






Abstract
Meperidine (Demerol®) is a mu- and kappa-opiate receptor agonist used for moderate to severe pain. Overdose can result in respiratory depression, hypotension and coma, while accumulation of its toxic metabolite, normeperidine, can cause delirium and seizures. Little data exist examining the inter- and intrasubject variability of the normeperidine-to-meperidine metabolic ratio (MR) in urine. This retrospective data analysis examined meperidine and normeperidine urine concentrations collected from chronic pain patients. In 98 subjects with multiple visits, the geometric mean urinary MR = 6.1 (coefficient of variation, %CV = 68%). From single specimens obtained from 799 subjects, the geometric mean urinary MR = 6.2 (%CV = 212%). The urinary MR increased in young subjects compared with elderly (P = 0.004) and middle-aged subjects (P = 0.01). A 27% difference was found between the male and female urinary MR (male geometric mean MR = 5.1, female geometric mean MR = 7.0, P = 0.02). Intersubject variability in meperidine metabolism was 3-fold greater than intrasubject variability. A significant difference in the urinary MR was found between males and females. The substantial variability in meperidine metabolism and the serious side effects of its metabolite normeperidine require greater vigilance in patient medication monitoring.
Introduction
Meperidine (Demerol®, pethidine [INN]) is a synthetic opioid analog indicated for moderate-to-severe pain (1). It was first synthesized in 1939 and initially considered to be a safer substitute for morphine, due to its antispasmodic qualities and short duration of action. Evidence exists that side effects such as nausea, vomiting, constipation and urinary retention are less likely with meperidine than other opioids (2, 3). Meperidine was one of the most commonly used narcotic analgesics in the USA, at one point being prescribed by up to 60% of physicians for acute pain and 22% for chronic pain (4–6). Administration has become less common due to more awareness of serious side effects. Several organizations have published recommendations for restrictions against its use (7, 8). Meperidine may still be prescribed due to physician familiarity with the medication, adverse reactions to other opioids and/or patient preference (8–10). Meperidine is clinically used for pain associated with pancreatitis, vasoocclusive pain associated with sickle-cell disease, for patients intolerant to morphine and as an analgesic during labor (11–15).
Meperidine acts as an opioid-receptor agonist with high affinity for mu receptors and moderate affinity for kappa receptors, which impart its analgesic property and antishivering activity (16–18). Meperidine is metabolized extensively in the liver, excreted renally and has an oral bioavailability ranging from 30 to 60% (10). Meperidine undergoes N-demethylation by cytochrome P450 (CYP) 2B6, 3A4 and 2C19 to normeperidine, which is also renally excreted (19). Both meperidine and normeperidine may be hydrolyzed to the inactive metabolites meperidinic acid and normeperidinic acid, respectively. The acid forms then undergo conjugation (20) (Figure 1). In healthy patients, meperidine has a half-life ranging from 2.5 to 4 h, whereas the half-life of normeperidine is ∼4–21 h (9). Normeperidine accumulates after multiple doses of meperidine particularly in renal failure, where normeperidine half-life approximates to 34.4 h (6).
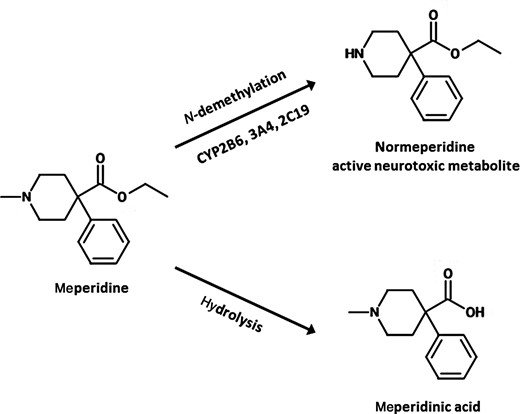
Meperidine metabolism.
Similar to morphine, meperidine is a Schedule II controlled substance with high abuse potential. Overdose can result in respiratory and circulatory depression (1), whereas accumulation of the toxic metabolite, normeperidine, can cause delirium and seizures (4, 6, 9, 10, 21). Meperidine differs from other opioids in that its symptoms of toxicity are not reversible. While the opioid antagonist, naloxone, may reverse respiratory depression, seizures may be exacerbated (22).
High metabolic ratios (MRs) of normeperidine-to-meperidine concentration in plasma have been associated with central nervous system (CNS) excitation leading to seizures and even death (6, 22). Complicating the ability to accurately predict the metabolism of meperidine is the observed intra- and intersubject variability in plasma MR. Considerable intra- and intersubject plasma MR variabilities have been found (up to 5- and 7-folds, respectively) (23). Age, in particular, has been shown to affect meperidine plasma concentrations (24).
Although studies have been carried out examining the variability of plasma MR, little data exist on urinary MR intra- and intersubject variability (6, 25). A urinary MR is a parameter used in urine drug testing in patient monitoring, which can determine possible misuse/use (26). An understanding of which factors influence the urinary MR variability is important in order to accurately interpret urinary MR values. This analysis aims to provide reference ranges for intra- and intersubject urinary MR variability and to examine the effect of sex, age and urinary pH on MR.
Methods
Collection and sorting
This was a retrospective data analysis that received the Institutional Review Board exempt status from the University of California, San Diego Human Research Protection Program. De-identified urine specimens were collected from patients receiving prescription medication treatment for chronic pain at clinician offices throughout the USA and mailed to Millennium Laboratories (San Diego, CA, USA) for drug testing. The specimens in this retrospective analysis were received between October 2009 and May 2011.
Specimen data including specimen creatinine concentration, urinary pH, subject sex and age were compiled into a Microsoft Excel (Microsoft Corp., Redmond, WA, USA) spreadsheet. The database was then sorted to exclude specimens with a creatinine concentration of <20 mg/dL as this value is consistent with dilution or tampering (27). The database was further sorted to exclude specimens that were not tested for meperidine and specimens with meperidine or normeperidine concentrations less than the lower limit of quantitation (LLOQ) of 50 ng/mL (Figure 2).
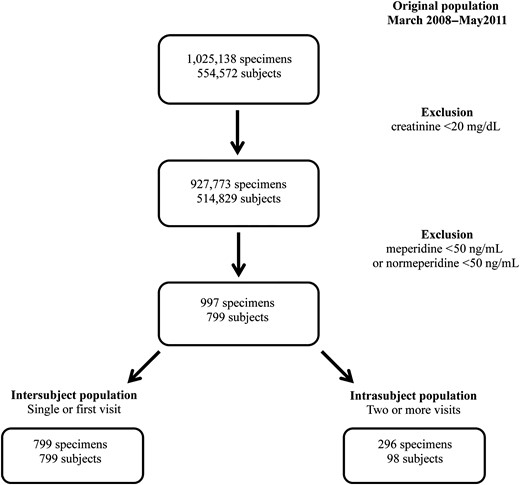
Summary flowchart depicting the inclusion criteria for the selection of the inter- and intrasubject populations.
LC–MS-MS analysis
Parent medication and metabolite concentrations from urine specimens were quantitated using LC–MS-MS at Millennium Laboratories. An Agilent 1200 series binary pump SL LC system, well plate sampler and thermostatted column compartment paired with an Agilent triple Quadrupole mass spectrometer and Agilent Mass Hunter software were used for the analysis of meperidine and normeperidine. A four-point calibration curve was created by using a linear fit and forcing the line to go through the origin. Accepted accuracy for calibrators was ±20% of the target value and the coefficient of determination (R2) was required to be ≥0.99 as verification of linearity and goodness of fit. An LLOQ for both the meperidine and normeperidine was 50 ng/mL. The upper limit of linearity for both the meperidine and normeperidine assays was 100,000 ng/mL.
Chromatographic separation was performed using an acetonitrile–formic acid–water gradient running at 0.4 mL/min and 2.1 × 50 mm, a 1.8-µm Zorbax SB C 18 column. Mobile Phase A = +0.1% formic acid in water, B = 0.1% formic acid in acetonitrile and column temperature was set to 50°C.
All spectra were collected using positive electrospray ionization. The optimized instrumental parameters were as follows: gas temperature, 350°C; drying gas, 12 L/min; nebulizer gas (nitrogen), 35 psi (∼24,100 Pa); capillary voltage, 3,000 V and fragmenter voltage, 60 V. Multiple reaction monitoring (MRM) mode was used for quantitation. Scan time was set to 500 ms. In the MRM mode, two transitions were used to identify and quantitate a single compound. Data were acquired running the QQQ in the MRM mode, using transitions meperidine-D4: 252.3 → 224.2, meperidine: 248.3 → 220.3, 248.3 → 174.2, normeperidine D4: 238.3 → 164.2, normeperidine: 234.1 → 188.1, 234.1 → 160.1.
A quantitative transition was used to calculate concentration based on the quantifier ion and a second transition was used to ensure accurate identification of the target compound based on the ratio of the quantifier ion to the quantifier ion.
HPLC grade water, acetonitrile, methanol and formic acid were obtained from VWR (Westchester, PA, USA). Meperidine and normeperidine were obtained from Cerilliant Corp. (Round Rock, TX, USA). The deuterated internal standards were diluted to 1,000 ng/mL by adding them to synthetic urine (Microgenics Corp., Fremont, CA, USA).
Variability and confounding variables
The intrasubject population consisted of specimen data taken from subjects with two or more office visits, resulting in 296 specimens from 98 subjects. The intersubject population consisted of specimen data from the first visit of those 98 subjects and an additional 701 subjects. To examine the relationship between urinary MR and age, subjects were divided into three age categories: young (17–36 years old), middle-aged (37–65 years old) and elderly (66–90 years old). Age categories were based on those established in a previous study (28).
Statistical analysis and calculations
Summary statistics were calculated with Microsoft Excel 2010. Statistical analyses and graphical representations were created using OriginPro 8.5.1 (OriginLab, Northampton, MA, USA). Meperidine and normeperidine concentrations were creatinine-corrected (mg/g of creatinine) in order to normalize for variations in water intake and hydration (29). Means and 95% confidence intervals (95% CI) were determined for meperidine and normeperidine. Urinary MRs were calculated as the concentration of metabolite divided by the concentration of parent medication ([normeperidine]/[meperidine]). Values were log-transformed in order to approximate a Gaussian distribution and then back-transformed (geometric data) for reporting in summary statistics. Percent coefficient of variation (%CV) was calculated as standard deviation/mean × 100% and employed as a measure of variability. Intrasubject variability was calculated by taking the mean of each subject's %CV. Two-sample t-tests were employed to compare populations. Statistical significance was defined as P < 0.05.
Results
Meperidine and normeperidine concentrations in urine
The intrasubject population had a geometric mean meperidine concentration of 1.9 mg/g creatinine and a geometric mean normeperidine concentration of 11 mg/g creatinine. Summary statistics for the intrasubject population are summarized in Table I.
Intrasubject (n = 98) population: summary statistics for meperidine, normeperidine and urinary MR
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 1.85 | 11.2 | 6.12 |
| 95% Confidence interval | 1.42–2.42 | 8.78–14.4 | 4.81–7.79 |
| 25th Percentile | 0.904 | 5.46 | 3.38 |
| 75th Percentile | 4.45 | 27.7 | 11.3 |
| % Coefficient of variation | – | – | 67.8 |
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 1.85 | 11.2 | 6.12 |
| 95% Confidence interval | 1.42–2.42 | 8.78–14.4 | 4.81–7.79 |
| 25th Percentile | 0.904 | 5.46 | 3.38 |
| 75th Percentile | 4.45 | 27.7 | 11.3 |
| % Coefficient of variation | – | – | 67.8 |
Meperidine and normeperidine concentrations are creatinine-corrected.
Intrasubject (n = 98) population: summary statistics for meperidine, normeperidine and urinary MR
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 1.85 | 11.2 | 6.12 |
| 95% Confidence interval | 1.42–2.42 | 8.78–14.4 | 4.81–7.79 |
| 25th Percentile | 0.904 | 5.46 | 3.38 |
| 75th Percentile | 4.45 | 27.7 | 11.3 |
| % Coefficient of variation | – | – | 67.8 |
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 1.85 | 11.2 | 6.12 |
| 95% Confidence interval | 1.42–2.42 | 8.78–14.4 | 4.81–7.79 |
| 25th Percentile | 0.904 | 5.46 | 3.38 |
| 75th Percentile | 4.45 | 27.7 | 11.3 |
| % Coefficient of variation | – | – | 67.8 |
Meperidine and normeperidine concentrations are creatinine-corrected.
The intersubject population had a geometric mean meperidine concentration of 0.95 mg/g creatinine and a geometric mean normeperidine concentration of 5.9 mg/g creatinine. Summary statistics for the intersubject population are presented in Table II. The log-transformed meperidine and normeperidine concentrations exhibited a Gaussian distribution (Figure 3A and B). Meperidine and normeperidine concentrations demonstrated a linear relationship, with no apparent saturation of metabolism at the upper ranges.
Intersubject (n = 799) population: summary statistics for meperidine, normeperidine and urinary MR
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 0.947 | 5.87 | 6.20 |
| 95% Confidence interval | 0.257–3.68 | 5.32–6.48 | 5.60–6.87 |
| 25th Percentile | 0.257 | 2.36 | 2.48 |
| 75th Percentile | 3.68 | 14.9 | 16.7 |
| % Coefficient of variation | – | – | 212 |
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 0.947 | 5.87 | 6.20 |
| 95% Confidence interval | 0.257–3.68 | 5.32–6.48 | 5.60–6.87 |
| 25th Percentile | 0.257 | 2.36 | 2.48 |
| 75th Percentile | 3.68 | 14.9 | 16.7 |
| % Coefficient of variation | – | – | 212 |
Meperidine and normeperidine concentrations are creatinine-corrected.
Intersubject (n = 799) population: summary statistics for meperidine, normeperidine and urinary MR
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 0.947 | 5.87 | 6.20 |
| 95% Confidence interval | 0.257–3.68 | 5.32–6.48 | 5.60–6.87 |
| 25th Percentile | 0.257 | 2.36 | 2.48 |
| 75th Percentile | 3.68 | 14.9 | 16.7 |
| % Coefficient of variation | – | – | 212 |
| Meperidine (mg/g creatinine) | Normeperidine (mg/g creatinine) | Urinary MR (normeperidine/meperidine) | |
|---|---|---|---|
| Mean | 0.947 | 5.87 | 6.20 |
| 95% Confidence interval | 0.257–3.68 | 5.32–6.48 | 5.60–6.87 |
| 25th Percentile | 0.257 | 2.36 | 2.48 |
| 75th Percentile | 3.68 | 14.9 | 16.7 |
| % Coefficient of variation | – | – | 212 |
Meperidine and normeperidine concentrations are creatinine-corrected.
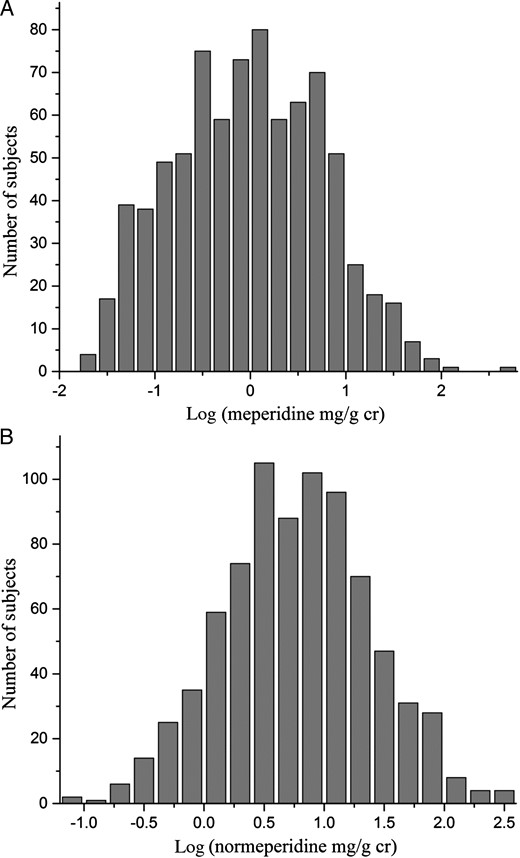
(A) Histogram of meperidine concentrations. Log-transformed, creatinine-corrected meperidine urinary concentrations in the intersubject population approach a Gaussian distribution. (B) Histogram of normeperidine concentrations. Log-transformed, creatinine-corrected normeperidine urinary concentrations in the intersubject population approach a Gaussian distribution.
Intra- and intersubject variability of MR
The intrasubject population consisted of 98 subjects with two or more separate office visits. The geometric mean urinary MR of the intrasubject population was 6.1. Log-transformed urinary MRs of the intrasubject population approach a Gaussian distribution (Figure 4A). Intrasubject variability ranged from %CV = 2–159%, with a mean %CV = 68%. The intersubject population consisted of 799 subjects with a geometric mean urinary MR of 6.2. Log-transformed urinary MRs of the intersubject population exhibit a Gaussian distribution (Figure 4B). The intersubject variability resulted in a %CV of 212%.
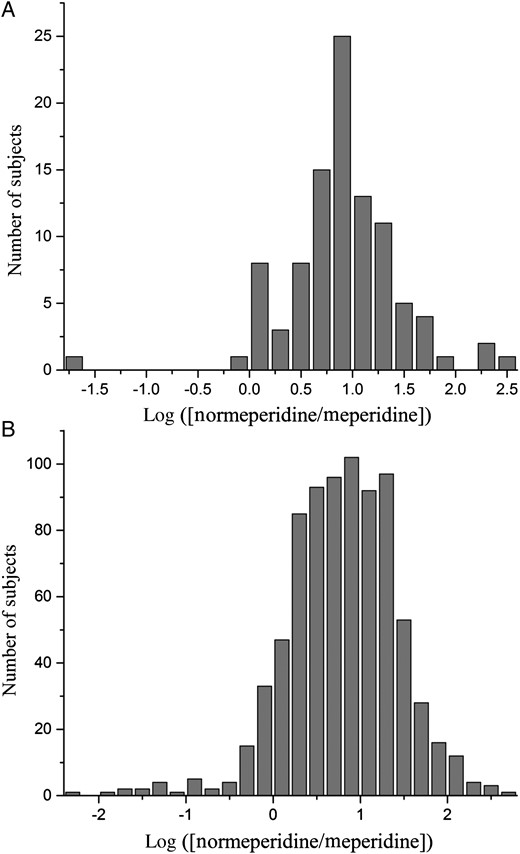
(A) Histogram of urinary MRs in the intrasubject population. Log-transformed, creatinine-corrected urinary MRs approach a Gaussian distribution. (B) Histogram of urinary MRs in the intersubject population. Log-transformed, creatinine-corrected urinary MRs approach a Gaussian distribution.
Sex, age, urine pH and MR
In the intersubject population, male geometric mean urinary MR was 5.1 (95% CI: 4.3–6), whereas female geometric mean urinary MR was 7.0 (95% CI: 6.2–7.9), with a 27% difference (P = 0.02) (Table III). The geometric mean urinary MRs of young, middle-aged and elderly subjects were 8.9, 5.9 and 5.1, respectively (Table IV). The urinary MR in young subjects was significantly higher compared with elderly (P = 0.004) and middle-aged subjects (P = 0.01). No significant difference was found between urinary MR in middle-aged, compared with elderly, subjects. Further stratification of age categories by sex revealed overall similar relationships with the age-only analysis. However, the male elderly category exhibited a smaller amount of variability in urinary MR (%CV = 87%).
Male and female summary statistics for urinary MR in the intersubject population
| Male urinary MR (N = 291) | Female urinary MR (N = 508) | |
|---|---|---|
| Mean | 5.07 | 6.97 |
| 95% Confidence interval | 4.26–6.04 | 6.15–7.89 |
| 25th Percentile | 2.24 | 2.75 |
| 75th Percentile | 14.8 | 17.4 |
| % Coefficient of variation | 184 | 215 |
| Male urinary MR (N = 291) | Female urinary MR (N = 508) | |
|---|---|---|
| Mean | 5.07 | 6.97 |
| 95% Confidence interval | 4.26–6.04 | 6.15–7.89 |
| 25th Percentile | 2.24 | 2.75 |
| 75th Percentile | 14.8 | 17.4 |
| % Coefficient of variation | 184 | 215 |
Male and female summary statistics for urinary MR in the intersubject population
| Male urinary MR (N = 291) | Female urinary MR (N = 508) | |
|---|---|---|
| Mean | 5.07 | 6.97 |
| 95% Confidence interval | 4.26–6.04 | 6.15–7.89 |
| 25th Percentile | 2.24 | 2.75 |
| 75th Percentile | 14.8 | 17.4 |
| % Coefficient of variation | 184 | 215 |
| Male urinary MR (N = 291) | Female urinary MR (N = 508) | |
|---|---|---|
| Mean | 5.07 | 6.97 |
| 95% Confidence interval | 4.26–6.04 | 6.15–7.89 |
| 25th Percentile | 2.24 | 2.75 |
| 75th Percentile | 14.8 | 17.4 |
| % Coefficient of variation | 184 | 215 |
Young, middle-aged and elderly summary statistics for urinary MR in the intersubject population
| Young (N = 108) 17- to 36-year-old urinary MR | Middle-aged (N = 589) 37- to 65-year-old urinary MR | Elderly (N = 80) 66- to 90-year-old urinary MR | |
|---|---|---|---|
| Mean | 8.91 | 5.90 | 5.11 |
| 95% Confidence interval | 6.65–11.94 | 5.22–6.65 | 4.04–6.52 |
| 25th Percentile | 2.79 | 2.37 | 2.83 |
| 75th Percentile | 25.75 | 16.27 | 9.49 |
| % Coefficient of variation | 206 | 176 | 229 |
| Young (N = 108) 17- to 36-year-old urinary MR | Middle-aged (N = 589) 37- to 65-year-old urinary MR | Elderly (N = 80) 66- to 90-year-old urinary MR | |
|---|---|---|---|
| Mean | 8.91 | 5.90 | 5.11 |
| 95% Confidence interval | 6.65–11.94 | 5.22–6.65 | 4.04–6.52 |
| 25th Percentile | 2.79 | 2.37 | 2.83 |
| 75th Percentile | 25.75 | 16.27 | 9.49 |
| % Coefficient of variation | 206 | 176 | 229 |
Young, middle-aged and elderly summary statistics for urinary MR in the intersubject population
| Young (N = 108) 17- to 36-year-old urinary MR | Middle-aged (N = 589) 37- to 65-year-old urinary MR | Elderly (N = 80) 66- to 90-year-old urinary MR | |
|---|---|---|---|
| Mean | 8.91 | 5.90 | 5.11 |
| 95% Confidence interval | 6.65–11.94 | 5.22–6.65 | 4.04–6.52 |
| 25th Percentile | 2.79 | 2.37 | 2.83 |
| 75th Percentile | 25.75 | 16.27 | 9.49 |
| % Coefficient of variation | 206 | 176 | 229 |
| Young (N = 108) 17- to 36-year-old urinary MR | Middle-aged (N = 589) 37- to 65-year-old urinary MR | Elderly (N = 80) 66- to 90-year-old urinary MR | |
|---|---|---|---|
| Mean | 8.91 | 5.90 | 5.11 |
| 95% Confidence interval | 6.65–11.94 | 5.22–6.65 | 4.04–6.52 |
| 25th Percentile | 2.79 | 2.37 | 2.83 |
| 75th Percentile | 25.75 | 16.27 | 9.49 |
| % Coefficient of variation | 206 | 176 | 229 |
Urine pH of each specimen in the intersubject population was plotted against subject urinary MR (Figure 5). A weak, positive relationship was found between specimen urine pH and urinary MR (log urinary MR = 0.20 × [specimen urine pH] − 0.44, R2 = 0.08, P < 0.001). This would indicate a higher urinary MR in alkaline urine. Similarly, a positive relationship was also found between specimen urine pH and urinary MR in the intrasubject population, with slope ranging from 0.27 to 0.43 and R2 ranging from 0.37 to 0.67 (data taken only from subjects in the intrasubject population with significant linear regression analyses, P < 0.05.)
![Relationship between urinary pH and urinary MR. Specimen urinary pH is plotted against log-transformed urinary MR (normeperidine/meperidine). Also shown is a linear regression fit (log ([normeperidine]/[meperidine]) = 0.20 × (specimen urine pH) − 0.44, R2 = 0.08, P < 0.001.](https://oup.silverchair-cdn.com/oup/backfile/Content_public/Journal/jat/38/1/10.1093/jat/bkt087/2/m_bkt08705.jpeg?Expires=1716427388&Signature=wxXU7rk5wNPzLRVVTugOhBYYeVD33d7TLENzNDfgVgw71q14YaJ8eZC67qrVKQw8STNLZxbidMM3Xp-WiSwIIMVlkB6OSzCtE3FN2iMi~vvTZJHcy-ICEOzq32jKudwUW-hDYAoP1BfHCEJWdH~MjZek45GThhyG52QPiTp~MU0HK6dWGwz5tJzSm1tBADsD1~yKQt~GtF0oZoHDu6FzYQtDIr5JOBtbfwIPGsYA77oDTDEfgr5ixjsJV9Ac5E1~rd4oumN6Tm5WyNkI3rRJ0lpkttmc3HdVnlpHLlxlBnxw80neDJ4eWprA29s2wT1qV-LI8acBkM9lIPD3qhsILQ__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Relationship between urinary pH and urinary MR. Specimen urinary pH is plotted against log-transformed urinary MR (normeperidine/meperidine). Also shown is a linear regression fit (log ([normeperidine]/[meperidine]) = 0.20 × (specimen urine pH) − 0.44, R2 = 0.08, P < 0.001.
Discussion
The geometric mean urinary MR of the intersubject population was 6.2, indicating roughly six times the concentration of normeperidine to meperidine in the urine. This high urinary MR may be caused by a prolonged normeperidine elimination half-life (t½ = 15–30 h) compared with meperidine (t½ = 2.4–4 h) (10). However, previously documented MRs in both plasma and urine are lower than the meperidine urinary MR found in this analysis (6, 20, 22, 25, 30). This may be due to differences in the sample population, dosing of meperidine, time of specimen collection and sample size. The high urinary MR in this analysis suggests rapid metabolism and/or substantial metabolite accumulation. This finding may help better understand meperidine side effects observed in renally impaired patients and patients taking repeated doses of meperidine. Given normeperidine's neurotoxicity, substantial accumulation may have serious consequences, causing delirium and seizures. The study by Kaiko et al. (22) found a mean plasma MR of 1.3 in patients with mild symptoms, while patients experiencing tremors and seizures had mean plasma MRs of 2.2 and 3.0, respectively. Szeto et al. (6) found plasma MRs of 4.8 and 6.4 in patients experiencing neurotoxicity. Clark et al. (9) support the role of high plasma MR over normeperidine concentration alone as a better indicator of neurotoxicity. Clark et al. propose that the CNS depressant activity of meperidine is protective of normeperidine-induced seizures. Indeed, CNS stimulation caused by normeperidine is not reversed by naloxone. Rather, naloxone's removal of meperidine CNS depression may precipitate seizures in a patient with normeperidine toxicity. However, Plummer et al. postulated that plasma MR is not a significant predictor in causing toxicity. Instead, high normeperidine concentrations due to accumulation may be the primary factor (10). Despite this, reliable toxic ranges of plasma meperidine and normeperidine have not been established. Kaiko et al. found a considerable overlap in ranges of plasma meperidine and normeperidine concentrations between asymptomatic and symptomatic patients (22). Tolerance due to chronic use of meperidine or other opioids may be a factor in this overlap.
Lethal concentrations reported in meperidine overdoses have a wide range as well. Siek reported 150 ng/mL urinary meperidine and 50 ng/mL urinary normeperidine in a fatality after oral ingestion of meperidine, and a range of 2–24 ng/mL urinary meperidine and 0.1–79 ng/mL urinary normeperidine in fatalities after intravenous administration of meperidine (31). The resulting urinary MRs range from 0.05 to 3.45. Time between administration of meperidine and time of death was not reported in the analysis, but likely had an effect on the urinary MRs.
Intersubject variability in meperidine metabolism was 3-fold greater than intrasubject variability (212/68%). Intrasubject variability ranged from 2 to 159%. This large range of variability implies unpredictability in meperidine metabolism. For most opioids, intersubject variability may be influenced by confounding factors such as genetic polymorphisms in CYP enzymes, ethnicity, disease states (such as hepatic and renal failure) and body mass, which were not examined in this analysis (32–34). A study by Chan et al. found that Asian subjects had a higher normeperidine : meperidine urinary excretion ratio than Caucasians under acidic urinary conditions (35, 36). Such racial differences may be from the known incidence of CYP2C19 polymorphisms (37, 38).
Of the factors examined in these analyses, sex and age contributed little to intersubject variability, with the exception of the male elderly category. Males between the ages of 67 and 90 exhibited an intersubject %CV of 89%. This low variability may be due to the small sample size of this category (n = 27).
Few studies have specifically examined the effect of these factors on urinary MR intra- and intersubject variability. Our analysis found an intersubject %CV in the MR of 212%. In previous studies, urinary excretion data from a small (n = 6) study indicate an intersubject %CV in the MR of 61% in healthy subjects (39). Urinary excretion data taken from another small sample size study (n = 5) result in a calculated intersubject %CV in the MR of 54.4%. Data taken from Szeto et al. resulted in a calculated plasma intersubject %CV of 27% in cancer patients (n = 7) and 49% in renal failure patients (n = 7) (6). The intersubject %CV of 212% in this analysis was larger compared with previous studies. This may be due to differences in study design. Previous studies had smaller sample sizes and a population of healthy subjects, cancer patients or renal failure patients. The population of this analysis included patients treated with chronic opioid therapy, with information on other disease states not available.
Our analysis found a higher urinary MR in females compared with males. A previous study has found that females experience more opioid side effects (nausea and vomiting), while another found no significant difference between sexes in neurotoxic effects from meperidine (2, 22). Information on side effects experienced by subjects was unavailable for this dataset. However, if the higher female urinary MRs found in this analysis were due to an increased metabolism of meperidine leading to greater formation of normeperidine, this would imply greater potential for neurotoxic effects in females. In addition, studies have found sex-dependent differences in CYP450 3A enzymes, with females exhibiting significantly greater hepatic CYP3A expression compared with males (40, 41). Considering the abundance of CYP3A4 enzyme in the liver and its role in meperidine N-demethylation, the higher urinary MR observed in females in this analysis is reasonable.
Our analysis has found a lower urinary MR in elderly, compared with young, subjects. These results are in agreement with a study by Odar-Cederlof et al. (42) that found similar excretion of meperidine in young (18–30 years old) and old (over 65 years old) patients, but decreased excretion of normeperidine in old patients. However, contrasting results have been published elsewhere. A previous study found that older subjects (over 70 years old) exhibited increased normeperidine excretion and decreased meperidine excretion, implying a higher urinary MR compared with younger subjects (under 30 years old) (43). The contrasting result found in our analysis may be due to differences in study design, such as sample size and patient population (healthy patients versus patients with pain). Older subjects have also exhibited an increased risk of respiratory depression due to opioid use (2), and more frequent adverse drug reactions to meperidine (11).
Our analysis found a weak, positive relationship between urine pH and urinary MR in the intersubject population (R2 = 0.08, P < 0.001). A positive relationship between urine pH and urinary MR was also found in the intrasubject population, with a stronger correlation coefficient (R2 range: 0.37–0.67, P < 0.05). Acidification of urine was found to increase urinary excretion of both meperidine and normeperidine in earlier studies (6, 43). Verbeeck et al. (30) found that meperidine excretion increased by 22-fold as urine pH was decreased, while normeperidine increased only 4-fold.
As this was a retrospective analysis, a limitation of this study was that a more complete set of information was not accessible. Dose amount, dose interval and elapsed time between medication administration and urine collection were not available. Due to the nature of urine drug tests in pain management offices, the dose of meperidine, the time of last dose and time of collection of urine specimens from patients could not be accounted for or controlled. Patient characteristics (such as race, CYP2C19 genotype status, body mass and the presence of hepatic or renal disease) were also not available. However, a large sample size was used in this study design in an attempt to correct for random urine specimen collection and to reduce impact on urinary MR and variability.
Conclusion
Despite the well-documented severe side effects following meperidine administration, particularly with chronic use, meperidine is still used today. Meperidine and normeperidine urinary concentrations demonstrated a linear relationship, with no apparent saturation of metabolism at the upper ranges. The characterization of meperidine metabolism, including the differences in urinary MR based on sex, age and urinary pH, may impact a prescriber's approach to meperidine. Our analysis found a higher urinary MR in females compared with males and a lower urinary MR in elderly, compared with younger, subjects. A positive relationship between urine pH and urinary MR was also found in both intra- and intersubject populations. The substantial variability in meperidine metabolism and the serious side effects of its metabolite normeperidine require greater vigilance in patient drug monitoring. The results presented here may help pain providers assess the effectiveness of therapy, assist in establishing a reference range for monitoring urine meperidine and normeperidine concentrations and may help to explain meperidine-associated adverse events and potential abuse.
Funding
This work was supported in part by an educational grant provided by the University of California, San Diego Skaggs School of Pharmacy and Pharmaceutical Sciences from an unrestricted gift from the Millennium Research Institute (to K.V.M.).
Acknowledgments
The authors acknowledge Amadeo J. Pesce, PhD, DABCC, for his crucial guidance and support throughout the entirety of this study. Urine specimens were tested and provided by Millennium Laboratories. Dr Joseph D. Ma is a paid consultant of Millennium Laboratories, Inc.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}