [CrossRef] [PubMed]
- Kokotailo, R.A.; Hill, M.D. Coding of stroke and stroke risk factors using international classification of diseases, revisions 9 and 10. Stroke 2005, 36, 1776–1781. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.C.; Chow, V.; Yong, A.S.; Chung, T.; Kritharides, L. Prognostic impact of the Charlson comorbidity index on mortality following acute pulmonary embolism. Respiration 2013, 85, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yang, K.S.; Hsann, Y.M.; Lim, V.; Ong, B.C. The effect of comorbidity and age on hospital mortality and length of stay in patients with sepsis. J. Crit. Care 2010, 25, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Albertsen, P.C.; Moore, D.F.; Shih, W.; Lin, Y.; Li, H.; Lu-Yao, G.L. Impact of comorbidity on survival among men with localized prostate cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 1335–1341. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Cheon, S.H. Analysis of variation in length of stay (LOS) after ischemic and hemorrhagic stroke using the Charlson Comorbidity Index (CCI). J. Phys. Ther. Sci. 2015, 27, 799–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lakomkin, N.; Kothari, P.; Dodd, A.C.; VanHouten, J.P.; Yarlagadda, M.; Collinge, C.A.; Obremskey, W.T.; Sethi, M.K. Higher Charlson Comorbidity Index Scores Are Associated With Increased Hospital Length of Stay After Lower Extremity Orthopaedic Trauma. J. Orthop. Trauma 2017, 31, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.J.; Greenberg, S.E.; Sathiyakumar, V.; Thakore, R.; Ehrenfeld, J.M.; Obremskey, W.T.; Sethi, M.K. Relationship between the Charlson Comorbidity Index and cost of treating hip fractures: Implications for bundled payment. J. Orthop. Traumatol. Off. J. Ital. Soc. Orthop. Traumatol. 2015, 16, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Kaatz, S.; Coleman, C.I.; Bookhart, B.; Laliberte, F.; Nelson, W.W.; Brown, K.; Martin, S.; Schein, J.; Lefebvre, P. Implications of stroke and bleeding risk scores and comorbidities on episode-based bundled payments for patients with nonvalvular atrial fibrillation. Curr. Med. Res. Opin. 2018, 34, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Rudin, R.S.; Gidengil, C.A.; Predmore, Z.; Schneider, E.C.; Sorace, J.; Hornstein, R. Identifying and Coordinating Care for Complex Patients: Findings from the Leading Edge of Analytics and Health Information Technology. Rand Health Q. 2017, 6, 2. [Google Scholar] [PubMed]
- Austin, S.R.; Wong, Y.N.; Uzzo, R.G.; Beck, J.R.; Egleston, B.L. Why Summary Comorbidity Measures Such As the Charlson Comorbidity Index and Elixhauser Score Work. Med. Care 2015, 53, e65–e72. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | All (n = 776) | CCI § | p-Value † | |
|---|---|---|---|---|
| Low (n = 296) | High (n = 480) | |||
| Mean age, years (SD) | 80.1 (8.3) | 79.7 (8.5) | 80.3 (8.2) | 0.123 |
| ≥85 years, n (%) | 265 (34.2) | 89 (30.1) | 176 (36.7) | 0.170 |
| Female, n (%) | 362 (46.7) | 144 (48.7) | 218 (45.4) | 0.381 |
| Country of birth, n (%) | ||||
| Australia | 399 (51.4) | 172 (58.1) | 223 (47.3) | 0.031 |
| Asia | 37 (4.8) | 11 (3.7) | 26 (5.4) | |
| Europe | 251 (32.3) | 82 (27.7) | 169 (35.2) | |
| Other | 86 (11.5) | 31 (10.5) | 58 (12.1) | |
| Interpreter required, n (%) | 82 (10.6) | 27 (9.1) | 55 (11.5) | 0.304 |
| Married or in a de facto relationship, n (%) | 391 (50.4) | 154 (51.4) | 239 (49.8) | 0.361 |
| Type of stroke, n (%) | ||||
| Haemorrhagic | 212 (27.3) | 102 (34.4) | 110 (22.9) | 0.001 |
| Ischaemic | 514 (66.2) | 174 (58.8) | 340 (70.8) | |
| Undetermined | 50 (6.4) | 20 (6.8) | 30 (6.3) | |
| Patient with multiple records, n (%) | 34 (4.4) | 12 (4.1) | 22 (4.6) | 0.726 |
| Comorbidities, n (%) | ||||
| Hypertension | 507 (65.3) | 192 (64.9) | 315 (65.6) | 0.829 |
| Diabetes with complication | 81 (10.4) | 0 (0.0) | 81 (16.9) | <0.001 |
| Metastatic cancer | 26 (3.4) | 0 (0.0) | 26 (5.4) | <0.001 |
| Atrial fibrillation | 188 (24.2) | 64 (21.6) | 124 (25.8) | 0.183 |
| Renal disease | 83 (10.7) | 0 (0.0) | 83 (17.3) | <0.001 |
| Congestive heart failure | 52 (6.7) | 5 (1.7) | 47 (9.8) | <0.001 |
| Dementia | 35 (4.5) | 13 (4.4) | 22 (4.6) | 0.901 |
| Chronic pulmonary disease | 25 (3.2) | 7 (2.4) | 18 (3.8) | 0.288 |
| Myocardial infarction | 49 (6.3) | 9 (3.0) | 40 (8.3) | 0.003 |
| Smoking (current), n (%) | 25 (3.2) | 9 (3.0) | 16 (3.3) | 0.822 |
| Treated in a stroke unit, n (%) | 480 (61.9) | 171 (57.8) | 309 (64.4) | 0.066 |
| Admitted to ICU, n (%) | 80 (10.3) | 29 (9.8) | 51 (10.6) | 0.713 |
| Developed complication, n (%) | 463 (59.7) | 147 (49.7) | 316 (65.8) | <0.001 |
| Patient from aged care residential facility, n (%) | 23 (3.0) | 6 (2.0) | 17 (3.5) | 0.372 |
| IRSAD, n (%) | ||||
| Quintile 1 (most disadvantaged) | 163 (21.0) | 75 (25.3) | 88 (18.4) | 0.031 |
| Quintile 2 | 160 (20.6) | 59 (19.9) | 101 (21.0) | |
| Quintile 3 | 196 (25.2) | 65 (22.0) | 131 (27.3) | |
| Quintile 4 | 127 (16.4) | 30 (13.5) | 87 (18.1) | |
| Quintile 5 (least disadvantaged) | 130 (16.8) | 57 (19.3) | 73 (15.2) | |
| Admission year, n (%) | ||||
| 2013 | 187 (24.1) | 74 (25.0) | 113 (23.5) | 0.885 |
| 2014 | 284 (36.6) | 106 (35.8) | 178 (37.1) | |
| 2015 | 305 (39.3) | 116 (39.2) | 189 (39.4) | |
| Model 1 a: 25th Percentile | Model 2 a: Median | Model 3 a: 75th Percentile | ||||
|---|---|---|---|---|---|---|
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| High CCI (≥2) | 1446 | 832–2060 ** | 2483 | 788–4175 ** | 3140 | 1214–5068 ** |
| Constant | 5148 | 4067–6229 ** | 9521 | 6539–12,501 ** | 11,257 | 7865–14,650 ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ofori-Asenso, R.; Zomer, E.; Chin, K.L.; Si, S.; Markey, P.; Tacey, M.; Curtis, A.J.; Zoungas, S.; Liew, D. Effect of Comorbidity Assessed by the Charlson Comorbidity Index on the Length of Stay, Costs and Mortality among Older Adults Hospitalised for Acute Stroke. Int. J. Environ. Res. Public Health 2018, 15, 2532. https://doi.org/10.3390/ijerph15112532
Ofori-Asenso R, Zomer E, Chin KL, Si S, Markey P, Tacey M, Curtis AJ, Zoungas S, Liew D. Effect of Comorbidity Assessed by the Charlson Comorbidity Index on the Length of Stay, Costs and Mortality among Older Adults Hospitalised for Acute Stroke. International Journal of Environmental Research and Public Health. 2018; 15(11):2532. https://doi.org/10.3390/ijerph15112532
Chicago/Turabian StyleOfori-Asenso, Richard, Ella Zomer, Ken Lee Chin, Si Si, Peter Markey, Mark Tacey, Andrea J. Curtis, Sophia Zoungas, and Danny Liew. 2018. "Effect of Comorbidity Assessed by the Charlson Comorbidity Index on the Length of Stay, Costs and Mortality among Older Adults Hospitalised for Acute Stroke" International Journal of Environmental Research and Public Health 15, no. 11: 2532. https://doi.org/10.3390/ijerph15112532