Analysis of a Real-World Cohort of Metastatic Breast Cancer Patients Shows Circulating Tumor Cell Clusters (CTC-clusters) as Predictors of Patient Outcomes

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Counts of CTCs and CTC-Clusters and Association with Clinicopathological Variables
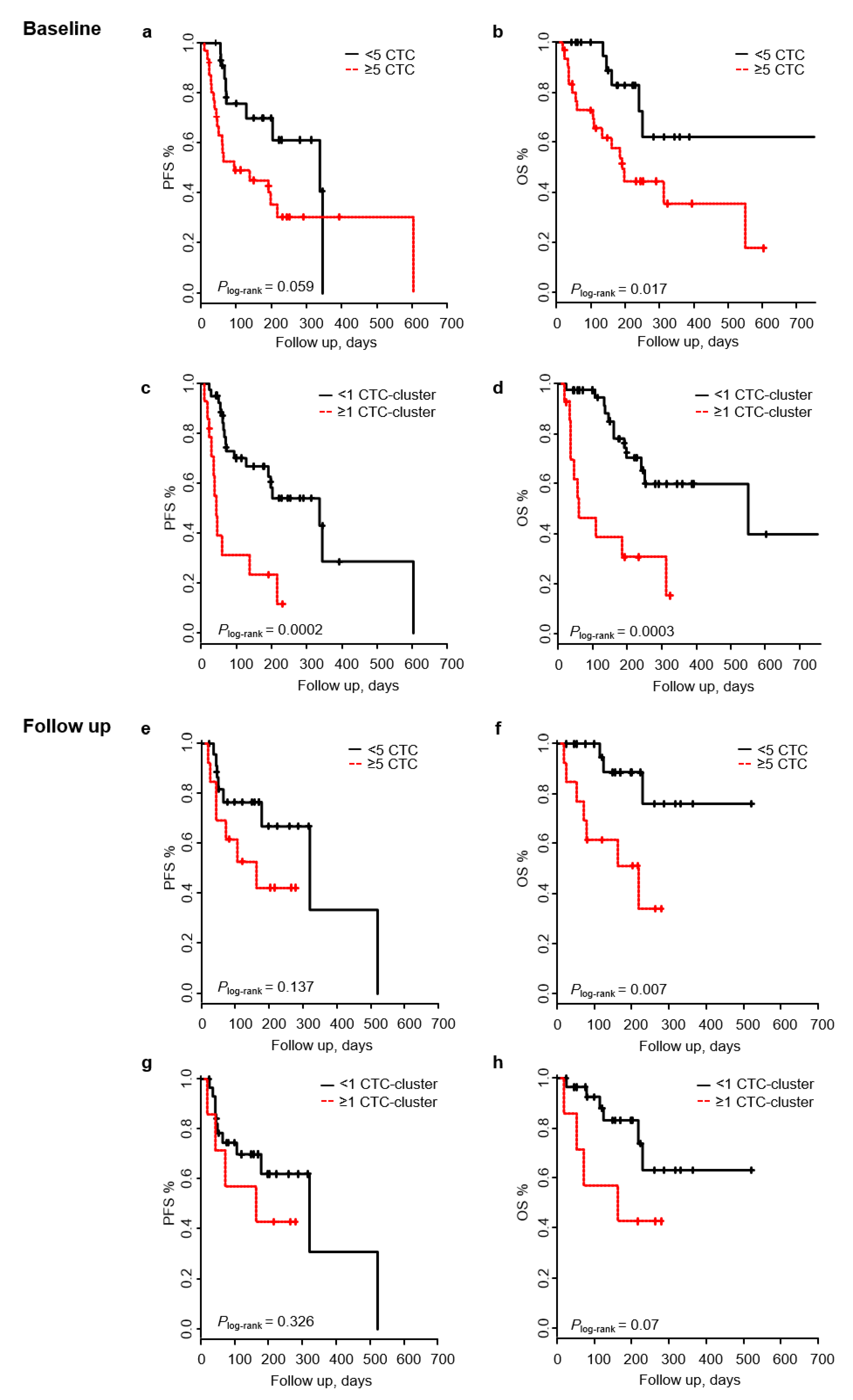
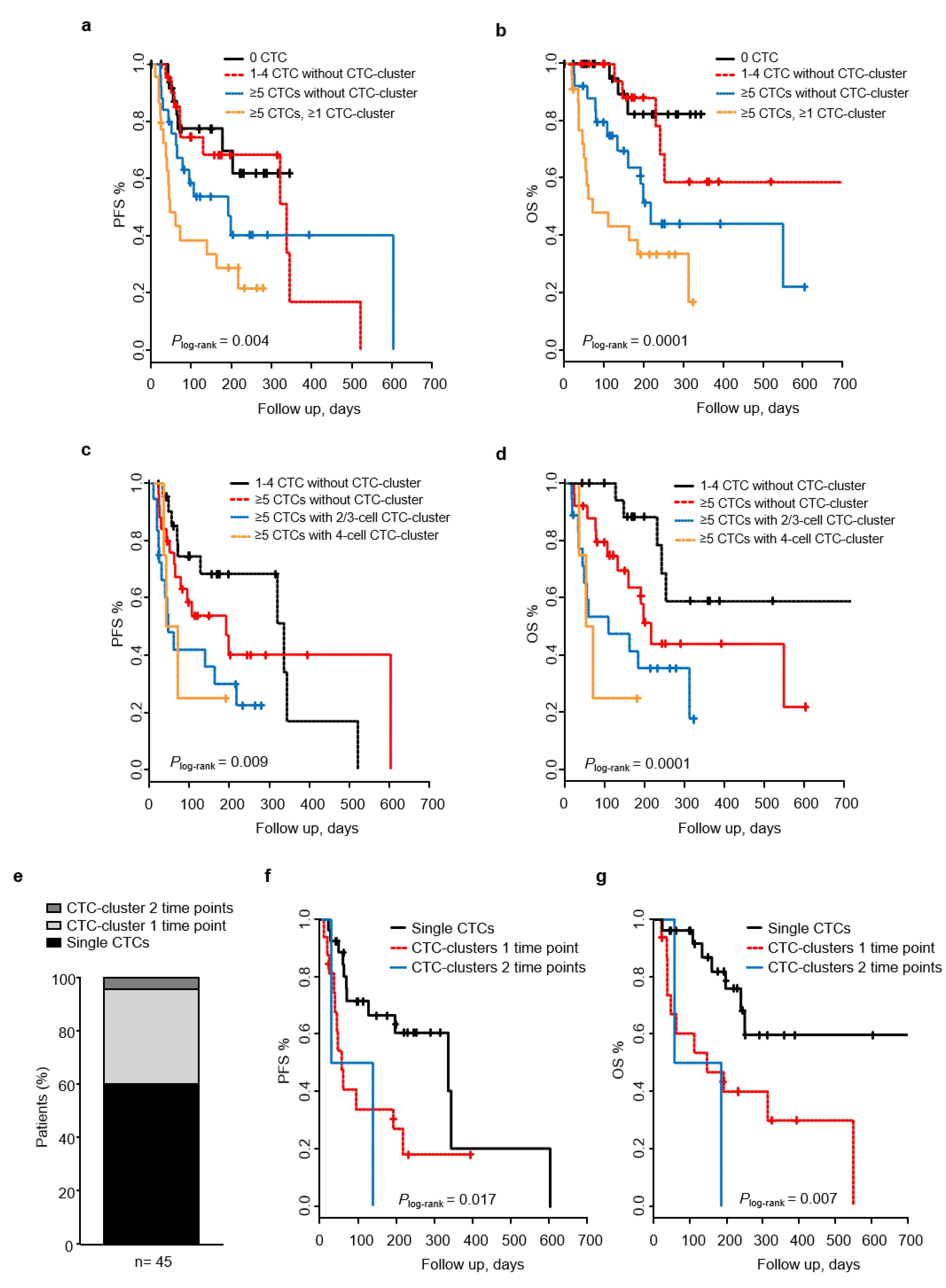
2.3. Presence of CTC-Clusters Predicts Patient Outcome at Baseline
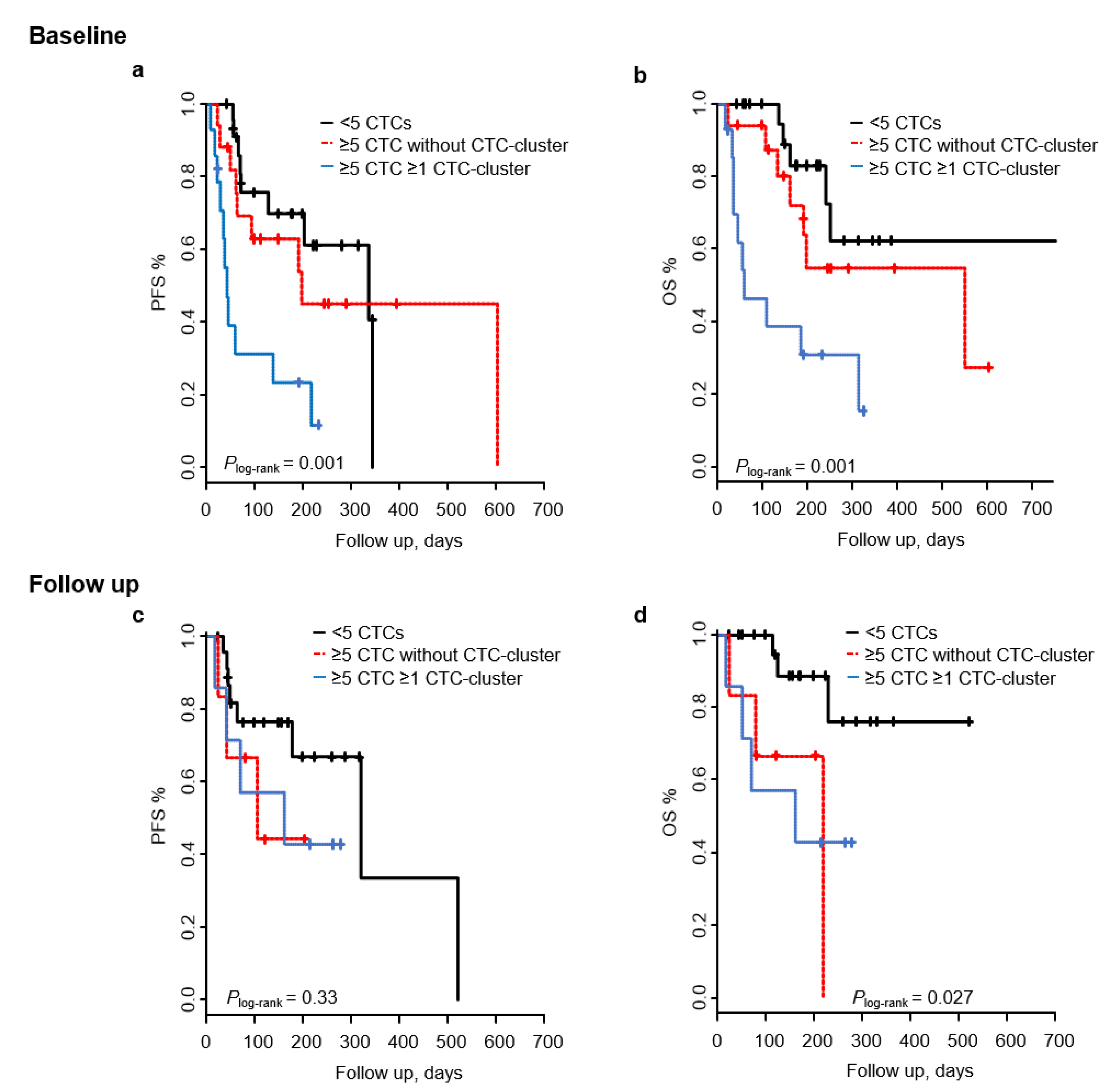
2.4. Joint Analysis of CTCs and CTC-Clusters for Patient Outcome Prediction
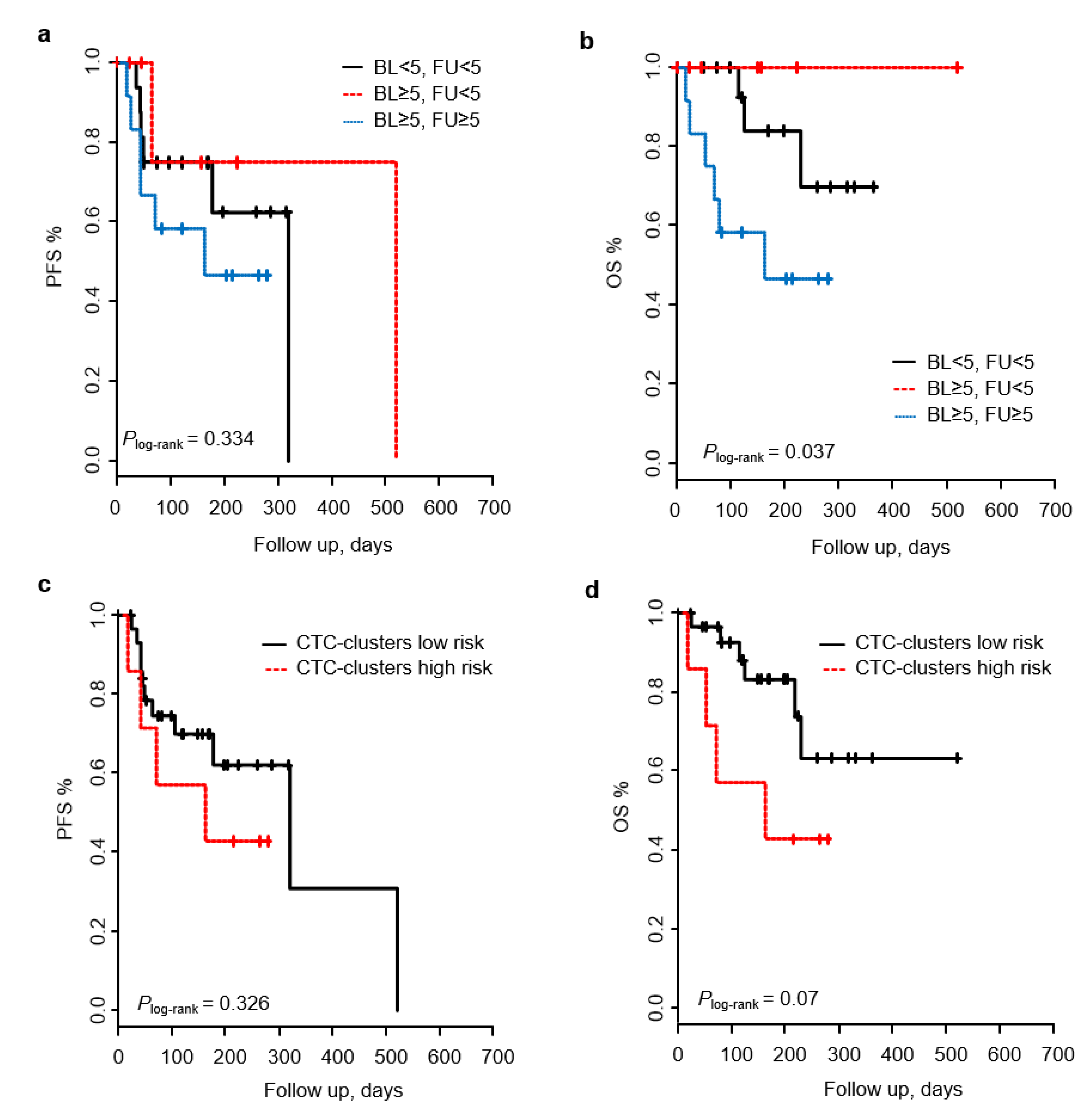
2.5. Patient Outcome Prediction Based on Baseline-to-Follow up Changes of CTCs and CTC-Clusters
2.6. Longitudinal Changes of CTC-Clusters and Cluster Size Predict Patient Outcomes
3. Discussion
4. Materials and Methods
4.1. Study Subjects
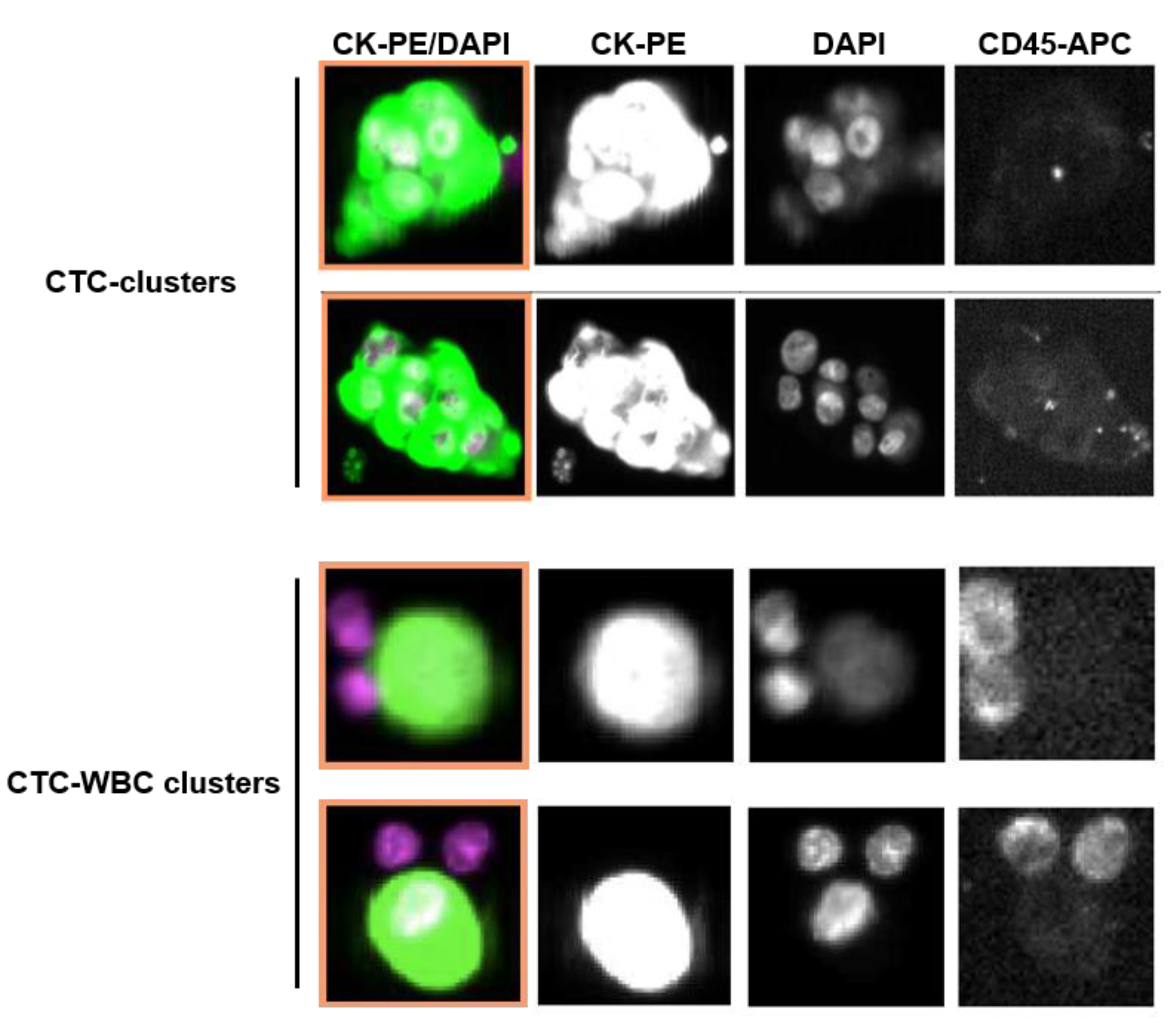
4.2. Enumerations of CTCs and CTC-Clusters
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA A Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redig, A.J.; McAllister, S.S. Breast cancer as a systemic disease: A view of metastasis. J. Intern. Med. 2013, 274, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peitzsch, C.; Tyutyunnykova, A.; Pantel, K.; Dubrovska, A. Cancer stem cells: The root of tumor recurrence and metastases. Semin. Cancer Biol. 2017, 44, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Mathai, R.A.; Vidya, R.V.S.; Reddy, B.S.; Thomas, L.; Udupa, K.; Kolesar, J.M.; Rao, M. Potential Utility of Liquid Biopsy as a Diagnostic and Prognostic Tool for the Assessment of Solid Tumors: Implications in the Precision Oncology. J. Clin. Med. 2019, 8, 373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bidard, F.-C.; Peeters, D.; Fehm, T.; Nolè, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; García-Sáenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Banys-Paluchowski, M.; Krawczyk, N.; Meier-Stiegen, F.; Fehm, T.; Information, P.E.K.F.C. Circulating tumor cells in breast cancer—current status and perspectives. Crit. Rev. Oncol. 2016, 97, 22–29. [Google Scholar] [CrossRef]
- Thery, L.; Meddis, A.; Cabel, L.; Proudhon, C.; Latouche, A.; Pierga, J.-Y.; Bidard, F.-C. Circulating Tumor Cells in Early Breast Cancer. JNCI Cancer Spectr. 2019, 3, pkz026. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Dawood, S.; Broglio, K.; Valero, V.; Reuben, J.; Handy, B.; Islam, R.; Jackson, S.; Hortobagyi, G.N.; Fritsche, H.; Cristofanilli, M. Circulating tumor cells in metastatic breast cancer. Cancer 2008, 113, 2422–2430. [Google Scholar] [CrossRef]
- Nakamura, S.; Yagata, H.; Ohno, S.; Yamaguchi, H.; Iwata, H.; Tsunoda, N.; Ito, Y.; Tokudome, N.; Toi, M.; Kuroi, K.; et al. Multi-center study evaluating circulating tumor cells as a surrogate for response to treatment and overall survival in metastatic breast cancer. Breast Cancer 2009, 17, 199–204. [Google Scholar] [CrossRef]
- Giuliano, M.; Giordano, A.; Jackson, S.; Hess, K.R.; De Giorgi, U.; Mego, M.; Handy, B.C.; Ueno, N.; Alvarez, R.H.; Laurentiis, M.; et al. Circulating tumor cells as prognostic and predictive markers in metastatic breast cancer patients receiving first-line systemic treatment. Breast Cancer Res. 2011, 13, R67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pierga, J.-Y.; Hajage, D.; Bachelot, T.; Delaloge, S.; Brain, E.; Campone, M.; Diéras, V.; Rolland, E.; Mignot, L.; Mathiot, C.; et al. High independent prognostic and predictive value of circulating tumor cells compared with serum tumor markers in a large prospective trial in first-line chemotherapy for metastatic breast cancer patients. Ann. Oncol. 2012, 23, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Yan, W.-T.; Cui, X.; Chen, Q.; Li, Y.-F.; Cui, Y.-H.; Wang, Y.; Jiang, J. Circulating tumor cell status monitors the treatment responses in breast cancer patients: A meta-analysis. Sci. Rep. 2017, 7, 43464. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.C.; Shields, P.G.; Warren, R.D.; Cohen, P.; Wilkinson, M.; Ottaviano, Y.L.; Rao, S.B.; Eng-Wong, J.; Seillier-Moiseiwitsch, F.; Noone, A.-M.; et al. Circulating Tumor Cells: A Useful Predictor of Treatment Efficacy in Metastatic Breast Cancer. J. Clin. Oncol. 2009, 27, 5153–5159. [Google Scholar] [CrossRef] [Green Version]
- Cristofanilli, M.; Hayes, D.F.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Reuben, J.M.; Doyle, G.V.; Matera, J.; Allard, W.J.; Miller, M.C.; et al. Circulating Tumor Cells: A Novel Prognostic Factor for Newly Diagnosed Metastatic Breast Cancer. J. Clin. Oncol. 2005, 23, 1420–1430. [Google Scholar] [CrossRef] [PubMed]
- Paoletti, C.; Li, Y.; Muñiz, M.C.; Kidwell, K.M.; Aung, K.; Thomas, D.G.; Brown, M.E.; Abramson, V.G.; Irvin, W.J.; Lin, N.U.; et al. Significance of Circulating Tumor Cells in Metastatic Triple-Negative Breast Cancer Patients within a Randomized, Phase II Trial: TBCRC 019. Clin. Cancer Res. 2015, 21, 2771–2779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, J.-M.; Krebs, M.; Lancashire, L.; Sloane, R.S.; Backen, A.; Swain, R.K.; Priest, L.J.; Greystoke, A.; Zhou, C.; Morris, K.; et al. Clinical Significance and Molecular Characteristics of Circulating Tumor Cells and Circulating Tumor Microemboli in Patients With Small-Cell Lung Cancer. J. Clin. Oncol. 2012, 30, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.-M.; Krebs, M.; Ward, T.; Sloane, R.S.; Priest, L.; Hughes, A.; Clack, G.; Ranson, M.; Blackhall, F.H.; Dive, C. Circulating Tumor Cells as a Window on Metastasis Biology in Lung Cancer. Am. J. Pathol. 2011, 178, 989–996. [Google Scholar] [CrossRef]
- Molnar, B.; Ladanyi, A.; Tanko, L.; Sréter, L.; Tulassay, Z. Circulating tumor cell clusters in the peripheral blood of colorectal cancer patients. Clin. Cancer Res. 2001, 7, 4080–4085. [Google Scholar]
- Brandt, B.; Junker, R.; Griwatz, C.; Heidl, S.; Brinkmann, O.; Semjonow, A.; Assmann, G.; Zänker, K.S. Isolation of prostate-derived single cells and cell clusters from human peripheral blood. Cancer Res. 1996, 56, 4556–4561. [Google Scholar]
- Kats-Ugurlu, G.; Roodink, I.; De Weijert, M.; Tiemessen, D.; Maass, C.; Verrijp, K.; Van Der Laak, J.; De Waal, R.; Mulders, P.; Oosterwijk, E.; et al. Circulating tumour tissue fragments in patients with pulmonary metastasis of clear cell renal cell carcinoma. J. Pathol. 2009, 219, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Aceto, N.; Bardia, A.; Miyamoto, D.T.; Donaldson, M.C.; Wittner, B.S.; Spencer, J.A.; Yu, M.; Pely, A.; Engstrom, A.; Zhu, H.; et al. Circulating tumor cell clusters are oligoclonal precursors of breast cancer metastasis. Cell 2014, 158, 1110–1122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, K.J.; Padmanaban, V.; Silvestri, V.; Schipper, K.; Cohen, J.D.; Fairchild, A.N.; Gorin, M.A.; Verdone, J.E.; Pienta, K.J.; Bader, J.S.; et al. Polyclonal breast cancer metastases arise from collective dissemination of keratin 14-expressing tumor cell clusters. Proc. Natl. Acad. Sci. USA 2016, 113, E854–E863. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Taftaf, R.; Kawaguchi, M.; Chang, Y.-F.; Chen, W.; Entenberg, D.; Zhang, Y.; Gerratana, L.; Huang, S.; Patel, D.B.; et al. Homophilic CD44 Interactions Mediate Tumor Cell Aggregation and Polyclonal Metastasis in Patient-Derived Breast Cancer Models. Cancer Discov. 2018, 9, 96–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gkountela, S.; Castro-Giner, F.; Szczerba, B.M.; Vetter, M.; Landin, J.; Scherrer, R.; Krol, I.; Scheidmann, M.C.; Beisel, C.; Stirnimann, C.U.; et al. Circulating Tumor Cell Clustering Shapes DNA Methylation to Enable Metastasis Seeding. Cell 2019, 176, 98–112.e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aceto, N.; Toner, M.; Maheswaran, S.; Haber, D.A. En Route to Metastasis: Circulating Tumor Cell Clusters and Epithelial-to-Mesenchymal Transition. Trends Cancer 2015, 1, 44–52. [Google Scholar] [CrossRef]
- Mu, Z.; Wang, C.; Ye, Z.; Austin, L.; Civan, J.; Hyslop, T.; Palazzo, J.P.; Jaslow, R.; Li, B.; Myers, R.E.; et al. Prospective assessment of the prognostic value of circulating tumor cells and their clusters in patients with advanced-stage breast cancer. Breast Cancer Res. Treat. 2015, 154, 563–571. [Google Scholar] [CrossRef]
- Wang, C.; Mu, Z.; Chervoneva, I.; Austin, L.; Ye, Z.; Rossi, G.; Palazzo, J.P.; Sun, C.; Abu-Khalaf, M.; Myers, R.E.; et al. Longitudinally collected CTCs and CTC-clusters and clinical outcomes of metastatic breast cancer. Breast Cancer Res. Treat. 2016, 161, 83–94. [Google Scholar] [CrossRef]
- Jansson, S.; Bendahl, P.-O.; Larsson, A.-M.; Aaltonen, K.E.; Rydén, L. Prognostic impact of circulating tumor cell apoptosis and clusters in serial blood samples from patients with metastatic breast cancer in a prospective observational cohort. BMC Cancer 2016, 16, 433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larsson, A.-M.; Jansson, S.; Bendahl, P.-O.; Jörgensen, C.L.T.; Loman, N.; Graffman, C.; Lundgren, L.; Aaltonen, K.E.; Rydén, L. Longitudinal enumeration and cluster evaluation of circulating tumor cells improve prognostication for patients with newly diagnosed metastatic breast cancer in a prospective observational trial. Breast Cancer Res. 2018, 20, 48. [Google Scholar] [CrossRef] [PubMed]
- Paoletti, C.; Miao, J.; Dolce, E.M.; Darga, E.P.; Repollet, M.I.; Doyle, G.V.; Gralow, J.R.; Hortobagyi, G.N.; Smerage, J.B.; Barlow, W.E.; et al. Circulating Tumor Cell Clusters in Patients with Metastatic Breast Cancer: A SWOG S0500 Translational Medicine Study. Clin. Cancer Res. 2019, 25, 6089–6097. [Google Scholar] [CrossRef] [Green Version]
- Maddipati, R.; Stanger, B.Z. Pancreatic Cancer Metastases Harbor Evidence of Polyclonality. Cancer Discov. 2015, 5, 1086–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topal, B.; Roskams, T.; Fevery, J.; Penninckx, F. Aggregated colon cancer cells have a higher metastatic efficiency in the liver compared with nonaggregated cells: An experimental study. J. Surg. Res. 2003, 112, 31–37. [Google Scholar] [CrossRef]
- Yu, M.; Bardia, A.; Wittner, B.S.; Stott, S.L.; Smas, M.E.; Ting, D.T.; Isakoff, S.J.; Ciciliano, J.C.; Wells, M.N.; Shah, A.M.; et al. Circulating Breast Tumor Cells Exhibit Dynamic Changes in Epithelial and Mesenchymal Composition. Science 2013, 339, 580–584. [Google Scholar] [CrossRef] [Green Version]
- Szczerba, B.M.; Castro-Giner, F.; Vetter, M.; Krol, I.; Gkountela, S.; Landin, J.; Scheidmann, M.C.; Donato, C.; Scherrer, R.; Singer, J.; et al. Neutrophils escort circulating tumour cells to enable cell cycle progression. Nature 2019, 566, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Heeke, S.; Mograbi, B.; Alix-Panabières, C.; Hofman, P. Never Travel Alone: The Crosstalk of Circulating Tumor Cells and the Blood Microenvironment. Cells 2019, 8, 714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprouse, M.L.; Welte, T.; Boral, D.; Liu, H.N.; Yin, W.; Vishnoi, M.; Goswami-Sewell, D.; Li, L.; Pei, G.; Jia, P.; et al. PMN-MDSCs Enhance CTC Metastatic Properties through Reciprocal Interactions via ROS/Notch/Nodal Signaling. Int. J. Mol. Sci. 2019, 20, 1916. [Google Scholar] [CrossRef] [Green Version]
- Moreira, L.L.; Netto, E.M.; Nascimento-Carvalho, C.M. Nosocomial Gastroenteritis in Children With and Without Rotavirus Infection. Pediatr. Infect. Dis. J. 2009, 28, 72. [Google Scholar] [CrossRef]
- Fidler, I.J. The relationship of embolic homogeneity, number, size and viability to the incidence of experimental metastasis. Eur. J. Cancer (1965) 1973, 9, 223–227. [Google Scholar] [CrossRef]
- Thompson, S.C. The Colony Forming Efficiency of Single Cells and Cell Aggregates from a Spontaneous Mouse Mammary Tumour Using the Lung Colony Assay. Br. J. Cancer 1974, 30, 332–336. [Google Scholar] [CrossRef] [Green Version]
- Liotta, L.A.; Kleinerman, J.; Saidel, G.M. Quantitative relationships of intravascular tumor cells, tumor vessels, and pulmonary metastases following tumor implantation. Cancer Res. 1974, 34, 997–1004. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total, n (%) |
|---|---|
| Age (years), mean | 58.5 |
| <65 years | 34 (63.0) |
| ≥65 years | 20 (37.0) |
| Tumor stage | |
| IV | 54 (100.0) |
| Baseline ECOG | |
| 0 | 18 (33.3) |
| 1 | 31 (57.4) |
| 2 | 5 (9.3) |
| Primary tumor NHG | |
| I | 4 (7.4) |
| II | 26 (48.1) |
| II | 15 (27.8) |
| Unknown | 9 (16.7) |
| Breast cancer subtypes | |
| HR+HER2- | 27 (50.9) |
| HER2+ | 11 (20.8) |
| HR-HER2- | 15 (25.8) |
| Unknown | 1 (1.8) |
| Site of metastasis * | |
| Non-visceral | 14 (25.9) |
| Visceral | 40 (74.1) |
| Number of metastatic sites | |
| <3 | 29 (53.7) |
| ≥3 | 25 (46.3) |
| First-line systemic therapy (n = 44) | |
| Chemotherapy | 23 (52.3) |
| Hormonal therapy | 15 (34.1) |
| Target therapy # | 6 (13.6) |
| Other lines (n = 10) | |
| Chemotherapy | 8 (80.0) |
| Hormonal therapy | 1 (10.0) |
| Target therapy # | 1 (10.0) |
| Variable | Total | Events, n (%) | HR (95% CI) | p Value | HR (95% CI) * | p Value * |
|---|---|---|---|---|---|---|
| Baseline | ||||||
| Associated with PFS | ||||||
| CTCs | ||||||
| <5 | 23 | 11 (47.8) | 1.00 | 1.00 | ||
| ≥5 | 31 | 20 (64.5) | 2.11 (0.95–4.70) | 0.0649 | 2.82 (1.15–6.87) | 0.022 |
| CTC-clusters | ||||||
| No | 40 | 18 (45.0) | 1.00 | 1.00 | ||
| Yes | 14 | 11 (78.6) | 3.95 (1.80–8.68) | 0.0006 | 4.46 (1.55–12.8) | 0.005 |
| Associated with OS | ||||||
| CTCs | ||||||
| <5 | 23 | 6 (26.1) | 1.00 | 1.00 | ||
| ≥5 | 31 | 17 (54.8) | 3.15 (1.16–8.55) | 0.024 | 3.33 (1.14–9.73) | 0.027 |
| CTC-clusters | ||||||
| No | 40 | 13 (32.5) | 1.00 | 1.00 | ||
| Yes | 14 | 10 (71.4) | 4.23 (1.8–10.1) | 0.0009 | 6.55 (1.78–23.8) | 0.004 |
| Follow up | ||||||
| Associated with PFS | ||||||
| CTCs | ||||||
| <5 | 25 | 8 (32) | 1.00 | 1.00 | ||
| ≥5 | 13 | 7 (53.8) | 2.3 (0.76–6.7) | 0.15 | 2.39 (0.47–12.04) | 0.29 |
| CTC-clusters | ||||||
| No | 31 | 11 (35.5) | 1.00 | 1.00 | ||
| Yes | 7 | 4 (57.1) | 1.8 (0.55–5.9) | 0.33 | 5.05 (1.24–20.52) | 0.023 |
| Associated with OS | ||||||
| CTCs | ||||||
| <5 | 25 | 3 (12.0) | 1.00 | 1.00 | ||
| ≥5 | 13 | 7 (53.8) | 5.3 (1.4–21) | 0.017 | 9.6 × 1017 (0.0-Inf) | 0.996 |
| CTC-clusters | ||||||
| No | 31 | 6 (19.4) | 1.00 | 1.00 | ||
| Yes | 7 | 4 (57.1) | 3 (0.83–11) | 0.09 | 29.74 (2.55–345.8) | 0.006 |
| Variables | Total | Events, n (%) | HR (95% CI) | p Value | HR (95% CI) * | p Value * |
|---|---|---|---|---|---|---|
| Joint effect of baseline CTC and CTC-clusters | ||||||
| Associated with PFS | ||||||
| <5 CTC without CTC-cluster | 23 | 9 (39.13) | 1.00 | 1.00 | ||
| ≥5 CTC without CTC-cluster | 17 | 9 (52.84) | 1.24 (0.47–3.24) | 0.66 | 1.74 (0.57–5.30) | 0.32 |
| ≥5 CTC, ≥1 CTC-cluster | 14 | 11 (78.57) | 4.34 (1.76–10.6) | 0.0013 | 5.16 (1.68–15.8) | 0.0041 |
| Associated with OS | ||||||
| <5 CTC without CTC-cluster | 23 | 6 (26.1) | 1.00 | 1.00 | ||
| ≥5 CTC without CTC-cluster | 17 | 7 (41.18) | 1.88 (0.59–5.98) | 0.28 | 1.84 (0.50–6.82) | 0.36 |
| ≥5 CTC, ≥1 CTC-cluster | 14 | 10 (71.43) | 5.79 (1.96–17.1) | 0.0014 | 7.79 (1.93–31.4) | 0.0038 |
| Joint effect of first follow up CTC and CTC-clusters | ||||||
| Associated with PFS | ||||||
| <5 CTC without CTC-cluster | 25 | 8 (32.0) | 1.00 | 1 | ||
| ≥5 CTC without CTC-cluster | 6 | 3 (50.0) | 2.3 (0.57–9.27) | 0.24 | 0.61 (0.08–4.53) | 0.635 |
| ≥5 CTC, ≥1 CTC-cluster | 7 | 4 (57.1) | 2.2 (0.62–7.84) | 0.22 | 4.45 (1.01–19.59) | 0.0484 |
| Associated with OS | ||||||
| <5 CTC without CTC-cluster | 25 | 3 (12.0) | 1.00 | 1.00 | ||
| ≥5 CTC without CTC-cluster | 6 | 3 (50) | 5.71 (1.11–29.4) | 0.037 | 1.2 × 1018 (0.0-Inf) | 0.996 |
| ≥5 CTC, ≥1 CTC-cluster | 7 | 4 (57.1) | 5.00 (1.11–22.4) | 0.0353 | 2.4 × 1018 (0.0-Inf) | 0.996 |
| Variables | Total | Events, n (%) | HR (95% CI) | p Value | HR (95% CI) * | p Value * |
|---|---|---|---|---|---|---|
| Baseline CTC to Follow up CTC | ||||||
| Associated with PFS | ||||||
| <5 CTC, <5 CTC | 18 | 6 (33.3) | 1.00 | |||
| ≥5 CTC, <5 CTC | 7 | 2 (28.6) | 0.430 (0.05–3.70) | 0.443 | 15.25 (0.42–553.3) | 0.137 |
| ≥5 CTC, ≥5 CTC | 12 | 6 (50) | 1.82 (0.572–5.82) | 0.308 | 3.09 (0.51–18.64) | 0.217 |
| Associated with OS | ||||||
| <5 CTC, <5 CTC | 18 | 3 (16.7) | 1.00 | |||
| ≥5 CTC, <5 CTC | 7 | 0 (0.0) | 1.67 × 10−8 (0.0-Inf) | 0.998 | 1.45 × 109 (0.0-Inf) | 0.997 |
| ≥5 CTC, ≥5 CTC | 12 | 6 (33.3) | 3.91 (0.97–15.79) | 0.055 | 9.75 × 1017 (0.0-Inf) | 0.999 |
| Baseline CTC-cluster to Follow up CTC-cluster | ||||||
| Associated with PFS | ||||||
| Low risk | 31 | 11 (35.5) | 1.00 | 1.00 | ||
| High risk | 7 | 4 (57.1) | 1.79 (0.55–5.85) | 0.33 | 5.05 (1.245–20.52) | 0.023 |
| Associated with OS | ||||||
| Low risk | 31 | 6 (19.4) | 1.00 | 1.00 | ||
| High risk | 7 | 4 (57.1) | 2.96 (0.83–10.56) | 0.09 | 29.7 (2.55–345.8) | 0.006 |
| Variable | Total | Events, n (%) | HR (95% CI) | p Value | HR (95% CI) * | p Value * |
|---|---|---|---|---|---|---|
| Associated with PFS | ||||||
| No CTC | 28 | 7 (25.0) | 1.00 | 1.00 | ||
| 1–4 CTC without CTC-cluster | 21 | 10 (47.6) | 1.39 (0.52–3.73) | 0.50 | 1.85 (0.62–5.46) | 0.26 |
| ≥5 CTC without CTC-cluster | 25 | 14 (56.0) | 1.82 (0.72–4.62) | 0.20 | 1.87 (0.69–5.05) | 0.21 |
| ≥5 CTC with 2–3 cell CTC-cluster | 18 | 13 (72.2) | 3.97 (1.58–9.97) | 0.0033 | 1.85 (0.34–10.0) | 0.470 |
| ≥5 CTC with ≥4 cell CTC-cluster | 4 | 3 (75.0) | 4.10 (1.05–16.0) | 0.0416 | 6.94 (1.32–36.4) | 0.021 |
| Associated with OS | ||||||
| No CTC | 28 | 3 (10.7) | 1.00 | 1.00 | ||
| 1–4 CTC without CTC-cluster | 21 | 6 (28.7) | 1.59 (0.38–6.70) | 0.52 | 2.62 (0.51–13.3) | 0.24 |
| ≥5 CTC without CTC-cluster | 25 | 12 (48.0) | 4.02 (1.12–14.38) | 0.0321 | 6.05 (1.47–24.8) | 0.01 |
| ≥5 CTC with 2–3 cell CTC-cluster | 18 | 12 (78.6) | 7.25 (2.04–25.74) | 0.0021 | 1.49 (0.13–16.2) | 0.741 |
| ≥5 CTC with ≥4 cell CTC-cluster | 4 | 3 (75) | 12.55 (2.49–63.2) | 0.0021 | 73.73 (8.77–619.4) | 0.00007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, C.; Muinelo-Romay, L.; Cebey-López, V.; Pereira-Veiga, T.; Martínez-Pena, I.; Abreu, M.; Abalo, A.; Lago-Lestón, R.M.; Abuín, C.; Palacios, P.; et al. Analysis of a Real-World Cohort of Metastatic Breast Cancer Patients Shows Circulating Tumor Cell Clusters (CTC-clusters) as Predictors of Patient Outcomes. Cancers 2020, 12, 1111. https://doi.org/10.3390/cancers12051111
Costa C, Muinelo-Romay L, Cebey-López V, Pereira-Veiga T, Martínez-Pena I, Abreu M, Abalo A, Lago-Lestón RM, Abuín C, Palacios P, et al. Analysis of a Real-World Cohort of Metastatic Breast Cancer Patients Shows Circulating Tumor Cell Clusters (CTC-clusters) as Predictors of Patient Outcomes. Cancers. 2020; 12(5):1111. https://doi.org/10.3390/cancers12051111
Chicago/Turabian StyleCosta, Clotilde, Laura Muinelo-Romay, Victor Cebey-López, Thais Pereira-Veiga, Inés Martínez-Pena, Manuel Abreu, Alicia Abalo, Ramón M. Lago-Lestón, Carmen Abuín, Patricia Palacios, and et al. 2020. "Analysis of a Real-World Cohort of Metastatic Breast Cancer Patients Shows Circulating Tumor Cell Clusters (CTC-clusters) as Predictors of Patient Outcomes" Cancers 12, no. 5: 1111. https://doi.org/10.3390/cancers12051111