
Abstract
Although severe COVID-19 in children is rare, they may develop multisystem inflammatory syndrome, long-COVID and downstream effects of COVID-19, including social isolation and disruption of education. Data on the effectiveness of the CoronaVac vaccine is scarce during the Omicron period. In Brazil, children between 6 to 11 years are eligible to receive the CoronaVac vaccine. We conducted a test-negative design to estimate vaccine effectiveness using 197,958 tests from January 21, 2022, to April 15, 2022, during the Omicron dominant period in Brazil among children aged 6 to 11 years. The estimated vaccine effectiveness for symptomatic infection was 39.8% (95% CI 33.7–45.4) at ≥14 days post-second dose. For hospital admission vaccine effectiveness was 59.2% (95% CI 11.3–84.5) at ≥14 days. Two doses of CoronaVac in children during the Omicron period showed low levels of protection against symptomatic infection, and modest levels against severe illness.
Similar content being viewed by others

Introduction
Randomized clinical trials have demonstrated high mRNA vaccine efficacy and immunogenicity in children and adolescents1, 2. However, data related to the inactivated-virus vaccine (CoronaVac) of efficacy and effectiveness (VE) against the SARS-CoV-2 B.1.1.529 (Omicron) variant are lacking for children aged 6–11 years.
Although severe COVID-19 is a rare condition in children3, the widespread distribution of SARS-CoV-2 infection and the increasing number of cases in this population has caused a significant public health impact. Besides, children are also susceptible to the multisystem inflammatory syndrome in Children (MIS-C), long-COVID syndrome3, 4 and downstream effects of COVID-19, including social isolation and interruption in education4. Therefore, there is an urgent need to collect more data on the effectiveness of vaccines, especially in the Omicron period, to guide decision-makers in adopting policies, such as mandating mask use in school settings.
In Brazil, the children’s vaccination campaign started on January 21, 20225, and CoronaVac has been used for children aged 6–11 years. On April 15, 2022, vaccine uptake for all vaccines used in children was 62.9% for the 1st dose and 26.6% for the second dose. For CoronaVac, vaccine uptake was 35.1% for 1st dose and 19.8% for the second dose. To our knowledge, no report estimates vaccine effectiveness for CoronaVac among children aged 6–11 years during the Omicron period. Therefore, in this observational study using a nationwide database from Brazil, we estimated the vaccine effectiveness (VE) of the CoronaVac against medically attended symptomatic and severe COVID-19 in children aged 6–11 years.
Results
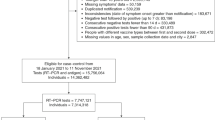
During the study period, 197,958 tests were performed on Brazilian children aged 6–11 years, with 89,595 (45.3%) cases and 108,363 (54.7%) controls, with 508 hospital admissions (Fig. S1). The age, sex, geographic region, socioeconomic position, comorbidities, and hospital admission were similar among the children who tested positive and negative (Table S1). For children between 6 and 11 years, VE against symptomatic COVID-19 during Omicron circulation was 21.2% (95% CI 18.6–23.8) after 13 days post first dose of CoronaVac. After the second dose, VE reached 30.8% (95% CI 24.2–36.8) at 0–13 days and 39.8% (95% CI 33.7–45.4) at ≥14 days (Table 1; Fig. 1) with most of the individuals being tested within 43 days after the second dose (Figure S2). For hospital admission among children vaccinated with one dose of CoronaVac at ≥14 days, the adjusted VE was 47.1% (95% CI 26.6–62.7). After two doses of CoronaVac, the adjusted VE was 82.4% (95% CI 44.2–97.1) at 0–13 days and 59.2% (95% CI 11.3–84.5) at ≥14 days (Table 1; Fig. 1). For ICU admission there were two cases among children vaccinated with two-dose at ≥14 days and the estimated VE for rare events was 20.9% (95% CI [−177.2]−85.0) (Table S2). No death events were detected among children vaccinated with two doses. The sensitivity analyses using multiple imputations for missing data in ethinicity (19.4%) produced similar results to the primary analyses (Table S3). Furthermore, the analyses excluding the previously infected group generated similar VE estimates (Table S4).

The dots represent the adjusted vaccine effectiveness (VE;1- adjusted odds ratio) estimates (sample n = 197,958), with error bars indicating the corresponding 95% Wald’s C.I. for symptomatic infection and Profile’s likelihood C.I. for hospital admission. Red represents adjusted VE against symptomatic infection, and blue against hospital admission considering vaccination status (in days post first and second dose). The comparison group was the unvaccinated.
Discussion
In this investigation of CoronaVac VE in children 6–11 years of age during Omicron variant predominance, we found that two doses of the CoronaVac vaccine were 39.8% effective against medically attended symptomatic COVID-19 and 59.2% effective in preventing hospital admission COVID-19 cases at ≥14 days after the second dose. The VE estimated in children 6–11 years in Brazil during the Omicron period was much lower than the effectiveness of 75.8% reported for the same demographic in Chile when B.1.617.2 (Delta) was the predominant circulating SARS-CoV-2 variant6. However, our data were comparable with results observed in children aged 3–5 during the Omicron outbreak in the same country, 38.2%; (95% CI, 36.5–39.9) against symptomatic disease and, 64.6% (95% CI, 49.6–75.2) against hospitalisation7. These findings are also in line with previous studies of VE in adult and adolescent populations that have shown a significant reduction in VE against Omicron compared with early pandemic variants8, 9. Although we have analysed VE at the optimal period of the second dose among children vaccinated with CoronaVac, it is likely to wane quickly, especially during the Omicron period as it was seen for the adolescent and children population vaccinated with BNT162b28, 10,11,12,13.
This study has strengths and limitations. A strength of this study is the high-quality nationwide database from Brazil. Furthermore, we used Test Negative Design (TND) to minimise bias related to access to health care and health-seeking behaviour. TND’s primary assumption is that people seeking and getting tested would be influenced by similar pressures regardless of vaccination status14. Another strength is the improbable under ascertainment of vaccination status since the all-vaccines doses administered against COVID-19 in Brazil are recorded in the national immunisation system (SI-PNI). An important limitation is the high rates of asymptomatic infection allied to limited testing in Brazil among children since the database from the study only accounts for tests from the healthcare system and not community testing. Also, the under ascertainment of previous infection may bias the VE estimates if this condition occurs differentially or non-differentially in the vaccinated and unvaccinated group15,16,17.
In summary, our findings indicate low levels of protection against symptomatic infection with the Omicron variant after two doses of vaccination with CoronaVac among children. Hence, in line with previous studies involving other vaccines and age groups, the vaccination program alone is unlikely to suppress viral circulation. However, this vaccine was 59.2% effective against COVID-19-hospital admissions, albeit with wide uncertainty intervals. Further studies will be necessary to assess the duration of protection, specially against complications of COVID-19 that occur in the pediatric population, such as MIS-C and long-COVID. Effectiveness also must continue to be monitored as new variants arise.
Methods
Data sources
Data were obtained from three routinely collected sources: the national surveillance system for RT-PCR and antigen tests for COVID-19 infection (e-SUS Notifica); the information system for severe acute respiratory illness (SIVEP-Gripe). These two datasets present notifications from public and private healthcare systems of SARS-CoV-2 suspected cases, and hospitalisation cases of SARS, respectively. Also, the national immunisation system (SI-PNI). A more detailed description from our database can be found in the Supplementary Materials. In addition, we deterministically linked the data using the information provided by DATASUS from the Brazilian Ministry of Health. Dataset quality assessment and linkage details have been described before18,19,20,21.
Study design
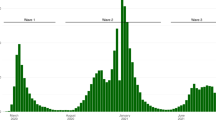
We used a test-negative design, which is a type of case-control study among the population tested, with controls selected from those who presented a negative test22. The study population comprised childrens aged 6–11 years with COVID-19-related symptoms in Brazil from January 21, 2022, to April 15, 2022, with a predominant circulation of the Omicron variant (>98% of sequenced viruses)23. We linked records of SARS-CoV-2 reverse transcription-polymerase chain reaction (RT-PCR) and antigen tests to national vaccination and clinical records. Participants were symptomatic children with a sample collected within ten days of symptom onset. Cases of confirmed infection were those with a positive SARS-CoV-2 RT-PCR or antigen test, and control had a negative SARS-CoV-2 RT-PCR or antigen test. Additionally, we evaluated severe COVID-19 (hospital admission), defined as a positive test that occurred within 14 days before the hospitalisation date and up to four days after hospital admission, and death occurring within 28 days after a positive test.
We excluded: (1) individuals older than 11 years and younger than 6 years; (2) individuals who received vaccines other than CoronaVac; and (3) tests among asymptomatic people and tests referring to a symptom onset date after the notification date; (4) individuals whose time interval between the first and second doses was less than 14 days and received first dose before January 21, 2022; (5) negative test within 14 days of a previous negative test; (6) negative test followed by a positive test up to 7 days; (7) any test after a positive test up to 90 days, and (8) tests with missing information on age, sex, city of residence, sample collection, or first symptoms date; (9) any individual which received the third dose. Our exposure was vaccination status stratified by the time since the last dose on the date of sample collection, categorised as: unvaccinated and, for the vaccinated, grouped in periods (days) after each dose: first dose (0–13 days, and ≥14 days), second dose (0–13, ≥14 days). In addition, the following confounders were included in the model: age, gender, ethnicity, time (month), region of residence, socioeconomic position measured by quintile of deprivation (the Índice Brasileiro de Privação in Brazil)24, previous SARS-CoV-2 infection (between 3–6 months or more six months ago), number of comorbidities commonly associated with COVID-19 illness. The odds ratio (OR) comparing the odds of vaccination between cases and controls and its associated 95% Confidence Interval (CI) were derived using logistic regression. VE was estimated as (1-OR)*100, obtained from an adjusted model including the described covariates, expressed as a percentage. All data processing and analyses were performed in R (version 4.1.1)25, using the Tidyverse package26. Missing values relating to ethnicity were imputed using multiple imputations, as sensitivity analyses. For these analyses, we used the MICE package (version 1.16) with five imputations27. We conducted a logistic regression for rare events (ICU admission) using Firth’s bias reduction method (Logistf package v. 1.24.1)28.
We followed the RECORD reporting guidelines (Table S5)29. The statistical analysis plan (SAP) was published in https://vigivac.fiocruz.br/. The Brazilian National Commission in Research Ethics approved the research protocol (CONEP approval number 4.921.308) and (CAAE registration no. 50199321.9.0000.0040). CONEP waived the requirement for informed consent because we did not have access to identified data. The Brazilian Ministry of Health authorized the use of these data by the Vaccination Digital Vigilance (VigiVac) program under the data protection law which allows such a consent for public health research.
Data availability
Our statistical analysis plan is available at https://vigivac.fiocruz.br. Regarding Brazilian data availability, one of the study coordinators (M.B.-N.) signed a term of responsibility on using each database made available by the Ministry of Health (MoH). Each member of the research team signed a term of confidentiality before accessing the data. Data was manipulated in a secure computing environment, ensuring protection against data leakage. The Brazilian National Commission in Research Ethics approved the research protocol (CONEP approval no. 4.921.308). Our agreement with the MoH for accessing the databases patently denies authorization of access to a third party. Any information for assessing the databases must be addressed to the Brazilian MoH at https://datasus.saude.gov.br/, and requests can be addressed to datasus@saude.gov.br. In this study, we used anonymized secondary data following the Brazilian Personal Data Protection General Law, but it is vulnerable to re-identification by third parties as they contain dates of relevant health events regarding the same person. To protect the research participants’ privacy, the approved Research Protocol (CONEP approval no. 4.921.308) authorises the dissemination only of aggregated data, such as the data presented here.
Code availability
All code used in this study is publicly available at https://github.com/cidacslab/vigivac/tree/main/tnd_02.
References
Frenck, R. W. et al. Safety, immunogenicity, and efficacy of the BNT162b2 Covid-19 vaccine in adolescents. N. Engl. J. Med. 385, 239–250 (2021).
Walter, E. B. et al. Evaluation of the BNT162b2 Covid-19 vaccine in children 5 to 11 years of age. N. Engl. J. Med. 386, 35–46 (2022).
Center for Disease Control and Prevention. Multisystem inflammatory syndrome in children (MIS-C) associated with coronavirus disease 2019 (COVID-19). (2020). Available at: https://emergency.cdc.gov/han/2020/han00432.asp. (Accessed: 14th May 2020).
Stein, M. et al. Project Report The Burden of COVID-19 in children and its prevention by vaccination: a joint statement of the israeli pediatric association and the israeli society for pediatric infectious diseases. Vaccines 10, 81 (2022).
Ministério da Saúde do Brasil. Nota Técnica No6/2022-Secovid/Gab/Secovid/Ms. (2022).
Jara, A. et al. Effectiveness of an inactivated SARS-CoV-2 vaccine in children and adolescents: a large- scale observational study. SSRN (2022).
Jara, A. et al. Effectiveness of CoronaVac in children 3 to 5 years during the omicron SARS-CoV-2 outbreak. Nat. Med. 28, 1377–1380 (2022).
Florentino, P. T. V. et al. Vaccine effectiveness of two-dose BNT162b2 over time against COVID-19 symptomatic infection and severe cases among adolescents: test negative design case control studies in Brazil and Scotland. The Lancet Infectious Diseases. 1–23 (2022).
Andrews, N. et al. Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant. N. Engl. J. Med. 386, 1532–1546 (2022).
Buchan, S. A., Nguyen, L., Wilson, S. E., Kitchen, S. A. & Kwong, J. Vaccine effectiveness of BNT162b2 against Omicron and Delta outcomes in adolescents. medRxiv 2022.04.07.22273319 (2022).
Veneti, L. et al. Vaccine effectiveness with BNT162b2 (Comirnaty, Pfizer-BioNTtech) vaccine against reported SARS-CoV-2 delta and omicron infection among adolescents, Norway, August 2021 to January 2022. SSRN Electron. J. 2, 1–11 (2022).
Dorabawila, V. et al. Effectiveness of the BNT162b2 vaccine among children 5–11 and 12–17 years in New York after the emergence of the Omicron Variant. medRxiv 2022.02.25.22271454 (2022).
Sacco, C. et al. Articles Effectiveness of BNT162b2 vaccine against SARS-CoV-2 infection and severe COVID-19 in children aged 5–11 years in Italy: a retrospective analysis of January-April, 2022. Lancet 2, 1–7 (2022).
Vandenbroucke, J. & Pearce, N. Test-negative designs differences and commonalities with other case–control studies with “other patient” controls. Epidemiology 30, 838–844 (2019).
Dawood, F. S., Porucznik, C. A., Veguilla, V. & Al, E. Incidence rates, household infection risk, and clinical characteristics of SARS-CoV-2 infection among children and adults in Utah and New York City, New York. Jama Pediatrics 176, 59–67 (2022).
Mensah, A. A. et al. Risk of SARS-CoV-2 reinfections in children: a prospective national surveillance study between January, 2020, and July, 2021, in England. Lancet Child Adolesc. Health 6, 384–392 (2022).
Lipsitch, M., Goldstein, E., Ray, G. T. & Fireman, B. Depletion-of-susceptibles bias in influenza vaccine waning studies: how to ensure robust results. Epidemiol. Infect. 147, e306 (2019).
Katikireddi, S. V. et al. Two-dose ChAdOx1 nCoV-19 vaccine protection against COVID-19 hospital admissions and deaths over time: a retrospective, population-based cohort study in Scotland and Brazil. Lancet 399, 25–35 (2022).
Cerqueira-Silva, T. et al. Vaccine effectiveness of heterologous CoronaVac plus BNT162b2 in Brazil. Nat. Med. 28, 838–843 (2022).
Cerqueira-Silva, T. et al. Vaccination plus previous infection: protection during the omicron wave in Brazil. Lancet Infect. Dis. 22, 1–2 (2022).
Cerqueira-Silva, T. et al. Effectiveness of CoronaVac, ChAdOx1 nCoV-19, BNT162b2, and Ad26.COV2.S among individuals with previous SARS-CoV-2 infection in Brazil: a test-negative, case-control study. Lancet Infect. Dis. 22, 791–801 (2022).
Vandenbroucke, J. P., Brickley, E. B., Vandenbroucke-Grauls, C. M. J. E. & Pearce, N. A test-negative design with additional population controls can be used to rapidly study causes of the SARS-COV-2 epidemic. Epidemiology 31, 836–843 (2020).
Fiocruz. GISAID. Rede Genômica (2020). Available at: http://www.genomahcov.fiocruz.br/#. (Accessed: 15th May 2022)
Allik, M. et al. Small-area Deprivation Measure for Brazil: Data Documentation. University of Glasgow (2020). Available at: https://researchdata.gla.ac.uk/980/. (Accessed: 15th May 2020).
Vienna, A. R. Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; (2021).
Wickham, H. et al. Welcome to the Tidyverse Tidyverse package. J. Open Source Softw. 4, 1–6 (2019).
van Buuren, S. & Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 45, 1–67 (2011).
Firth, D. “Bias reduction of maximum likelihood estimates.”. Biometrika 82, 667 (1995).
Benchimol, E. I. et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement. PLoS Med. 12, 1–22 (2015).
Acknowledgements
This study is part of the Fiocruz VigiVac programme and the authors acknowledge DATASUS for its diligent work in providing the unidentified Brazilian databases. This study was partially supported by a donation from the “Fazer o bem faz bem” program, from JBS, S.A, GLW, MLB, VB and M.B-N. are research fellows from the Brazilian National Research Council. M.B-N. acknowledges Fundação de Amparo à Pesquisa do Estado da Bahia (FAPESB)–Grant PNX0008/2014/ Fapesb, Edital 08/2014–Programa de Apoio a Núcleos de Excelência. G.L.W. acknowledges Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (E-26/210.180/2020). ESP is funded by the Wellcome Trust [Grant number 213589/Z/18/Z]. E.P.S. is funded by the Wellcome Trust [Grant number 213589/Z/18/Z]. The funders had no role in study design, data collection, data analysis, data interpretation, the report’s writing, or decision to publish. For the purpose of Open Access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript (AAM) version arising from this submission.
Author information
Authors and Affiliations
Contributions
E.S.P., M.L.B. and M.B.-N. conceived the idea for the study. All authors contributed to the study design, with P.T.V.F., E.S.P., A.G.J. and T.C.-S. drafting the statistical analysis plan. P.T.V.F. conducted the statistical analysis, E.S.P. checked the analysis code. P.T.V.F., J.B.S.J., T.C.-S. and V.dAO. had access to individual-level data for Brazil and performed data linkage. M.B.-N., V.dAO. and M.L.B. organised the data linkage and secured funding. E.S.P., P.T.V.F. and F.J.O.A. wrote the initial draft of the manuscript. E.S.P., L.R., G.L.W., G.O.P., M.L.B., V.B., N.P., and M.B.-N. critically revised the manuscript. PTVF and VdAO accessed and verified the data and analyses. All authors critically revised the manuscript and approved the final version for submission.
Corresponding author
Ethics declarations
Competing interests
M.B.-N. reports grants from the Fazer o bem faz bem program from JBS. S.A. V.dA.O., V.B., M.L.B., and M.B.-N. are employees of Fiocruz, a federal public institution, which manufactures Vaxzevria in Brazil, through a full technology transfer agreement with AstraZeneca. Fiocruz allocates all its manufactured products to the Ministry of Health for public health use. The remaining authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Nimalan Arinaminpathy and Alejandro Jara for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Florentino, P.T.V., Alves, F.J.O., Cerqueira-Silva, T. et al. Vaccine effectiveness of CoronaVac against COVID-19 among children in Brazil during the Omicron period. Nat Commun 13, 4756 (2022). https://doi.org/10.1038/s41467-022-32524-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41467-022-32524-5
This article is cited by
-
Real-world effectiveness and factors associated with effectiveness of inactivated SARS-CoV-2 vaccines: a systematic review and meta-regression analysis
BMC Medicine (2023)
-
Effectiveness of BNT162b2 and CoronaVac in children and adolescents against SARS-CoV-2 infection during Omicron BA.2 wave in Hong Kong
Communications Medicine (2023)
-
Effectiveness of COVID-19 vaccines among children and adolescents against SARS-CoV-2 variants: a meta-analysis
European Journal of Pediatrics (2023)
-
Immunogenicity, effectiveness, and safety of COVID-19 vaccines among children and adolescents aged 2–18 years: an updated systematic review and meta-analysis
World Journal of Pediatrics (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
