
Acute Effects of Surgical and FFP2 Face Masks on Physiological Responses and Strength Performance in Persons with Sarcopenia

 , ,
, ,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
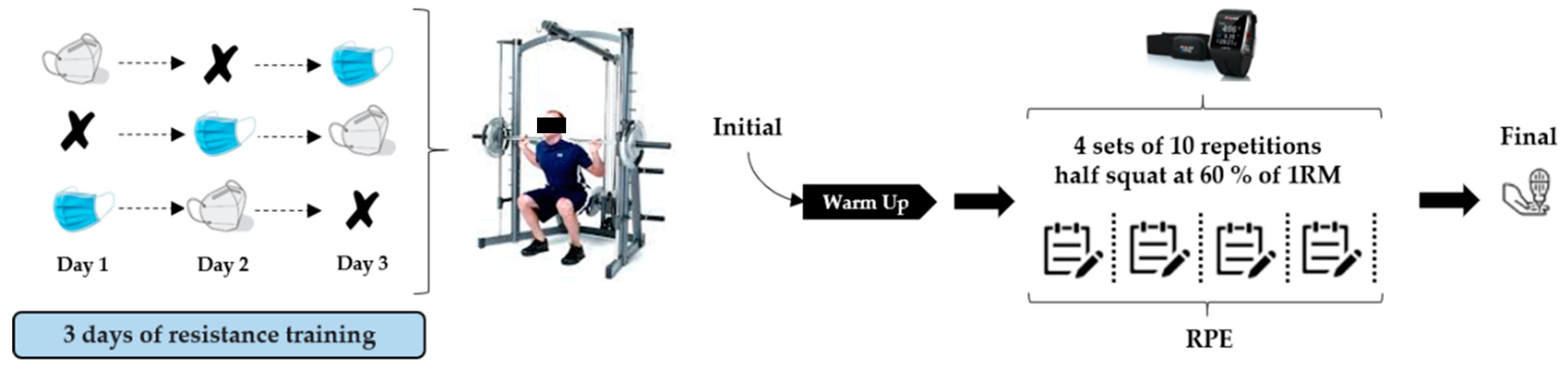
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shafiee, G.; Keshtkar, A.; Soltani, A.; Ahadi, Z.; Larijani, B.; Heshmat, R. Prevalence of sarcopenia in the world: A systematic review and meta- analysis of general population studies. J. Diabetes Metab. Disord. 2017, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Harris-Love, M.O.; Benson, K.; Leasure, E.; Adams, B.; McIntosh, V. The influence of upper and lower extremity strength on performance-based sarcopenia assessment tests. J. Funct. Morphol. Kinesiol. 2018, 3, 53. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloom, I.; Shand, C.; Cooper, C.; Robinson, S.; Baird, J. Diet quality and sarcopenia in older adults: A systematic review. Nutrients 2018, 10, 308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckwée, D.; Delaere, A.; Aelbrecht, S.; Baert, V.; Beaudart, C.; Bruyere, O.; de Saint-Hubert, M.; Bautmans, I. Exercise Interventions for the Prevention and Treatment of Sarcopenia. A Systematic Umbrella Review. J. Nutr. Health Aging 2019, 23, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Cossarizza, A.; De Biasi, S.; Guaraldi, G.; Girardis, M.; Mussini, C. SARS-CoV-2, the Virus that Causes COVID-19: Cytometry and the New Challenge for Global Health. Cytom. Part A 2020, 97, 340. [Google Scholar] [CrossRef] [PubMed]
- González-Sanguino, C.; Ausín, B.; Castellanos, M.Á.; Saiz, J.; López-Gómez, A.; Ugidos, C.; Muñoz, M. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain. Behav. Immun. 2020, 87, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Covid-19 home confinement negatively impacts social participation and life satisfaction: A worldwide multicenter study. Int. J. Environ. Res. Public Health 2020, 17, 6237. [Google Scholar] [CrossRef]
- Alomari, M.A.; Khabour, O.F.; Alzoubi, K.H. Changes in physical activity and sedentary behavior amid confinement: The bksq-covid-19 project. Risk Manag. Healthc. Policy 2020, 13, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- González-Gross, M.; Meléndez, A. Sedentarism, active lifestyle and sport: Impact on health and obesity prevention. Nutr. Hosp. 2013, 28, 89–98. [Google Scholar] [PubMed]
- Arocha Rodulfo, J.I. Sedentarism, a disease from xxi century. Clin. Investig. Arterioscler. 2019, 31, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Carriedo, A.; Cecchini, J.A.; Fernandez-Rio, J.; Méndez-Giménez, A. COVID-19, Psychological Well-being and Physical Activity Levels in Older Adults During the Nationwide Lockdown in Spain. Am. J. Geriatr. Psychiatry 2020, 28, 1146–1155. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D′Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Lesser, I.A.; Nienhuis, C.P. The impact of COVID-19 on physical activity behavior and well-being of canadians. Int. J. Environ. Res. Public Health 2020, 17, 3899. [Google Scholar] [CrossRef]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2020, 1–22. [Google Scholar] [CrossRef]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.D.; MacDougall, C.C.; Johnstone, J.; Copes, R.A.; Schwartz, B.; Garber, G.E. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: A systematic review and meta-analysis. CMAJ 2016, 188, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Scheid, J.L.; Lupien, S.P.; Ford, G.S.; West, S.L. Commentary: Physiological and psychological impact of face mask usage during the covid-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6655. [Google Scholar] [CrossRef]
- Chandrasekaran, B.; Fernandes, S. “Exercise with face mask; Are we handling a devil’s sword?”—A physiological hypothesis. Med. Hypotheses 2020, 144, 110002. [Google Scholar] [CrossRef]
- Fikenzer, S.; Uhe, T.; Lavall, D.; Rudolph, U.; Falz, R.; Busse, M.; Hepp, P.; Laufs, U. Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity. Clin. Res. Cardiol. 2020, 109, 1522–1530. [Google Scholar] [CrossRef] [PubMed]
- Shaw, K.; Butcher, S.; Ko, J.; Zello, G.A.; Chilibeck, P.D. Wearing of cloth or disposable surgical face masks has no effect on vigorous exercise performance in healthy individuals. Int. J. Environ. Res. Public Health 2020, 17, 8110. [Google Scholar] [CrossRef]
- Epstein, D.; Korytny, A.; Isenberg, Y.; Marcusohn, E.; Zukermann, R.; Bishop, B.; Minha, S.; Raz, A.; Miller, A. Return to training in the COVID-19 era: The physiological effects of face masks during exercise. Scand. J. Med. Sci. Sport. 2020, 31, 70–75. [Google Scholar] [CrossRef]
- Garnacho-Castaño, M.V.; Dominguez, R.; Maté-Muñoz, J.L. Understanding the meaning of lactate threshold in resistance exercises. Int. J. Sports Med. 2015, 36, 371–377. [Google Scholar]
- Albesa-Albiol, L.; Serra-Payá, N.; Garnacho-Castaño, M.A.; Cano, L.G.; Cobo, E.P.; Maté-Muñoz, J.L.; Garnacho-Castaño, M.V. Ventilatory efficiency during constant-load test at lactate threshold intensity: Endurance versus resistance exercises. PLoS ONE 2019, 14, e0216824. [Google Scholar] [CrossRef] [Green Version]
- Garnacho-Castaño, M.V.; Albesa-Albiol, L.; Serra-Payá, N.; Bataller, M.G.; Felíu-Ruano, R.; Cano, L.G.; Cobo, E.P.; Maté-Muñoz, J.L. The slow component of oxygen uptake and efficiency in resistance exercises: A comparison with endurance exercises. Front. Physiol. 2019, 10, 357. [Google Scholar] [CrossRef] [PubMed]
- Andre, T.L.; Gann, J.J.; Hwang, P.S.; Ziperman, E.; Magnussen, M.J.; Willoughby, D.S. Restrictive breathing mask reduces repetitions to failure during a session of lower-body resistance exercise. J. Strength Cond. Res. 2018, 32, 2103–2108. [Google Scholar] [CrossRef]
- Motoyama, Y.; Joel, G.; Pereira, P.; Esteves, G.; Azevedo, P. Airflow-Restricting Mask Reduces Acute Performance in Resistance Exercise. Sports 2016, 4, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagim, A.R.; Dominy, T.A.; Camic, C.L.; Wright, G.; Doberstein, S.; Jones, M.T.; Oliver, J.M. Acute effects of the elevation training mask on strength performance in recreational weight lifters. J. Strength Cond. Res. 2018, 32, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Campo, D.J.; Rubio-Arias, J.A.; Dufour, S.; Chung, L.; Ávila-Gandía, V.; Alcaraz, P.E. Biochemical responses and physical performance during high-intensity resistance circuit training in hypoxia and normoxia. Eur. J. Appl. Physiol. 2017, 117, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Delgado-Moreno, R.; González, B.; Ortega, J.; Ramos-Campo, D.J. Amateur endurance triathletes’ performance is improved independently of volume or intensity based training. Physiol. Behav. 2019, 205, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Fernandes, R.J.; Arroyo-Toledo, J.J.; Figueiredo, P.; González-Ravé, J.M.; Vilas-Boas, J.P. Autonomic adaptation after traditional and reverse swimming training periodizations. Acta Physiol. Hung. 2015, 102, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Jidovtseff, B.; Harris, N.K.; Crielaard, J.M.; Cronin, J.B. Using the load-velocity relationship for 1RM prediction. J. Strength Cond. Res. 2011, 25, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.; Hassmén, P.; Lagerström, M. Perceived exertion related to heart rate and blood lactate during arm and leg exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1987, 56, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Roberge, R.J.; Coca, A.; Williams, W.J.; Powell, J.B.; Palmiero, A.J. Physiological impact of the n95 filtering facepiece respirator on healthcare workers. Respir. Care 2010, 55, 569–577. [Google Scholar] [PubMed]
- De La Cruz Torres, B.; López, C.L.; Orellana, J.N. Analysis of heart rate variability at rest and during aerobic exercise: A study in healthy people and cardiac patients. Br. J. Sports Med. 2008, 42, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Gastin, P.B. Energy system interaction and relative contribution during maximal exercise. Sport. Med. 2001, 31, 725–741. [Google Scholar] [CrossRef]
- Gentil, P.; De Lira, C.A.B.; Souza, D.; Jimenez, A.; Mayo, X.; De Fátima Pinho Lins Gryschek, A.L.; Pereira, E.G.; Alcaraz, P.; Bianco, A.; Paoli, A.; et al. Resistance Training Safety during and after the SARS-Cov-2 Outbreak: Practical Recommendations. BioMed Res. Int. 2020, 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- da Silveira, M.P.; da Silva Fagundes, K.K.; Bizuti, M.R.; Starck, É.; Rossi, R.C.; de Resende e Silva, D.T. Physical exercise as a tool to help the immune system against COVID-19: An integrative review of the current literature. Clin. Exp. Med. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Without Mask | Surgical Mask | FFP2 Mask | F | p | η2 | |
|---|---|---|---|---|---|---|
| Session Mean | 0.396 | 0.387 | 0.391 | 0.138 | 0.918 | 0.005 |
| Velocity (m/s) | (0.042) | (0.037) | (0.042) | |||
| Session Peak | 0.771 | 0.771 | 0.760 | 0.335 | 0.846 | 0.009 |
| Velocity (m/s) | (0.090) | (0.080) | (0.086) | |||
| Session Mean | 422.68 | 412.96 | 415.72 | 0.089 | 0.957 | 0.002 |
| Power (W) | (84.20) | (85.16) | (96.53) | |||
| Session Peak | 881.95 | 886.32 | 862.56 | 0.427 | 0.808 | 0.011 |
| Power (W) | (197.40) | (186.40) | (217.26) | |||
| Session Mean | 1070.52 | 1067.87 | 1077.56 | 0.008 | 0.992 | 0.002 |
| Force (N) | (151.95) | (155.33) | (222.21) | |||
| Session Peak | 1282.98 | 1294.92 | 1283.16 | 0.014 | 0.986 | 0.007 |
| Force (N) | (199.17) | (203.85) | (240.00) | |||
| RPE (a.u.) | 4.12 | 4.29 | 4.46 | 0.697 | 0.508 | 0.059 |
| (0.61) | (0.60) | (0.88) | ||||
| Lac (mmol/L) | 4.17 | 5.28 | 4.49 | 0.833 | 0.447 | 0.073 |
| (1.89) | (2.07) | (2.45) |
| Variable | Without Mask | Surgical Mask | FFP2 Mask | F | p | η2 |
|---|---|---|---|---|---|---|
| Mean HR (bpm) | 123.46 | 120.54 | 117.92 | 0.760 | 0.479 | 0.040 |
| (17.37) | (11.14) | (10.54) | ||||
| Peak HR (bpm) | 160.92 | 161.08 | 157.89 | 0.436 | 0.652 | 0.078 |
| (21.07) | (17.68) | (10.84) | ||||
| RMSSD (ms) | 37.69 | 30.53 | 30.40 | 0.532 | 0.594 | 0.030 |
| (21.07) | (16.58) | (21.81) | ||||
| SDNN (ms) | 66.93 | 59.85 | 69.02 | 0.629 | 0.542 | 0.015 |
| (27.78) | (17.83) | (26.80) | ||||
| LnRMSSD (ms) | 3.47 | 3.24 | 3.14 | 0.824 | 0.451 | 0.030 |
| (0.60) | (0.68) | (0.80) | ||||
| pNN50 (%) | 13.23 | 9.42 | 9.92 | 0.437 | 0.651 | 0.041 |
| (12.28) | (7.94) | (10.44) | ||||
| Mean RR (ms) | 503.79 | 513.24 | 526.51 | 0.573 | 0.571 | 0.050 |
| (63.79) | (48.10) | (46.48) | ||||
| Total Power (ms2) | 1902.64 | 992.47 | 2353.68 | 1.275 | 0.302 | 0.018 |
| (2571.40) | (1059.86) | (3845.95) | ||||
| LF/HF | 0.98 | 1.47 | 1.67 | 5.47 | 0.065 | 0.144 |
| (0.56) | (0.99) | (0.67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramos-Campo, D.J.; Pérez-Piñero, S.; Muñoz-Carrillo, J.C.; López-Román, F.J.; García-Sánchez, E.; Ávila-Gandía, V. Acute Effects of Surgical and FFP2 Face Masks on Physiological Responses and Strength Performance in Persons with Sarcopenia. Biology 2021, 10, 213. https://doi.org/10.3390/biology10030213
Ramos-Campo DJ, Pérez-Piñero S, Muñoz-Carrillo JC, López-Román FJ, García-Sánchez E, Ávila-Gandía V. Acute Effects of Surgical and FFP2 Face Masks on Physiological Responses and Strength Performance in Persons with Sarcopenia. Biology. 2021; 10(3):213. https://doi.org/10.3390/biology10030213
Chicago/Turabian StyleRamos-Campo, Domingo Jesús, Silvia Pérez-Piñero, Juan Carlos Muñoz-Carrillo, Francisco Javier López-Román, Esther García-Sánchez, and Vicente Ávila-Gandía. 2021. "Acute Effects of Surgical and FFP2 Face Masks on Physiological Responses and Strength Performance in Persons with Sarcopenia" Biology 10, no. 3: 213. https://doi.org/10.3390/biology10030213