Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Registration
2.2. Search Strategy
2.3. Inclusion Criteria and Study Selection
2.4. Quality Assessment for Each Eligible Study
2.5. Data Extraction and Data Synthesis
3. Results
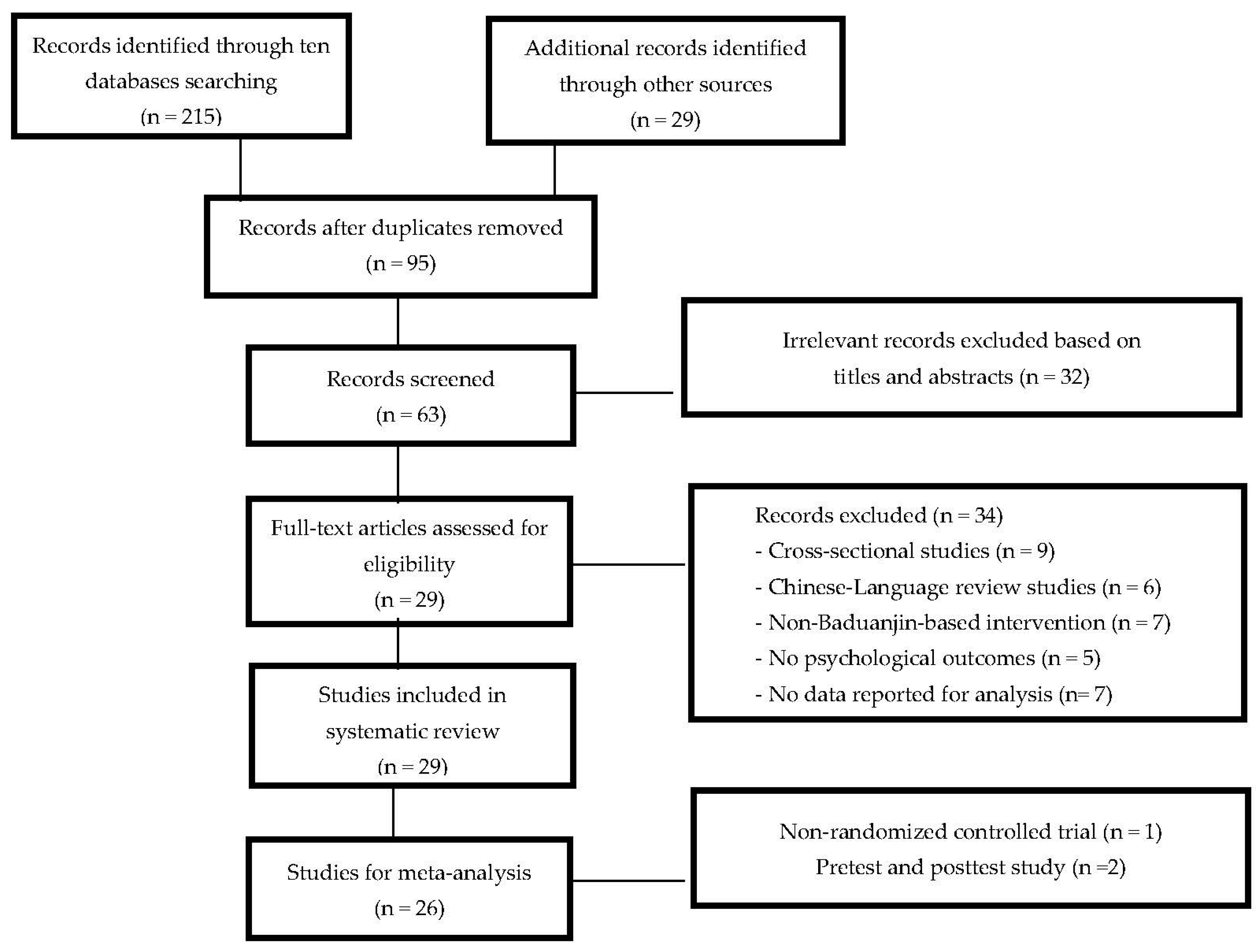
3.1. Literature Search
3.2. Study Characteristics
3.3. Methodological Quality
3.4. Effects of Baduanjin on Anxiety and Depression
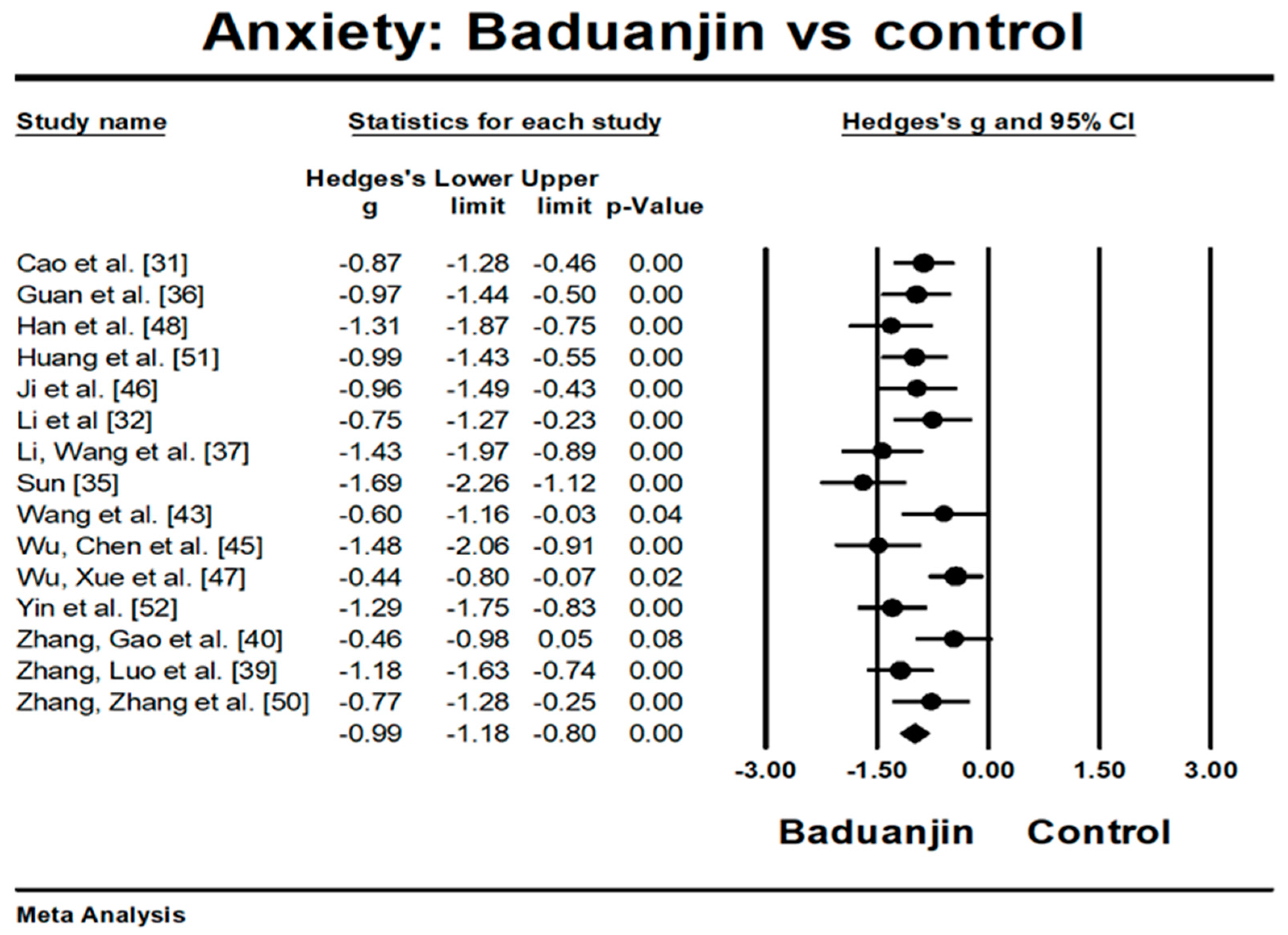
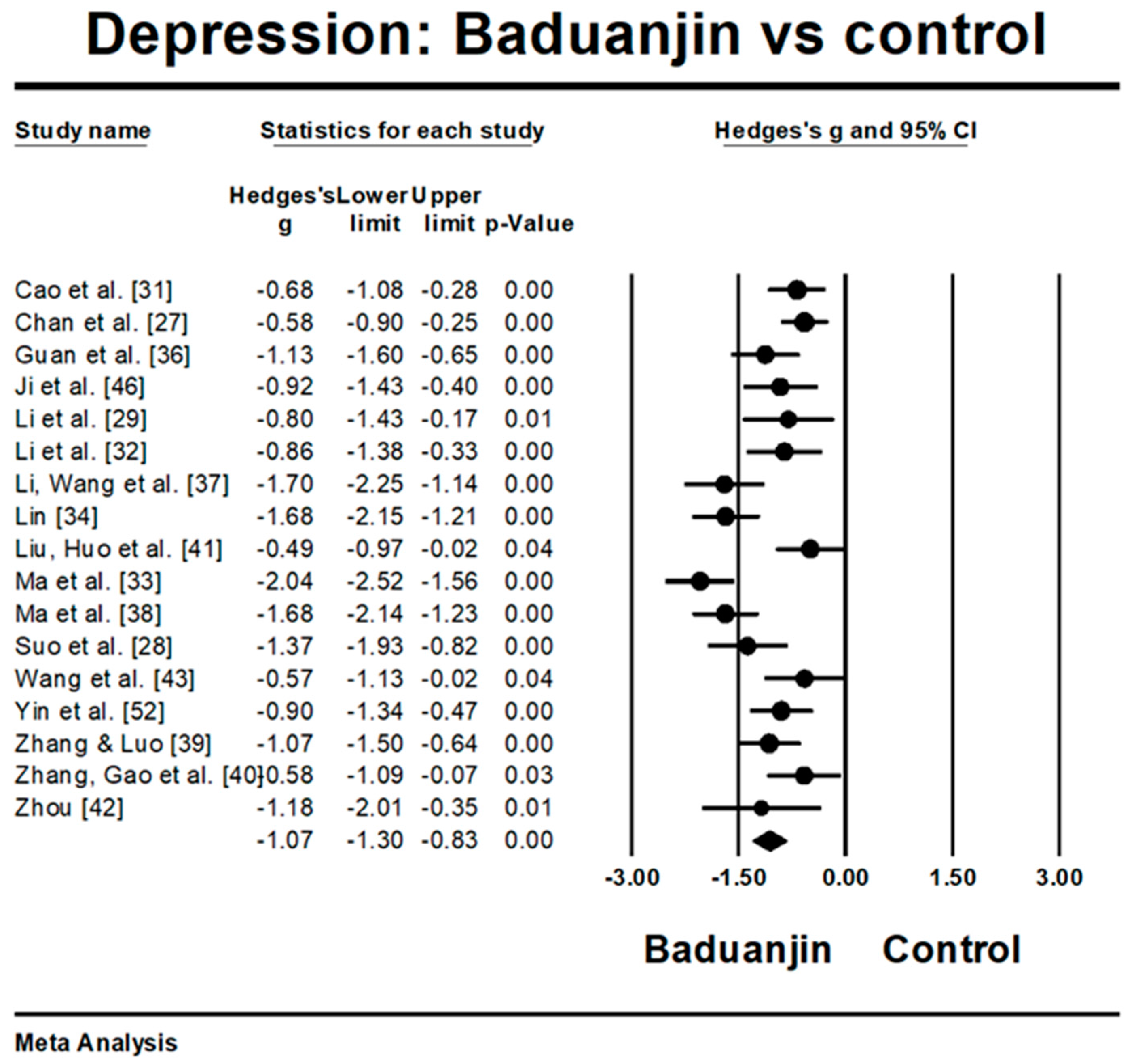
3.4.1. Baduanjin Intervention Versus Control Group on Anxiety and Depression
3.4.2. Moderator Analysis
4. Discussion
5. Conclusion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Zou, L.; Pan, Z.; Yeung, A.; Talwar, S.; Wang, C.; Liu, Y.; Shu, Y.; Chen, X.; Thomas, G. A review study on the beneficial effects of Baduanjin. J. Alter. Comp. Med. 2017, 23, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X.; Boyden, S.; Wang, H. Systematic Review and Meta-Analysis of Mindfulness-Based (Baduanjin) Exercise for Alleviating Musculoskeletal Pain and Improving Sleep Quality in People with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Yu, D. Effect of a long-term modified Tai Chi-based intervention in attenuating bone mineral density in postmenopausal women in southeast China: Study protocol for a randomized controlled trial. Clin. Trials Degener. Dis. 2017, 2, 46–52. [Google Scholar]
- Zou, L.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M.; Li, T.; Du, G.; Liu, Y. Tai chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, E0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, K.; Shu, Y.; Chen, X.; Luo, L.; Zhao, X. The Effect of Taichi Practice on Attenuating Bone Mineral Density Loss: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2017, 14, 1000. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Tian, Z.; Wang, H.; Shu, Y. Effect of Yang-Style Tai Chi on Gait Parameters and Musculoskeletal Flexibility in Healthy Chinese Older Women. Sports 2017, 5, 52. [Google Scholar] [CrossRef]
- Jing, J.; Qiu, X.; Qin, Y. Comparative study of the influences of Liu Zi Jue and Ba Duan Jin on college students. Hebei Sports Sci. 2013, 32, 1056–1059. [Google Scholar]
- Chen, H.; Yeh, M.; Lee, F. The effects of Baduanjin Qigong in the prevention of bone loss for middle-aged women. Am. J. Chin. Med. 2006, 34, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Liu, J.; Egorova, N.; Chen, X.; Sun, S.; Xue, X.; Huang, J.; Zheng, G.; Wang, Q.; Chen, L.; et al. Increased Hippocampus-Medial Prefrontal Cortex Resting-State Functional Connectivity and Memory Function after Tai Chi Chuan Practice in Elder Adults. Front. Aging Neurosci. 2016, 8, 25. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Zhuang, Y. Effect of health Baduanjin Qigong for mild to moderate Parkinson’s disease. Geriatr. Gerontol. Int. 2015, 16, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Zhuang, Y.; Kang, Y. Effect of Health Qigong Baduanjin on Fall Prevention in Individuals with Parkinson’s Disease. J. Am. Geriatr. Soc. 2016, 64, 227–228. [Google Scholar] [CrossRef] [PubMed]
- An, B.C.; Wang, Y.; Jiang, X.; Lu, H.; Fang, Z.; Wang, Y.; Dai, K. Effects of Baduanjin exercise on knee osteoarthritis: A one-year study. Chin. J. Integr. Med. 2013, 19, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.H.; Tan, C.; Yuan, S. Baduanjin exercise for insomnia: A systematic review and meta-analysis. Behav. Sleep Med. 2017, 4, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Mei, L.; Chen, Q.; Li, G. Systematic review of Chinese traditional exercise Baduanjin modulating the blood lipid metabolism. Evid. Based Complement. Alternat. Med. 2012, 2012, 282131. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Sasaki, J.E.; Wang, H.; Xiao, Z.; Fang, Q.; Zhang, M. A Systematic Review and Meta-Analysis of Baduanjin Qigong for Health Benefits: Randomized Controlled Trials. Evid. Based Complement. Alternat. Med. 2017, 2017, 4548706. [Google Scholar] [CrossRef] [PubMed]
- Levav, I.; Rutz, W. The WHO World Health Report 2001 new understanding—New hope. Isr. J. Psychiatry Relat. Sci. 2002, 39, 50–56. [Google Scholar] [PubMed]
- The World Health Organization. Shaping the Future: Burden of disease in DALYs by cause, sex, and mortality stratum in WHO regions, estimates for 2002. In World Health Report; The World Health Organization: Geneva, Switzerland, 2003; pp. 160–165. [Google Scholar]
- Hiroeh, U.; Appleby, L.; Mortensen, P.B. Death by homicide, suicide, and other unnatural causes in people with mental illness: A population-based study. Lancet 2001, 358, 2110–2112. [Google Scholar] [CrossRef]
- Januzzi, J.L.; Stern, T.A.; Pasternak, R.C.; DeSanctic, R. The influence of anxiety and depression on outcomes of patients with coronary artery disease. Arch. Intern. Med. 2000, 160, 1913–1921. [Google Scholar] [CrossRef] [PubMed]
- Mental Illness Statistics and Facts. Available online: http://www.selfhelparticles.net (accessed on 29 June 2009).
- Cheng, F. Effects of Baduanjin on mental health: A comprehensive review. J. Bodyw. Mov. Ther. 2015, 19, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Crouse, J.C.; Lin, J.H. Using active video games for physical activity promotion: A systematic review of the current state of research. Health Educ. Behav. 2013, 40, 171–192. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Slipp, L.; Niles, H.; Jacquart, J.; Chow, C.; Fava, M.; Denninger, J.; Benson, H.; Fricchione, G. Effectiveness of the relaxation response-based group intervention for treating depressed Chinese American immigrants: A pilot Study. Int. J. Environ. Res. Public Health 2014, 11, 9186–9201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. A Guide for Population-Based Approaches to Increasing Levels of Physical Activity: Implementation of the WHO Global Strategy on Diet, Physical Activity and Health; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Egger, M.; Smith, G.D.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.M.; Ho, R.T.H.; Chung, K.F.; Wang, C.; Yao, T.; Ng, S.; Chan, C. Qigong Exercise Alleviates Fatigue, Anxiety, and Depressive Symptoms, Improves Sleep Quality, and Shortens Sleep Latency in Persons with Chronic Fatigue Syndrome-Like Illness. Evid. Based Complement. Alternat. Med. 2014, 2014, 106048. [Google Scholar] [CrossRef] [PubMed]
- Suo, L.; Yu, H. Jieyu decotion with psychological intervention and Ba Duan Jin exercises improve depressive symptoms in perimenopausal patients. J. Changchun Univ. Tradit. Chin. Med. 2016, 32, 131–133. [Google Scholar]
- Li, C.; Tan, Z.; Liu, S. A research of Baduanjin exercise treating college students with depression. Sports Sci. Res. 2014, 18, 72–75. [Google Scholar]
- Yang, Q.; Huang, R. Effects of Baduanjin on psychology and life quality of type 2 diabetic patients accompanied with depression. Chin. Med. Mod. Distance Educ. China 2017, 15, 52–54. [Google Scholar]
- Cao, C.; Guo, X.; Chen, N.; Yan, X.; Zhang, H. Research of effects of eight-brocade of TCM on treating anxiety and depression in the elderly patients with lung-spleen Qi deficiency in stable period of COPD. J. Liaoning Univ. TCM. 2016, 18, 120–123. [Google Scholar]
- Li, Q.; Wang, L.; Zhang, X. Effects of Baduanjin on emotion and life quality of breast cancer patients during post-operation radiotherapy. Chin. Gen. Practice Nurs. 2017, 15, 2257–2259. [Google Scholar]
- Ma, S.; Dou, N.; Chen, C.; Zhao, Y.; Li, S. Effect of the traditional Baduanjin exercise in women with peri-menopausal syndrome and depression. Chin. Gen. Practice 2010, 25. [Google Scholar]
- Lin, Q. Effects and cognitive improvements of Baduanjin exercise on elder patients with mild cognitive impairment. Chin. J. Gerontol. 2017, 37, 3358–3360. [Google Scholar]
- Sun, Y. Effects of Baduanjin combined with relaxation exercise on community type 2 diabetics with dysthymic disorder. Chin. Rural Health Serv. Adm. 2015, 35, 357–359. [Google Scholar]
- Guan, Y.; Wang, S.; Ma, M. Effect of Baduanjin-based exercise intervention on related parameters in type 2 diabetes patients. J. Nurs. Sci. 2012, 27, 23–24. [Google Scholar]
- Li, Q.; Wang, L.; Jiao, H. Application of eight-section brocade in postoperative rehabilitation of non-small cell lung cancer patients. Chin. Nurs. Res. 2017, 31, 3755–3759. [Google Scholar]
- Ma, S.; Dou, N.; Chen, C.; Zhao, Y. Rehabilitation effects of walking and Baduanjin to the perimenopausal syndrome with depression. Chin. J. Rehabilit. Med. 2011, 26, 738–741. [Google Scholar]
- Zhang, L.; Luo, L. Effects of nursing intervention on sleep quality and mental health of women with perimenopausal syndrome. Mod. J. Integr. Tradit. Chin. West Med. 2016, 25, 556–557. [Google Scholar]
- Zhang, Z.; Gao, J.; Liang, Y.; Zhang, L. Effects of Baduanjin Qigong on psychological state and life quality of patients with primary glaucoma. China J. Chin. Ophthalmol. 2016, 26, 234–238. [Google Scholar]
- Liu, Y.; Huo, R.; Lai, Y.; Yao, Q.; Chen, C.; Chen, Y. Community-based study on effects of Chinese Qigong-Baduanjin on depression symptoms and life quality of patients with type 2 diabetes mellitus. Chin. J. Sports Med. 2012, 31, 212–217. [Google Scholar]
- Zhou, T. Observation of blood sugar and mental intervention of health Qigong on 25 cases of diabetic patients with depression. Nei. Mongol. J. Tradit. Chin. Med. 2014, 24, 70. [Google Scholar]
- Wang, R.; Guan, F.; Yan, X. Qigong Baduanjin rehabilitation of elderly patients with coronary artery disease. J. Changchun Univ. Chin. Med. 2016, 32, 752–754. [Google Scholar] [CrossRef]
- Zhang, F.; Lin, Z.; Zhang, L.; Wang, C. Observation of clinical effect by paroxetine combined with eight trigrams boxing exercise therapy for depression patients. Chin. J. Mod. Drug Appl. 2017, 11, 109–111. [Google Scholar]
- Wu, Y.; Chen, O.; Luo, Y.; Ji, R.; He, S. Application of Tai Ji Quan and Eight Duan Jin in improving anxiety and depression of patients with coronary heart disease. Chin. Nurs. Res. 2016, 30, 4050–4052. [Google Scholar]
- Ji, X.; Wang, Q.; Fang, C. Effect of exercise therapy on anxiety and depression in the patients with diabetes mellitus. Practical Geriatr. 2012, 26, 331–333. [Google Scholar]
- Wu, X.; Xue, W.; Fang, J.; Wang, J.; Fang, X.; Ma, X.; Liu, Z.; Ye, C.; Duan, J. Baduanjin of movements on the risk of falls in community elderly people for 60 cases. Chin. Med. Mod. Distance Educ. China 2017, 3, 106–109. [Google Scholar]
- Han, Y.; Wang, Q.; Luo, D.; Xue, J. Effects of Baduanjin training on anxiety and anxiety-related serum protein in postoperative patients with breast cancer. J. Nurs. Sci. 2017, 48, 42–44. [Google Scholar]
- Liu, H.; Chen, Y.; Yi, X.; Zhang, Y.; Zhou, Q.; Yu, Y.; Huang, Y. Effect of Baduanjin exercise prescription on physical and mental regulation in type 2 diabetes patients with anxiety. Hunan J. Tradit. Chin. Med. 2014, 30, 16–18. [Google Scholar]
- Zhang, J.; Zhang, W.; Shen, H. The effect of Baduanjin practice on the generalized anxiety disorder. Chin. J. Sports Med. 2016, 35, 231–233. [Google Scholar]
- Huang, X.; Wu, S.; Xu, H. Clinical observation of anxiety improvement of Baduanjin exercise combined with adanon on heroin addicts. Shenzhen J. Integr. Tradit. Chin. West Med. 2015, 25, 98–99. [Google Scholar]
- Yin, H.; Zhao, B.; Liao, Y. The influence of eight infantile finger loops and whorls in combination with psychomatic relaxation exercise on blood sugar and emotional disorder of patients with diabetes mellitus combined with emotional disorder. Henan Tradit. Chin. Med. 2016, 36, 2214–2216. [Google Scholar]
- Guan, F.; Liu, X.; Cheng, N.; Lin, Q.; Lin, Y.; Lin, X. The influence of Baduanjin and broadcast gymnastics on depression of psychiatric inpatients. China Med. Pharm. 2016, 6, 142–144. [Google Scholar]
- Wu, X.; Li, L.; Ding, P.; Li, J. Effect of Baduanjin on depression in 62 patients with coronary heart disease and depression. World Chin. Med. 2014, 9, 39–43. [Google Scholar]
- Zhou, H.; Chen, C.; Ma, S. Effect of Baduanjin intervention on depression in women with perimenopausal syndrome and depression. J. Nurs. 2011, 25, 1448–1489. [Google Scholar]
- Chen, K.; Berger, C.; Manheimer, E.; Forde, D.; Magidson, J.; Dachman, L.; Lejuez, C. Meditative therapies for anxiety: A systematic review and meta-analysis of randomized controlled trials. Depress Anxiety 2012, 29, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, G.; Rampes, H.; Tuffrey, V.; Richardson, J.; Pikington, K. Yoga for anxiety: A systematic review of the research evidence. Br. J. Sports Med. 2005, 39, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Singh, S.; Sibinga, E.M.; Gould, N.; Rowland-Seymour, A.; Sharma, R.; Berger, Z.; Sleicher, D.; Maron, D.; Shihab, H.; et al. Meditation Programs for Psychological Stress and Well-being A Systematic Review and Meta-analysis. JAMA Intern. Med. 2014, 174, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Man, J.; Lee, E.; Wu, T.; Benson, H.; Fricchione, G.; Wang, W.; Yeung, A. The effects of Qigong on anxiety, depression, and psychological well-being: A systematic review and Meta-analysis. Evid. Based Complement. Alternat. Med. 2013, 2013, 152738. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Ryu, S.; Noh, J.; Lee, J. The Effectiveness of Daily Mindful Breathing Practices on Test Anxiety of Students. PLoS ONE 2016, 11, e0164822. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chan, C.; Ho, R.; Chan, J.; Ng, S.; Chan, C. Managing stress and anxiety through qigong exercise in healthy adults: A systematic review and meta-analysis of randomized controlled trials. BMC Complement. Altern. Med. 2014, 14, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, L.; Ma, W.; Huang, J.; Tseng, L.; Hsueh, K. Effect of relaxation-breathing training on anxiety and asthma signs/symptoms of children with moderate-to-severe asthma: A randomized controlled trial. Int. J. Nurs. Stud. 2009, 46, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Yackle1, K.; Schwarz, L.; Kam, K.; Sorokin, J.; Huguenard, J.; Feldman, J.; Luo, L.; Krasnow, M. Breathing control center neurons that promote arousal in mice. Science 2017, 355, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.; Li, A.; Ng, S.; Ho, R.; Xu, A.; Yao, T.; Wang, X.; So, K.; Chan, C. Adiponectin potentially contributes to the ant depressive effects of Baduanjin Qigong exercise in women with chronic fatigue syndrome-like illness. Cell Transplant. 2017, 26, 493–501. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author [Reference] | Location (Language) | ISZ (AR) | Study Participants | Intervention Protocol | Exercise Intensity | Outcome Measured | Adverse Event; Follow-Up | ||
|---|---|---|---|---|---|---|---|---|---|
| Training Duration and Dosage (Qualification of Instructor) | Total Hour | No. of Session | |||||||
| Randomized controlled trials | |||||||||
| Chan et al. (2014) [27] | Hong Kong, China (English) | 150 (13.3%) | CFS-like illness with mild anxiety and depression (a mean age of 39) | BJ: 16 90-min sessions for 9 weeks (a Qigong master) (daily 30-min home practice); CG: Waitlist | 24 | 16 | NR | Anxiety and depression (HADS) | No; 3-month |
| Suo, Yu et al. (2016) [28] | Nanjin, China (Chinese) | 60 (0%) | Perimenopasual women with depression (aged 44–56) | BJ: 7 × 60 min/wk for 12 weeks (trained nurse) + mental therapy (2 × 30 min/wk for 12 weeks) + usual drug therapy; CG: mental therapy (2 × 30 min/wk for 3 weeks) + usual drug therapy | 84 | 84 | NR | Depression (HAMD) | No/ 6-month |
| Li et al. (2014) [29] | Hengyan, China (Chinese) | 45 (11.1%) | College students with depression (aged 20–23) | BJ: 5 × 60 min /wk for 40 weeks (an Qigong instructor); CG: Usual physical education classes (training volume was NR) | 200 | 200 | NR | Depression (SDS) | NR; No |
| Yang et al. (2017) [30] | Zhengzhou, China (Chinese) | 110 (4.5%) | Type 2 DM patients with depression (aged 32–70) | BJ: 7× 60 min/wk for 12 weeks (an Qigong instructor) + usual care; CG: 2 × 30 min/wk for 3 weeks (educational program) + usual care | 84 | 84 | NR | Depression (HAMD) | NR No |
| Cao et al. (2016) [31] | Nangjin, China (Chinese) | 103(0.97%) | COPD patients with anxiety and depression (a mean age of 70.49) | BJ: 4 × 30 min/wk for 24 weeks (trained instructors) + usual care; CG: 4 × 30 min/wk for 24 weeks (self-selected pace walking) + usual care | 48 | 96 | NR | Anxiety (SAS) Depression (SDS) | NR; 12-week |
| Li et al. (2017) [32] | ShanXi, China (Chinese) | 68(10.3%) | Patients with breast cancer (a mean age of 45.45) | BJ: 5 sessions (session length was NR; trained nurse)/wk for 12 weeks + usual care CG: Usual care | NA | 60 | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| Ma et al. (2010) [33] | Tangshan, China (Chinese) | 100 (0%) | Perimenopasual women with depression (aged 45–55) | BJ: 7 × 45 min/wk for 12 weeks (instructor qualification was NR); CG: Unaltered lifestyle | 63 | 84 | AHR:100 bpm | Depression (CESD) | NR; No |
| Lin (2017) [34] | FuZhou, China Chinese | 94(0%) | Older adults with mild cognitive impairment (aged 61–79) | BJ: 6 sessions (session length was NR; instructor qualification was NR)/wk for 24 weeks + usual care; CG: Usual care | NA | 144 | NR | Depression (GDS) | NR; No |
| Sun (2015) [35] | Jilin, China (Chinese) | 65 (0%) | Type 2 DM patients (a mean age of 46.1) | BJ: 5 × 60 min/wk for 24 weeks (trained instructor) CG: Unaltered lifestyle | 120 | 120 | ARH:100 bpm | Anxiety (SAS) Depression (SDS) | NR; No |
| Guan et al. (2012) [36] | Hefei, China (Chinese) | 80(1.25%) | Type 2 DM patients (aged 45–70) | BJ: 7 × 60 min/wk for 16 weeks + usual care CG: Usual care | 112 | 112 | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| Li, Wang et al. (2017) [37] | Shanxi, China (Chinese) | 70(4.3%) | Patients with Non-small cell lung cancer (a mean age of 56). | BJ: at least 3 × 30 min/wk for 12 weeks (trained nurse) + usual care CG: Usual care | 18 | 36 | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| Ma et al. (2011) [38] | Tangshan, China (Chinese) | 145 (0%) | Perimenopausal women with depression (aged 45–55) | BJ: 54 × 45 min/wk for 12 weeks (trained instructor) CG1: 5 × 45/wk for 12 weeks (self-selected pace walking); CG2: Unaltered lifestyle | 45 | 60 | THR: 100 bpm | Depression (CESD) | No; No |
| Zhang & Luo (2016) [39] | Chengdu, China (Chinese) | 93(0%) | Perimenopausal women with depression and anxiety (aged 45–55) | BJ: 7 × 45 min/wk for 12 weeks (community doctor) + educational program (twice per week); CG: Twice per week (educational program) | 63 | 84 | NR | Anxiety (SAS) Depression (SDS) | No; No |
| Zhang, Gao et al. (2016) [40] | Bejing, China (Chinese) | 60(0%) | Patients with glaucoma (aged 40–60) | BJ: 7 × 30 min/wk for 12 weeks (hospital doctor) + usual care CG: Usual care | 42 | 84 | NR | Anxiety (SAS) Depression (SDS) | No; No |
| Liu, Huo et al. (2012) [41] | Beijing, Ching (Chinese) | 88(21.6%) | Type 2 DM patients with depression (a mean age of 64.2) | BJ: 3 × 40 min/wk for 12 weeks (trained instructor) +educational program (a total of 6 30 min educational sessions); CG: Educational program (a total of 6 30 min sessions). | 24 | 36 | NR | Depression (SDS) | No; No |
| Zhou (2014) [42] | Beijing, China (Chinese) | 25 (0%) | Type 2 DM patients with depression (aged 51–80) | BJ: 7 × 60 min/wk for 12 weeks (NR) +usual care CG: Usual care | 84 | 84 | NR | Depression (SDS) | No; No |
| Wang et al. (2016) [43] | Fuzhou, China (Chinese) | 50 (0%) | Patients with coronary heart disease (aged 60–70) | BJ: (Training volume was NR) for 12 weeks (NR) + usual drug therapy + educational program CG: Usual drug therapy + educational program | NA | NA | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| Zhang, Lin et al. (2017) [44] | Liaochen, China (Chinese) | 124 (0%) | Patients with depression (a mean age of 42.8). | BJ: 7 × 60 min/wk for 6 weeks (trained instructor) +usual drug therapy CG: Usual drug therapy | 42 | 42 | NR | Depression (HAMD) | NR;no |
| Wu, Chen et al. (2016) [45] | Changsha, China (Chinese) | 60 (0%) | Patients with coronary heart disease (aged 49–79) | BJ: 5 × 60 min/wk for 12 weeks (NR) + usual care CG: Usual care | 60 | 60 | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| Ji et al. (2012) [46] | Wuxi, China (Chinese) | 62(0%) | DM patients (aged 36–81) | BJ: 7 × 45 min/wk for 8 weeks (physical therapist) + usual care + education program CG: Usual care + educational program | 42 | 56 | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| Wu, Xue et al. (2017) [47] | Beijing, China (Chinese) | 120(0%) | Older adults with anxiety and balance impaired (aged 65–80). | BJ: 2 sessions (session length was NR) per day for 30 days (hospital doctor) CG: Unaltered lifestyle | NA | 60 | NR | Anxiety (SAS) | NR; no |
| Han et al. (2017) [48] | TaiYuan, China (Chinese) | 64(6.25%) | Patients with breast cancer and depression (a mean age of 46.23). | BJ: 5 × 20 min/wk for 12 weeks (five trained nurses) + usual care CG: Usual care | 20 | 60 | NR | Anxiety (SAS) | NR; No |
| Liu, Chen et al. (2014) [49] | Changsha, China (Chinese) | 40(0%) | Type 2 DM with anxiety (a mean of 57). | BJ: 5 × 30 min/wk for 24 weeks (NR) + usual care + drug therapy CG: Usual care + drug therapy | 60 | 120 | NR | Anxiety (SAS) | NR; No |
| Zhang, Zhang et al. (2016) [50] | Beijing, China (Chinese) | 64(3.1%) | Patients with generalized anxiety disorder (aged 22–65). | BJ: 2 × 60 min/wk for 12 weeks (NR) (daily 30 min home practice) + usual care + drug therapy CG: Usual care + drug therapy | 24 | 24 | NR | Anxiety (SAS and HARS) | NR; No |
| Huang et al. (2015) [51] | Zhuhai, China (Chinese) | 100(12%) | Heroin addicts with anxiety (aged 18–50) | BJ: 7 × 30 min/wk for 20 weeks (NR) + mental therapy + drug therapy; CG: Mental therapy + drug therapy | 70 | 140 | NR | Anxiety (SAS) | NR; No |
| Yin et al. (2016) [52] | Zhuhai, China (Chinese) | 88(0%) | DM patients with mental illness (a mean age of 55.47) | BJ:2 x 60 min/wk for 24 weeks (trained nurse) (daily 60min home practice) +usual care +mental therapy CG: Usual care + mental therapy | 48 | 48 | NR | Anxiety (SAS) Depression (SDS) | NR; No |
| 2. Non-randomized controlled studies | |||||||||
| Non-randomized controlled trial | |||||||||
| Guan, Liu et al. (2016) [53] | Fuzhou, China (Chinese) | 60 (0%) | Inpatients with depression (a mean age of 41.4) | BJ: 7 × 30 min/wk for 6 weeks (trained nurse) + usual care + drug therapy; CG1: The choreographed aerobic exercise (dosage was not reported) + usual care + drug therapy CG2: Usual care + drug therapy | 21 | 42 | NR | Depression (HAMD) | NR; No |
| Author [Reference] | Study Location | ISZ (AT) | Health Status | Duration and Dosage | Exercise Intensity | QOI | Outcome Measured | Conclusion | p | AE/FU |
|---|---|---|---|---|---|---|---|---|---|---|
| Wu, Li (2014) [54] | Beijing, China (Chinese) | 68 (8.8%) | Patients with coronary heart disease and depression, with a mean age of 53. | BJ: 3 × 30 min/wk, 2 weeks | NR | Trained instructor | Depression (SDS and HAMD) | SDS: 68(11.34) vs. 67.63(11.46) HAMD: 33.23(6.9) vs. 32.60(7.13) Effectively reduced depression | 0.02 0.004 | NR/No |
| Zhou, Chen et al. (2011) [55] | Tangshan, China (Chinese) | 30 (0%) | Perimenopausal women with depression, with a mean age of 48.05. | BJ: Daily morning practice (training volume was not specifically reported), 6 months | NR | Trained instructor | Depression (CESD) | CESD: 25.67(5.82) vs. 19.03(4.93) Effectively reduced depression | <0.01 | NR/No |
| Author [Reference] | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Randomized controlled trials or non-randomized controlled studies | ||||||||||
| Chan, Li et al. (2014) [27] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 9/9 |
| Suo, Yu et al. (2016) [28] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Li, Tan et al. (2014) [29] | Yes | Yes | Yes | Yes | Yes | Yes | No | No | Yes | 7/9 |
| Yang, Huang et al. (2017) [30] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Cao, Guo et al. (2016) [31] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Li et al. (2017) [32] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Ma, Dou et al. (2010) [33] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | 8/9 |
| Lin (2017) [34] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Sun (2015) [35] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Guan, Wang et al. (2012) [36] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Li, Wang et al. (2017) [37] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Ma, Dou et al. (2011) [38] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | 8/9 |
| Zhang & Luo (2016) [39] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Zhang, Gao et al. (2016) [40] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Liu, Huo et al. (2012) [41] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Zhou (2014) [42] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Wang, Guan et al. (2016) [43] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Zhang, Lin et al. (2017) [44] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Wu, Chen et al. (2016) [45] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Ji, Wang et al. (2012) [46] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Wu, Xue et al. (2017) [47] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | 8/9 |
| Han, Wang et al. (2017) [48] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Liu, Chen et al. (2014) [49] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Zhang, Zhang et al. (2016) [50] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Huang, Wu et al. (2015) [51] | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | 6/9 |
| Yin, Zhao et al. (2016) [52] | Yes | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 7/9 |
| Guan, Liu et al. (2016) [53] | No | Yes | No | Yes | Yes | Yes | Yes | No | Yes | 6/9 |
| Wu, Li (2014) [54] | No | No | Yes | Yes | Yes | No | No | No | Yes | 4/9 |
| Zhou, Chen et al. (2011) [55] | No | No | Yes | Yes | Yes | No | No | No | Yes | 4/9 |
| Categorical Moderator | Outcome | Level | No. of Studies | Hedge’s g | 95% CI | I2, % | Test for Between-Group Homogeneity | ||
|---|---|---|---|---|---|---|---|---|---|
| Q-Value | df(Q) | p-Value | |||||||
| Intervention duration | Anxiety | <16 weeks | 9 | −0.99 | −1.23 to −0.75 | 45.87% | 0.55 | 1 | 0.46 |
| ≥16 weeks | 5 | −1.13 | −1.39 to −0.86 | 38.64% | |||||
| Training frequency | Anxiety | <5 sessions/week | 5 | −0.93 | −1.21 to −0.65 | 44.89% | 1.51 | 1 | 0.22 |
| ≥5 sessions/week | 10 | −1.20 | −1.52 to −0.87 | 74.31% | |||||
| Session length | Anxiety | Less than 1 h | 8 | −1.15 | −1.47 to −0.83 | 67.61% | 0.09 | 1 | 0.76 |
| 1 h or longer | 5 | −1.22 | −1.54 to −0.90 | 47% | |||||
| Control type | Anxiety | Active | 7 | −0.98 | −1.15 to −0.80 | 0% | 0.113 | 1 | 0.736 |
| passive | 8 | −1.04 | −1.39 to −0.70 | 73.19% | |||||
| Study quality | Anxiety | Low risk | 8 | −1 | −1.33 to −0.67 | 72.68% | 0.00 | 1 | 0.96 |
| High risk | 7 | −0.99 | −1.17 to −0.81 | 0% | |||||
| Continuous Moderator | Level | No. of Studies | 95% Confidence Interval | Q-Value | df | p | |||
| Total hour | Anxiety | 13 | −0.0053 | −0.009 to −0.0014 | 6.9 | 1 | 0.008 | ||
| Number of total sessions | Anxiety | 14 | −0.0009 | −0.005 to 0.003 | 0.2 | 1 | 0.66 | ||
| Categorical Moderator | Outcome | Level | No. of Studies | Hedge’s g | 95% CI | I2, % | Test for between-Group Homogeneity | ||
|---|---|---|---|---|---|---|---|---|---|
| Q-Value | df(Q) | p-Value | |||||||
| Intervention duration | Depression | <16 weeks | 12 | −1.08 | −1.39 to −0.77 | 78.3% | 0.03 | 1 | 0.87 |
| ≥6 weeks | 5 | −1.04 | −1.4 to −0.68 | 64.98% | |||||
| Training frequency | Depression | <5 sessions/week | 5 | −0.84 | −1.20 to −0.48 | 2.822 | 2.8 | 1 | 0.09 |
| ≥5 sessions/week | 11 | −1.22 | −1.50 to −0.95 | ||||||
| Session length | Depression | Less than 1 h | 8 | −1.14 | −1.54 to −0.74 | 82.75% | 0.7 | 1 | 0.4 |
| 1 h or longer | 6 | −0.94 | −1.19 to −0.68 | 37.51% | |||||
| Control type | Depression | Active | 8 | −0.84 | −1.02 to −0.66 | 16% | 3.74 | 1 | 0.053 |
| passive | 9 | −1.27 | −1.65 to −0.89 | 82.16% | |||||
| Study quality | Depression | Low risk | 12 | −1.11 | −1.41 to −0.82 | 76.8% | 0.44 | 1 | 0.51 |
| High risk | 5 | −0.95 | −1.34 to −0.57 | 68.97% | |||||
| Continuous Moderator | Level | No. of Studies | 95% Confidence Interval | Q-Value | df | p | |||
| Total hour | Depression | 14 | −0.0018 | −0.0051 to 0.0015 | 1.088 | 1 | 0.297 | ||
| Number of total sessions | Depression | 16 | −0.0023 | −0.006 to −0.0004 | 4.85 | 1 | 0.028 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, L.; Yeung, A.; Quan, X.; Hui, S.S.-C.; Hu, X.; Chan, J.S.M.; Wang, C.; Boyden, S.D.; Sun, L.; Wang, H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 321. https://doi.org/10.3390/ijerph15020321
Zou L, Yeung A, Quan X, Hui SS-C, Hu X, Chan JSM, Wang C, Boyden SD, Sun L, Wang H. Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2018; 15(2):321. https://doi.org/10.3390/ijerph15020321
Chicago/Turabian StyleZou, Liye, Albert Yeung, Xinfeng Quan, Stanley Sai-Chuen Hui, Xiaoyue Hu, Jessie S. M. Chan, Chaoyi Wang, Sean David Boyden, Li Sun, and Huiru Wang. 2018. "Mindfulness-Based Baduanjin Exercise for Depression and Anxiety in People with Physical or Mental Illnesses: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 15, no. 2: 321. https://doi.org/10.3390/ijerph15020321