





Abstract
The isolation and treatment of symptomatic individuals, coupled with the quarantining of individuals that have a high risk of having been infected, constitute two commonly used epidemic control measures. Although isolation is probably always a desirable public health measure, quarantine is more controversial. Mass quarantine can inflict significant social, psychological, and economic costs without resulting in the detection of many infected individuals. The authors use probabilistic models to determine the conditions under which quarantine is expected to be useful. Results demonstrate that the number of infections averted (per initially infected individual) through the use of quarantine is expected to be very low provided that isolation is effective, but it increases abruptly and at an accelerating rate as the effectiveness of isolation diminishes. When isolation is ineffective, the use of quarantine will be most beneficial when there is significant asymptomatic transmission and if the asymptomatic period is neither very long nor very short.
When the global severe acute respiratory syndrome (SARS) outbreak began in 2003, public health officials in all affected areas scrambled to introduce measures aimed at controlling its spread. Initially, this mainly involved alerting health-care providers and providing them with diagnostic protocols. This allowed many of the SARS cases to be identified, thereby making the isolation and treatment of infected individuals more effective. It was soon recognized, however, that the extent to which the disease had spread was much greater than initially thought (1–4). As a result, several countries/regions introduced the use of mass quarantine for all individuals suspected of having had contact with a confirmed SARS case. These coordinated global efforts were remarkably effective at curtailing the spread of the disease, and to date SARS has not made a significant reemergence.
This recent experience with SARS has illustrated that there are two central questions that must be addressed by policy makers in the face of an emerging or reemerging infectious disease. The first is whether or not basic public health measures, such as isolation (i.e., the removal of symptomatic individuals from the general population) and quarantine (i.e., the removal of individuals who have had contact with an infected individual but are not displaying symptoms), are likely to be sufficient to control the spread of the disease. A recent paper by Fraser et al. (5) has provided a very general answer to this question, and they demonstrate that the crucial factors are the extent to which the disease is transmitted asymptomatically, as well as its basic reproduction number (5).
For cases where these basic public health measures are sufficient (e.g., SARS), the second question is then whether or not both isolation and quarantine should be used. For example, even in retrospect, it is not clear whether isolation or quarantine had the greater impact in stopping the spread of SARS, or whether both control measures were essential (1, 6–9). This is an important question, because the use of mass quarantine is controversial. In the case of SARS, for example, only a tiny percentage of the quarantined individuals were actually infected (7, 8, 10). While it is true that the removal of even a small number of infected individuals from the general population is likely to be beneficial from the standpoint of community health, it definitely impinges upon individual rights and freedoms. Moreover, as seen in the case of SARS, it also imposes considerable economic and social costs (10–12).
By use of a variety of modeling approaches, several previous studies have examined the extent to which quarantine was probably important in stopping the spread of SARS in different locales. These include the typical continuous-time or discrete-time compartmental models tailored specifically to the case of SARS (13–17), as well as more sophisticated contact-network models (18, 19). Although the results are somewhat mixed, a reasonably general conclusion stemming from all of the above studies is that SARS is likely to be effectively contained in the absence of quarantine only if very stringent and effective isolation measures are in place.
In this article, we derive general mathematical results that predict the number of infections averted when quarantine is used in addition to isolation for arbitrary diseases. Our goal is to elucidate the factors that make quarantine a relatively effective control measure for some diseases but not for others. We suppose that an emerging infectious disease is in the initial stages of spreading within a community and assume that isolation and treatment of symptomatic individuals are about to be imposed as the primary measures to halt the spread of the disease. Our index of the utility of quarantine is the number of infections that can be averted if quarantine is used in addition to isolation/treatment. We relate the expected utility of quarantine to observable parameters of a disease outbreak, so that it might be used to inform policy decisions.
MATERIALS AND METHODS
The transmission of many diseases can be viewed as a branching process, whereby each infected individual gives rise to some number of new infections before either dying or recovering (Web appendix 1). (This information is described in the first of four supplementary appendices; each is referred to as “Web appendix” in the text and is posted on the Journal's website (http://aje.oxfordjournals.org/).) Typically, we expect the number of susceptible hosts to decline during this process, but because we are considering the initial stages of an emerging infectious disease, the number of susceptible individuals will be largely unaffected by the transmission process over the timescale of interest. For example, in the case of SARS, of the approximately 4 million people in the greater Toronto area, only 225 satisfied the case definition of SARS (6).
Given these considerations, in the absence of quarantine, the spread of the disease can be modeled by assuming that each infected individual produces a random number of new infections, RI, the value of which is drawn from some probability distribution, pI(·). This number of new infections includes those generated in all stages of the disease, in the absence of quarantine but in the presence of isolation. For example, it includes all new infections produced while asymptomatic, while symptomatic but not isolated, and while isolated and receiving treatment. The subscript “I” refers to the fact that isolation alone is being used.
If quarantine is used in addition to isolation, then there are two pathways down which an infected individual can travel (figure 1). First, an infected individual can eventually be quarantined before developing symptoms and being placed in isolation. We assume that this happens with probability, q. Thus, if considerable effort and resources are put into quarantine (e.g., through the use of thorough contact tracing), then q will be relatively large. Conversely, q = 0 in the absence of quarantine. Second, an infected individual might escape being quarantined and therefore be removed from the general population only after developing symptoms. This happens with probability 1 − q. We note that, in reality, q will undoubtedly change through time as the efficacy of quarantine procedures increases during an outbreak, but our goal here is to examine the effectiveness of a constant level of quarantine. In this sense, our results can be viewed as a best-case scenario for the utility of quarantine.
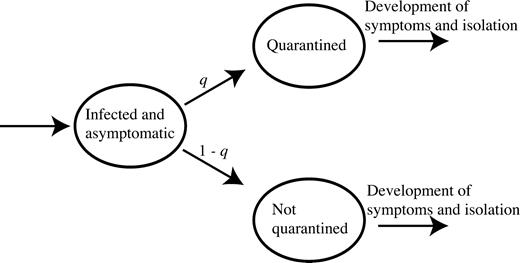
A schematic diagram of the two pathways down which an infected individual can move when quarantine protocols are in place.
Individuals that escape being quarantined generate the same number of new infections as would occur in the absence of quarantine procedures. For those individuals that are placed into quarantine, the number of new infections generated will differ from this. Infections might still be generated while in the asymptomatic stage (before being quarantined), and they can also be generated while in quarantine and/or while in isolation after symptoms develop. We assume that the number of infections generated by such individuals is also a random variable, RQI, but it is drawn from a different distribution, pQI(·).
A key parameter in the results that follow is
Given the parameters q and ρ, the product qρ lies between zero and one, and it is an index of the effectiveness of quarantine at the level of infected individuals; qρ = 0 only when quarantine is absent (i.e., q = 0) and/or when placing an individual into quarantine has no effect on the number of infections that he/she generates (e.g., because there is no asymptomatic transmission and quarantine does not improve isolation procedures). Conversely, qρ ≈ 1 only if all infected asymptomatic individuals are identified and quarantined (i.e., q = 1) and if quarantine (in conjunction with isolation) prevents all disease transmission (i.e., ρ = 1).
RESULTS
The notation in the first set of parentheses in equation 1 represents the percentage of infections that quarantine can be expected to avert. Figure 2a plots equation 1 with I0 = 1 for different values of the product qρ. This represents the number of cases averted by quarantine for each initially infected individual. Even if quarantine is extremely effective (i.e., qρ = 1), which requires that all asymptomatic individuals be identified and placed into quarantine (i.e., q = 1) and that an individual generates no new infections once quarantined (i.e., ρ = 1), quarantine still has only a marginal effect on the expected number of infections averted over a wide range in R̄I (which, recall, is the expected number of infections generated by an infected person if isolation alone is used). For example, if the reproduction number is R̄I = 0.5, then quarantine is predicted to prevent only one extra infection for each individual that was initially infected. The number of infections averted becomes significant, only when the effectiveness of isolation decreases to the point where it is no longer able to stop the spread of disease (i.e., only when R̄I approaches one). Also note that, because of the form of equation 1, its predictions are relatively insensitive to error in the estimates of R̄I unless R̄I is close to one (figure 2).
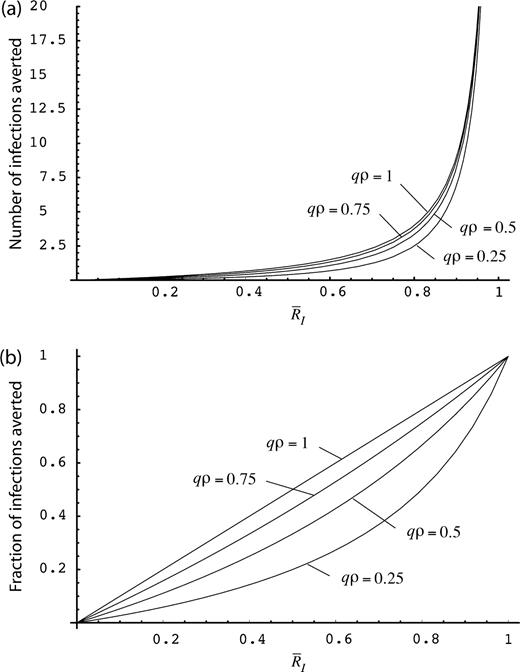
The effect of the reproduction number in the presence of isolation, R̄I, on the efficacy of quarantine, as shown by the total expected number of infections averted by quarantine during an epidemic for each initially infected person (a) and the percentage of infections averted by quarantine during an epidemic (b). The parameter combination qρ is an overall measure of the effectiveness of trying to place an individual into quarantine, q is the probability that an asymptomatic individual will be identified and placed into quarantine, and ρ is the proportion of infections generated by an individual that can be prevented by placing the individual into quarantine (which is roughly equal to the proportion of infections generated by asymptomatic individuals).
The above results give an expectation of the number of infections averted by quarantine, but how likely is it that, by chance, the number might be greater than this? This question is more difficult to answer but, subject to some mild assumptions, one can derive a conservative estimate that applies for any distribution of infections generated by each infected individual, p1(·) or pQI(·) (Web appendix 2). Figure 3 plots a conservative 80th-percentile upper bound on the number of infections averted through the use of quarantine, for the best-case scenario in which the probability of quarantining an infected individual is one (i.e., q = 1). There is at least an 80 percent probability that the actual number of infections averted through the use of perfect quarantine in any given outbreak lies below these upper bounds. These results are very general and further strengthen the finding that quarantine is unlikely to have a significant impact unless isolation alone is relatively ineffective (i.e., R̄I is large). Furthermore, these analytical results appear to be quite conservative when judged against results from a fully stochastic simulation (Web appendix 3).
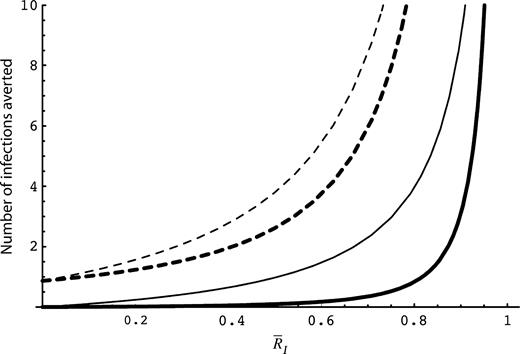
The mean number of infections averted by quarantine (solid curves), along with the mean plus 2 standard deviations (dashed curves). We expect at least 80 percent of the outcomes to lie below the bounds given by the dashed curves (Web appendix 2). Bold curves: σI = 0.5, σQI = 0.25, ρ = 0.05; thin curves: σI = 0.5, σQI = 0.25, ρ = 0.95. All results assume that q = 1.
Further insight can be gained from the above results by examining the case where there is very little asymptomatic transmission (ρ is small). This appears to be true for several diseases (table 1; Web appendix 4), including SARS (1, 4, 9, 20). To apply the results to SARS, we require an estimate for the reproduction number when isolation alone is being used. There are currently no direct estimates of this parameter available, but we can estimate it indirectly by using the component parameter estimates of Gumel et al. (14). Bearing in mind the uncertainty in such estimates, we obtain a potential range of values from R̄I = 0.28 to R̄I = 0.46. Taking R̄I = 0.5 as a conservative estimate, the results given by the bold curve in figure 3 (for which ρ = 0.05) suggest that there is a probability of at least 80 percent that the use of perfect quarantine for SARS (i.e., q = 1) would reduce the number of cases by no more than approximately 2.6 cases for each initially infected person (assuming that the values σI = 0.5 and σQI = 0.25 of figure 3 are reasonable for SARS). This is a very conservative upper bound on the expected outcome, however, and therefore, unless the variance in the number of infections generated by individuals is much larger than those used to generate figure 3, the use of quarantine is predicted to have very little effect. As a result, investing limited resources in ensuring that isolation is very effective (e.g., quick removal of symptomatic people from the population; extremely secure isolation facilities to prevent transmission by such individuals) is likely to be a much more valuable control strategy for SARS than the use of mass quarantine.
Estimates of the proportion of infections that are generated by asymptomatic individuals, ρ, for a variety of diseases*
Disease | Proportion, ρ |
|---|---|
| Whooping cough | 0.25 |
| Scarlet fever | 0.25 |
| Measles | 0.46 |
| Influenza | ∼0.5 |
| Chickenpox | ∼0.53 |
| Mumps | 0.74 |
| Rubella | 0.81 |
| Diphtheria | Relatively high |
| Poliomyelitis | 0.97 |
| Smallpox | ∼1 |
| Hepatitis B | ∼1 |
Disease | Proportion, ρ |
|---|---|
| Whooping cough | 0.25 |
| Scarlet fever | 0.25 |
| Measles | 0.46 |
| Influenza | ∼0.5 |
| Chickenpox | ∼0.53 |
| Mumps | 0.74 |
| Rubella | 0.81 |
| Diphtheria | Relatively high |
| Poliomyelitis | 0.97 |
| Smallpox | ∼1 |
| Hepatitis B | ∼1 |
Refer to Web appendix 4 for more information. Quarantine is expected to be useful only for those diseases that have relatively large values of ρ. Results are based on data from table 3.1 of Anderson and May (23).
Estimates of the proportion of infections that are generated by asymptomatic individuals, ρ, for a variety of diseases*
Disease | Proportion, ρ |
|---|---|
| Whooping cough | 0.25 |
| Scarlet fever | 0.25 |
| Measles | 0.46 |
| Influenza | ∼0.5 |
| Chickenpox | ∼0.53 |
| Mumps | 0.74 |
| Rubella | 0.81 |
| Diphtheria | Relatively high |
| Poliomyelitis | 0.97 |
| Smallpox | ∼1 |
| Hepatitis B | ∼1 |
Disease | Proportion, ρ |
|---|---|
| Whooping cough | 0.25 |
| Scarlet fever | 0.25 |
| Measles | 0.46 |
| Influenza | ∼0.5 |
| Chickenpox | ∼0.53 |
| Mumps | 0.74 |
| Rubella | 0.81 |
| Diphtheria | Relatively high |
| Poliomyelitis | 0.97 |
| Smallpox | ∼1 |
| Hepatitis B | ∼1 |
Refer to Web appendix 4 for more information. Quarantine is expected to be useful only for those diseases that have relatively large values of ρ. Results are based on data from table 3.1 of Anderson and May (23).
DISCUSSION
Our results indicate that there are three main requirements for quarantine to substantially reduce the number of infections that occur during a disease outbreak. These are the following: 1) a large disease reproduction number in the presence of isolation alone; 2) a large proportion of infections generated by an individual that can be prevented through quarantine, ρ; and 3) a large probability that an asymptomatic infected individual will get placed into quarantine before he/she develops symptoms and is isolated, q.
Having a relatively large reproduction number in the presence of isolation is necessary for quarantine to have a substantial impact, but it is not sufficient. It must also be true that a large proportion of infections generated by an individual can be prevented through quarantine (i.e., ρ is large). How can we estimate this parameter for different diseases? As a first approximation, we can equate ρ with the proportion of infections generated when an individual is asymptomatic (5). We can then use the data on the length of infectious periods, along with incubation, latency periods, and the likelihood of completely asymptomatic infections occurring for different diseases to estimate ρ (Web appendix 4). Table 1 presents estimates of the proportion of infections that are generated by asymptomatic individuals for a variety of diseases. The diseases with the largest values of ρ are smallpox and hepatitis B, whereas those with the smallest values of ρ are whooping cough and scarlet fever.
Aside from the above disease-specific factors, there are also some ways in which public health officials can increase the parameter ρ. One possibility is to ensure the strictest adherence to quarantine protocols. This will ensure that the number of infections generated by individuals in quarantine is as small as possible. Second, quarantine can be used to enhance the speed of isolation of symptomatic individuals (e.g., because asymptomatic individuals in quarantine are under close scrutiny). In this case, quarantine would reduce the number of infections generated by an individual, in part, by reducing the number of infections generated by symptomatic individuals. If this is the main reason for ρ being large, however, then there is an alternative to quarantine that might be more suitable. Rather than placing the suspected asymptomatic people into quarantine, simply inform them of their status and tell them to report to a hospital at the first sign of any symptoms. This approach has nearly all the benefits of quarantine in terms of enhancing isolation procedures without incurring the costs of actual quarantine.
Having a relatively large reproduction number and having a relatively large value of ρ are not sufficient for quarantine to have a substantial impact, either, however; it must also be true that q can be made large. This is the probability that an infected, asymptomatic individual will be placed into quarantine before he/she develops symptoms and is isolated. The chief way in which this can be increased is by investing more in rapid contact tracing. Nevertheless, there are two reasons why this might still be infeasible.
First, if the duration of the asymptomatic period is too short, then it is unlikely that much can be done to identify infected individuals prior to their developing symptoms. Of course, there might still be a benefit in attempting to do so through the increased rate at which symptomatic individuals are removed from the population, but this is a matter of quarantine's being useful through its effects on enhancing isolation procedures rather than being useful in itself.
Second, if the duration of the asymptomatic period is too long, then it will be extremely difficult to identify those individuals that are likely to have been infected by a given infected person (by virtue of their having had many contacts during the asymptomatic phase). Furthermore, if the asymptomatic period is very long, then the quarantine period must also be correspondingly long (21). Such lengthy quarantine periods would be very difficult to implement, again making it unlikely that q can be made very large. For example, even though the value of ρ is large for hepatitis B (table 1), it is unlikely that q could be large enough for quarantine to prove a useful control measure for this disease.
It is worth noting that public health interventions aimed at increasing q (e.g., increased effort in contact tracing) might also result in a beneficial increase in ρ. In the development of the model, we have assumed that the likelihood of an individual's being placed into quarantine, q, varied independently of ρ, the proportion of infections that are prevented (per infected individual) by placing a person into quarantine. For some quarantining techniques such as contact tracing, however, increasing the resources devoted to this task in the hopes of increasing q might also increase ρ. In other words, not only would asymptomatic individuals have a greater likelihood of being quarantined, but they would likely be placed into quarantine more quickly as well (thereby potentially increasing ρ). As a result, it is important to bear in mind that any real-world public health intervention can result in alterations to more than one of the relevant parameters in the theory developed here.
Finally, we note that the application of the above results for any emerging or reemerging infectious disease rests heavily on the ability to obtain an estimate of the disease reproduction number in the presence of isolation alone (i.e., RI). There has been much research on the estimation of disease reproduction numbers in general, but a recent paper by Wallinga and Teunis (22) offers the most useful approach in the context of our results. From data from epidemic curves, these researchers presented a real-time method that can be used to estimate the reproduction number over time. Given that isolation will often be the first invention used for emerging diseases, this method might thereby be used to obtain quick estimates of RI in the initial stages of an outbreak.
In summary, the above results suggest that the number of infections averted through the use of quarantine is expected to be very low provided that isolation is effective. If isolation is ineffective, then the use of quarantine will be most beneficial only when there is significant asymptomatic transmission and if the asymptomatic period is neither very long nor very short.
Editor's note: References 24–32 are cited in the Web-only appendices posted on the Journal's website (http://aje.oxfordjournals.org/).
This research was funded by Natural Sciences and Engineering Research Council of Canada Discovery Grants (T. D., A. G., N. M., J. W.), support from the Canada Research Chairs Program (T. D., J. W.), and funding from the Mathematics of Information Technology and Complex Systems (T. D., A. G., A. P., N. M., J. W.).
Conflict of interest: none declared.
References
Parashar UD, Anderson LJ. Severe acute respiratory syndrome: review and lessons of the 2003 outbreak.
Poutanen SM, Low DE. Severe acute respiratory syndrome: an update.
Fraser C, Riley S, Anderson RM, et al. Factors that make an infectious disease outbreak controllable.
Svoboda T, Henry B, Shulman L, et al. Public health measures to control the spread of the severe acute respiratory syndrome during the outbreak in Toronto.
Ou J, Li Q, Zeng G. Efficiency of quarantine during an epidemic of severe acute respiratory syndrome—Beijing, China, 2003.
Speakman J, Gonzalez-Martin F, Perez T. Quarantine in severe acute respiratory syndrome (SARS) and other emerging infectious diseases.
Hawryluck L, Gold WL, Robinson S, et al. SARS control and psychological effects of quarantine, Toronto, Canada.
Gupta AG, Moyer CA, Stern DT. The economic impact of quarantine: SARS in Toronto as a case study.
Lloyd-Smith JO, Galvani AP, Getz WM. Curtailing transmission of severe acute respiratory syndrome within a community and its hospital.
Gumel AB, Ruan S, Day T, et al. Modelling strategies for controlling SARS outbreaks.
Nishiura H, Patanarapelert K, Sriprom M, et al. Modelling potential responses to severe acute respiratory syndrome in Japan: the role of initial attack size, precaution, and quarantine.
Zhou YC, Ma Z, Brauer F. A discrete epidemic model for SARS transmission and control in China.
Zhang J, Lou H, Ma Z, et al. A compartmental model for the analysis of SARS transmission patterns and outbreak control measures in China.
Meyers LA, Pourbohloul B, Newman MEJ, et al. Network theory and SARS: predicting outbreak diversity.
Pourbohloul B, Meyers LA, Skowronski DM, et al. Modeling control strategies of respiratory pathogens.
Lee HKK, Tso EY, Chau TN, et al. Asymptomatic severe acute respiratory syndrome-associated coronavirus infection.
Wallinga J, Teunis P. Different epidemic curves for severe acute respiratory syndrome reveal similar impacts of control measures.
Anderson RM, May RM. Infectious diseases of humans: dynamics and control. Oxford, United Kingdom: Oxford University Press,
Shen Z, Ning F, Zhou WG, et al. Superspreading SARS events, Beijing, 2003.
Li YG, Yu ITS, Xu PC, et al. Predicting super spreading events during the 2003 severe acute respiratory syndrome epidemics in Hong Kong and Singapore.
Diekmann O, Heesterbeek JAP. Mathematical epidemiology of infectious disease. New York, NY: Wiley,
Donnelly CA, Ghani AC, Leung GM, et al. Epidemiological determinants of spread of causal agent of severe acute respiratory syndrome in Hong Kong.
Riley S, Fraser C, Donnelly CA, et al. Transmission dynamics of the etiological agent of SARS in Hong Kong: impact of public health interventions.
Lipsitch M, Cohen T, Cooper B, et al. Transmission dynamics and control of severe acute respiratory syndrome.
Chowell G, Castillo-Chavez C, Fenimore PW, et al. Model parameters and outbreak control for SARS.


{kind=link}
{kind=link}
{kind=link}