
Abstract
Whether circulating tumor cells (CTCs) can be used as an indicator of treatment response in breast cancer (BC) needs to be clarified. We addressed this issue by a meta-analysis. PubMed, EMBase and Cochrane library databases were searched in June 2016. Effect measures were estimated as pooled risk ratio (RR), odds ratio (OR) or mean difference by fixed- or random-effect models, according to heterogeneity of included studies. In total, 50 studies with 6712 patients were recruited. Overall analysis showed that there was a significant reduction of CTC-positive rate (RR = 0.68, 95% CI: 0.61–0.76, P < 0.00001) after treatment. Subgroup analyses revealed that neoadjuvant treatment, adjuvant treatment, metastatic treatment or combination therapy could reduce the CTC-positive rate, but surgery could not; moreover, the reduction was only found in HER2+ or HER2- patients but not in the triple-negative ones. Reduction of CTC-positive rate was associated with lower probability of disease progression (OR = 0.54, 95% CI: 0.33–0.89, P = 0.01) and longer overall survival period (mean difference = 11.61 months, 95% CI: 8.63–14.59, P < 0.00001) as well as longer progression-free survival period (mean difference = 5.07 months, 95% CI: 2.70–7.44, P < 0.0001). These results demonstrate that CTC status can serve as an indicator to monitor the effectiveness of treatments and guide subsequent therapies in BC.
Similar content being viewed by others

Introduction
Metastasis is the major cause of cancer-related death in patients with breast cancer (BC)1. Despite the improvements in treatment, metastatic relapse may occur in about 30% of BC patients with lymph node-negative axilla and about 50% of BC patients with positive axilla within 5 years2. During the process of metastasis, cancer cells shed from primary tumors and migrate to distal sites through the blood or lymphatic system. Those migrating cells found in peripheral blood are known as circulating tumor cells (CTCs). CTCs are the metastatic precursors, which may have potential roles not only in predicting the risk of metastatic relapse and monitoring the treatment efficacy, but also in acting as a therapeutic target for preventing metastasis of cancers, including BC3,4,5,6,7,8,9.
Up to now, CTCs have been well studied and are currently being used in the clinical setting10. However, there are controversial results about the effectiveness of different treatments to reduce CTCs. For example, Martin M. et al. analyzed the change of CTCs in 117 BC patients and observed a substantial decline in CTC-positive rate after chemotherapy11, but Rack B. et al. conducted a larger perspective study with 2026 BC patients and found that the detection rate of CTCs after chemotherapy (22.1%) was even a bit higher than the baseline condition (21.5%)12. In addition, it needs also to be clarified whether molecular subtypes of BC affect CTC status under same treatments13. Hence, we conducted a meta-analysis of the published researches with measurement of CTCs before and after treatment in BC patients, and estimated the CTC-reducing effect of the current anti-tumor therapies. The CTC-reducing effects by different treatments were investigated separately in subgroup analyses, so were the effects in patients with different molecular subtypes. Then we also analyzed the relationship between reduction of CTCs and disease progression probability as well as survival period. This study followed the PRISMA criterions.
Results
Study characteristics
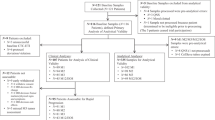
We initially retrieved 1004 articles through database searching. 846 articles were excluded based on the title and abstract. Further, 108 articles were excluded after reviewing full-texts, in which the results of CTC status before and after treatment were not completely contained, or sample size was less than 20, and or duplicated data with other studies was reported. Finally, 50 studies were eligible for meta-analysis (Fig. 1)4,5,9,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57.

Flowchart for article search.
The eligible studies were conducted between 2009 and 2016 in America (USA), Asia (China, Japan and Korea) and Europe (Belgium, Czech, Denmark, France, Germany, Greece, Italy, Norway, Russia, Slovakia, Spain, and Turkey). The sample sizes of studies ranged from 21 to 2026 patients, accumulating 8019 patients before treatments and 6712 patients after treatments in total. Some studies reported the results in patients with particular molecular subtype BC, such as the HER2-positve or the triple-negative ones. The treatments performed in the studies included surgery, neoadjuvant treatment, adjuvant treatment, metastatic treatment, etc., either alone or in combination. The main characteristics of these studies are listed in Table S1. The quality of the studies was also estimated (Table S2).
Overall CTC-positive rate is significantly decreased after therapies
The CTC status was detected with different platforms or methods and presented with different indicators in the 50 studies with 6712 patients. The CTC-positive rate was reported in all of the studies, in which the different cut-off values of CTC count for CTC-capturing methods were used, such as ≥5 CTCs/7.5 mL, ≥1 CTCs/7.5 mL and so on, and the different expression thresholds of epithelial genes (EpCAM, CK18, CK19) were used for RT-PCR method. Some studies also presented the CTC status as CTC count. We first performed an overall analysis of the 50 studies with 6712 patients with CTC-positive rate by the random-effects model, and found that the CTC-positive rate was significantly decreased after treatment compared to the baseline (RR = 0.68, 95% CI: 0.61 to 0.76, P < 0.00001; I2 = 73%, P < 0.00001) (Fig. 2).

The black diamond and its extremities indicate the pooled risk ratio center and 95% confidential interval.
We then analyzed the change of CTC counts in the 7 studies (2324 cases) that simultaneously reported CTC-positive rate and CTC count before and after treatments. No significant change of CTC counts was observed (mean difference = −1.17 CTCs/7.5 mL, 95% CI: −3.17 to 0.84, P = 0.25; I2 = 65%, P = 0.009) (Fig. 3), while a significant reduction was observed with CTC-positive rate in the 7 studies investigated after treatment (RR = 0.65, 95% CI: 0.48 to 0.87, P = 0.004; I2 = 85%, P < 0.00001) (Figure S1). This inconsistent results between CTC-positive rate and CTC count might attribute to the heterogeneity among the studies, because the CTC count, a continuous variable, could be more susceptible to the variance caused by individual study than the CTC-positive rate, a dichotomized variable. So we made a sensitivity analysis by removing each study, and found that one of them (Bidard FC 2012) substantially affected the result. Once it was excluded, the significant decrease of CTC level after treatment was observed compared to pre-treatment (mean difference = −0.94, 95% CI: −1.49 to −0.38, P = 0.0010 by fixed-effects model). These results confirmed the promising application of CTCs in monitoring the effectiveness of treatments for BC.

The black diamond indicates the difference of CTC counts (cells/7.5 mL peripheral blood; the post-therapeutic counts minus the pre-therapeutic counts). Its center indicates the mean and the extremities indicate the 95% confidential interval.
In addition, different methods as well as different cut-off values for a method were used in the studies. Hence, we also investigated the CTC-positive rate before and after treatment in the subgroups of different CTC-measuring methods. A significant reduction of CTC-positive rate after treatment was observed no matter how the CTC positivity was defined as ≥5CTCs/7.5 mL, ≥1CTCs/7.5 mL, or other threshold including a threshold for RT-PCR technique (Fig. 4).

The results of ≥5 CTCs/7.5 mL as positive (A) ≥1 CTCs/7.5 mL as positive (B) other threshold as positive (C) and RT-PCR method (D) are shown, respectively. The center of black diamond and its extremities indicate the pooled risk ratio and 95% confidential interval.
CTC-positive rates are decreased after neoadjuvant treatment, adjuvant treatment, metastatic treatment and combination therapy, but not after surgery
Clinically, many therapeutic methods are employed in treatment of BC. The therapeutic methods involved in the pooled 50 studies could be roughly classified into neoadjuvant setting, adjuvant setting, metastatic setting, surgery and combination therapy. To clarify the efficacy of various therapies on decreasing CTC-positive rate, we performed a subgroup analysis. Compared to pre-treatment, CTC-positive rate were decreased after treatment in the neoadjuvant setting (RR = 0.65, 95% CI: 0.48 to 0.88, P = 0.006; I2 = 40%, P = 0.08), and adjuvant setting (RR = 0.89, 95% CI: 0.76 to 1.02, P = 0.10; I2 = 62%, P = 0.007), the metastatic setting (RR = 0.59, 95% CI: 0.50 to 0.70, P < 0.00001; I2 = 66%, P < 0.0001) and the combination therapy (RR = 0.78, 95% CI: 0.62 to 0.97, P = 0.03; I2 = 29%, P = 0.20), but not in the surgery (RR = 1.27, 95% CI: 0.71 to 2.27, P = 0.42; I2 = 45%, P = 0.16) (Fig. 5). These results indicate that surgery as a local treatment can not eliminate CTCs timely, because CTCs can survive in peripheral blood for a certain amount of time58, suggesting that patients with CTC positive should be further treated with other therapies after surgery, in order to decrease the risk of metastasis and recurrence.

The results of neoadjuvant setting (A), adjuvant setting (B), metastatic setting (C), surgery (D) and combination therapy (E) are shown, respectively. The center of black diamond and its extremities indicate the pooled risk ratio and 95% confidential interval.
CTC-positive rates are decreased after therapies in the HER2 -positive or -negative patients, but not in the triple-negative patients
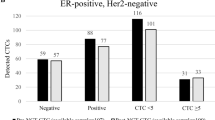
Currently, the clinical management of breast cancer mainly relies on the molecular subtypes based on the expression of estrogen receptor, progesterone receptor and HER2 in primary tumors. It is well known that different molecular subtypes of BC are associated with distinct malignant nature and drug response. Therefore, we further assessed the effects of therapies on reduction of CTCs in different subgroups, including HER2-positive, HER2-negative and triple-negative BC. Compared to pre-therapy, CTC-positive rates were significantly decreased after treatment in HER2-positive patients (RR = 0.68, 95% CI: 0.57 to 0.82, P < 0.0001; I2 = 0%, P = 0.59) and HER2-negative patients (RR = 0.52, 95% CI: 0.31 to 0.86, P = 0.01; I2 = 66%, P = 0.01), but not in the triple-negative ones (RR = 0.38, 95% CI: 0.06 to 2.33, P = 0.29; I2 = 72%, P = 0.06) (Fig. 6). These results indicate that different molecular subtypes of BC affect the efficacy of therapeutics on reducing CTCs. The poor reduction of CTC-positive rate in triple-negative BC is consistent with clinical outcome, implying that current therapies should be further optimized and the new therapeutic methods should be developed for this specific molecular subtype.

The results of HER2-positive subtype (A) HER2-negative subtype (B) and triple-negative subtype (C) are shown, respectively. The black diamond and its extremities indicate the pooled risk ratio center and 95% confidential interval.
Correlation between status of CTCs after treatment and prognosis of the patients
Because CTCs are shed from the primary tumor and serve as the metastatic precursors, the changes of CTC status after therapies may associate with the risk of metastasis as well as the outcome of patients. We compared the prognosis of the CTC-reduced patients with that of the CTC-unchanged or -elevated patients after treatment. The overall survival (OS) of patients after treatment was available in 2 studies (71 cases), in both of which the patients received metastatic setting. The CTC-reduced patients had a longer overall survival period compared to the CTC-unchanged or -elevated patients (mean difference = 11.61 months, 95% CI: 8.63 to 14.59, P < 0.00001; I2 = 69%, P = 0.07) (Fig. 7). The progression-free survival (PFS) of patients after treatment were available in 3 studies (125 patients), in which all the patients received metastatic setting. The CTC-reduced patients had a longer PFS than the CTC-unchanged or -elevated patients (mean difference = 5.07 months, 95% CI: 2.70 to 7.44, P < 0.0001; I2 = 96%, P < 0.00001) (Fig. 7). The disease progression of patients after treatments was available in 11 studies with 1363 patients. A significantly lower probability of disease progression was observed in the CTC-reduced patients (OR = 0.54, 95% CI: 0.33 to 0.89, P = 0.01; I2 = 45%, P = 0.05) (Fig. 7). The 11 studies could be divided into 3 subgroups, namely metastatic setting (6 studies with 244 patients), adjuvant setting (3 studies with 1095 patients), neoadjuvant setting (2 studies with 24 patients). Significantly lower probability of disease progression in CTC-reduced patients was observed in the metastatic setting subgroup (OR = 0.37, 95% CI: 0.20 to 0.66, P = 0.0008; I2 = 13%, P = 0.33) (Fig. 8). But there was no significant difference of probability of disease progression in patients with or without CTC reduction in the adjuvant setting subgroup (OR = 0.73, 95% CI: 0.44 to 1.22, P = 0.23; I2 = 54%, P = 0.11) and in the neoadjuvant setting subgroup (OR = 0.30, 95% CI: <0.01 to 77.67, P = 0.67; I2 = 80%, P = 0.03) (Fig. 8). There was a significant heterogeneity in the adjuvant-setting subgroup. When a study (Rack B 2014) was excluded, the heterogeneity was relieved (P = 0.68, I2 = 0%) and the correlation of CTC status and disease progression became significant (OR = 0.57, 95%CI: 0.37 to 0.86, P = 0.008 by fixed-effect model). In the neoadjuvant setting subgroup, the sample size was extremely small, implying that did not have adequate statistic power. The results showed that the reduction of CTCs was significantly associated with decreased probability of disease progression, increased overall survival and progression-free survival period.

The diamond indicated the odds ratio of disease progression (A) the difference of progression-free survival (B) or overall survival period (C). The centers of the diamonds indicated the pooled odds ratio (A) or the mean difference (B,C) and the extremities indicated the 95% confidential interval.

The diamond indicated the odds ratio of disease progression in the metastatic setting (A), the adjuvant setting (B) or the neoadjuvant setting (C). The centers of the diamonds indicated the pooled odds ratio and the extremities indicated the 95% confidential interval.
Sensitivity Analysis and Publication Bias
Among the 50 studies included for the pooled RR estimation, no single one contributed substantial influence. When we analyzed the change of CTC counts post-treatments with 7 studies reported CTC status both in CTC-positive rate and CTC counts, the sensitivity analysis was tested by removal of each study. One of them (Bidard FC 2012) was found to substantially affect the heterogeneity and the significance of overall effect: when it was excluded, the heterogeneity was relieved (P = 0.69, I2 = 0%) and the change of CTC counts after treatment became significant (mean difference = −0.94, 95%CI: −1.49 to −0.38, P = 0.0010 by fixed-effect model). In the adjuvant-setting subgroup analysis of disease progression (Fig. 8), one of the three recruited studies (Rack B 2014) was found to substantially affect the heterogeneity and the significance of overall effect: when it was excluded, the heterogeneity was relieved (P = 0.68, I2 = 0%) and the correlation of CTC status and disease progression became significant (OR = 0.57, 95%CI: 0.37 to 0.86, P = 0.008 by fixed-effect model). No substantial publication bias was found according to the Funnel plot (Fig. 9).

Funnel plot for the studies included for comparison of CTC-positive rate before and after treatment.
Discussion
It has been well known that even localized tumors without clinically apparent metastasis give rise to CTCs. Because generation of CTCs is an indispensable step of the metastatic process of tumors, the promising application as a noninvasive blood biomarker in prognosis and response to therapy are very attractive. Although the actual utility of CTCs remains largely academic59, many studies have reported the detection of CTCs to facilitate early diagnosis of relapse or metastasis and improve the treatment decisions. In present meta-analysis, we analyzed the changes of CTC status after therapies compared to that of before therapies in pooled 50 studies with 6712 BC patients, and demonstrated that CTC status was a useful indicator to monitor the treatment response, and predict the outcome of patients.
The actual application of CTCs in clinical setting relies on the progression of detection technologies. In the past decades, a number of technically diverse platforms have been developed for CTC assay60. However, for any technology to be used in the clinic, demonstration of analytic validity, clinical validity, and clinical utility is required60. Up to now, the only system approved by the Food and Drug Administration (FDA) as an aid in monitoring patients with metastatic breast, colorectal, or prostate cancer is CellSearch® (Veridex, Raritan, NJ, USA). Also, CellSearch® is the only semi-automated system and has contributed considerably to the development of standards for CTC enumeration. Nevertheless, there are disadvantages to be perfect for it. Its enrichment/capture technology is based on epithelial marker EpCAM, which is usually with low sensitivity and efficiency, due to the lost expression of EpCAM in CTCs by EMT process61,62. In our meta-analysis, other CTC detection methods are employed in some studies, including RT-PCR, which determined the CTC status by detecting the mRNA expression of epithelial markers, such as EpCAM or CKs. There is a probability that the CTC detection methods based on different labels or rationales would find different counts of CTCs in the same individual patients. Given the CTC rarity, especially in non-metastatic breast cancer, continuous training and central image review is required in order to gain best inter-reader agreement. A recent study evaluated the inter-reader agreement in 22 readers from 15 academic laboratories and 8 readers from two Veridex laboratories with non-metastatic (M0) and metastatic (M1) breast cancer samples. For CTC definition (No CTC vs. CTC), the median agreement between academic readers and VC was 92% (range 69 to 97%) with a median κ of 0.83 (range: 0.37 to 0.93). The inter-reader agreement for CTC definition was high. Reduced agreement was observed in M0 patients with low CTC counts63. In addition, the inconsistence of the cut-off value to determine CTC-positive amongst studies would be a limitation for actual application of CTCs in clinical setting (Fig. 4). Standard or uniform protocol for CTC measurement would be required before this indicator could be clinically adopted.
There were several limitations in the present research. First, most of studies included in this meta-analysis were consisted of patients receiving certain therapy alone without an appropriate negative control. Second, some studies with substantial sample heterogeneities, which were caused by the complexity of patient characteristics (race, age), therapeutic details (drug, dose, treatment periodicity, etc.) or other factors, were excluded in our subgroup analyses. Third, the sample sizes of some subgroups were relatively small, which might affect the detection of potential difference. Fourth, CTCs were thought to be a set of cells with different characteristics, so it would be more meaningful to investigate the correlation of change of the CTC subpopulations after treatment with patient prognosis. However, so far few data are available to perform an analysis.
In summary, the present meta-analysis demonstrated that the status of CTCs is a useful indicator of the efficacy of therapies for BC, which may help clinicians make a decision for further personalized therapy of patients. However, it is on the way for application of CTCs in clinical setting because there are still challenges presented in analytic validity, clinical validity, and clinical utility of CTCs.
Methods
Search strategy
A comprehensive literary search for potential studies was searched in June 2016 without time or language restrictions. The electronic databases include PubMed, EMBase and Cochrane library. The keywords and MeSH terms were variably combined: “circulating tumor cell (s)”, “breast cancer”, “therapy”. The search strategy was intended to exclude reviews, comments, letters and editorials, which have irrelevant study data, by screening the titles and abstracts of publications.
Eligibility criteria
Inclusion criteria: (i) enrolled patients with BC were pathologically diagnosed; (ii) CTCs were detected by any method, including cell capture and quantitative PCR; (iii) the patients’ CTC status both pre- and post-therapy was reported.
Exclusion criteria: (i) cell-line experiments or animal models; (ii) a small size <20 patients; (iii) when information of the same patients was reported in different studies, only the latest and most informative one was included; (iv) CTC status was reported pre- or post-therapy alone; (v) CTC status pre- and post-therapy was reported in different cohort of patients; (vi) Studies which reported CTCs only in continuous style were excluded, as their results could not be integrated with the majority of studies which reported the results in dichotomous pattern (positive vs. negative).
Data extraction
Studies were reviewed and extracted independently by two reviewers (WT Yan and Q Chen). The primary data of the included studies were following: the general information (i.e., the first author, the year of publication, the nationality of studies), sample size, the patients’ characteristics (i.e., ages, tumor stage, molecular subtypes of tumor), assessment of CTCs (i.e., methods of CTC detection, blood volume, the cut-off value of CTCs, the count of CTCs and/or the positive rate of CTCs) and the type of the treatments. If CTCs at more than one phase of follow ups were reported in a study, the latest phase with follow-up rate ≥75% was chosen; if no phase met the criteria, the earliest phase was chosen. The prognosis (progression-free survival, overall survival) was also extracted for assessing prognostic value of reducing CTCs.
Quality assessment of primary studies
The quality of each included study was evaluated by a scale based on the Newcastle–Ottawa Quality Assessment Scale.
Statistical analysis
The pooled RR (relative risk) and mean difference were calculated to analyze the difference of CTCs between pre-therapy and post-therapy by fixed model or random-effects model according to the heterogeneity of the studies, which was estimated by the Cochran’s Q test and the I2 index (P value < 0.10 or I2 over 50% was define as substantial heterogeneity). RR less than 1 or mean difference less than 0 indicated declined CTCs in the peripheral blood. Pooled OR (odds ratio) and mean difference were calculated to analyze the difference of progression between the patients with different dynamic conditions of CTCs (decreasing vs. increasing or persistent elevated). Subgroup analyses were performed for CTC determination methods, treatments and molecular subtypes of primary tumor as long as two or more studies were available to be included. Forest plot was used to illustrate the pooled RR mean difference. All analyses were run by Review Manager Version 5.3 (Cochrane Collaboration, Copenhagen, Denmark).
Sensitivity analysis and estimation of publication bias
To evaluate the influence of individual study on the pooled RR or mean difference, sensitivity analysis was performed by removing each eligible study separately. Funnel plot developed by Begg was used to detect potential publication bias which might affect the validity of the results.
Additional Information
How to cite this article: Yan, W.-T. et al. Circulating tumor cell status monitors the treatment responses in breast cancer patients: a meta-analysis. Sci. Rep. 7, 43464; doi: 10.1038/srep43464 (2017).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Ursaru, M., Jari, I., Naum, A., Scripcariu, V. & Negru, D. Causes of Death in Patients with Stage 0-Ii Breast Cancer. Revista medico-chirurgicala a Societatii de Medici si Naturalisti din Iasi 119, 374–378 (2015).
Maltoni, R., Gallerani, G., Fici, P., Rocca, A. & Fabbri, F. CTCs in early breast cancer: A path worth taking. Cancer Lett 376, 205–210, doi: 10.1016/j.canlet.2016.03.051 (2016).
Beije, N., Jager, A. & Sleijfer, S. Circulating tumor cell enumeration by the CellSearch system: the clinician’s guide to breast cancer treatment? Cancer Treat Rev 41, 144–150, doi: 10.1016/j.ctrv.2014.12.008 (2015).
Wallwiener, M. et al. Serial enumeration of circulating tumor cells predicts treatment response and prognosis in metastatic breast cancer: a prospective study in 393 patients. BMC Cancer 14, 512, doi: 10.1186/1471-2407-14-512 (2014).
Pierga, J. Y. et al. Circulating tumor cell detection predicts early metastatic relapse after neoadjuvant chemotherapy in large operable and locally advanced breast cancer in a phase II randomized trial. Clin Cancer Res 14, 7004–7010, doi: 10.1158/1078-0432.CCR-08-0030 (2008).
Janni, W. et al. Pooled Analysis of the Prognostic Relevance of Circulating Tumor Cells in Primary Breast Cancer. Clin Cancer Res, doi: 10.1158/1078-0432.ccr-15-1603 (2016).
Pierga, J. Y. et al. Impact of targeted therapy on circulating tumor cells in metastatic breast cancer treated by first-line chemotherapy: IC 2006-04 study. Cancer Research 71 (2011).
Smerage, J. B. et al. Circulating tumor cells and response to chemotherapy in metastatic breast cancer: SWOG S0500. J Clin Oncol 32, 3483–3489, doi: 10.1200/JCO.2014.56.2561 (2014).
Aurilio, G. et al. Circulating Tumor Cells (Ctcs) and Metronomic Oral Vinorelbine (Ov) in Advanced Breast Cancer (Abc) Patients (Pts): Exploratory Prospective Analysis. Annals of Oncology 23, 26–26, doi: 10.1093/annonc/mds040 (2012).
Masuda, T. et al. Clinical and biological significance of circulating tumor cells in cancer. Mol Oncol 10, 408–417, doi: 10.1016/j.molonc.2016.01.010 (2016).
Martin, M. et al. Circulating tumor cells following first chemotherapy cycle: An early and strong predictor of outcome in patients with metastatic breast cancer. Oncologist 18, 917–923 (2013).
Rack, B. et al. Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J Natl Cancer Inst 106, doi: 10.1093/jnci/dju066 (2014).
Van Dalum, G. et al. Circulating tumor cells before and during follow-up after breast cancer surgery. International Journal of Oncology 46, 407–413 (2015).
Cabinakova, M. et al. Predictive factors for the presence of tumor cells in bone marrow and peripheral blood in breast cancer patients. Neoplasma 62, 259–268, doi: 10.4149/neo_2015_031 (2015).
Magbanua, M. J. et al. Circulating tumor cell analysis in metastatic triple-negative breast cancers. Clin Cancer Res 21, 1098–1105, doi: 10.1158/1078-0432.CCR-14-1948 (2015).
Maltoni, R. et al. Circulating tumor cells in early breast cancer: A connection with vascular invasion. Cancer Lett 367, 43–48, doi: 10.1016/j.canlet.2015.06.020 (2015).
Kasimir-Bauer, S. et al. Does primary neoadjuvant systemic therapy eradicate minimal residual disease? Analysis of disseminated and circulating tumor cells before and after therapy. Breast Cancer Res 18, 20, doi: 10.1186/s13058-016-0679-3 (2016).
Pierga, J. Y. et al. Pathological response and circulating tumor cell count identifies treated HER2+ inflammatory breast cancer patients with excellent prognosis: BEVERLY-2 survival data. Clin Cancer Res 21, 1298–1304, doi: 10.1158/1078-0432.CCR-14-1705 (2015).
Wang, H. Y. et al. Detection of circulating tumor cell-specific markers in breast cancer patients using the quantitative RT-PCR assay. International Journal of Clinical Oncology (2015).
Zhang, J. L. et al. Effects of Herceptin on circulating tumor cells in HER2 positive early breast cancer. Genet Mol Res 14, 2099–2103, doi: 10.4238/2015.March.20.20 (2015).
Barnadas, A. et al. Bone turnover markers as predictive indicators of outcome in patients with breast cancer and bone metastases treated with bisphosphonates: Results from a 2-year multicentre observational study (ZOMAR study). Bone 68, 32–40 (2014).
Bian, L. et al. Prediction value for dynamic changes of circulating tumor cell in therapeutic response and prognosis of Chinese metastatic breast cancer patients. Zhonghua Yi Xue Za Zhi 94, 265–268 (2014).
Horn, P., Jakobsen, E. H., Madsen, J. S. & Brandslund, I. New approach for interpreting changes in circulating tumour cells (CTC) for evaluation of treatment effect in metastatic breast cancer. Translational Oncology 7, 694–701 (2014).
Lavrov, A. V. et al. Analysis of Circulating Tumor Cells in Patients with Triple Negative Breast Cancer during Preoperative Chemotherapy. Bulletin of Experimental Biology and Medicine (2014).
Mikulova, V. et al. Detection of circulating tumor cells during follow-up of patients with early breast cancer: Clinical utility for monitoring of therapy efficacy. Scand J Clin Lab Invest 74, 132–142, doi: 10.3109/00365513.2013.864784 (2014).
Peeters, D. J. et al. Detection and prognostic significance of circulating tumour cells in patients with metastatic breast cancer according to immunohistochemical subtypes. Br J Cancer 110, 375–383, doi: 10.1038/bjc.2013.743 (2014).
Usiakova, Z. et al. Circulating tumor cells in patients with breast cancer: monitoring chemotherapy success. In Vivo 28, 605–614 (2014).
Azim, H. A. Jr. et al. Circulating tumor cells and response to neoadjuvant paclitaxel and HER2-targeted therapy: a sub-study from the NeoALTTO phase III trial. Breast 22, 1060–1065, doi: 10.1016/j.breast.2013.08.014 (2013).
Bidard, F. C. et al. Time-dependent prognostic impact of circulating tumor cells detection in non-metastatic breast cancer: 70-month analysis of the REMAGUS02 study. International Journal of Breast Cancer 2013 (2013).
Boutrus, R. R. et al. Circulating tumor cells as predictors of response and failure in breast cancer patients treated with preoperative chemotherapy. International Journal of Biological Markers 28, 17–23 (2013).
Jiang, Z. F. et al. Circulating tumor cells predict progression-free and overall survival in Chinese patients with metastatic breast cancer, HER2-positive or triple-negative (CBCSG004): a multicenter, double-blind, prospective trial. Ann Oncol, doi: 10.1093/annonc/mdt246 (2013).
Karaba, M. et al. Circulating tumor cells (CTCs) and epithelial mesenchymal transition (EMT) in primary breast cancer. Journal of Clinical Oncology 31 (2013).
Mathiesen, R. R. et al. Detection and monitoring of circulating endothelial cells, circulating tumor cells and disseminated tumor cells during neoadjuvant breast cancer treatment including bevacizumab. Cancer Research 73 (2013).
Nakayama, Y., Takahashi, S. & Ito, Y. A phase II clinical trial of neoadjuvant therapy with zoledronic acid for operable breast cancer. Journal of Clinical Oncology 31 (2013).
Neugebauer, J. K. et al. Persistence of HER2 overexpression on circulating tumor cells in patients after systemic treatment for HER2-positive breast cancer: Follow-up results of the German Success B trial. Journal of Clinical Oncology 31 (2013).
Pierga, J. Y. et al. Circulating tumor cells and brain metastasis outcome in patients with HER2-positive breast cancer: The LANDSCAPE trial. Annals of Oncology 24, 2999–3004 (2013).
Roop, R. P. et al. A randomized phase II trial investigating the effect of platelet function inhibition on circulating tumor cells in patients with metastatic breast cancer. Clin Breast Cancer 13, 409–415, doi: 10.1016/j.clbc.2013.08.006 (2013).
Smerage, J. B. et al. Monitoring apoptosis and Bcl-2 on circulating tumor cells in patients with metastatic breast cancer. Molecular Oncology 7, 680–692 (2013).
Tryfonidis, K. et al. A multicenter phase I-II study of docetaxel plus epirubicin plus bevacizumab as first-line treatment in women with HER2-negative metastatic breast cancer. Breast 22, 1171–1177, doi: 10.1016/j.breast.2013.08.017 (2013).
Turker, I. et al. Detection of circulating tumor cells in breast cancer patients: Prognostic predictive role. Asian Pacific Journal of Cancer Prevention 14, 1601–1607 (2013).
Xenidis, N. et al. Differential effect of adjuvant taxane-based and taxane-free chemotherapy regimens on the CK-19 mRNA-positive circulating tumour cells in patients with early breast cancer. Br J Cancer 108, 549–556, doi: 10.1038/bjc.2012.597 (2013).
Bidard, F. C. et al. Assessment of circulating tumor cells and serum markers for progression-free survival prediction in metastatic breast cancer: a prospective observational study. Breast Cancer Res 14, R29, doi: 10.1186/bcr3114 (2012).
Hayashi, N. et al. Prognostic value of HER2-positive circulating tumor cells in patients with metastatic breast cancer. Int J Clin Oncol 17, 96–104, doi: 10.1007/s10147-011-0260-0 (2012).
Mego, M. et al. Prognostic value of EMT-circulating tumor cells in metastatic breast can-cer patients undergoing high-dose chemotherapy with autologous hematopoietic stem cell transplantation. Journal of Cancer 3, 369–380 (2012).
Nadal, R. et al. Biomarkers characterization of circulating tumour cells in breast cancer patients. Breast Cancer Res 14, R71, doi: 10.1186/bcr3180 (2012).
Serrano, M. J. et al. Dynamics of circulating tumor cells in early breast cancer under neoadjuvant therapy. Exp Ther Med 4, 43–48, doi: 10.3892/etm.2012.540 (2012).
Daskalakis, M. et al. Assessment of the effect of surgery on the kinetics of circulating tumour cells in patients with operable breast cancer based on cytokeratin-19 mRNA detection. Eur J Surg Oncol 37, 404–410, doi: 10.1016/j.ejso.2011.02.003 (2011).
Hartkopf, A. D., Wagner, P., Wallwiener, D., Fehm, T. & Rothmund, R. Changing levels of circulating tumor cells in monitoring chemotherapy response in patients with metastatic breast cancer. Anticancer Res 31, 979–984 (2011).
Reinholz, M. M. et al. Cytokeratin-19 and mammaglobin gene expression in circulating tumor cells from metastatic breast cancer patients enrolled in North Central Cancer Treatment Group trials, N0234/336/436/437. Clin Cancer Res 17, 7183–7193, doi: 10.1158/1078-0432.CCR-11-0981 (2011).
Tokudome, N. et al. Detection of circulating tumor cells in peripheral blood of heavily treated metastatic breast cancer patients. Breast Cancer 18, 195–202, doi: 10.1007/s12282-011-0259-4 (2011).
Bidard, F. C. et al. Clinical value of circulating endothelial cells and circulating tumor cells in metastatic breast cancer patients treated first line with bevacizumab and chemotherapy. Ann Oncol 21, 1765–1771, doi: 10.1093/annonc/mdq052 (2010).
Cristofanilli, M. et al. Circulating tumor cells and FDG-PET/CT: Biological and functional methods for therapeutic monitoring in metastatic breast cancer. Cancer Research 69 (2009).
Serrano, M. J., Sanchez-Rovira, P., Delgado-Rodriguez, M. & Gaforio, J. J. Detection of circulating tumor cells in the context of treatment: prognostic value in breast cancer. Cancer Biol Ther 8, 671–675 (2009).
Xenidis, N. et al. Cytokeratin-19 mRNA-positive circulating tumor cells after adjuvant chemotherapy in patients with early breast cancer. J Clin Oncol 27, 2177–2184, doi: 10.1200/JCO.2008.18.0497 (2009).
Nole, F. et al. Variation of circulating tumor cell levels during treatment of metastatic breast cancer: prognostic and therapeutic implications. Ann Oncol 19, 891–897, doi: 10.1093/annonc/mdm558 (2008).
Muller, V. et al. Circulating tumor cells in breast cancer: correlation to bone marrow micrometastases, heterogeneous response to systemic therapy and low proliferative activity. Clin Cancer Res 11, 3678–3685, doi: 10.1158/1078-0432.ccr-04-2469 (2005).
Cristofanilli, M. et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. The New England journal of medicine 351, 781–791, doi: 10.1056/NEJMoa040766 (2004).
Broersen, L. H., van Pelt, G. W., Tollenaar, R. A. & Mesker, W. E. Clinical application of circulating tumor cells in breast cancer. Cell Oncol (Dordr) 37, 9–15, doi: 10.1007/s13402-013-0160-6 (2014).
Adams, D. L. et al. Mitosis in circulating tumor cells stratifies highly aggressive breast carcinomas. Breast Cancer Res 18, 44, doi: 10.1186/s13058-016-0706-4 (2016).
Ignatiadis, M., Lee, M. & Jeffrey, S. S. Circulating Tumor Cells and Circulating Tumor DNA: Challenges and Opportunities on the Path to Clinical Utility. Clinical Cancer Research 21, 4786–4800, doi: 10.1158/1078-0432.CCR-14-1190 (2015).
Liu, Z. et al. Negative enrichment by immunomagnetic nanobeads for unbiased characterization of circulating tumor cells from peripheral blood of cancer patients. Journal of translational medicine 9, 70, doi: 10.1186/1479-5876-9-70 (2011).
Cen, P. T., Ni, X. L., Yang, J. X., Graham, D. Y. & Li, M. Circulating tumor cells in the diagnosis and management of pancreatic cancer. Bba-Rev Cancer 1826, 350–356, doi: 10.1016/j.bbcan.2012.05.007 (2012).
Ignatiadis, M. et al. International study on inter-reader variability for circulating tumor cells in breast cancer. Breast Cancer Res 16, R43, doi: 10.1186/bcr3647 (2014).
Acknowledgements
This work was supported by Major Project of Chongqing (Grant No. cstc2015shms-ztzx10005), P. R. China.
Author information
Authors and Affiliations
Contributions
J.J. and C.Y.H. conceived the study, participated in drafting the final manuscript. Y.W.T., C.Q. and C.X. analyzed the data and completed the final draft of the manuscript. L.Y.F. and W.Y. prepared all the figures. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Yan, WT., Cui, X., Chen, Q. et al. Circulating tumor cell status monitors the treatment responses in breast cancer patients: a meta-analysis. Sci Rep 7, 43464 (2017). https://doi.org/10.1038/srep43464
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep43464
This article is cited by
-
Clinical applications of circulating tumor cells in patients with solid tumors
Clinical & Experimental Metastasis (2024)
-
CdSe@CdS quantum dot–sensitized Au/α-Fe2O3 structure for photoelectrochemical detection of circulating tumor cells
Microchimica Acta (2023)
-
In vivo detection demonstrates circulating tumor cell reduction instead of baseline number has prognostic value in bladder cancer patients receiving neoadjuvant chemotherapy
Cellular Oncology (2023)
-
Collective metastasis: coordinating the multicellular voyage
Clinical & Experimental Metastasis (2021)
-
Tumor microenvironment complexity and therapeutic implications at a glance
Cell Communication and Signaling (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
