
Identifying Meteorological Drivers for the Seasonal Variations of Influenza Infections in a Subtropical City — Hong Kong

Abstract
:1. Introduction
2. Materials and Methods
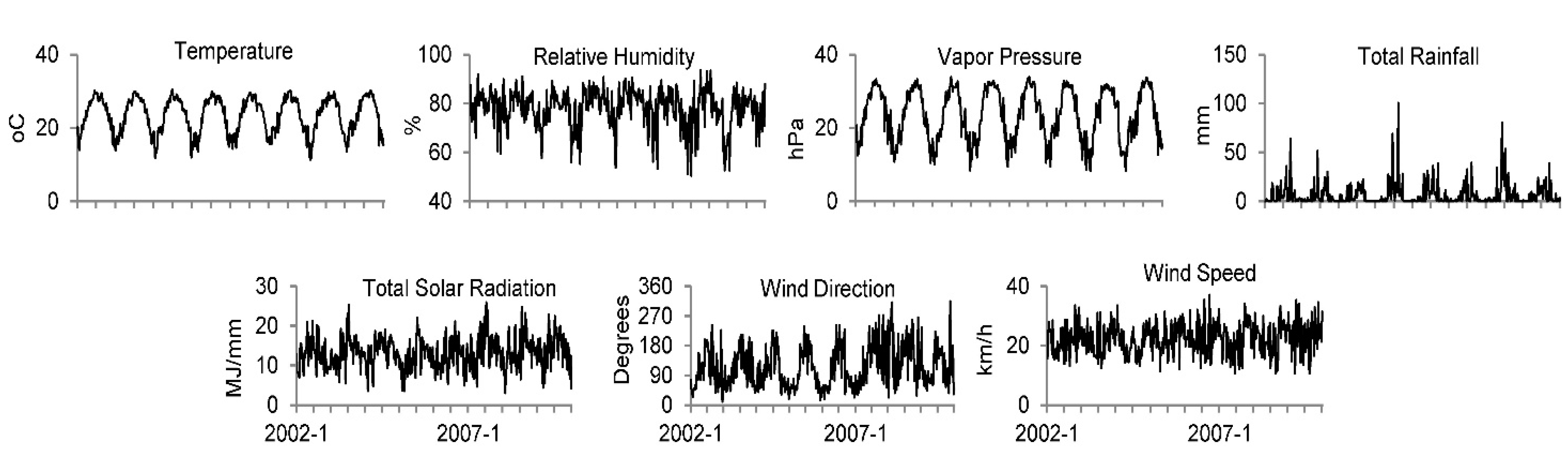
2.1. Data


2.2. Mathematical Model
2.3. Parameter Estimation
2.4. Sensitivity Analysis
- (1)
- (2)
- Model structure: In addition to the linear form of Equation (5), a multiplicative exponential form was also adopted in model fitting to test whether this would produce different results:
3. Results
3.1. Model Goodness of Fit

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables a | Year | ||||||
|---|---|---|---|---|---|---|---|
| 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | |
| Temperature | −4.1 (0.8) | −9.8 (2.9) | −2.6 (1.2) | −2.9 (1.2) | −5.2 (1.0) | −3.7 (0.6) | |
| Rel. humidity | 3.6 (1.4) | −3.5 (0.7) | |||||
| Abs. humidity | |||||||
| Rainfall | 10.7 (3.1) | 4.5 (2.0) | 2.3 (0.6) | 9.8 (2.3) | −12.7 (3.9) | 5.5 (1.9) | |
| Solar radiation | 10.9 (3.4) | ||||||
| Wind velocity (EW) | 7.6 (3.5) | −12.5 (2.8) | |||||
| Wind velocity (NS) | 10.9 (3.1) | ||||||
| AIC | 262.6 | 246.8 | 258.9 | 251.1 | 262.4 | 216.8 | 208.7 |
| Adj-R2 (%) | 66.5 | 37.1 | 48.8 | 32.9 | 47.4 | 84.0 | 67.2 |
| ΔAdj-R2 (%) | 18.9 | 22.1 | 2.9 | 16.1 | 32.9 | 38.7 | 56.9 |

3.2. Significant Meteorological Determinants
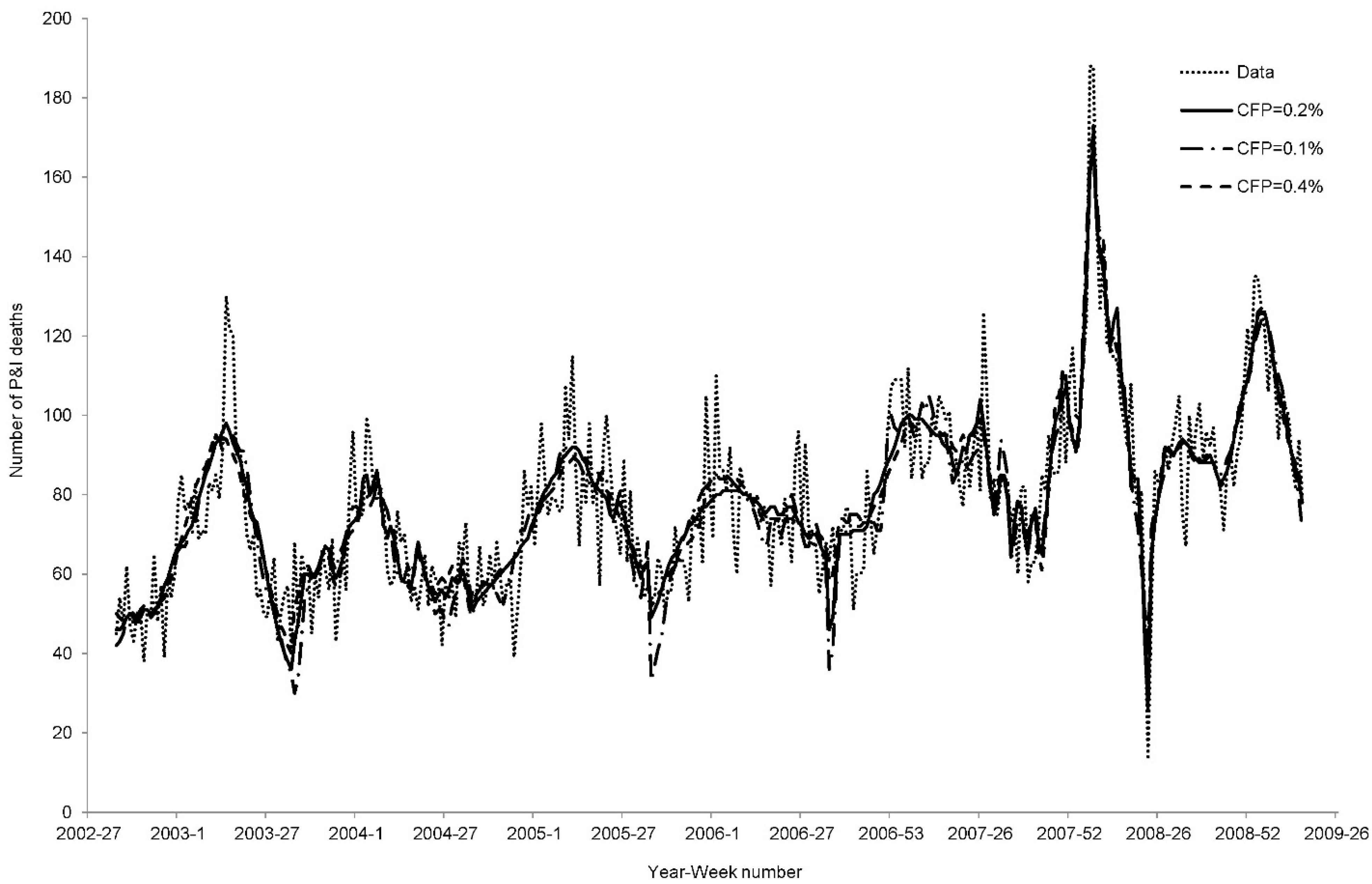
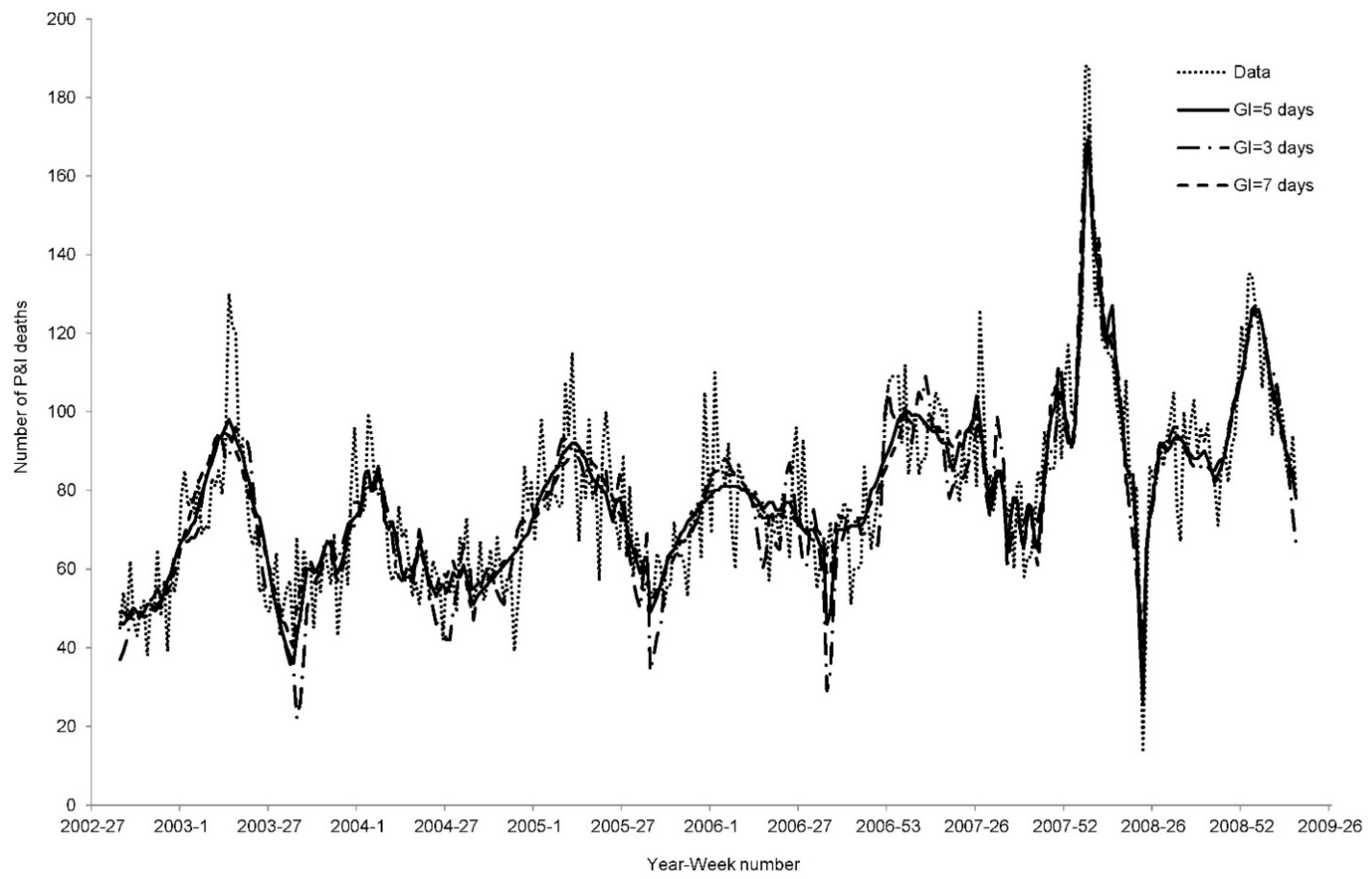
3.3. Sensitivity Analysis


| CFP = 0.1% | Year | ||||||
| Variables a | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Temperature | −6.8 (2.0) | −9.3 (3.3) | −3.5 (1.5) | −7.7 (1.6) | 7.6 (0.9) | −6.6 (0.3) | |
| Rel. humidity | 7.8 (1.5) | 2.8 (1.0) | 2.6 (1.2) | ||||
| Abs. humidity | |||||||
| Rainfall | 14.4 (2.9) | 9.9 (3.2) | 7.3 (0.7) | 16.2 (2.9) | |||
| Solar radiation | 8.4 (3.2) | 11.5 (3.9) | 9.5 (2.4) | ||||
| Wind velocity (EW) | −10.6 (2.9) | ||||||
| Wind velocity (NS) | 5.7 (2.7) | 9.3 (1.8) | 9.1 (3.2) | ||||
| AIC | 268.7 | 261.2 | 264.4 | 261.8 | 271.3 | 218.5 | 211.3 |
| Adj-R2 (%) | 62.9 | 15.6 | 45.1 | 17.6 | 40.0 | 83.4 | 63.8 |
| CFP = 0.4% | Year | ||||||
| Variables | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Temperature | −4.4 (0.6) | −10.0 (2.9) | −1.6 (0.5) | −5.7 (1.0) | −2.3 (0.6) | ||
| Rel. humidity | −2.4 (0.9) | −6.7 (1.2) | −4.8 (0.7) | ||||
| Abs. humidity | −3.3 (1.5) | ||||||
| Rainfall | 8.1 (3.1) | 2.2 (1.0) | 6.7 (2.8) | 7.3 (1.9) | |||
| Solar radiation | 11.0 (3.4) | ||||||
| Wind velocity (EW) | 9.2 (3.4) | −14.0 (2.9) | |||||
| Wind velocity (NS) | 11.4 (3.3) | ||||||
| AIC | 261.6 | 245.3 | 257.2 | 248.5 | 260.6 | 221.4 | 207.7 |
| Adj-R2 (%) | 66.5 | 38.8 | 49.6 | 37.3 | 49.2 | 82.2 | 68.0 |
| GI = 3 days | Year | ||||||
| Variables a | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Temperature | −7.8 (2.1) | −9.4 (3.7) | −3.6 (1.5) | −4.1 (1.5) | −10.4 (1.8) | −8.2 (0.9) | −7.1 (0.8) |
| Rel. humidity | 10.4 (1.6) | 4.8 (1.1) | 7.2 (1.2) | ||||
| Abs. humidity | |||||||
| Rainfall | 19.3 (3.3) | 12.6 (3.2) | 15.5 (1.9) | 21.3 (3.3) | |||
| Solar radiation | 13.0 (3.4) | 11.3 (4.3) | 14.0 (2.7) | −4.0 (1.6) | |||
| Wind velocity (EW) | −8.5 (3.0) | ||||||
| Wind velocity (NS) | 6.7 (2.8) | 13.8 (2.0) | 7.7 (3.2) | ||||
| AIC | 274.4 | 273.1 | 269.6 | 271.3 | 282.9 | 221.6 | 216.4 |
| Adj-R2 (%) | 58.6 | 12.3 | 39.2 | 15.6 | 25.2 | 82.1 | 60.3 |
| GI=7 days | Year | ||||||
| Variables | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 |
| Temperature | −4.4 (0.6) | −10.1 (2.9) | −1.6 (0.5) | −5.8 (1.0) | −2.3 (0.6) | ||
| Rel. humidity | −2.4 (0.9) | −6.7 (1.2) | −4.8 (0.7) | ||||
| Abs. humidity | −3.3 (1.5) | ||||||
| Rainfall | 8.2 (3.1) | 2.2 (1.0) | 6.9 (2.8) | 7.3 (1.9) | |||
| Solar radiation | 11.1 (3.4) | ||||||
| Wind velocity (EW) | 9.3 (3.4) | −14.1 (3.0) | |||||
| Wind velocity (NS) | 11.5 (3.3) | ||||||
| AIC | 261.6 | 245.3 | 257.1 | 248.5 | 260.5 | 221.4 | 207.7 |
| Adj-R2 (%) | 66.5 | 38.9 | 49.6 | 37.2 | 49.3 | 82.2 | 68.0 |
4. Discussion
5. Study Limitations and Uncertainties
6. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Chan, P.K.; Mok, H.Y.; Lee, T.C.; Chu, I.M.; Lam, W.Y.; Sung, J.J. Seasonal influenza activity in Hong Kong and its association with meteorological variations. J. Med. Virol. 2009, 81, 1797–1806. [Google Scholar] [CrossRef] [PubMed]
- Viboud, C.; Alonso, W.J.; Simonsen, L. Influenza in tropical regions. PLoS Med. 2006, 3. [Google Scholar] [CrossRef]
- Lipsitch, M; Viboud, C. Influenza seasonality: Lifting the fog. PNAS 2009, 106, 3645–3646. [Google Scholar]
- World Health Organization. Media Centre: Influenza (Seasonal): Fact Sheet 2009. Available online: http://www.who.int/mediacentre/factsheets/fs211/en/ (accessed on 1 April 2014).
- Wong, C.M.; Chan, K.P.; Hedley, A.J.; Peiris, J.M. Influenza-associated mortality in Hong Kong. Clin. Infect. Dis. 2004, 39, 1611–1617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, C.M.; Yang, L.; Chan, K.P.; Leung, G.M.; Chan, K.H.; Guan, Y.; Lam, T.H.; Hedley, A.J.; Peiris, J.S. Influenza-associated hospitalization in a subtropical city. PLoS Med. 2006, 3. [Google Scholar] [CrossRef] [Green Version]
- Dushoff, J.; Plotkin, J.B.; Levin, S.A.; Earn, D.J. Dynamical resonance can account for seasonality of influenza epidemics. PNAS 2004, 101, 16915–16916. [Google Scholar] [CrossRef] [PubMed]
- Shaman, J.; Pitzer, V.E.; Viboud, C.; Grenfell, B.T.; Lipsitch, M. Absolute humidity and the seasonal onset of influenza in the continental United States. PLoS Biol. 2010, 8. [Google Scholar] [CrossRef] [PubMed]
- Shaman, J.; Jeon, C.Y.; Giovannucci, E.; Lipsitch, M. Shortcomings of vitamin D-based model simulations of seasonal influenza. PLoS One 2011, 6. [Google Scholar] [CrossRef] [PubMed]
- Te Beest, D.E.; van Boven, M.; Hooiveld, M.; van den Dool, C.; Wallinga, J. Driving factors of influenza transmission in the Netherlands. Amer. J. Epidemiol. 2013, 178, 1469–1477. [Google Scholar] [CrossRef]
- Census and Statistics Department. The Government of the Hong Kong Special Administrative Region: Table 2: Population Figures from Mid-2002 to Mid-2013. Mid-Year Population for 2013. Available online: http://gia.info.gov.hk/general/201308/13/P201308130528_0528_115779.pdf (accessed on 1 April 2014).
- Bolton, D. The computation of equivalent potential temperature. Mon. Weather Rev. 1980, 108, 1046–1053. [Google Scholar] [CrossRef]
- Tetens, O. Über einige meteorologische Begriffe. Z. Geophys. 1930, 6, 297–309. (In German) [Google Scholar]
- Wong, W.T. Comparison of Algorithms for the Computation of the Thermodynamic Properties of Moist Air. Technical Note; Hong Kong Observatory. 1989. Available online: http://www.weather.gov.hk/publica/tnl/tnl051.pdf (accessed on 26 January 2015). [Google Scholar]
- Chowell, G.; Viboud, C.; Simonsen, L.; Miller, M.; Alonso, W.J. The reproduction number of seasonal influenza epidemics in Brazil, 1996–2006. Proc. R. Soc. B 2010, 277, 1857–1866. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Seasonal Influenza: Clinical Signs and Symptoms of Influenza. Available online: http://www.cdc.gov/flu/professionals/acip/clinical.htm (accessed on 1 April 2014).
- Li, F.C.K.; Choi, B.C.K.; Sly, T.; Pak, A.W.P. Finding the real case-fatality rate of H5N1 avian influenza. J. Epidemiol. Community Health 2008, 62, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Chowell, G.; Miller, M.A.; Viboud, C. Seasonal influenza in the United States, France, and Australia: Transmission and prospects for control. Epidemiol. Infect. 2008, 136, 852–864. [Google Scholar] [PubMed]
- Burnham, K.P.; Anderson, D.R. Model Selection and Multimodel Inference: A Practical Information-Theoretic Approach, 2nd ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Soebiyanto, R.P.; Adimi, F.; Kiang, R.K. Modeling and predicting seasonal influenza transmission in warm regions using climatological parameters. PLoS One 2010, 5. [Google Scholar] [CrossRef] [PubMed]
- Lowen, A.C.; Mubareka, S.; Steel, J.; Palese, P. Influenza virus transmission is dependent on relative humidity and temperature. PLoS Pathog. 2007, 3. [Google Scholar] [CrossRef]
- Lofgren, E.; Fefferman, N.; Naumov, Y.N.; Gorski, J.; Naumova, E.N. Influenza seasonality: Underlying causes and modeling theories. J. Virol. 2007, 81, 5429–5436. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.; Goggins, W.; Yue, J.; Lee, P. Hospital admissions as a function of temperature, other weather phenomena and pollution levels in an urban setting in China. Bull. WHO 2013, 91, 576–584. [Google Scholar] [PubMed]
- Goggins, W.B.; Chan, E.Y.; Yang, C.; Chong, M. Associations between mortality and meteorological and pollutant variables during the cool season in two Asian cities with sub-tropical climates: Hong Kong and Taipei. Environ. Health 2013, 12. [Google Scholar] [CrossRef]
- Shaman, J.; Kohn, M. Absolute humidity modulates influenza survival, transmission, and seasonality. PNAS 2009, 106, 3243–3248. [Google Scholar] [CrossRef] [PubMed]
- Lowen, A.C.; Steel, J.; Mubareka, S.; Palese, P. High temperature (30 ºC) blocks aerosol but not contact transmission of influenza virus. J. Virol. 2008, 82, 5650–5652. [Google Scholar] [CrossRef] [PubMed]
- Soebiyanto, R.P.; Kiang, R. Meteorological parameters as predictors for seasonal influenza. Geocarto Int. 2014, 29, 39–47. [Google Scholar] [CrossRef]
- Soebiyanto, R.P.; Clara, W.; Jara, J.; Castillo, L.; Sorto, O.R.; Marinero, S.; de Antinori, M.E.; McCracken, J.P.; Widdowson, M.A.; Azziz-Baumgartner, E.; Kiang, R.K. The role of temperature and humidity on seasonal influenza in tropical areas: Guatemala, El Salvador and Panama, 2008–2013. PLoS One 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Juzeniene, A.; Ma, L.W.; Kwitniewski, M.; Polev, G.A.; Lagunova, Z.; Dahlback, A.; Moan, J. The seasonality of pandemic and non-pandemic influenzas: The roles of solar radiation and vitamin D. Int. J. Infect. Dis. 2010, 14, 1099e1105. [Google Scholar] [CrossRef]
- Moan, J.; Dahlback, A.; Ma, L.; Juzeniene, A. Influenza, solar radiation and vitamin D. Dermatoendocrinology 2009, 1, 307–309. [Google Scholar] [CrossRef]
- Urashima, M.; Segawa, T.; Okazaki, M.; Kurihara, M.; Wada, Y.; Ida, H. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren. Amer. J. Clin. Nutr. 2010, 91, 1255–1260. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.P.; Stilianakis, N.I. A note on the inactivation of influenza A viruses by solar radiation, relative humidity and temperature. Photochem. Photobiol. 2008, 84, 1601–1602. [Google Scholar] [CrossRef] [PubMed]
- Chong, K.C.; Zee, B.C. Modeling the impact of air, sea, and land travel restrictions supplemented by other interventions on the emergence of a new influenza pandemic virus. BMC Infect. Dis. 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Grais, R.F.; Ellis, J.H.; Glass, G.E. Assessing the impact of airline travel on the geographic spread of pandemic influenza. Eur. J. Epidemiol. 2003, 18, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.T.; Cowling, B.J.; Lau, E.H.; Ip, D.K.; Ho, L.M.; Tsang, T.; Chuang, S.K.; Leung, P.Y.; Lo, S.V.; Liu, S.H.; et al. School closure and mitigation of pandemic (H1N1) 2009, Hong Kong. Emerg. Infect. Dis. 2010, 16, 538–541. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Lau, E.H.Y.; Lam, C.L.H.; Cheng, C.K.; Kovar, J.; Chan, K.H.; Peiris, J.S.; Leung, G.M. Effects of school closures, 2008 winter influenza season, Hong Kong. Emerg. Infect. Dis. 2008, 14, 1660–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serfling, R.E. Methods for current statistical-analysis of excess pneumonia-influenza deaths. Public Health Rep. 1963, 78, 494–506. [Google Scholar]
- Simonsen, L.; Clarke, M.J.; Williamson, G.D.; Stroup, D.F.; Arden, N.H.; Schonberger, L.B. The impact of influenza epidemics on mortality: Introducing a severity index. Amer. J. Public Health 1997, 87, 1944–1950. [Google Scholar] [CrossRef]
- Lo, J.Y.; Tsang, T.H.; Leung, Y.H.; Yeung, E.Y.; Wu, T.; Lim, W.W. Respiratory infections during SARS outbreak, Hong Kong, 2003. Emerg. Infect. Dis. 2005, 11, 1738–1741. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, L.; Fukuda, K.; Schonberger, L.B.; Cox, N.J. The impact of influenza epidemics on hospitalizations. J. Infect. Dis. 2000, 181, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Monto, A.S.; Gravenstein, S.; Elliott, M.; Schweinle, J. Clinical signs and symptoms predicting influenza infection. Arch. Intern. Med. 2000, 160, 3243–3247. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chong, K.C.; Goggins, W.; Zee, B.C.Y.; Wang, M.H. Identifying Meteorological Drivers for the Seasonal Variations of Influenza Infections in a Subtropical City — Hong Kong. Int. J. Environ. Res. Public Health 2015, 12, 1560-1576. https://doi.org/10.3390/ijerph120201560
Chong KC, Goggins W, Zee BCY, Wang MH. Identifying Meteorological Drivers for the Seasonal Variations of Influenza Infections in a Subtropical City — Hong Kong. International Journal of Environmental Research and Public Health. 2015; 12(2):1560-1576. https://doi.org/10.3390/ijerph120201560
Chicago/Turabian StyleChong, Ka Chun, William Goggins, Benny Chung Ying Zee, and Maggie Haitian Wang. 2015. "Identifying Meteorological Drivers for the Seasonal Variations of Influenza Infections in a Subtropical City — Hong Kong" International Journal of Environmental Research and Public Health 12, no. 2: 1560-1576. https://doi.org/10.3390/ijerph120201560