Abstracts
This is a two-phase study, the first was a literature review that aimed to identify a set of competencies for professional practice that would be relevant for the health care of People with disabilities (PwD). These competencies were then used to plan a thirty-hour multidisciplinary course for undergraduate health care students. The educational intervention led to improvements in the students’ learning experiences, including the development of empathy and knowledge related to the care of PwD, improved knowledge around accessibility, and an awareness of the need to humanize the care of PwD. Students reported enhanced learning experiences and an increase in knowledge related to the care of PwD, and also highlighted the need to humanize the care.
Health education; Disabled persons; Health care
Este é um estudo de duas fases, a primeira foi uma revisão da literatura buscando identificar um conjunto de competências para a prática professional, relevantes para o cuidado em saúde das Pessoas com deficiências (PcD). Estas competências foram utilizadas na segunda fase, para planejar um curso multidisciplinar de trinta horas para estudantes de graduação da área da saúde. A intervenção educacional levou a melhorias em experiências de aprendizagem dos alunos, incluindo o desenvolvimento de empatia e de conhecimentos relacionados com cuidados de PcD, melhorar o conhecimento sobre a acessibilidade, e consciência da necessidade de humanizar o cuidado de PcD. Estudantes relataram experiências de aprendizagem melhoradas e maior conhecimento relacionado com o cuidado de PcD, e destacaram a necessidade de humanizar o cuidado.
Educação em saúde; Pessoas com deficiência; Assistência à saúde
Este es un estudio de dos fases, la primera fue una revisión de la literatura buscando identificar un conjunto de competencias para la práctica profesional, relevantes para el cuidado de la salud de las PcD. Estas competencias se utilizaron para planificar un curso multidisciplinario de treinta horas. La intervención educativa llevó a experiencias de aprendizaje de los alumnos, incluyendo el desarrollo de la empatía y de conocimientos relacionados con cuidados de las PcD, mejorar el conocimiento sobre la capacidad de acceso, y conciencia de la necesidad de humanizar el cuidado de las PcD. Los estudiantes relataron experiencias de aprendizaje mejoradas y mayor conocimiento relacionado con el cuidado de las PcD, y subrayaron la necesidad de humanizar el cuidado de las PcD.
Educación en salud; Personas con discapacidad (PcD); Prestación de atención de salud
Introduction
The biomedical model of healthcare has had an important influence on health professions education11. Almeida AH, Soares CB. Ensino de educação nos cursos de graduação em enfermagem. Rev Bras Enferm. 2010; 63(1):111-6., which has been problematic for health care in general. The concern is that it presents the person as a purely biological being, excluding other important dimensions such as the social22. Moyer CA, Adongo PB, Aborigo RA, Hodgson A, Engmann CM, Devries R. “It’s up to the woman’s people”: how social factors influence facility-based delivery in rural northern Ghana. Matern Child Health J. 2014; 18(1):109-19., psychological33. Sirey JA. The impact of psychosocial factors on experience of illness and mental health service use. Am J Geriatr Psychiatry. 2008; 16(9):703-5. and environmental44. Yeager V, Menachemi N, Ginter P, Sen B, Savage G, Beitsch LM. Environmental factors and quality improvement in county and local health departments. J Public Heal Manag Pract. 2013; 19(3):240-9. factors that influence therapeutic outcomes. The biomedical approach is also problematic because it places the disability within the person 55. Johnston M. Models of disability. Psychologist. 1996; 9:205-10. rather than seeing it as the result of the interactions between the person and the environment66. WHO. International classification of functioning, disability and health (ICF) [Internet]. Geneva: World Health Organization; 2007. p. 112-9 [cited 11 May 2016]. Available from: http://www.who.int/classifications/icf/en/.
http://www.who.int/classifications/icf/e...
. By limiting our understanding of the factors involved we also limit the intervention possibilities, thereby making management of the patient more difficult.
This understanding of the concept of disability may result in the unsatisfactory management of PwD. Therefore, if health students are taught with an understanding of disability that is influenced by the biomedical model, they will reproduce this problematic understanding in their practice and PwD will continue to receive inadequate health care. For that reason, it is important to replace the biomedical model of disability with the bio-psychosocial model in the undergraduate curriculum77. Domenech J, Sánchez-Zuriaga D, Segura-Ortí E, Espejo-Tort B, Lisón JF. Impact of biomedical and biopsychosocial training sessions on the attitudes, beliefs, and recommendations of health care providers about low back pain: a randomised clinical trial. Pain. 2011; 152(11):2557-63.. The incorporation of innovative educational interventions that aim to improve the care of PwD have produced encouraging results. These include positive changes in the attitudes of students towards PwD88. Amosun SL, Volmink L, Rosin R. Perceived images of disability: the reflections of two undergraduate medical students in a university in South Africa on life in a wheelchair. Disabil Rehabil. 2005; 27(16):961-6., more comfort in dealing with PwD99. Crotty M, Finucane P, Ahern M. Teaching medical students about disability and rehabilitation: methods and student feedback. Med Educ. 2000; 34(8):659-64., and improvement in the knowledge and attitudes of students towards PwD1010. Graham CL, Brown RS, Zhen H, McDermott S. Teaching medical students about disability in family medicine. Fam Med. 2009; 41(8):542-4..
The purpose of this paper is to provide an overview of an educational intervention that aimed to improve the understanding and competencies required by students in the holistic management of PwD, that moves beyond a biomedical model of understanding disability.
Methods
This study used a qualitative survey design with open-ended questions to determine if the new teaching intervention led to any changes in students’ holistic understanding of the management of PwD.
The study was divided into two phases. The first phase used a review of the literature and the national curriculum guidelines for Brazilian undergraduate health courses to identify the competencies that health professionals need for the holistic management of PwD. These competencies were then categorized by profession (Medicine, Nursing, Nutrition, Occupational Therapy (OT), Physiotherapy, Psychology and a set of competencies that were common to all health professions).
In the second phase, we used these identified competencies to plan a multidisciplinary, thirty-hour elective course for a variety of health professional students. The course was presented by a physiotherapist and an occupational therapist and aimed to strengthen the competencies that had been identified as being necessary for the holistic management of PwD. Chart1 presents the overall structure of the course.
A convenient sample of twelve students enrolled in the course. At the end of the course, participants completed a questionnaire that gathered qualitative data about their learning experiences in the course using the following open-ended questions: 1) “Do you think this course provided you with knowledge or experience that will help you as a professional? Please explain your answer.”; 2) “In your opinion, what do you think was the most important point in the course that influenced your professional formation? Please explain your answer.” Responses to these open ended questions were transcribed and analyzed using the Discourse of the Collective Subject method, described as a qualitative data organization technique carried out through a speech synthesis. This speech is written in the first person singular and prepared with the most significant similar sense of testimonials extracted from the qualitative data. It is based on the theory of social representations and aims to analyze the main ideas, anchors and key phrases that are present in the individual responses1515. Reis CB, Andrade SMO. Representações sociais das enfermeiras sobre a integralidade na assistência à saúde da mulher na rede básica. Cienc Saude Colet. 2008; 13(1):61-70., but it could be used to extract the key concepts from an open response1616. Castro SS, Lefèvre F, Lefèvre AMC, Cesar CLG. Accessibility to health services by persons with disabilities. Rev Saude Publica. 2011; 45(1):99-105..
The project was approved by the Ethics Committee of the Federal University of the Triângulo Mineiro (protocol number 2260/2012). The anonymity of participants was guaranteed by replacing student names with alphanumeric codes and participation in the study was voluntary. The participants signed a consent form after being provided with information about the study and were free to withdraw their consent at any time without any negative consequences.
Results
In Chart 2 the competencies that were identified by the literature review in the first phase of the project are presented.
Participant responses to the questionnaire at the end of the course indicated that almost 90% reported that they had mastered the Communication competency; approximately 64% reported being competent with the Patient assessment competency; about 64% of participants identified the health professional and patient relationship as a competency that they had mastered; 58% reported having mastered the ethical attitude; about 48% reported being competent in patient-centered practice and quality of care; and about 27% reported being competent in their clinical knowledge.
We also identified six central ideas (cited 23 times) after analyzing the transcribed data from the first survey question, at the end of the course, which are presented in Graph 1.
Central ideas that emerged from the question “Do you think this course provided you with some knowledge or experience that will help you as a professional?”. Numbers represent participants who answered “Yes”.
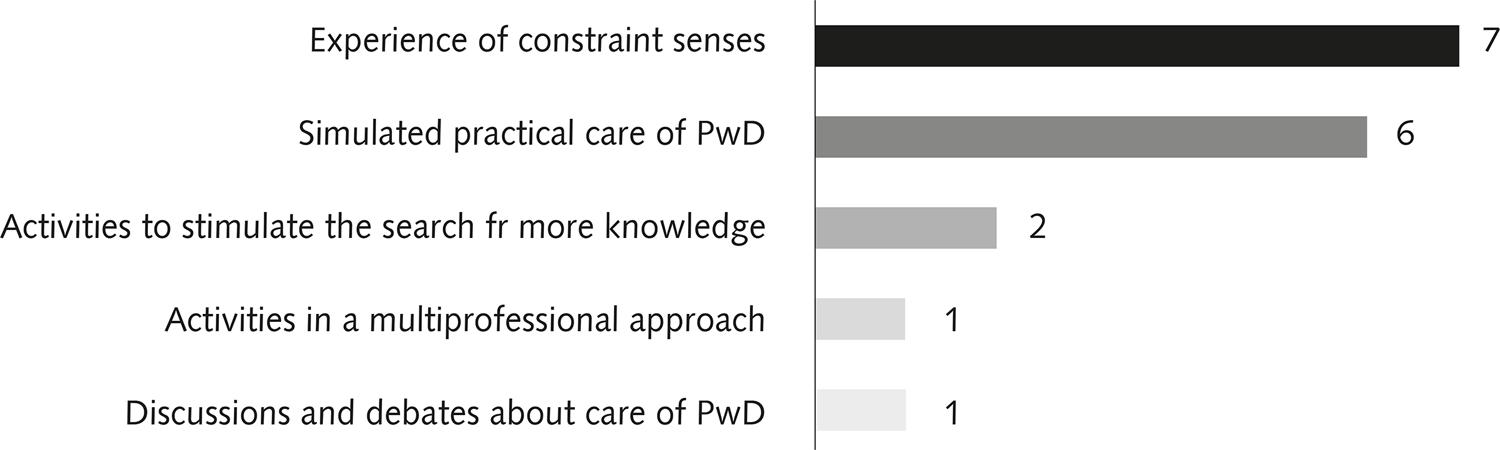
In response to the second question, participants reported five central ideas (cited 17 times), which are presented in Graph 2.
Central ideas that emerged from the question: “In your opinion, what do you think was the most important point in the course that influenced your professional formation?”
Discussion
Literature review to identify generic health professional competencies in the management of PwD
Communication and decision-making were identified from the literature as competencies that are common to all health professions. In the clinical context communication not only means keeping patients informed by using a common language but also listening to them as participants in the health care relationship. As part of interprofessional health care, communication is an essential component of providing better patient outcomes in shorter time frames, higher satisfaction among patients, and improvement in the work environment3333. Zwarenstein M, Reeves S, Russell A, Kenaszchuk C, Conn LG, Miller KL, et al. Structuring Communication Relationships for Interprofessional Teamwork (SCRIPT): a cluster randomized controlled trial. Trials. (2007); 8:23.. Moreover, effective communication is positively correlated with patient adherence to treatment3434. DiMatteo MR. Patient adherence to pharmacotherapy: the importance of effective communication. Formulary. 1995; 30(10):596-8, 601-2, 605-605.,3535. Zolnierek KBH, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009; 47(8):826-34., preventative action by patients3636. Anders MP, Nolte S, Waldmann A, Capellaro M, Volkmer B, Greinert R, et al. The German SCREEN project - design and evaluation of the communication strategy. Eur J Public Health. 2015; 25(1):150-5. and can lead to improvement in patients’ quality of health3737. Ports KA, Reddy DM, Barnack-Tavlaris JL. Sex differences in health care provider communication during genital herpes care and patients’ health outcomes. J Health Commun. 2013; 18(12):1436-48..
Decision-making as a competence is about combining the desires and beliefs of the team in order to choose a course of action. This process includes the following components: courses of action; beliefs about objective states, processes, and events; and desires, values, or utilities that describe the consequences associated with the outcomes of each action-event combination3838. Hastie R. Problems for judgment and decision making. Annu Rev Psychol. 2001; 52:653-83.. This competency, when present in the process of health care, could mitigate the inequalities in the use of health services3939. Durand MA, Carpenter L, Dolan H, Bravo P, Mann M, Bunn F, et al. Do interventions designed to support shared decision-making reduce health inequalities? A systematic review and meta-analysis. PLoS One. 2014; 9(4):e94670., resulting in benefits to all stakeholders in the system. If used properly, effective decision-making can make the health professional team more productive and coordinated, resulting in improved health care.
The literature review also identified other common competencies across the health professions, including: Health attention; Leadership; Management; and Continuing education. Health attention is the ability to develop preventive, promotional, protective and rehabilitation interventions while considering the individual patient and the community. This competency promotes continuous and integrated health care at the individual and community levels4040. Silva MJ, Sousa EM, Freitas CL. Formação em enfermagem: interface entre as diretrizes curriculares e os conteúdos de atenção básica. Rev Bras Enferm. 2011; 64(2):315-21.. It should occur continuously and be integrated with critical thinking that is focused on general social problems that exist in the community2020. Sanford J, Stratford P, Solomon P. Clinical evaluation: physiotherapists’ ranking of competencies. Med Teach. 1993; 15(4):369-77.. If this competency is adequately developed in undergraduate health professionals education, new graduates will be better prepared to face real-world clinical environments4141. Nascimento D, Oliveira M. Reflexões sobre as competências profissionais para o processo de trabalho nos núcleos de apoio à saúde da família. O mundo da Saúde. 2010; 34(1):92-6. in which the holistic management of PwD is prioritized and made more effective.
Leadership is defined as “the process of influencing an organized group toward accomplishing their goals”4242. Rauch C, Behling O. Functionalism: basis for alternate approach to the study of leadership. Leaders and Managers. Elmsford, NY: Pergamon Press; 1984.. The presence of this competency in a multi-professional health team can improve the efficiency of the health care system4343. Hunziker S, Bühlmann C, Tschan F, Balestra G, Legeret C, Schumacher C, et al. Brief leadership instructions improve cardiopulmonary resuscitation in a high-fidelity simulation: a randomized controlled trial. Crit Care Med. 2010; 38(4):1086-91. resulting in more effective management processes by the health team and an improved patient experience in the health system.
Management is related to the ability to deal with members of the health team, physical and material resources, and with information. At the same time managers should be able to engage in dialogue with employers and other health professionals in leadership positions2323. Ministério da Educação (BR). Resolução CNE/CES no 3, de 7 de novembro de 2001. Institui diretrizes curriculares nacionais do curso de graduação em enfermagem [Internet]. Brasília; 2001 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES03.pdf.
http://portal.mec.gov.br/cne/arquivos/pd...
. Along with the Leadership competency, the Management competency could be a key feature for successful teamwork in the health care system.
Continuing education has as one of its goals the improvement of professional practice in order to enhance health care4444. Thomson OMA, Freemantle N, Oxman AD, Wolf F, Davis DA, Herrin J. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2001; (2):CD003030.. Therefore, it should not only direct health professionals to seek new knowledge and skills but also to carry out changes in the process of care4545. Gray JA. Continuing education: what techniques are effective? Lancet. 1986; 2(8504):447-8.. There is also evidence that a lack of continuing education among health service professionals may increase the costs of patient care, thus making it more expensive, together with a reduction in quality4646. Bloom BS. Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews. Int J Technol Assess Health Care. 2005; 21(3):380-5.. Continuing education appears to improve the acquisition and retention of knowledge, attitudes, skills, behaviors and clinical outcomes4747. Marinopoulos SS, Dorman T, Ratanawongsa N, Wilson LM, Ashar BH, Magaziner JL, et al. Effectiveness of continuing medical education. Evid Rep Technol Assess (Full Rep). 2007; (149):1-69. all of which have a positive impact on patients health.
The review of the literature therefore served to highlight a range of generic competencies that have been shown to improve health service delivery in ways that may be beneficial for PwD. The next phase of the project was to develop a teaching intervention that aimed to develop in students these competencies, with specific reference to the holistic management of PwD.
Outcomes of the educational intervention, based on student responses in the survey
The results of the open-ended questions in the survey (see Charts 1 and 2) presented concepts related to students’ knowledge and experience regarding the care of PwD. These were key points that had been highlighted by the literature and it is important that they are addressed in the development of undergraduate students in order to offer better health care for PwD. Furthermore, students identified that clinical knowledge was their least frequently mastered competency in this intervention.
Knowledge related to accessibility was also reported by students as having improved as a result of the educational intervention. The concept of accessibility is an important characteristic of health services that can act either as a barrier or a facilitator for PwD and an understanding of it is essential for health professionals to work effectively with PwD. Physical accessibility is a central point because it influences the quality of the health care service and the willingness of PwD to use health systems4848. DeJong G. Primary care for persons with disabilities. An overview of the problem. Am J Phys Med Rehabil. 1997; 76(3 Suppl):S2-8.,4949. Morrison EH, George V, Mosqueda L. Primary care for adults with physical disabilities: perceptions from consumer and provider focus groups. Fam Med. 2008; 40(9):645-51.. If health professionals are aware of the challenges related to accessibility, they would be better prepared to reduce the barriers experienced by PwD, and therefore offer a better health care service. In other words, awareness of this concept would make health services more accessible leading to improvements in responsiveness5050. Kroll T, Jones GC, Kehn M, Neri MT. Barriers and strategies affecting the utilisation of primary preventive services for people with physical disabilities: a qualitative inquiry. Health Soc Care Community. 2006;14(4):284-93. and will be more closely aligned with the principle of equality in the Brazilian National Health System (SUS)5151. Senna MCM. Eqüidade e política de saúde: algumas reflexões sobre o Programa Saúde da Família. Cad Saude Publica. 2002; 18 Supl:S203-11..
The need to humanize health care was another point that students raised, which is important to note as it is a central component of the SUS, not only for PwD but for all citizens. In 2003 the SUS introduced a National Policy of Humanization5252. Pasche DF, Passos E, Hennington EA. Cinco anos da política nacional de humanização: trajetória de uma política pública. Cienc Saude Colet. 2011; 16(11):4541-8. that aimed to improve the quality of national health care5353. Santos-Filho SB. Perspectivas da avaliação na Política Nacional de Humanização em Saúde: aspectos conceituais e metodológicos. Cienc Saude Colet. 2007; 12(4):999-1010. and which led to positive outcomes in the management of patients5454. Pasche DF. National Humanization Policy as a commitment to collective production of changes in management and care methods. Interface (Botucatu). 2009; 13 Supl 1:701-8.. The results of this study highlight the fact that students believed that humanization is an important competency in their professional development5555. Goulart BNG, Chiari BM. Humanização das práticas do profissional de saúde: contribuições para reflexão. Cienc Saude Colet. 2010; 15(1):255-68..
Self-assurance related to the care of PwD and the need for change regarding an increased social awareness about PwD were also reported by participants as important outcomes of the educational intervention. There is evidence that students who have received instructions and experiences related to disability care feel more confident in the care process5656. Kinne RD, Stiefel DJ. Assessment of student attitude and confidence in a program of dental education in care of the disabled. J Dent Educ. 1979; 43(5):271-5. and that social awareness could be a factor that acts towards decreasing barriers if working in the health care services environment5757. Cook V, Griffin A, Hayden S, Hinson J, Raven P. Supporting students with disability and health issues: lowering the social barriers. Med Educ. 2012; 46(6):564-74..
The students’ experience of having their senses limited put them into a similar circumstance that patients find themselves in and was cited as one of the most important aspects of this educational intervention. The simulation of health care situations are commonly used in undergraduate courses and have been shown to improve health care5858. Wayne DB, Didwania A, Feinglass J, Fudala MJ, Barsuk JH, McGaghie WC. Simulation-based education improves quality of care during cardiac arrest team responses at an academic teaching hospital: a case-control study. Chest. 2008; 133(1):56-61.. In addition, there is evidence that the development of empathy in undergraduate students can have a positive effect on student learning, reducing the risk of burnout and promoting student well-being5959. Brazeau CMLR, Schroeder R, Rovi S, Boyd L. Relationships between medical student burnout, empathy, and professionalism climate. Acad Med. 2010; 85 Supl 10:S33-6.. As part of the development of a healthcare professional who is capable of enhanced social and interpersonal skills, helping students to understand how others’ experience their interaction is an important part of health professional training6060. Ioannidou F, Konstantikaki V. Empathy and emotional intelligence: what is it really about? Int J Caring Sci. 2008; 1(3):118-23..
The requirement to conduct additional research during the program was also cited by students as one of the most important aspects of the intervention. This is directly related to the concept of continuous education for health professionals, which has been shown to reduce the incidence of adverse events6161. Pinto WAM, Rossetti HB, Araújo A, Spósito Júnior JJ, Salomão H, Mattos SS, et al. Impact of a continuous education program on the quality of assistance offered by intensive care physiotherapy. Rev Bras Ter Intensiva. 2014; 26(1):7-12., as well as improve the quality of care6262. Twig G, Lahad A, Kochba I, Ezra V, Mandel D, Shina A, et al. Effect of a tailor-made continuous medical education program for primary care physicians on self-perception of physicians’ roles and quality of care. Isr Med Assoc J. 2010; 12(9):521-5. and knowledge acquisition6363. Weiner SJ, Jackson JL, Garten S. Measuring continuing medical education outcomes: a pilot study of effect size of three CME interventions at an SGIM annual meeting. J Gen Intern Med. 2009; 24(5):626-9..
The students also reported that the discussion and debate about the care of PwD were important components of the educational intervention. These are common strategies used as learning tools in health professions education6464. Hanna LA, Barry J, Donnelly R, Hughes F, Jones D, Laverty G, et al. Using debate to teach pharmacy students about ethical issues. Am J Pharm Educ. 2014; 78(8):57.,6565. Nguyen VQC, Hirsch MA. Use of a policy debate to teach residents about health care reform. J Grad Med Educ. 2011; 3(3):376-8. and can stimulate critical thinking in students, as well as promote an interest in complex and controversial issues6666. Strawbridge JD, Barrett AM, Barlow JW. Interprofessional ethics and professionalism debates: findings from a study involving physiotherapy and pharmacy students. J Interprof Care. 2014; 28(1):64-5..
Learning activities that were conducted from a multi-professional perspective were also reported by the participants as being especially important. Participation in the multi-professional team is an important aspect of professional practice that should be reinforced as a skill to be developed among students4646. Bloom BS. Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews. Int J Technol Assess Health Care. 2005; 21(3):380-5.,4747. Marinopoulos SS, Dorman T, Ratanawongsa N, Wilson LM, Ashar BH, Magaziner JL, et al. Effectiveness of continuing medical education. Evid Rep Technol Assess (Full Rep). 2007; (149):1-69.,4949. Morrison EH, George V, Mosqueda L. Primary care for adults with physical disabilities: perceptions from consumer and provider focus groups. Fam Med. 2008; 40(9):645-51.. This kind of collaborative work brings additional benefits like novel insights and points of view, the development of respect and equality for other members of the team, improvement of communication skills and a more holistic approach to health6767. Payne H, Pelz F, Brooks R, Horrocks L, Kemp A, Webb E, et al. Benefits of interprofessional learning: an interprofessional MSc in child health. Hosp Med. 2005; 66(4):239-41.. These all lead to increased patient satisfaction, a reduction in error rates and more effective teamwork6868. Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev. 2013; 3:CD002213..
It is important to stress that the students pointed out that the most important points of the course included a positive influence on their professional identity, learning about alternative methods and strategies of teaching and learning, an increased focus on sensory experiences, simulations, and activities that stimulate research, in the benefits of a multi-professional approach, and discussions and debates about the care of PwD. This result reinforced the innovative character of the course and shows that students are sensitive and attentive to new teaching methods, which is in line with the literature6969. Fidler DC, Khakoo R, Miller LA. Teaching scholars programs: faculty development for educators in the health professions. Acad Psychiatry. 2007; 31(6):472-8.
70. Jhaveri KD, Chawla A, Shah HH. Case-based debates: an innovative teaching tool in nephrology education. Ren Fail. 2012; 34(8):1043-5.-7171. Hicks J. Students’ views of cooperative learning and group testing. Radiol Technol. 2007; 78(4):275-83..
Limitations of the study
The first limitation is that the research was only conducted in one university and we believe that a larger sample size that is spread across multiple universities would lead to an outcome that could more confidently be asserted. In addition, the participation of students from a greater variety of health disciplines would offer better opportunities in the design of the educational intervention.
Conclusions
This paper describes a plan for designing an innovative educational intervention that aimed to help health students to develop important competencies that are relevant for the holistic management of PwD. Students reported an increase in experience and knowledge related to the care of PwD, the need to humanize the care of PwD, and also described the need for educational change to increase social awareness about PwD in the undergraduate program.
The study also highlighted the set of competencies needed for the satisfactory holistic management of PwD and described an educational intervention that aimed to develop those competencies in undergraduate health professions students. This experience could be used as a starting point by others to improve the educational approach by developing the main competencies and abilities of health professions undergraduate students in the care of PwD.
References
-
1Almeida AH, Soares CB. Ensino de educação nos cursos de graduação em enfermagem. Rev Bras Enferm. 2010; 63(1):111-6.
-
2Moyer CA, Adongo PB, Aborigo RA, Hodgson A, Engmann CM, Devries R. “It’s up to the woman’s people”: how social factors influence facility-based delivery in rural northern Ghana. Matern Child Health J. 2014; 18(1):109-19.
-
3Sirey JA. The impact of psychosocial factors on experience of illness and mental health service use. Am J Geriatr Psychiatry. 2008; 16(9):703-5.
-
4Yeager V, Menachemi N, Ginter P, Sen B, Savage G, Beitsch LM. Environmental factors and quality improvement in county and local health departments. J Public Heal Manag Pract. 2013; 19(3):240-9.
-
5Johnston M. Models of disability. Psychologist. 1996; 9:205-10.
-
6WHO. International classification of functioning, disability and health (ICF) [Internet]. Geneva: World Health Organization; 2007. p. 112-9 [cited 11 May 2016]. Available from: http://www.who.int/classifications/icf/en/
» http://www.who.int/classifications/icf/en/ -
7Domenech J, Sánchez-Zuriaga D, Segura-Ortí E, Espejo-Tort B, Lisón JF. Impact of biomedical and biopsychosocial training sessions on the attitudes, beliefs, and recommendations of health care providers about low back pain: a randomised clinical trial. Pain. 2011; 152(11):2557-63.
-
8Amosun SL, Volmink L, Rosin R. Perceived images of disability: the reflections of two undergraduate medical students in a university in South Africa on life in a wheelchair. Disabil Rehabil. 2005; 27(16):961-6.
-
9Crotty M, Finucane P, Ahern M. Teaching medical students about disability and rehabilitation: methods and student feedback. Med Educ. 2000; 34(8):659-64.
-
10Graham CL, Brown RS, Zhen H, McDermott S. Teaching medical students about disability in family medicine. Fam Med. 2009; 41(8):542-4.
-
11Gramaglia C, Jona A, Imperatori F, Torre E, Zeppegno P. Cinema in the training of psychiatry residents: focus on helping relationships. BMC Med Educ. 2013; 13:90.
-
12Hanna LA, Barry J, Donnelly R, Hughes F, Jones D, Laverty G, et al. Using debate to teach pharmacy students about ethical issues. Am J Pharm Educ. 2014; 78(3):57.
-
13Baerheim A, Alraek TJ. Utilizing theatrical tools in consultation training. A way to facilitate students’ reflection on action? Med Teach. 2005; 27(7):652-4.
-
14Leo J, Goodwin D. Negotiated meanings of disability simulations in an adapted physical activity course: learning from student reflections. Adapt Phys Activit Q. 2014; 31(2):144-61.
-
15Reis CB, Andrade SMO. Representações sociais das enfermeiras sobre a integralidade na assistência à saúde da mulher na rede básica. Cienc Saude Colet. 2008; 13(1):61-70.
-
16Castro SS, Lefèvre F, Lefèvre AMC, Cesar CLG. Accessibility to health services by persons with disabilities. Rev Saude Publica. 2011; 45(1):99-105.
-
17ACOTRO, Association of Canadian Occupational Therapy Regulatory Organizations. Essential competencies of practice for occupational therapists in Canada 2011 [Internet]. 2011 [cited 11 May 2016]. Available from: http://www.coto.org/pdf/essent_comp_04.pdf
» http://www.coto.org/pdf/essent_comp_04.pdf -
18National Physiotherapy Advisory Group N. Essential competency profile for physiotherapists in Canada 2009 [Internet]. 2009 [cited 11 May 2016]. Available from: http://www.physiotherapyeducation.ca/Resources/Essential Comp PT Profile 2009.pdf
» http://www.physiotherapyeducation.ca/Resources/Essential Comp PT Profile 2009.pdf -
19Porcel JM, Casademont J, Conthe P, Pinilla B, Pujol R, García-Alegría J. Core competencies in internal medicine. Eur J Intern Med. 2012; 23(4):338-41.
-
20Sanford J, Stratford P, Solomon P. Clinical evaluation: physiotherapists’ ranking of competencies. Med Teach. 1993; 15(4):369-77.
-
21Sottas B. Learning outcomes for health professions: the concept of the swiss competencies framework. GMS Z Med Ausbild. 2011; 28(1):Doc11.
-
22Ministério da Educação (BR). Resolução CNE/CES no 4, de 19 de fevereiro de 2002. Institui diretrizes curriculares nacionais do curso de graduação em fisioterapia [Internet]. Brasília; 2002 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES042002.pdf
» http://portal.mec.gov.br/cne/arquivos/pdf/CES042002.pdf -
23Ministério da Educação (BR). Resolução CNE/CES no 3, de 7 de novembro de 2001. Institui diretrizes curriculares nacionais do curso de graduação em enfermagem [Internet]. Brasília; 2001 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES03.pdf
» http://portal.mec.gov.br/cne/arquivos/pdf/CES03.pdf -
24Aston-McCrimmon E. Analysis of the ratings of competencies used in physical therapy practice. Phys Ther. 1986; 66(6):954-60.
-
25Ministério da Educação (BR). Parecer CNE/CES no 49 de julho de 2001. Institui as diretrizes curriculares nacionais dos cursos de filosofia, história, geografia, serviço social, comunicação social, ciências sociais, letras, biblioteconomia, arquivologia e museologia [Internet]. Brasília; 2001 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES0492.pdf
» http://portal.mec.gov.br/cne/arquivos/pdf/CES0492.pdf -
26Ministério da Educação (BR). Resolução CNE/CES no 5, de 7 de novembro de 2001. Institui diretrizes curriculares nacionais do curso de graduação em nutrição [Internet]. Brasília; 2001 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES05.pdf
» http://portal.mec.gov.br/cne/arquivos/pdf/CES05.pdf -
27Ministério da Educação (BR). Resolução CNE/CES no 4, de 7 de novembro de 2001. Institui diretrizes curriculares nacionais do curso de graduação em medicina [Internet]. Brasília; 2001 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES04.pdf
» http://portal.mec.gov.br/cne/arquivos/pdf/CES04.pdf -
28Ministério da Educação (BR). Resolução CNE/CES no 5, de 15 de março de 2011. Institui diretrizes curriculares nacionais do curso de graduação em psicologia [Internet]. Brasília; 2011 [cited 11 May 2016]. Available from: http://portal.mec.gov.br/index.php?option=com_content&id=12991&Itemid=866
» http://portal.mec.gov.br/index.php?option=com_content&id=12991&Itemid=866 -
29Canadian Interprofessional Health Collaborative. Interprofessional education & core competencies [Internet]. Vancouver; 2011 [cited 11 May 2016]. Available from: http://www.cihc.ca/files/publications/CIHC_IPE-LitReview_May07.pdf
» http://www.cihc.ca/files/publications/CIHC_IPE-LitReview_May07.pdf -
30Epstein R, Hundert E. Defining and assessing professional competence. JAMA. 2002; 287(2):226.
-
31Frank JR, Langer B. Collaboration, communication, management, and advocacy: teaching surgeons new skills through the CanMEDS Project. World J Surg. 2003; 27(8):972-8; discussion 978.
-
32Thomas AC, Crabtree MK, Delaney KR, Dumas MA, Kleinpell R, Logsdon MC, et al. Nurse Practitioner Core Competencies 2011 [Internet]. 2011 [cited 11 May 2016]. Available from: http://c.ymcdn.com/sites/www.nonpf.org/resource/resmgr/imported/IntegratedNPCoreCompsFINALApril2011.pdf
» http://c.ymcdn.com/sites/www.nonpf.org/resource/resmgr/imported/IntegratedNPCoreCompsFINALApril2011.pdf -
33Zwarenstein M, Reeves S, Russell A, Kenaszchuk C, Conn LG, Miller KL, et al. Structuring Communication Relationships for Interprofessional Teamwork (SCRIPT): a cluster randomized controlled trial. Trials. (2007); 8:23.
-
34DiMatteo MR. Patient adherence to pharmacotherapy: the importance of effective communication. Formulary. 1995; 30(10):596-8, 601-2, 605-605.
-
35Zolnierek KBH, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009; 47(8):826-34.
-
36Anders MP, Nolte S, Waldmann A, Capellaro M, Volkmer B, Greinert R, et al. The German SCREEN project - design and evaluation of the communication strategy. Eur J Public Health. 2015; 25(1):150-5.
-
37Ports KA, Reddy DM, Barnack-Tavlaris JL. Sex differences in health care provider communication during genital herpes care and patients’ health outcomes. J Health Commun. 2013; 18(12):1436-48.
-
38Hastie R. Problems for judgment and decision making. Annu Rev Psychol. 2001; 52:653-83.
-
39Durand MA, Carpenter L, Dolan H, Bravo P, Mann M, Bunn F, et al. Do interventions designed to support shared decision-making reduce health inequalities? A systematic review and meta-analysis. PLoS One. 2014; 9(4):e94670.
-
40Silva MJ, Sousa EM, Freitas CL. Formação em enfermagem: interface entre as diretrizes curriculares e os conteúdos de atenção básica. Rev Bras Enferm. 2011; 64(2):315-21.
-
41Nascimento D, Oliveira M. Reflexões sobre as competências profissionais para o processo de trabalho nos núcleos de apoio à saúde da família. O mundo da Saúde. 2010; 34(1):92-6.
-
42Rauch C, Behling O. Functionalism: basis for alternate approach to the study of leadership. Leaders and Managers. Elmsford, NY: Pergamon Press; 1984.
-
43Hunziker S, Bühlmann C, Tschan F, Balestra G, Legeret C, Schumacher C, et al. Brief leadership instructions improve cardiopulmonary resuscitation in a high-fidelity simulation: a randomized controlled trial. Crit Care Med. 2010; 38(4):1086-91.
-
44Thomson OMA, Freemantle N, Oxman AD, Wolf F, Davis DA, Herrin J. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2001; (2):CD003030.
-
45Gray JA. Continuing education: what techniques are effective? Lancet. 1986; 2(8504):447-8.
-
46Bloom BS. Effects of continuing medical education on improving physician clinical care and patient health: a review of systematic reviews. Int J Technol Assess Health Care. 2005; 21(3):380-5.
-
47Marinopoulos SS, Dorman T, Ratanawongsa N, Wilson LM, Ashar BH, Magaziner JL, et al. Effectiveness of continuing medical education. Evid Rep Technol Assess (Full Rep). 2007; (149):1-69.
-
48DeJong G. Primary care for persons with disabilities. An overview of the problem. Am J Phys Med Rehabil. 1997; 76(3 Suppl):S2-8.
-
49Morrison EH, George V, Mosqueda L. Primary care for adults with physical disabilities: perceptions from consumer and provider focus groups. Fam Med. 2008; 40(9):645-51.
-
50Kroll T, Jones GC, Kehn M, Neri MT. Barriers and strategies affecting the utilisation of primary preventive services for people with physical disabilities: a qualitative inquiry. Health Soc Care Community. 2006;14(4):284-93.
-
51Senna MCM. Eqüidade e política de saúde: algumas reflexões sobre o Programa Saúde da Família. Cad Saude Publica. 2002; 18 Supl:S203-11.
-
52Pasche DF, Passos E, Hennington EA. Cinco anos da política nacional de humanização: trajetória de uma política pública. Cienc Saude Colet. 2011; 16(11):4541-8.
-
53Santos-Filho SB. Perspectivas da avaliação na Política Nacional de Humanização em Saúde: aspectos conceituais e metodológicos. Cienc Saude Colet. 2007; 12(4):999-1010.
-
54Pasche DF. National Humanization Policy as a commitment to collective production of changes in management and care methods. Interface (Botucatu). 2009; 13 Supl 1:701-8.
-
55Goulart BNG, Chiari BM. Humanização das práticas do profissional de saúde: contribuições para reflexão. Cienc Saude Colet. 2010; 15(1):255-68.
-
56Kinne RD, Stiefel DJ. Assessment of student attitude and confidence in a program of dental education in care of the disabled. J Dent Educ. 1979; 43(5):271-5.
-
57Cook V, Griffin A, Hayden S, Hinson J, Raven P. Supporting students with disability and health issues: lowering the social barriers. Med Educ. 2012; 46(6):564-74.
-
58Wayne DB, Didwania A, Feinglass J, Fudala MJ, Barsuk JH, McGaghie WC. Simulation-based education improves quality of care during cardiac arrest team responses at an academic teaching hospital: a case-control study. Chest. 2008; 133(1):56-61.
-
59Brazeau CMLR, Schroeder R, Rovi S, Boyd L. Relationships between medical student burnout, empathy, and professionalism climate. Acad Med. 2010; 85 Supl 10:S33-6.
-
60Ioannidou F, Konstantikaki V. Empathy and emotional intelligence: what is it really about? Int J Caring Sci. 2008; 1(3):118-23.
-
61Pinto WAM, Rossetti HB, Araújo A, Spósito Júnior JJ, Salomão H, Mattos SS, et al. Impact of a continuous education program on the quality of assistance offered by intensive care physiotherapy. Rev Bras Ter Intensiva. 2014; 26(1):7-12.
-
62Twig G, Lahad A, Kochba I, Ezra V, Mandel D, Shina A, et al. Effect of a tailor-made continuous medical education program for primary care physicians on self-perception of physicians’ roles and quality of care. Isr Med Assoc J. 2010; 12(9):521-5.
-
63Weiner SJ, Jackson JL, Garten S. Measuring continuing medical education outcomes: a pilot study of effect size of three CME interventions at an SGIM annual meeting. J Gen Intern Med. 2009; 24(5):626-9.
-
64Hanna LA, Barry J, Donnelly R, Hughes F, Jones D, Laverty G, et al. Using debate to teach pharmacy students about ethical issues. Am J Pharm Educ. 2014; 78(8):57.
-
65Nguyen VQC, Hirsch MA. Use of a policy debate to teach residents about health care reform. J Grad Med Educ. 2011; 3(3):376-8.
-
66Strawbridge JD, Barrett AM, Barlow JW. Interprofessional ethics and professionalism debates: findings from a study involving physiotherapy and pharmacy students. J Interprof Care. 2014; 28(1):64-5.
-
67Payne H, Pelz F, Brooks R, Horrocks L, Kemp A, Webb E, et al. Benefits of interprofessional learning: an interprofessional MSc in child health. Hosp Med. 2005; 66(4):239-41.
-
68Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev. 2013; 3:CD002213.
-
69Fidler DC, Khakoo R, Miller LA. Teaching scholars programs: faculty development for educators in the health professions. Acad Psychiatry. 2007; 31(6):472-8.
-
70Jhaveri KD, Chawla A, Shah HH. Case-based debates: an innovative teaching tool in nephrology education. Ren Fail. 2012; 34(8):1043-5.
-
71Hicks J. Students’ views of cooperative learning and group testing. Radiol Technol. 2007; 78(4):275-83.
Publication Dates
-
Publication in this collection
03 July 2017 -
Date of issue
Apr-Jun 2018
History
-
Received
13 Dec 2016 -
Accepted
21 Feb 2017