AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2692-9406/075
*Corresponding Author: Jesan Zaman, Division of Cardiology, Department of Internal Medicine, University of South Alabama.
Citation: J Zaman, A Amritphale, C Malozzi, N Amritphale, M Sehgal. (2021) Costs and predictors of early readmissions in patients with Infective Endocarditis. Utilizing the Nationwide Readmission Database. Biomedical Research and Clinical Reviews. 4(3); DOI: 10.31579/2692-9406/075
Copyright: © 2021 Jesan Zaman, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
# Co-first authors; contributed equally to all aspects of the research.
Received: 02 July 2021 | Accepted: 13 July 2021 | Published: 16 July 2021
Keywords: aha guidelines; infective endocarditis; unplanned readmissions; nationwide readmission database
BACKGROUND: There have been previous studies detailing the variables involved in readmissions in patients with a primary admission diagnosis of infective endocarditis – however those studies were done prior to the 2015 change in AHA guidelines and introduction to ICD-10 codes.
OBJECTIVES:
The aim of this study was to describe the frequency, causes, factors, and costs associated with infective endocarditis encounters.
METHODS:
Utilizing the 2017 national readmission database (NRD), we identified all patients that were admitted with infective endocarditis. These patients were evaluated for the rates, predictors, and costs of unplanned 30 days readmissions. Weighted analysis was performed to obtain nationally representative data.
RESULTS:
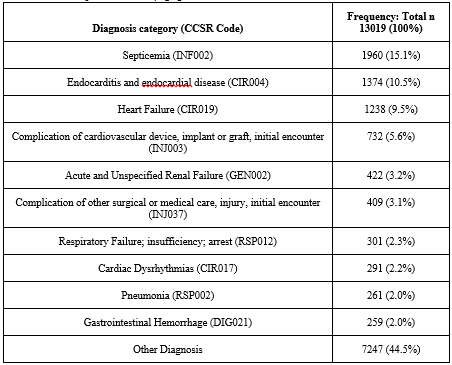
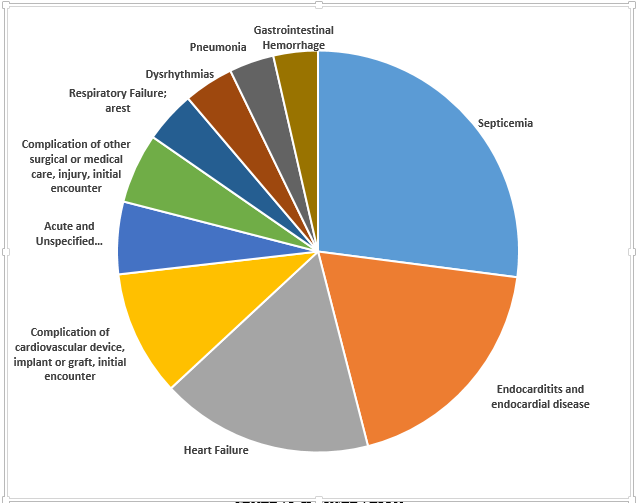
56,357 patients were identified to have been admitted with a diagnosis of infective endocarditis of whom 13,004 patients (23%) were readmitted within 30 days of the index discharge. The most common causes of readmission were septicemia (15.1%), endocarditis and endocardial disease (10.5%), heart failure (9.5%), and complication of cardiovascular device, implant or graft, initial encounter (5.6%). Data showed that there were certain comorbidities that resulted in a higher risk of being readmitted, these include chronic kidney disease, COPD, tobacco use, and hepatic failure. Cost of readmissions per patient was approximately $22,059 (IQR $11,630 - $49,964).
CONCLUSIONS:
Thirty-day unplanned readmissions remain a significant issue affecting nearly 1 in 6 patients with infective endocarditis. This is associated with significant mortality and financial burden. Multi-disciplinary approach may help decrease readmissions, reduce complications, and improve overall outcomes as well as the overall quality of life of our patients.
NRD Nationwide Readmission Database
IE Infective Endocarditis
IQR Interquartile Ratio
AHA American Heart Association
IVDU Intravenous Drug Use
ICD International Classification of Diseases
CMS Centers for Medicare & Medicaid Services
CCSR Clinical Classification Software refined
APR-DRG All Patient Refined-Diagnosis Related Group
Despite a low incidence rate of 3-10 individuals per 100 person-years, infection of the endocardium and/or heart valves, known as Infective Endocarditis (IE) is a potentially lethal process associated with significant mortality and morbidity [1].
The mortality rate of IE is alarmingly high as detailed in a prior study with in-hospital rates of up to 20% and a 1-year mortality rate of up to 40% [1]. In addition, patients with IE were found to be at a higher risk for unplanned readmissions, a study by Aggarwal et al (2020) conducted over 6 years period, consisting of 187,438 patients with a primary diagnosis of IE, showed 24% of patients were readmitted within 30 days. Over half of the re-admissions (51%) occurred within the first 11 days of discharge [2]. Various factors have been implicated to achieve a better prognosis for IE patients ranging from early diagnosis and initiation of treatment, to different combinations or medical therapy, and surgical intervention during index admission; however, they require reevaluation to represent current practice patterns due to recent changes in the IE guidelines in relation to diagnosis, antimicrobial therapy, and management of complications [3].
With the advent of ICD-10, the complexity of diagnosis/coding has increased multi-fold, which provides greater specificity to the research and more ability to pinpoint factors that may alter management [4]. This in addition to updated practice patterns with updated society guidelines, we evaluated large real-world data from the Nationwide Readmissions Database (NRD), to understand comorbidities and predictors associated with early unplanned readmissions in patients discharged with IE.
We followed the direction of previous well-conceived studies using the database that have evaluated the risks of readmissions in patients with carotid stenting and pediatric sepsis [20, 21]
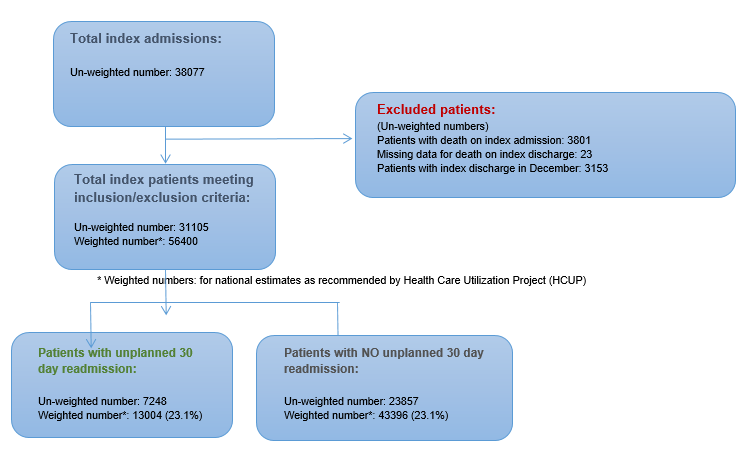
The NRD is a national representative sample of all-age, all-payer discharges from U.S. nonfederal hospitals which comes from the Agency of Healthcare Research and Quality. It contains data from 28 geographically dispersed states across the U.S. It has about 18 million discharges from the year 2017 (Weighted estimated to roughly 36 million discharges). To be fair however we have presented a flowchart in Figure 3 that gives the unweighted numbers. The NRD holds full information on both primary hospitalization and following readmissions within the states. In this study we utilized the data that represents 60% of the U.S. population and 58.2% of all U.S. hospitalizations.
Within 2017, hospitalizations and rehospitalizations were determined using a de-identified unique patient linkage number assigned to each patient, which let us track them across hospitals within a state. Each patient was assigned up-to 40 diagnosis codes and 25 procedure codes for each hospitalization. Often times a diagnosis established when a patient, presents is based on initial symptoms and then the overall main diagnosis of infective endocarditis is subsequently discovered during the actual course of admission. There is no way to tell which was the initial diagnosis and thus up to 40 diagnosis codes were utilized in our study. Additionally, patient information is note carried on from year to year and so it is counted as a new patient/diagnosis; patients cannot be tracked across years. Patients that had elective admissions were also not counted as an unplanned readmission. We also wanted to ensure that regarding readmission it was not just a short 1-night admission to ensure follow up, and this is taken care of because the NRD only captures patients that have inpatient status, not observation which is less than 24hrs. The University of South Alabama Institutional Review Board (IRB) approved the study for an exempt status.
We defined infective endocarditis with the procedure codes from ICD-10 as seen in Appendix Online Table 1. The primary outcome was first unplanned readmission after being diagnosed with infective endocarditis during the year 2017. Even if a patient had multiple such admissions in a year, we only used the first encounter for the analysis. Patients admitted in December were excluded as they may not have 30 days of follow-up, leading to immortal time bias. In addition, any patient that died during the initial hospitalization or had missing data were excluded.
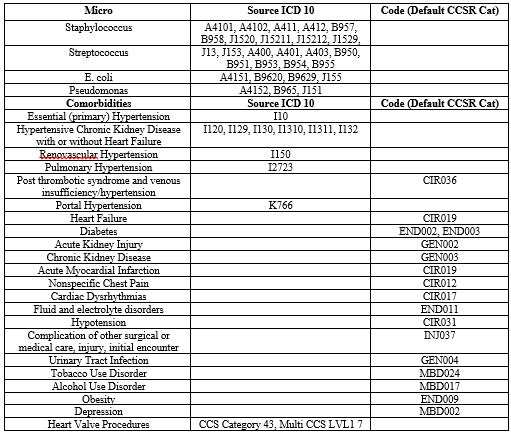

ICD-10 codes were used to define pertinent clinical variables. Data on status of hospital being teaching or non-teaching, urban or rural, the control/ownership, and even hospital bed sizes were collected. We performed a cost analysis by analyzing data on index admission length of stay (days), index admission cost (U.S.$), discharge destination to home/self-care, transfer to other hospital, care home, discharge against medical advice, on primary expected payer, quartile of median household income, readmission length of stay (days), readmission charges & costs (U.S.$), and readmission death. We multiplied the hospital charges with the Agency for Healthcare Research and Quality’s all-payer cost-to-charge ratios to determine costs. The first diagnosis on the basis of Clinical Classification Software codes (CCSR) determined the causes of readmission. All ICD-10 and CCSR codes used in this study are presented in the appendix section.
Statistical analysis was performed using IBM SPSS Statistics for Windows, version 1.0.0.118 (IBM Corp., Armonk, N.Y., USA). We used 2-sided tests with a significance level of 0.05 for statistical analysis. We examined baseline characteristics of participants and tested for statistical differences using the Pearson Chi Square test for categorical variables and Mann-Whitney U-Test for continuous variables with no readmission as the reference group. To determine the predictors of readmission within each time period with adjustments for all variables except the elective variable we utilized multivariable logistic regressions.
Population Characteristics and Descriptive Results
30,413,839 patient encounters from January through December 2017 among hospitalized patients 18 years of age and older were included in the NRD. We identified those patients diagnosed with infective endocarditis using a weighted analysis. After index admission went infective endocarditis, 13,004 (23%) patients had an unplanned 30-day readmission.
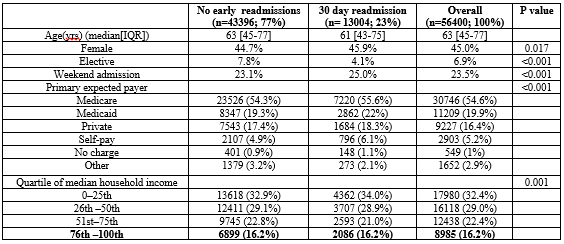
General population and hospital data can be found in Tables 1 and 2. The median length of days of readmission was 10 days (IQR 5 to 18). 9.2% of the total and admission population received valvular surgery and among those readmitted, 7.7% received valvular surgery. The most common pathogen on readmission was Staphylococcus with 25.4%, followed by streptococcus which made up about 8%. Compared with the patients who were not readmitted within 30 days, those readmitted were more likely to have comorbidities chronic kidney disease, COPD, and tobacco use disorder. Additionally, those who received valvular surgery (95.7% of patients that got valve surgery received it during index admission) were less likely to have been readmitted according to our data with a odds ratio of 0.73 (0.67-0.80, P<0>

Cost analysis and length of stay results
The median hospital costs of index encounters were $20,241 [IQR $10,280 – $45,184]. The median length of stay for index admission and readmission encounters were 9 days (IQR 5-18 days) and 10 days (IQR 5-18 days, P<0>
Due to a change in infective endocarditis guidelines in 2015 we decided to reassess the quality of hospital care and performance utilizing 30 day readmissions in the year of 2017 as a metric. In this study we found that unplanned 30 day readmission rate after a primary diagnosis of infective endocarditis was 23%. This was relatively similar to the rates after primary diagnosis of cardiac dysrhythmias (16.73%), Urinary tract infections (18.31%), and acute myocardial infarction (19.66%). The condition with the highest percentage of readmissions was congestive heart failure at 28.05 % [5]. A previous study analyzing patients with infective endocarditis after discharge, reported slightly higher rates of readmissions at about 24.8% [1]. This indicates a slight positive trend in treatment that may have occurred due to the change in guidelines in 2015, however readmission statistics are still a concern, and risk factors should be evaluated to decrease the rate further, to alleviate hospital costs. Studies have also shown that most readmissions occurred within the period immediately after discharge, and nearly 1 in 12 patients died during those events which further emphasize a need to focus on early prevention and intervention on the risk factors and comorbidities that were highlighted in our study [1]. Table 4 details the comorbidities and procedure related factors during index admissions for infective endocarditis.
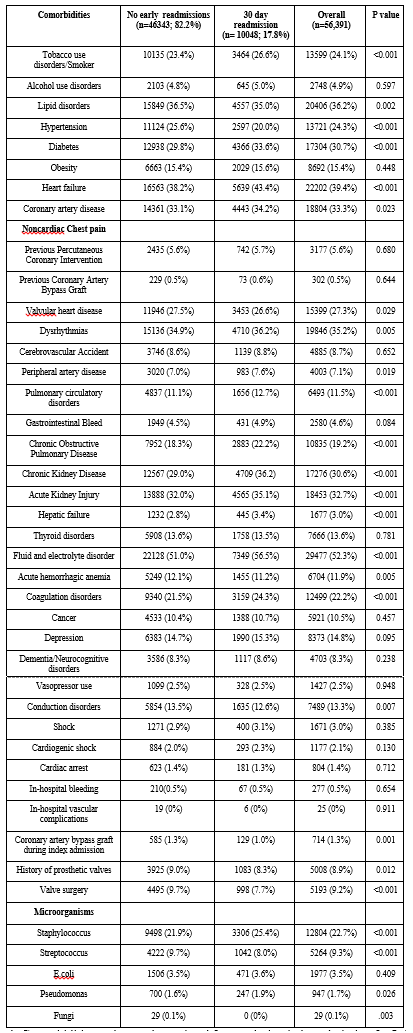
The AHA study showed that the most common diagnosis was endocarditis itself, however the most common cause of readmission for infective endocarditis within 30 days in our study was a primary diagnosis of septicemia, followed by heart failure and then endocarditis1. Our study also found that chronic kidney disease had the highest odds of readmission compared to any other comorbidity despite only accounting for 1.9% of readmission (not even making the top 10 causes for readmission). An elevated serum creatinine in a past study was associated with higher mortality as it can reflect other issues systematically [6]. All of this including the results from table 5 and figure 2 shows the importance of focusing on comorbidities and appropriately managing those risk factors that may be associated with readmission, these selected variables were also chosen based on clinical importance. Considering sepsis was the most common primary diagnosis on readmission suboptimal antibiotic treatment may have been a variable involved. A study showed that although there seemed to be an increased incidence of sepsis over time, it was in fact due to increasing clinical awareness of sepsis, more screening, lower diagnostic thresholds, and better coding practices, with all of that in mind, the sepsis incidence and mortality rate has been relatively stable over the last decade [7]. Something to note is that treatment guidelines are not always followed in real life and therefore the index admissions are very short, and many patients are readmitted with sepsis and thus having severe financial consequences on the entire system. Additionally, a higher focus on patients with chronic kidney disease could help decrease their added risk of being readmitted as well. Outpatient parenteral antibiotic treatment (OPAT) may be the reason for the relatively short median admission time for the index hospitalization (9 days). Being able to conduct further studies to specifically track these concerns would be greatly influential. According to the new guidelines from 2015, an antibiotic treatment period of about four weeks or greater was considered appropriate [8,3], changes such as a trend to stop or reduce Gentamicin use, optimization of Vancomycin troughs, recommendations to utilize Daptomycin due to being superior to Vancomycin for MSSA and MRSA were all important in improvement of management. Given the data we collected is from 2017, further trials are needed to evaluate duration of therapy and need for follow up of cultures/ inflammatory markers. In our study, Staphylococcus was the most common microorganism found in approximately 25.4% of readmissions. This could also be due to inadequate antibiotic management or increased resistance. A study also detailed how the United States has the highest incidence of infective endocarditis in the world at 15 per 100,000 people, which could be attributed to better detection and easy availability to blood cultures and echocardiography, most likely due to an increase in the aging population as well as intravenous drug abuse (staphylococcus is well known to be one of the most common microbes to be found when a patient has a history of IVDU) [9].
We also aimed to find which variables had higher odds of readmission in comparison to others as shown in table 6 and figure 1. There was a variable that led to a significant decrease in odds of readmission which was valvular surgery. Even amongst readmitted patients, 7.9% of them received valve surgery. There was also an element of selection bias because surgery was obviously not an option in high risk patients even when indicated. This issue was also of concern in prior studies and considering similar results in data, there could be an argument to further weigh the risks and benefits of a more aggressive approach to valve surgery even in high risk patients. The 2015 AHA guideline promotes surgical intervention during index admission with congestive heart failure being the most common indication for it [1]. Early surgery within 48 hours was compared in a recent trial to delayed surgery during the remainder of the hospital admission or follow up, which showed that those who underwent early surgery had a lower rate of death, embolic event, or reoccurrence of infective endocarditis at six months [10]. A recent meta-analysis also showed patients with infective endocarditis that had surgery within the first week had a lower risk of mortality [11]. All of this recent data suggests that there could be an argument to adjust the 2015 guidelines to push for more aggressive and earlier surgical intervention within the 1st few days of admission.

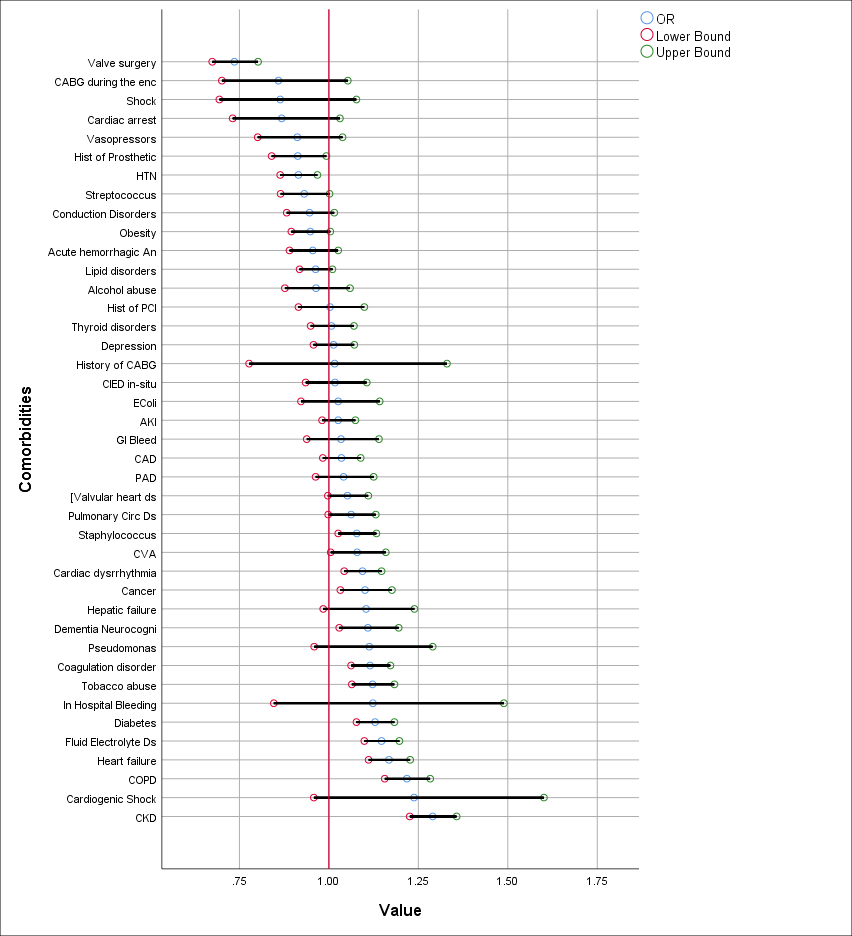
Of note there were several comorbidities that were independent predictors of 30 day readmission after infective endocarditis. Considering the symptoms of IE can be so variable initially and clinically similar to other infectious processes, that can contribute to significant complications such as embolization and heart failure [12, 13, 14]. It is important to be able to properly differentiate all of the signs and symptoms and attribute them to the correct etiology. Other than the already mentioned CHF, diabetes mellitus was present as a comorbidity in 33.6% of readmissions (29.8% in no readmissions, P<0>
Previous studies did not note tobacco use disorder and fluid and electrolyte disorders to be significance when it came to readmissions, however since the new guidelines and the latest data from 2017 we have concluded that they are indeed significant risk factors for readmission and should be critically assessed during discharge planning. Previous studies have also noted depression (increased odds of readmission) to be of significance, but we found that it did not, although it was a present as a comorbidity in 15.3% of readmissions. Finally, factors such as chronic kidney disease, COPD, hepatic failure, heart failure, coagulopathy, diabetes were all noted to be of significant risk factors in prior studies as well as ours [1]. The idea that these comorbidities (that in itself are associated with poor outcomes), irrespective of infectious diseases entity, show also a poor outcome in infective endocarditis, and hence, a higher likelihood for readmission is not novel idea, however we hope that by presenting more data and evidence, it can lead to more studies and further research to help reduce readmissions as it is still a problem.
While health care costs remain one of the biggest problems in the United States, an effort to decrease the financial strain that comes with readmissions should be of primary focus. A study noted that the U.S. spent approximately twice as much as other high income countries on healthcare [19]. The initial median admission duration from our data lasted approximately 9 days, while median readmission number was 10 days (IQR, 5-18). Essentially, we are spending more money (median, $22,059) when a patient is readmitted than on their initial admission (median, $20,241). While quick discharges have always been a motivation for hospital systems, physicians must reanalyze their assessment and plans in coherence with administration to evaluate if early discharge indeed helps financial burden overall and if early follow up may help mitigate overall costs. Additionally, a more specific and critical individualized follow up within the first few days after discharge may be considered and prediction scores be developed to help with such interventions. More work is necessary to increase awareness about infective endocarditis and factors associated with worse outcomes using social media, YouTube and Smart Phone applications as have been done for other disease conditions in the past [22, 23].
Further research should follow on the lines of using artificial intelligence and the deep neural network to identify unidentified associations as has been pioneered inpublished studies on carotid artery stenting and Covid-1920 [24].
Study limitations
By design, NRD does not allow the determination of regional variations within the dataset such that we cannot compare one state to that of another. This study does not capture data of patients who were admitted as an outpatient observation status and represents only hospital admissions. Other limitations include inaccurate coding or subjective coding by physicians as well as patients admitted outside the tracking hospitals could have been missed. As with any observational data, the results do not suggest causal relationships, as there can be other unmeasured confounders. Of note, the diagnosis codes are assigned to patients throughout an admission process based on various things such as symptoms, labs and procedures ordered, and of course results, unfortunately the NRD does not detail on validation studies to 100% confirm if a diagnosis is true, however the diagnosis codes we utilized are related to infective endocarditis and that there is a high probability that a patient actually had it. The earlier mentioned statement of the U.S having the highest incidence of IE in the world could also be due to misdiagnosis in “national database coding studies” and thus this would also be a limitation. Outpatient follow up is an extremely important component after hospital stays, but unfortunately this cannot be tracked or studied utilizing the NRD; specifically knowing how outpatient parenteral antibiotic treatment is handled is something that should be a focus in a future study.
Our analysis suggests that over 1 in 5 patients admitted with infective endocarditis end up with an unplanned readmission within 30 days of discharge with the main diagnosis during readmission encounter being septicemia, heart failure, and then endocarditis itself. Surgical intervention during index admission as well as other patient and hospital related factors were associated with readmissions as well. Additionally, close follow up for sepsis and electrolyte and fluid balance disorders should be conducted to alleviate read mission burden. Patients who had co-morbidities like CKD with higher odds of readmission should have closer outpatient follow up to help prevent the readmissions as well. Data retrieved from this study that was conducted after the change in guidelines and utilization of ICD-10 may help develop protocols and management plans to reduce overall healthcare costs and improve patient outcomes.
Perspectives
Competency in Patient Care: Patient should be counselled appropriately on risk factors that may have contributed to onset of infective endocarditis, future complications, as well as comorbidities that need to be managed much more closely that can worsen clinical conditions.
Competency in Medical Knowledge: Early IV antibiotic management is the preferred method of management for Infective Endocarditis
Interpersonal and Communication Skills: Medicine, Surgery, and Primary Care Provider need to communicate effectively with each-other as well as the patient in order to achieve the best possible outcomes at, during, and after admission and discharge.
Translational Outlook 1: Despite being a study involving data from one calendar year, readmissions from other years after the 2015 guidelines could provide more data and support for our interpretations in this study
Translational Outlook 2: There seems to be a push for surgical intervention during index admission (in patients that qualify) – there could be a more detailed comparative study done with specific surgical interventions and the times at which they were performed during an admission, i.e. within the first week of admission, vs. 2 weeks, vs. 3 weeks.
Translational Outlook 3: Closer follow-up and coordination with primary care providers outpatient should be re-evaluated in regard to repeat lab work and comorbidities that have led to a higher odds of being readmitted. A study to compare groups with closer follow-up within 1 week could be compared to those that had follow up past 1 week and those that never had follow-ups at all.
Funding: None
Disclosures: None
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.
