
Abstract
Following severe adverse reactions to the AstraZeneca ChAdOx1-S-nCoV-19 vaccine1,2, European health authorities recommended that patients under the age of 55 years who received one dose of ChAdOx1-S-nCoV-19 receive a second dose of the Pfizer BNT162b2 vaccine as a booster. However, the effectiveness and the immunogenicity of this vaccination regimen have not been formally tested. Here we show that the heterologous ChAdOx1-S-nCoV-19 and BNT162b2 combination confers better protection against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection than the homologous BNT162b2 and BNT162b2 combination in a real-world observational study of healthcare workers (n = 13,121). To understand the underlying mechanism, we conducted a longitudinal survey of the anti-spike immunity conferred by each vaccine combination. Both combinations induced strong anti-spike antibody responses, but sera from heterologous vaccinated individuals displayed a stronger neutralizing activity regardless of the SARS-CoV-2 variant. This enhanced neutralizing potential correlated with increased frequencies of switched and activated memory B cells that recognize the SARS-CoV-2 receptor binding domain. The ChAdOx1-S-nCoV-19 vaccine induced a weaker IgG response but a stronger T cell response than the BNT162b2 vaccine after the priming dose, which could explain the complementarity of both vaccines when used in combination. The heterologous vaccination regimen could therefore be particularly suitable for immunocompromised individuals.
Similar content being viewed by others


Main
The ChAdOx1-S-nCoV-19 and BNT162b2 vaccines (hereafter referred to as ChAd and BNT, respectively) have been shown to confer strong protection against SARS-CoV-2 infection and to induce robust immune responses directed against the spike protein of SARS-CoV-2 when administered in a homologous setting3,4,5. However, the effectiveness of a ChAd–BNT combination as a prime–boost regimen has not been formally tested in vaccine trials. To compare the risk of SARS-CoV-2 infection following heterologous ChAd–BNT or homologous BNT–BNT vaccination schedules, we extracted data from the occupational medicine database of the University Hospital of Lyon (Hospices Civils de Lyon), France. Specifically, we analysed the number of individuals who received each vaccination regimen (which started in January 2021 in both groups) and the number of SARS-CoV-2 infections (documented by a positive PCR with reverse transcription (RT–PCR) result) that occurred at least 2 weeks after the booster dose in each group (Table 1). Ten infections were identified out of 2,512 individuals (0.40%) in the heterologous vaccination group compared with 81 infections out of 10,609 individuals (0.76%) in the homologous vaccination group (Fig. 1). As the age of the individual and the vaccination regimen are known covariates, we used a multiple logistic regression model to model the probability of being infected. Our predictors were age (set as a continuous variable, considered as a possible confounder) and the vaccination regimen. Results showed that age is not associated with infection status (P = 0.4514). In particular, patients aged 60 years or above (715 out of 13,121) were not more infected (3 out of 715; 0.42%) than patients aged 60 years or below (88 out of 12,406 (0.71%); two-sided Fisher’s exact test, P = 0.4890). However, the vaccination regimen was significantly associated with the probability of being infected after vaccination (P = 0.0384). Individuals vaccinated with BNT–BNT were twice as likely to be infected than those vaccinated with ChAd–BNT (relative risk of 2.03).

Histograms show the infection rate (as documented by a positive SARS-CoV-2 RT–PCR result) among groups of HCWs who were vaccinated with the homologous BNT–BNT combination (n = 81 out of 10,609) within the recommended 4-week timeframe between the two doses or with the BNT boost after receiving the first ChAd dose (n = 10 out of 2,512) approximately 12 weeks before, as recorded by the service of occupational medicine, Hospices Civils de Lyon. Data show the infection rates that occurred 14 days after receiving booster up to the end of recording (15 August 2021). Statistical significance was calculated using a logistic regression model adjusted for age. Demographic data and other statistics are available in Table 1.
Antibodies and virus neutralization
To understand the immunological basis of this difference, we assembled a cohort of healthcare workers (HCWs) without comorbidity (Covid-Ser-Vac). Half of this HCW cohort received the homologous BNT–BNT combination within the recommended 4-week interval between the two doses, whereas the second half received the BNT booster after receiving the first ChAd dose approximately 12 weeks before. For both groups, the mean age was 41 years and 34 years, respectively, and about 70% of participants were female (Table 2). Three blood samples were drawn: before vaccination, before the second dose and 4 weeks after the second dose. Immunological analyses were performed longitudinally (Extended Data Fig. 1), and a linear regression model was used to compare immune parameters between groups to adjust for age differences.
As previously shown6,7, the BNT vaccine induced a stronger level of SARS-CoV-2 receptor binding domain (RBD) or spike S1-specific IgG than the ChAd vaccine after the first dose. However, these IgG titres were no longer statistically different between groups after the second dose (Fig. 2a, b). Moreover, the positivity rate was 100% for both heterologous and homologous vaccinations. Serum IgA levels measured after the booster vaccination tended to be greater in the homologous than in the heterologous setting (median (interquartile range (IQR)) of 46.7 ng m–1 equivalent (Eq) (36.30–78.70 ng m–1 ng Eq) versus 37.4 ng ml–1 Eq (25.40–59.80 ng ml–1 Eq), respectively; equivalence was to the standard used (Methods)) (Fig. 2c).

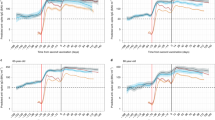
a–c, Sera from ChAd–BNT (n = 29) or BNT–BNT (n = 31) individuals were assayed for S1-specific IgG (a), RBD-specific IgG (b) or S1-specific IgA (c) levels using commercial or custom-made ELISA tests at different times during the vaccination process as indicated (a, b) or 4 weeks after full vaccination (c). In a–c, concentrations are expressed in binding antibody units per ml (BAU ml–1) or ng ml–1 Eq of immunoglobulin as indicated. Each serum sample was evaluated as a single measurement (a, b) or in triplicate (c). Dotted lines in a and b indicate positive detection according to the manufacturer. d–f, Sera from ChAd–BNT (n = 29) or BNT–BNT (n = 31) vaccinated individuals were assayed in triplicate for their capacity to neutralize the entry of virus-like particles pseudotyped with the Wuhan strain SARS-CoV-2 envelope (d) or in duplicate for their capacity to neutralize infection of Vero E6 cells by different SARS-CoV-2 strains (e, f), as indicated. Data show the per cent of neutralization relative to a positive control (d) or the 50% plaque reduction neutralization test (PRNT50) (e), and are expressed as dot plots, with one dot corresponding to one individual. The limit of detection is shown as a dotted line in e. FC, fold change in the mean of the indicated groups. In all panels, box-and-whiskers plots are shown (see Methods for details), and the median is represented by the magenta middle line. A linear regression model was used to compare values between groups, and this model was corrected for age. Exact P values are shown for the indicated comparisons when significant or nearly significant. f, Comparison of serum neutralizing activity against the reference lineage 19A and against the variants of concern for each group. P values are shown and calculated using the linear regression model described in e.
We then measured the ability of serum samples to neutralize SARS-CoV-2 spike-pseudotyped viral particles8. None of the sera displayed a detectable neutralizing activity before vaccination or after the first dose. However, most of the sera displayed a neutralizing activity after the second dose, and those from the ChAd–BNT vaccinated individuals displayed a higher neutralizing efficacy than those from the BNT–BNT vaccinated individuals (median (IQR) of 62% (34–93%) versus 99% (89–100%) of neutralization, respectively; P < 0.001) (Fig. 2d).
To validate these results, we tested the ability of the sera to prevent Vero E6 cell infection by SARS-CoV-2 isolates belonging to various clades, including 19A (B38 lineage), Alpha (B.1.1.7 lineage), Beta (B.1.351 lineage), Gamma (P1) and Delta (B.1.617.2 lineage)9. Each SARS-CoV-2 isolate was sequenced and confirmed to contain the characteristic mutations of its viral clade. The ChAd–BNT vaccinated individuals exhibited 2.3-fold to 3.6-fold higher serum neutralizing antibody titres against the different variants than BNT–BNT vaccinated individuals (Fig. 2e). Moreover, in the latter group, the neutralizing responses observed against the Beta, Gamma and Delta variants were significantly reduced compared with that against the 19A clade. By contrast, the neutralizing activity detected in sera from ChAd–BNT vaccinees was similarly high against all strains except the Beta clade (Fig. 2e, f). These data demonstrate that the neutralizing potential of antibodies generated by heterologous vaccination is less affected by spike mutations appearing in variants of concern than that of antibodies induced by homologous vaccination.
Vaccine-induced memory cells
We then studied the memory B cell (mBC) compartments using fluorescently labelled tetrameric RBDs to track RBD-specific mBCs and to analyse their phenotype (the gating analysis is presented in Extended Data Fig. 2a). As shown in Fig. 3a and Extended Data Fig. 2b, which correspond to concatenated flow cytometry plots, the frequency of RBD-binding mBCs was comparable for both vaccination groups after the prime dose but was on average twofold higher for the ChAd–BNT vaccination schedule after the booster dose. Moreover, switched (IgD–CD27+) mBCs accounted for about 67% and 47% of the RBD-specific mBC pool in the ChAd–BNT group and the BNT–BNT group, respectively (Fig. 3b, c, Extended Data Fig. 2c). The expression pattern of IgM and IgG isotypes was next used to compare the immunoglobulin isotype distribution among the switched mBCs. The results showed that the homologous vaccination schedule promoted more IgG-switched mBCs (62% versus 48%) than the heterologous vaccination schedule (Fig. 3d, Extended Data Fig. 2d). Finally, to address the activation status of mBCs, we analysed their expression of CD21 and CD11c. It is generally considered that the concurrent loss of CD21 and the upregulation of CD11c are phenotypic features associated with B cell activation independent of the developmental stage10. Resting mBCs were therefore defined as CD21+CD11c– cells, whereas CD21+CD11c+, CD21–CD11c+ and CD21–CD11c– cells were globally considered as activated mBCs. The frequencies of activated RBD-specific mBCs were significantly enhanced in the ChAd–BNT group compared with the BNT–BNT group (Fig. 3e, Extended Data Fig. 2e). In particular, the proportions of the CD21–CD11c+ subset were almost three times higher in the ChAd–BNT group. Altogether, our results indicate that compared with the homologous vaccination schedule, the ChAd–BNT combination induces significantly more RBD-specific B cells, increases the frequencies of post-switch mBCs and induces a more active mBC generation process.

a–e, Flow cytometry analyses of spike-specific mBCs. a, Frequencies of SARS-CoV-2 RBD-binding mBCs among the pool of polyclonal mBCs before vaccination, after prime and after boost injections. b, c, Proportions of unswitched (b) and switched (c) RBD-binding mBCs in per cent of RBD-binding mBCs. d, Pattern of immunoglobulin isotypes expressed by switched mBCs. e, Proportions of resting (CD21+CD11c–) and activated (CD21–CD11c+, CD21–CD11c– and CD21+CD11c+) mBCs among the entire pool of RBD-binding mBCs. f–h, T cell responses. f, IFNγ release after whole-blood stimulation with RBD peptides. IFNγ was measured by ELISA in the supernatant. g, h, Flow cytometry analyses of the percentage of cells positive for intracellular IFNγ expression among CD4 (g) or CD8 (h) T cells after PBMC stimulation with commercial spike peptides. In all panels, box-and-whiskers plots (see Methods for details) of n = 29 and n = 31 participants in heterologous and homologous vaccination groups, respectively, are shown. The median value is shown in each group as a purple line. A high cellular mortality rate at the thawing step led to the exclusion of a few samples in each panel; each individual dot corresponds to one participant, and each measurement was performed once. In all panels, a linear regression model was used to compare values between groups, and this model was corrected for age. Exact P values are shown for the indicated comparisons when significant or nearly significant.
We then longitudinally monitored the T cell response of vaccinees against RBD peptides using a whole-blood interferon-γ (IFNγ) release assay. The T cell response was higher after ChAd immunization than after BNT priming and was similarly increased by the BNT booster dose in both groups (median of 0.33 UI ml–1 versus 0.43 UI ml–1) (Fig. 3f). To confirm and consolidate these results, we measured the spike-specific CD4 and CD8 T cell response at the single-cell level by flow cytometry after stimulating peripheral blood mononuclear cells (PBMCs) from vaccinees with a pool of commercial peptides spanning the entire spike protein and then staining for intracellular IFNγ (the gating strategy is presented in Extended Data Fig. 3). Both vaccination regimens were able to induce a progressive increase in the frequency of S-reactive CD4 and CD8 T cells from the pre-vaccine to the post-booster phase (Fig. 3g, h). However, the heterologous combination resulted in a stronger CD4 T cell response, both after priming and boosting, and in an increasing trend in the CD8 T cell response after the booster dose.
Finally, to understand interrelations between immune parameters, we performed a matrix analysis (Extended Data Fig. 4). This confirmed that the neutralizing antibody activity correlated with the titres of spike-specific IgG, regardless of the variant analysed, and not correlated with IgA levels. Moreover, the neutralization activity correlated with the percentage of switched RBD+ mBCs and with the percentage of activated RBD+ mBCs. This provides further support that better neutralizing antibodies are produced as a result of sustained B cell activation.
Discussion
Heterologous prime–boost vaccinations have been reported to be more immunogenic than homologous ones in experimental settings11. This has also been proven for some human vaccines12,13. Moreover, studies using mice have demonstrated the strong immunogenicity of the ChAd–BNT combination14. Here we report that heterologous ChAd–BNT vaccination confers better protection against infection—which is associated with more switched mBCs and higher virus neutralizing antibody titres—irrespective of the variant analysed. This finding is of particular importance considering the global increase in the SARS-CoV-2 Delta variant15. Other studies reported better neutralizing potential of sera from ChAd–BNT vaccinated individuals compared with BNT–BNT vaccinated individuals, but these studies only used surrogate16,17 or pseudovirus18 neutralization assays. Moreover, the ability of such assays to predict neutralizing activity against authentic clinical virus isolates is still debated19.
Heterologous vaccination induced antibodies with a stronger neutralization potential than homologous vaccination, but the spike-specific IgG antibody titres were comparable. This result suggests that it is the quality of the antibodies that underlies the neutralization potential of the antibody response induced by heterologous vaccination. Assuming that the secondary antibody response is primarily derived from the mBC clones generated by primo-immunization, we can postulate that ChAd and BNT formulations elicit different mBC compartments. mBCs generated by the ChAd formulation could, for example, bear antigen receptors displaying a larger breadth of epitope recognition or a better fit for the SARS-CoV-2 spike protein. This could be linked to the different conformations of the spike protein, as that of the BNT vaccine bears a mutation stabilizing the protein in its pre-fusion conformation20. Our data showed that mBCs still exhibit features of activation 4 weeks after the booster dose in the heterologous regimen, which suggests that the post-boost process of mBC differentiation is more active in this schedule. This could result from a more efficient or long-lasting germinal centre reaction that facilitates an extended cycle of somatic hypermutations and possibly output of B cell clones with higher affinity antigen receptors. An enlarged pool of CD4+ T helper cells could contribute to an amplified or prolonged germinal centre reaction. In keeping with this notion, we report here a higher frequency of spike-specific CD4 T cells after priming with the ChAd vaccine, which has been observed in other studies6,7. Moreover, stronger T cell responses may contribute to better protection independently of B cell responses21.
The better neutralization potential of sera from ChAd–BNT vaccinated individuals could also be linked to their relatively lower level of S1-specific IgA levels. Indeed, plasma IgA monomers specific to SARS-CoV-2 proteins are twofold less potent than IgG equivalents22. Furthermore, IgA levels persist better than IgG after infection, which coincides with a reduction in the serum neutralizing potential23. Following a possible competition between serum IgA and IgG, the decrease in IgA levels in heterologous vaccination conditions may lead to better neutralization effects. This phenomenon has already been observed in the context of the RV144 vaccination trial against HIV-1, in which the level of envelope-specific IgA correlated with the risk of infection24. In this context, IgA was also found to inhibit antibody-dependent cell cytotoxicity by competing with IgG25.
Our data do not allow the discarding of the possibility that the later timing of administration of the booster dose contributed to the high efficacy of the heterologous regimen. Still, it is noteworthy that the size of the RBD+ mBC pool after the prime dose was comparable for both groups of vaccinees, despite the disparity in the analysis time point after the prime vaccination (4 versus 12 weeks). This observation indicates that the extended interval between prime and boost in the ChAd–BNT cohort has not been translated into a greater size of the RBD-specific mBC compartment. It has been recently demonstrated for both the ChAd vaccine26 and the BNT vaccine27 that long injection time intervals (12 weeks or more) provide higher binding and neutralizing antibody titres than shorter intervals (less than 6 weeks). For a comparable long vaccination interval (more than 9 weeks), the heterologous ChAd–BNT vaccination schedule induced better humoral immunity (titres and neutralization) than the homologous ChAd–ChAd combination28. To our knowledge, there is only one study in which ChAd–BNT and BNT–BNT vaccination schedules were compared with the same prime–boost interval (4 weeks)6. That study6 concluded that for short intervals, the humoral responses induced by both regimens were comparable. However, a longer interval (that is, 12 weeks) between prime and boost could be needed to allow the synergy between heterologous vaccines.
Together, we present a real-world observational study of HCWs showing that the heterologous ChAd–BNT vaccination regimen confers stronger protective immunity than the homologous BNT–BNT prime–boost schedule. As hidden confounding factors might be present in our study (for example, different levels of exposure to the virus), confirmatory studies and a longer follow-up of vaccinated participants are warranted. However, our data suggest that the heterologous combination could be particularly suitable for immunocompromised individuals.
Methods
Ethical statement and cohort description
The use and analysis of data from the occupational health medical file were authorized after a regulatory declaration to the National Commission for Information Technology and Civil Liberties according to the reference methodology (declaration MR004 number 20-121 of 30 April 2020). The declaration of SARS-CoV-2 infection is compulsory for all staff to obtain daily allowances without loss of salary during the imposed quarantine.
For the Covid-Ser-Vac study, clinical data were recorded by a trained clinical research associate using Clinsight software (v.Csonline 7.5.720.1). Blood samples were processed and stored at the Centre de Ressource Biologique Neurobiotec, 69500 Bron. Sixty naive HCWs for COVID-19 and vaccinated with BNT and/or ChAd vaccines were included in a prospective longitudinal cohort study conducted at the Hospices Civils de Lyon. Blood sampling was performed before vaccination, before the second dose of vaccine and 4 weeks after the end of vaccination schedule. The absence of previous SARS-CoV-2 infection was confirmed using the Wantai SARS-CoV-2 Ab total assay in the pre-vaccine sample. Demographic characteristics and delays between doses are depicted in Table 2 and Extended Data Fig. 1. Written informed consent was obtained from all participants. Ethics approval was obtained from the national review board for biomedical research in April 2020 (Comité de Protection des Personnes Sud Méditerranée I, Marseille, France; ID RCB 2020-A00932-37), and the study was registered at ClinicalTrials.gov (NCT04341142).
Measurement of IgG titres
Sera were immediately stored at –80 °C after blood sampling. S1-specific IgG and RBD-specific IgG were measured using Siemens Atellica IM SARS-CoV-2 IgG (sCOVG) and bioMérieux Vidas SARS-CoV-2 IgG diagnosis kits, respectively, according to the manufacturers’ recommendations. For standardization of these assays to the first World Health Organization international standard, the concentrations were transformed into binding antibody units per ml (BAU ml–1) using the conversion factors provided by the manufacturers.
Measurement of spike-specific IgA
ELISAs to evaluate IgA binding to the SARS-CoV-2 spike protein were performed as previously described29. High-binding 96-half-well plates (2310M, Nunc) were coated with 100 μl per well of a spike protein solution (1 μg ml–1; 40591-V08H spike S1-RBD, Sino Biologicals) in PBS overnight at 4 °C. Plates were washed with washing buffer containing 1× PBS with 0.05% Tween 20 (Sigma-Aldrich) and incubated with 170 μl of blocking buffer per well containing 1× PBS with 3% fat milk powder and 0.05% Tween 20 (Sigma-Aldrich) for 1 h at room temperature. Immediately after blocking, recombinant anti-RBD IgA (B Cell Design, IB3C4 PV) or serum samples diluted in PBS were added and incubated for 1 h at 37 °C. Plasma samples were assayed at a 1:100 starting dilution and 7 additional 3-fold serial dilutions. Recombinant human anti-RBD IgA was used to perform a calibration curve starting at 1.5 µg ml–1. Plates were washed and then incubated with anti-human IgA (A0295, Sigma-Aldrich) secondary antibody conjugated to horseradish peroxidase in blocking buffer at 1:10,000. Plates were developed by the addition of the horseradish peroxidase substrate 3,3′,5,5′-tetramethylbenzidine (TMB; 34021, Thermo Fisher Scientific) for 10 min, and the developing reaction was stopped by adding 50 μl of 1 M HCl. Optical density units were measured at 450 nm in a microplate reader (Tecan). For serum samples, a positive control (serum pool from critically ill patients with COVID-19, diluted 200-fold in PBS) and a negative control (pool of historical serum samples) were added in duplicate to each run. After deduction of the background, a relative content in IgA equivalent (ng ml–1 Eq) was calculated using the calibration curve. The limit of detection of the assay was 0.1 ng ml–1 Eq.
Live-virus neutralization experiments
A plaque reduction neutralization test (PRNT) was used for the detection and titration of neutralizing antibodies. A tenfold dilution of each serum specimen in culture medium was first heated for 30 min at 56 °C to avoid complement-linked reduction of viral activity. Serial twofold dilutions (tested in duplicate) of the serum specimens in culture medium were mixed in equal volume with the live SARS-CoV-2 virus. After gentle shaking and a contact of 30 min at room temperature in plastic microplates, 150 µl of the mix was transferred into 96-well microplates covered with Vero E6 cells (American Type Culture Collection (ATCC), CRL-1586, not authenticated but regularly tested for mycoplasma contamination). The plates were incubated at 37 °C in a 5% CO2 atmosphere. Infection efficiency was evaluated by microscopy 5 days later when the cytopathic effect of the virus control reached 100–500 TCID50 (median culture infectious dose) per 150 µl. Neutralization was recorded if more than 50% of the cells present in the well were preserved. The neutralizing titre was expressed as the inverse of the higher serum dilution that exhibited neutralizing activity; a threshold of 20 was used (PRNT50 titre ≥ 20). All experiments were performed in a biosafety level 3 laboratory. The different viral strains that were used were sequenced and deposited at GISAID (https://www.gisaid.org/) (accession numbers EPI_ISL_1707038 19A (B.38 lineage); EPI_ISL_1707039 Alpha (B.1.1.7 lineage); EPI_ISL_768828 Beta (B.1.351 lineage); EPI_ISL_1359892 Gamma (P.1 lineage); and EPI_ISL_1904989 Delta (B.1.617.2 lineage)).
Monitoring of T cell responses using whole-blood IFNγ release assay
Fresh blood collected in heparinized tubes was stimulated for 22 h at 37 °C under 5% CO2 with SARS-CoV-2 peptide pools (derived from the prototype Wuhan strain NC_045512.2) targeting RBD (46 peptides, [C] = 8 µg ml–1) (bioMérieux) diluted in IGRA solution (bioMérieux). The peptides (15-mer) encompassed the entire protein sequence and overlapped by five residues. The IGRA solution was used as a negative control and a mitogen as a positive control. The concentration of IFNγ in the supernatant was measured using a VIDAS automated platform (VIDAS IFNγ RUO, bioMérieux). The measuring range was 0.08–8 IU ml–1 and WB IGRA positivity thresholds were defined at 0.08 IU ml–1. The IFNγ response was defined as detectable when the IFNγ concentration of the test was above threshold and the negative control was below threshold or when the IFNγ concentration of the test minus IFNγ concentration of the negative control was above threshold.
Monitoring of T cell responses by flow cytometry
Overnight-rested PBMCs were stimulated with SARS-CoV-2 overlapping peptide pools against SARS-CoV-2 spike protein (PepTivator, Miltenyi Biotec) at a final concentration of 1 μg ml–1 for 1 h in the presence of 1 μg ml–1 monoclonal antibodies CD28 and CD49d, and then for an additional 5 h with GolgiPlug and GolgiStop (BD Biosciences). Dead cells were labelled using Fixable Viability eFluor 780 dye (Thermo Fisher Scientific). Surface markers were stained using BV786-conjugated anti-CD3 (BD Biosciences, 565491; diluted 1:100), BUV486-conjugated anti-CD4 (BD Biosciences, 612937; 1:50), PE-Cy7-conjugated anti-CD8 (BioLegend, 301012; 1:100), APC-Cy7-conjugated anti-CD14 (BioLegend, 301820; 1:100), APC-Cy7-conjugated anti-CD56 (BioLegend, 362512; 1:100) and APC-Cy7- conjugated anti-CD19 (BioLegend, 302218; 1:100). Cells were then washed, fixed with Cytofix/Cytoperm (BD Biosciences) and stained with PE-conjugated anti-IFNγ (BioLegend). Negative controls without peptide stimulation were run for each sample. All results were acquired on a BD LSRFortessa (BD Biosciences) flow cytometer using the BD FACSDIVA v.8.01 software and analysed using FlowJo v.10.6.1 software.
SARS-CoV-2 pseudoparticle preparation and neutralization
SARS-CoV-2 spike-pseudotyped murine leukaemia virus retrovirus particles were produced as described for SARS-CoV30. In brief, HEK293T cells (ATCC, CRL-1573, not authenticated but regularly tested for mycoplasma contamination) were transfected with constructs expressing murine leukaemia virus Gag-Pol, the green fluorescent protein (GFP) reporter and the SARS-CoV-2 spike protein (a gift from D. Lavillette (CAS Key Laboratory of Molecular Virology & Immunology, Institut Pasteur of Shanghai Chinese Academy of Sciences, Pasteurien College, Soochow University, Jiangsu, China)). Control particles pseudotyped with the unrelated RD114 virus surface glycoprotein (from a cat endogenous virus) were generated as previously described31. For neutralization assays, a sample of approximately 1 × 103 pseudoparticles was incubated with a 100-fold dilution of sera or control antibodies for 1 h at 37 °C, spinoculated for 2 h at 2,500g before infection of Vero E6 cells. After 72 h of infection, the percentage of GFP-positive cells was determined by flow cytometry. As a control, the same procedure was performed using RD114 pseudoparticles. Anti-spike SARS-CoV-2 RBD (Sino Biological, 40150-V08B2) and anti-gp70 RD114 (ViroMed Biosafety Labs) antibodies were used with a 100-fold dilution as positive and negative control, respectively.
Generation of fluorescent SARS-CoV-2 RBD tetramers
Biotinylated recombinant RBD domain of SARS-CoV-2 RBD was purchased from Miltenyi Biotech (130-127-457) and tetramerized with either streptavidin-PE (Becton Dickinson (BD)) or with streptavidin-APC (BioLegend, 105243).
Flow cytometry analysis of SARS-CoV-2 RBD-specific B cells
Cryopreserved PBMCs were centrifuged and suspended in PEB buffer (PBS with 0.5% BSA and 2 mM EDTA) and incubated with Fc receptor block (Miltenyi, 130-059-901) for 15 min at 4 °C (dilution 1:10). Next, cells were washed in PEB and stained for 30 min in brilliant stain buffer at 4 °C in the dark using the following antibodies together with both the PE- and APC-conjugated recombinant RBD tetramers: anti-CD3-APC Fire 810 (BioLegend, 344858; diluted 1:100); anti-CD11c-BV785 (BioLegend, 301644; 1:50); anti-CD19-PE Vio770 (Miltenyi, 130-113-170; 1:100); anti-CD20-BV421 (BD, 562873; 1:100); anti-CD21-BUV496 (BD, 750614; 1:50); anti-CD27-PercP-Vio700 (Miltenyi, 130-113-632; 1:100); anti-CD38-Viobright FITC (Miltenyi, 130-113-433: 1:50); anti-IgM-PE-CF594 (BD, 562539; 1:50); anti-IgD-BV605 (BioLegend, 348232; 1:50); and anti-IgG-BV480 (BD, 746341; 1:50). Cells were washed in PEB and resuspended in a PEB dilution (1:500) of the fixable viability dye eFluor 780 (eBiosciences, 65-0865-18). They were next washed and fixed with 4% paraformaldehyde for 20 min at 4 °C in the dark before a final wash and resuspension for analysis. Cells were then acquired on a Cytek Aurora spectral flow cytometer equipped with five lasers operating at 355 nm, 405 nm, 488 nm, 561 nm and 640 nm using the SpectroFlo V.2.2.0 (Cytek) software. Data were analysed using FlowJo 10.6.1 software (BD).
Statistical analyses
Statistical modelling for epidemiological data
To model the probability of being infected knowing the subject age and the used vaccination regimen, we used the generalized linear model (glm) function in R to perform a multiple logistic regression model with the logit link function. The outcome variable was the infection status, whereby infected = 1 and not infected = 0. Our predictors were the age, as a continuous variable (considered as a possible confounder), and the vaccination regimen, whereby Chad–BNT = 0 and BNT–BNT = 1. On the basis of the model coefficients for the vaccination regimen (B0 = –5.306 and B1 = 0.712), we also assessed the relative risk (RR) as follows: RR = (1 + exp(–B0))/(1 + exp(–B0 – B1)).
Statistical analysis for immunological and virological analyses
ChAd–BNT and BNT–BNT populations showed a significant difference in the average ages. To test for the consequence of the vaccination regimen on the different immune parameters, we fitted a multiple linear regression model, which allows for the correction of age (as a possible confounding factor) by including age and vaccination regimen simultaneously as predictors in the right explanatory side of the lm function in R (one model per immune parameter). Results of statistical significance displayed in Figs. 2 and 3 are from these adjusted models, for which age showed no effect. For box and whiskers plots, the upper and lower bounds of the box are the 75th and the 25th percentile (the third Q3 and first Q1 quartile), respectively. The IQR = Q3 – Q1; an observation was considered an outlier if it was above Q3 + 1.5 × IQR or below Q1 – 1.5 × IQR. Upper and lower whiskers represent the maximum and the minimum values, respectively, without taking into account the outliers.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this paper.
Data availability
Viral sequences are available at GISAID (accession numbers EPI_ISL_1707038 19A (B.38 lineage); EPI_ISL_1707039 Alpha (B.1.1.7 lineage); EPI_ISL_768828 Beta (B.1.351 lineage); EPI_ISL_1359892 Gamma (P.1 lineage); and EPI_ISL_1904989 Delta (B.1.617.2 lineage). Source data are provided with this paper.
References
Greinacher, A. et al. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N. Engl. J. Med. 384, 2092–2101 (2021).
Scully, M. et al. Pathologic antibodies to platelet factor 4 after ChAdOx1 nCoV-19 vaccination. N. Engl. J. Med. 384, 2202–2211 (2021).
Polack, F. P. et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 383, 2603–2615 (2020).
Ramasamy, M. N. et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime–boost regimen in young and old adults (COV002): a single-blind, randomised, controlled, phase 2/3 trial. Lancet 396, 1979–1993 (2021).
Voysey, M. et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 397, 99–111 (2021).
Liu, X. et al. Safety and immunogenicity of heterologous versus homologous prime–boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): a single-blind, randomised, non-inferiority trial. Lancet 398, 856–869 (2021).
Hillus, D. et al. Safety, reactogenicity, and immunogenicity of homologous and heterologous prime–boost immunisation with ChAdOx1 nCoV-19 and BNT162b2: a prospective cohort study. Lancet Respir. Med. 9, 1255-1265 (2021).
Legros, V. et al. A longitudinal study of SARS-CoV-2-infected patients reveals a high correlation between neutralizing antibodies and COVID-19 severity. Cell. Mol. Immunol. 18, 318–327 (2021).
Gonzalez, C. et al. Live virus neutralisation testing in convalescent patients and subjects vaccinated against 19A, 20B, 20I/501Y.V1 and 20H/501Y.V2 isolates of SARS-CoV-2. Emerg. Microbes Infect. 10, 1499–1502 (2021).
Sanz, I. et al. Challenges and opportunities for consistent classification of human B cell and plasma cell populations. Front. Immunol. 10, 2458 (2019).
Lu, S. Heterologous prime–boost vaccination. Curr. Opin. Immunol. 21, 346–351 (2009).
Jou, J., Harrington, K. J., Zocca, M.-B., Ehrnrooth, E. & Cohen, E. E. W. The changing landscape of therapeutic cancer vaccines—novel platforms and neoantigen identification. Clin. Cancer Res. 27, 689–703 (2021).
Levine, M. Z. et al. Heterologous prime–boost with A(H5N1) pandemic influenza vaccines induces broader cross-clade antibody responses than homologous prime-boost. NPJ Vaccines 4, 22 (2019).
Spencer, A. J. et al. Heterologous vaccination regimens with self-amplifying RNA and adenoviral COVID vaccines induce robust immune responses in mice. Nat. Commun. 12, 2893 (2021).
Alizon, S. et al. Rapid spread of the SARS-CoV-2 Delta variant in some French regions, June 2021. Euro Surveill. 26, 2100573 (2021).
Schmidt, T. et al. Immunogenicity and reactogenicity of heterologous ChAdOx1 nCoV-19/mRNA vaccination. Nat. Med. 27, 1530–1535 (2021).
Tenbusch, M. et al. Heterologous prime–boost vaccination with ChAdOx1 nCoV-19 and BNT162b2. Lancet Infect. Dis. 21, 1212–1213 (2021).
Groß, R. et al. Heterologous ChAdOx1 nCoV-19 and BNT162b2 prime–boost vaccination elicits potent neutralizing antibody responses and T cell reactivity. Preprint at https://doi.org/10.1101/2021.05.30.21257971 (2021).
von Rhein, C. et al. Comparison of potency assays to assess SARS-CoV-2 neutralizing antibody capacity in COVID-19 convalescent plasma. J. Virol. Methods 288, 114031 (2021).
Juraszek, J. et al. Stabilizing the closed SARS-CoV-2 spike trimer. Nat. Commun. 12, 244 (2021).
Sette, A. & Crotty, S. Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 184, 861–880 (2021).
Wang, Z. et al. Enhanced SARS-CoV-2 neutralization by dimeric IgA. Sci. Transl. Med. 13, eabf1555 (2021).
Wang, Z. et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature 595, 426–431 (2021).
Haynes, B. F. et al. Immune-correlates analysis of an HIV-1 vaccine efficacy trial. N. Engl. J. Med. 366, 1275–1286 (2012).
Tomaras, G. D. et al. Vaccine-induced plasma IgA specific for the C1 region of the HIV-1 envelope blocks binding and effector function of IgG. Proc. Natl Acad. Sci. USA 110, 9019–9024 (2013).
Voysey, M. et al. Single-dose administration and the influence of the timing of the booster dose on immunogenicity and efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine: a pooled analysis of four randomised trials. Lancet 397, 881–891 (2021).
Payne, R. P. et al. Immunogenicity of standard and extended dosing intervals of BNT162b2 mRNA vaccine. Cell 184, 5699–5714 (2021).
Barros-Martins, J. et al. Immune responses against SARS-CoV-2 variants after heterologous and homologous ChAdOx1 nCoV-19/BNT162b2 vaccination. Nat. Med. 27, 1525–1529 (2021).
Amanat, F. et al. A serological assay to detect SARS-CoV-2 seroconversion in humans. Nat. Med. 26, 1033–1036 (2020).
Broer, R., Boson, B., Spaan, W., Cosset, F.-L. & Corver, J. Important role for the transmembrane domain of severe acute respiratory syndrome coronavirus spike protein during entry. J. Virol. 80, 1302–1310 (2006).
Lavillette, D. et al. Human serum facilitates hepatitis C virus infection, and neutralizing responses inversely correlate with viral replication kinetics at the acute phase of hepatitis C virus infection. J. Virol. 79, 6023–6034 (2005).
Acknowledgements
This study was supported by IDEX Lyon (HPI-2019), operated by the French National Research Agency (ANR-11-IDEX-0007), INSERM-Transfert and by institutional grants from Fondation des Hospices Civils de Lyon, INSERM, CNRS, UCBL1 and ENS de Lyon. We thank the following staff members and individuals: all the staff members of the Occupational Health and Medicine Department of the Hospices Civils de Lyon (who contributed to the sample collection) and all the clinical research associates for their excellent work; the staff members of SFR Biosciences (UAR3444/CNRS, US8/INSERM, ENS de Lyon, UCBL) AniRA-cytometry, E. Devêvre, S. Dussurgey and V. Malassigné; K. Brahima and all the members of the clinical research and innovation department for their reactivity (DRCI, Hospices Civils de Lyon); and all the HCWs for their participation in this clinical study. Human biological samples and associated data were obtained from NeuroBioTec (CRB HCL, Lyon France, Biobank BB-0033-00046).
Author information
Authors and Affiliations
Consortia
Contributions
B.P., V.L., S. Djebali, V.B., M. Villard, L.P., M.Y.-N., S. Denolly, B.B., T.B., M. Valette, A.B. and K.B.-P. performed experiments and analysed the data. T.A. helped with the analysis of flow cytometry data and O.A. performed statistical analyses. N.G., J.-B.F. and A.M.-P. analysed the clinical infection data. The Covid-Ser study members collected the samples and performed experiments. B.L. supervised some of the experimental tasks. F.-L.C., S.P., T.D., J.M., T.W. and S.T.-A. designed the study, analysed the data and wrote the manuscript.
Corresponding authors
Ethics declarations
Competing interests
K.B.-P. is a bioMérieux employee.
Additional information
Peer review information Nature thanks Yunda Huang, Pei-Yong Shi and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
Extended Data Fig. 1 Study design.
Sixty HCWs naïve for COVID-19 and vaccinated with the Pfizer ChAd/BNT or the BNT/BNT combination were included in a prospective longitudinal cohort study. Blood sampling was performed as described, before vaccination, before the second dose of vaccine and 4 weeks after the end of vaccination schedule. Different immunological analyses were performed on the blood samples, including serological investigations (Spike-specific IgA and IgG), serum neutralization assays (both plaque reduction neutralization test (PRNT) and pseudoneutralization), analysis of Spike-specific T cells and RBD-specific memory B cells, at various time points indicated in the text. Parts of the figure were drawn by using pictures from Servier Medical Art (http://smart.servier.com/), licensed under a Creative Commons Attribution 3.0 Unported License (https://creativecommons.org/licenses/by/3.0/).
Extended Data Fig. 2 Analysis of RBD-specific memory B cells.
(A) Gating strategy. From left to right, the first three pseudo-color plots show the successive gates applied for single cells and viable cells. B cells were gated as CD19+/CD3- cells (4th plot). Within the B cell gate, memory B cells (mBCs) were defined as non-naïve B cells on the same biparameter plot (5th plot). (B-E) Concatenated phenotypic profiles of RBD-specific mBCs for all individuals in the ChAd/BNT and BNT/BNT groups at three time points (before vaccination, before the 2nd dose, after the second dose). For each group, the phenotypic profiles correspond to the concatenation of the FACS analysis data collected from 30 individual vaccinees. (B) Visualization of RBD-binding B cells in the mBC gate. (C) Visualization of the proportion of switched (IgD-) and unswitched (IgD+) B cells among the RBD-specific mBC pool. (D) Visualization of the pattern of Ig isotype expression by RBD-specific mBCs. (E) Visualization of the distribution of RBD-binding B cells within the resting (CD21+CD11c-) and “activated” (CD21-CD11c+/CD21-CD11c-/ CD21+CD11c+) mBC compartments. The mean frequencies of RBD-specific mBCs falling into each quadrant are indicated in red.
Extended Data Fig. 3 Analysis of SARS-CoV-2-specific T cells.
PBMCs were stimulated as detailed in the methods and stained for CD3, CD4, CD8, CD14, CD56 and CD19 expression and with a dead cell marker. Cells were gated from left to right and top to bottom. The Viab/dump channel includes antibodies against CD14, CD19, CD56 and a viability marker. The frequency of CD4 or CD8 T cells positive for intracellular IFNg was measured as shown in the central and right bottom panels.
Extended Data Fig. 4 Analysis of inter-relationships between immune parameters.
A matrix file with all immunological measurements for all vaccinated individuals showing the Spearman correlations and associated p-values. The size and the color of the circles correspond to the correlation, as indicated, and the stars indicate the significance of the correlation.
Supplementary information
Rights and permissions
About this article

Cite this article
Pozzetto, B., Legros, V., Djebali, S. et al. Immunogenicity and efficacy of heterologous ChAdOx1–BNT162b2 vaccination. Nature 600, 701–706 (2021). https://doi.org/10.1038/s41586-021-04120-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41586-021-04120-y
This article is cited by
-
An intranasal combination vaccine induces systemic and mucosal immunity against COVID-19 and influenza
npj Vaccines (2024)
-
Hybrid and herd immunity 6 months after SARS-CoV-2 exposure among individuals from a community treatment program
Scientific Reports (2023)
-
New-onset aplastic anemia after SARS-CoV-2 vaccination
International Journal of Hematology (2023)
-
IgA antibody dynamics in healthcare workers after CoronaVac® vaccination and heterologous Comirnaty® booster dose
Brazilian Journal of Microbiology (2023)
-
Case reports of management of aplastic anemia after COVID-19 vaccination: a single institute experience in Taiwan
International Journal of Hematology (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
