
Abstract
Glaucoma care has evolved dramatically over the past generation, with changes that have incorporated new technology and improved understanding of the disease process. A major need is to construct a useful definition of glaucomatous optic neuropathy that can be used to compare data across clinical research studies. The treatment of glaucoma should now be based on achievement of a goal target for intraocular pressure, unique to each patient. Adherence with eye drop treatment is far from ideal and can be improved using reminder systems. Sustained delivery of glaucoma medication is on the horizon. New surgical approaches to glaucoma are being actively studied but have not as yet found their place in its care, with rigorous testing against present treatments needed.
Similar content being viewed by others


Introduction
This perspective on glaucoma care will point to important, evidence-based diagnostic and therapeutic methods in glaucoma care. In each discussion area, I will highlight future needs and developing conceptual improvements. As is true in many aspects of modern life, the developments include the application of innovative technology to known problems that physicians and patients face in mitigating the effects of glaucoma.
It is time for an improved definition of glaucoma
In defining our problems and their solutions for glaucoma, a first step is the definition of the disease itself. One commonly reads in published literature on glaucoma that subjects were defined as having glaucoma because they had “characteristic optic disc and visual field defects as judged by a glaucoma expert.” This definition is overtly subjective and patently impossible to compare across studies, leaving us unable to know if we are studying persons with the same disease. In 2002, a more objective and reproducible definition of glaucomatous optic neuropathy (GON) was proposed for use in population-based prevalence surveys [1]. The method was based on the cup-to-disc ratio and automated visual field test result. In addition, terminology related to the levels of angle closure disease were included. Since then, this initial consensus definition has been cited in the peer-reviewed literature 1,350 times, comprising 10% of all articles dealing with glaucoma in the past 15 years. Clearly, there was a need served by this definitional structure in standardizing the interchange of ideas in glaucoma research.
It is now time, however, to move beyond this initial definition, as we have improved imaging technology to quantify the state of retinal ganglion cells and their axons. To develop such a definition of GON, an on-line discussion among glaucoma specialists worldwide used a Delphi methodology [2]—a series of discussion and conclusion sessions leading to an on-line survey that reached several initial conclusions about a definitional structure for GON. There was a consensus that GON could be defined by a combination of abnormality in optical coherence tomography (OCT) imaging and automated visual field testing if the locations “match” (e.g.-, an upper field defect matching a lower OCT defect). The group did not feel that any intraocular pressure (IOP) level should be stated as part of the definition. Finally, a clinical exam of the optic disc and retina were felt to be needed to rule out non-glaucoma causes of the test findings. The validation of such a new definition is now underway.
This effort is not intended to define clinical entities falling under the term glaucoma, nor is it intended to denote which eyes merit IOP-lowering therapy, nor to provide public policy coding descriptions for national systems that determine reimbursement for care. Rather, the approach is only to provide a definitional basis for comparison between clinical research studies. Hopefully, consensus can be reached on a useful set of parameters for an objective GON definition.
Improved diagnosis and medical treatment will be more important than new surgery
I propose that improvements in diagnostic accuracy and prediction of the future course of glaucoma will have greater impact in glaucoma care than will newer forms of surgery. New developments in ophthalmic surgery have always generated appropriate attention, though the steps and mis-steps in their maturing have been equally dramatic. Phacoemulsification, combined with intraocular lens implantation, may stand as the greatest advance in eye care in the 20th century. Its impact on improved visual function and lower complication rates brought worldwide improvement in visual function over previous cataract surgical methods. However, there were generations of lens implants placed in the anterior chamber or fixated to the iris that were dangerous to the eye and were abandoned after having detrimental effects. The collateral damage of innovation should be minimized by the use of planned and controlled observations in the early stage of new developments
Glaucoma surgical innovation is vitally needed and interest in this area may provide alternative treatment approaches; however, the vast majority of glaucoma patients are now [3] and will be into the foreseeable future cared for by non-surgical monitoring and treatments. Likewise, selective laser trabeculoplasty, while popular, has not significantly decreased the proportion of persons being treated medically or surgically for glaucoma. In fact, eye drop treatment remains the IOP-lowering therapy for most of those with open angle glaucoma (OAG) and for post-iridotomy eyes with angle closure that merit treatment. Issues that need improvement in medical therapy are dominant issues in our practices. The two greatest issues here are: how much should IOP be lowered, and how can we defeat the poor adherence with eye drop use that is so prevalent.
Kill the magic number
We have so far failed to eliminate the incorrect notion that the IOP value 21 mm Hg is meaningful or represents a benchmark for treatment. For 50 years, it has been known that the majority of European- and African-derived persons with OAG have untreated IOP in the range found in their non-glaucoma populations [4]. In some regions of the world (Japan in particular) [5], three fourth or more of those with OAG have IOP in the same range as those who do not have OAG. Yet, studies of clinical behavior in the United States show that ophthalmologists continue to act as if “normalizing” the IOP is meaningful as a treatment goal. In this century, we must realize that the untreated, baseline IOP that is associated with development of GON must be determined in each person and each eye and a reasonable target lowering set and achieved. These facts are independent of the whole issue of central corneal thickness (CCT) and its effect on tonometric IOP measurement. While those with thinner CCT are probably at greater risk to develop GON and to progressively worsen, the absolute IOP is essentially irrelevant. We should not care if the baseline IOP is 30, 20, or 10 mm Hg, as we will use whatever is the baseline to set a target lowering. James Brandt, who identified the fact that thinner CCT is a glaucoma risk factor [6], has urged us NOT to “correct” the IOP [7].
The baseline and target approach
Once we accept the idea that the baseline IOP needs to be assessed, we should avoid beginning therapy on the first visit. To estimate baseline effectively, we must make at least three visits to measure IOP. The average glaucoma patient is treated for two decades [8]. Do we truly wish to base that entire process on one initial IOP value when we know how it can vary from day to day? After the initial discussion about whether to lower IOP with drops, laser angle treatment, or operation, schedule another visit soon with no treatment, and then a third visit. After three measurements to determine a baseline IOP, a unilateral treatment trial of drops can start (or laser angle treatment or surgery be performed). In this way, at least we have three IOP measurements to provide an average baseline value.
Since OAG occurs at any level of IOP, the acceptable amount of IOP lowering needs to be set as the medium term goal for therapy [9]. What we and our patients care about most is their visual function, but that changes only over years in many typical OAG patients, so we need a benchmark for how treatment is succeeding in short and medium time periods. Thus we follow a goal or target IOP. Clearly, if the baseline is 20 mm Hg and eye drop lead to a fall to 18 mm Hg, the effect is too minimal. The goal in the Ocular Hypertension Treatment study was to lower glaucoma suspects by 20% and <21 mm Hg [10], which is a reasonable initial target range for many early OAG eyes. However, the target range was tailored to the degree of glaucoma injury in the Collaborative Initial Glaucoma Treatment Study, extending to 40% lowering for those with severe damage at baseline [11]. The rationale was that there is a greater consequence of further vision loss in those who already have significant injury; hence, a more aggressive target is appropriate.
I believe that starting eye drops in one eye at a time (a unilateral treatment trial) has many advantages. In treating only one eye, the fellow eye can be used as a control for both effectiveness and side effects. While the value of unilateral trials has been both questioned and championed, sometimes by the same author [12], the chief criticism was that two eyes do not perfectly mimic each other in their variability. While not perfectly in synchrony, the correlation between eyes is quite good in their variation up or down over short intervals. Furthermore, two visits in close proximity under unilateral treatment give an excellent idea of the true lowering that is occurring in the treated eye compared to its fellow.
Since the advent of accurate tonometry in the 1950s, we have been aware that our sampling of IOP is far too infrequent—often only 2–4 measurements for a whole year. In internal medicine, devices have been developed to allow patients to sample their blood pressures or their blood sugars daily or even more frequently. Some such devices share the data through the cell phone system to the doctor’s office to provide real-time surveillance. In ophthalmology, three areas of IOP frequent monitoring are either in use or in development. The Triggerfish device is a contact lens worn for 24 h at a time that samples the strain at the limbus each 5 min, sending a signal to a bandage attached to the face and thence to a computer interface. This provides a measure of variation related to IOP that has been linked to the likelihood of progressive change in visual field [13]. It is not practical to wear the device for extended periods, and its exact calibration against IOP level has not been confirmed. Tonometry performed by a family member at home was suggested by Jensen and Maumenee with Schiotz tonometry [14] and has become much more practical with the development of the ICare Home tonometer [15], recently approved by the U.S.F.D.A. While prototypes of an even more powerful tool have been developed, full implementation of an intraocular tonometric sensor that records and transmits IOP in real time awaits development as part of intraocular lens implants placed during cataract surgery. This step would, for the first time, permit large-scale measurement and understanding of the role of IOP in glaucoma. Furthermore, it is easy to see how patients could be kept informed of deviations from the safe range of IOP, including those due to poor adherence with therapy. The software associated with such a device could be monitored in the physician’s office by automated systems that detect periods of unsafe IOP.
Improved adherence by cell phone
The need for ongoing monitoring of IOP control is evidenced by the overwhelming evidence that many patients are poorly adherent with eye drop medication for glaucoma. While patients believe that they are taking 95% of their eye drops, actual electronic monitoring shows that even under ideal conditions they take only 70% [16]. That figure was derived from clinical research studies during which patients knew that they were being monitored and were given medication to use. In the real world, it is likely that the average patient is taking only half of their topical medication. The characteristics of those who are least adherent have been delineated. They are the younger and the older patients among OAG subjects, they are more likely to know little about glaucoma except what they are told in the office, and they tend not to believe that the medication is going to prevent vision loss. A single question that identifies the less adherent is: “I know how hard it is to remember taking medicine every day. Do you think in the last 2 weeks you might have missed taking drops even once or twice?” Poor adherence is so widespread that we have studied what interventions could improve this situation. Among several approaches, the most effective was to use cell-phone-based reminders [17]. There are now free phone “aps” that can give audible alarms to assist patients in remembering their drops. Another approach is an eye drop bottle holder that records squeezing of the bottle and send ongoing patient behavior immediately via the cell phone system to central servers. Again, this could provide immediate feedback to both doctor and patient of inadequate adherence.
Sustained delivery is an answer
A more effective approach to local IOP-lowering therapy is sustained delivery of drugs. A variety of approaches to this area are being tried, including reservoirs attached to the eye, punctal plugs containing medication [18], rings worn on the eye surface that elute drug [19], and depot delivery of medication into the anterior chamber [20] or under the conjunctiva [21]. Some of these are approaching approval for general use, while others are still in animal or early human trials. If patients take only half of their eye drops, then an effective sustained delivery of medication needs to be half as effective at IOP lowering to be non-inferior to drops. Continuous drug delivery is more likely to eliminate fluctuations in IOP that are believed to augment glaucoma damage. Further, there is almost surely lower toxicity, as the preservatives that cause such ocular damage are not needed in most sustained delivery methods. And, the continuous delivery of very low doses of drug would be expected to have fewer general side effects than the massive overdosing and run-off into the nasal mucosa that occurs with eye drops. Microparticles containing standard eye medications have recently been shown to prevent glaucoma damage in animal models with only one delivery subconjunctivally [22]. For the average glaucoma patient, whose disease requires treatment for 20 years, injections or sustained delivery devices would need to be applied about 40 times (i.e., every 6 months for 2 decades). These must have essentially no side effects nor any long-term detrimental effects on the eye or person to be a general replacement for drops. This is an attainable goal but must be equally or more cost effective than existing drop treatments.
Retaining the lost sheep
In performing large-scale identification of those with eye disease in the community, it became evident that the best single question to use in finding a person with glaucoma among senior citizens in Baltimore was to ask: “Have you been told you have glaucoma and dropped out of care?” [23] Indeed, among Americans prescribed initial medication for glaucoma, 23% never filled the second prescription [24], and by the end of 1 year after entry into a free glaucoma management program, 50% of persons had stopped coming. Present glaucoma care is a revolving door that needs to stop. Most evaluations of glaucoma screening programs have concluded that it is simply not a cost effective endeavor. In fact, there are thousands of undiagnosed persons with glaucoma who we could call on the telephone at much lower cost. They are the first degree relatives of existing glaucoma patients. Given the high rate of glaucoma among family members of those with OAG and angle closure glaucoma [25], we called 300 family members of our glaucoma patients to see if they were under observation or care. While most reported that they had had an eye exam within the last year, more than half did not recognize a visual field test when we asked if they had had an exam with a light flashing in a bowl-shaped device and pressed on a button. This suggests that even these high-risk persons are not undergoing annual surveillance that would protect them if they develop the disease. We need to utilize the strengths of on-line databases and social media to assemble and maintain listings from our patients of their family members and to “bug” them to keep up with examinations. Even more important, each office or care organization must assure that persons already diagnosed with glaucoma remain under care. When they drop off the system, we need to identify what factors led to this and to correct them.
Painless glaucoma visits
Clearly, the need to take many hours off from work or leisure to come for examinations for glaucoma care is a serious barrier to effective management. It would be important to modify present exam approaches to make testing and communication easier for patients (and physicians). Ignoring for the moment the issues of how some countries or insurance systems reimburse for care, let us imagine what could be done immediately to develop efficient systems that do a better job for monitoring. Much of the time “wasted” in care is travel to the doctor’s office, which is often in a central city with costs of transport and parking. The major tests that we need for patient monitoring are IOP measurement, optic disc/nerve fiber layer/retinal imaging, and visual field testing. Test facilities could be set up in multiple locations throughout a metropolitan area in partnership with optical shops, pharmacies, and other medical offices. It has been previously shown that experienced patients can perform visual field testing with minimal oversight [26]. We recently showed how straightforward it is to carry out OCT imaging in non-standard locations with modest technical training [27]. Patients can be given the option to learn the outcome of their testing by text or email, or to have a Skype or Facetime discussion with the physician, or when appropriate to have a face-to-face meeting to discuss findings with actual physician examination.
Doing the right spacing of visual field testing
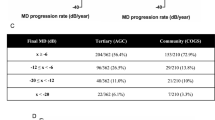
Glaucoma testing has most often been conducted by annual exams with photos/images and with visual fields. Recent large database analysis shows that the vast majority of OAG patients who are under therapy by standard approaches are stable or at the least are worsening at very minimal rates [28]. By contrast, a small proportion are losing function at catastrophically greater rates. The “one size fits all” approach to the initial monitoring of glaucoma patients is inadequate. Even for the more rapidly progressive OAG eyes, testing at once per year means that it will take 5–6 years to determine that the patient is worse [29]—and by then the eye will have lost 10 decibels in mean deviation (a diminution of sensitivity to 10 times worse than normal). A simple solution is to perform 4–6 field tests in the first 18 months of care. Doing so will identify the catastrophic few, who can then undergo more aggressive treatment, while permitting the remaining vast majority to drop back to annual examinations. Even more important would be to improve the overall quality and experience of field testing. The recent development of the IMO instrument by Matsumoto et al. is a potential step in that direction [30]. This device, whose basic test paradigm is similar to present techniques, is a head-mounted display that eliminates the physical conformational issues that confront many older subjects. It requires no patching as the display is shown to both eyes without the subjects awareness of which screen is being illuminated. Eye tracking provides no need to hold the eye still during tests. Even further improvements are needed to find and monitor glaucoma damage. Different targets that specify damage better are needed. Some argue for more testing in the central visual field [31]. And, shorter test times would be welcomed by all.
Reversible nerve damage
OCT imaging has been the greatest improvement in glaucoma diagnosis during the past 20 years, permitting quantification of nerve loss to supplement our quantitative information on functional damage [32]. The changes in the optic disc rim are a combination of both physical configuration changes in connective tissues of the nerve head as well as loss of nerve fibers in the rim. As a result, we have moved to the peripapillary nerve fiber layer and the macular retinal thickness to assess stability. The imaging of blood vessels, called OCT-A, has sparked much interest, but unfortunately this is not a measure of nutritional blood flow but only of the visible presence of the vasculature. While it gives similar information to fluorescein angiography and does so more quickly and safely, studies of OCT-A findings in glaucoma need to be specified as either a preceding cause of nerve loss or more likely as a simple consequence of neural atrophy with secondary capillary downregulation. Ultimately, however, we look toward a biomarker that shows one or more additional features. These would be either an indication of the susceptibility of the posterior eye to glaucoma damage or, even more importantly, a reversible sign of ganglion cell injury prior to cell death. The latter has been the goal of an effort to label dying ganglion cells with annexin V, but it is likely that so few cells are actually dying at any one time and the death process proceeds so rapidly that this will not be the answer [33]. Signaling of axon injury back to the cell body is now known to be carried by the proteins of the kinase systems, particularly dual leucine zipper kinase [34]. We will benefit from the ability to identify the activation of transcription factors or early events in the injury cascade. Such a method would greatly enhance our ability to carry out neuroprotection studies in glaucoma, much as the OCT-based measurement of retinal thickness did for the intravitreal treatments so common now for macular disease.
A second aspect of biomarker identification is to determine methods that show susceptibility to glaucoma injury. Using present OCT imaging of the optic nerve head, we and others have shown that the flexibility of the lamina cribrosa can be measured by imaging at two different IOPs. At a simple level, the anterior border of the lamina is easily seen and now can be detected in an automated algorithm without laborious human marking [35]. Remarkably, if one measures the lamina border after increasing IOP, the expected movement out of the eye (in response to the translaminar pressure gradient) happens in some eyes, but in others the lamina goes the “wrong” way—into the eye at higher IOP. By analyzing which eyes do which movement, we have shown that eyes with early glaucoma, in which stiffening of the peripapillary sclera has not yet occurred, have a widening of the nerve head that pulls the lamina back into the eye at higher IOP. Thus both the amount of movement and its direction are expressions of the state of the nerve head tissues at the heart of glaucoma damage. Further developments in nerve head biomechanics and longitudinal studies that demonstrate their predictive value will be important next steps.
The Emperor’s new surgeries
The search for improvements in glaucoma surgery that occurred in each of the past few decades have accelerated recently. The major new procedures included: in the 1970s, trabeculectomy; in the 1980s tube shunt surgery; and after 2000 the trabectome and Express shunt surgery. The first two have established value and have stood the test of time for eyes failing on medical and laser angle treatment. In the past 15 years, many devices and approaches have been touted, but most have not been objectively or fully evaluated in trials against trabeculectomy. This is despite the claims that these procedures are better or safer. Surgery that is called minimally invasive often has more invasive steps than either trabeculectomy or tube surgery, if one considers entry to the eye for extended periods during viscocanalostomy, 360 degree angle surgery, trabectome, or supraciliary shunt devices. Some devices simply add cost to cataract surgery with no compensatory benefit. Others (IStent) were approved for use in the U.S. with phacoemulsification, but by 2 years postoperatively are not significantly better than phacoemulsification alone. It can be argued that phacoemulsification itself is better than most minimally invasive glaucoma surgeries, giving those with early glaucoma injury a reduction in ocular hypertension that can last for some years. Other touted improvements over existing procedures have not been definitively demonstrated—selective laser trabeculoplasty being a prime example. The most recent example of newness outweighing data-driven change is the micropulse method of diode ciliodestruction, for which no studies have been published that compare it to standard diode application. In contrast, in an impressively designed and implemented study, trabeculectomy has been shown to have advantages over tube shunt surgery in a controlled, randomized clinical trial for eyes without past glaucoma surgery [36]. To be sure, improvements in glaucoma surgery are truly needed and the excitement in the many attempts shows this need. One example of such a potential would be to place an adjustable valve in a tube shunt device, capable of increasing or decreasing flow to lower undesirably high IOP or to stop hypotony due to overfiltration. A rotatable valve responsive to an external magnet would suffice. Further, such a tube shunt could have an IOP-measuring monitor attached to control the valve and at the same time to send the IOP by telemetry to software residing in physicians’ offices.
Moving beyond animals
A great hope for glaucoma treatment is the development of neuroprotection treatments that supplement or even replace IOP lowering. There are multiple pathogenic pathways leading to ganglion cell death that have been shown to be amenable to modification in animal models. Those expecting to find a quick and easy method to demonstrate that animal trials can be converted to human therapy for glaucoma will be frustrated. On the other hand, neuroprotection trials for glaucoma are not impossible and are not more difficult than translational research for stroke, dementia, or Parkinson’s disease [37]. Like Alzheimer’s, glaucoma has a generally slow course, with variable worsening rates among patients. Unlike central nervous system diseases, it is not episodic (like stroke) and we have highly quantitative methods of monitoring progressive change (OCT and fields). Field testing is the present “gold standard” for approval by the F.D.A., and to accommodate its inter-test variability, studies of neuroprotection should recruit those who are known field takers with low variability. They need not be limited to eyes with a high risk for worsening, since recruitment speed is paramount, and generalizability is a desirable feature of any such study. Since we know that IOP lowering is beneficial, all persons in such trials will need to have IOP treatment, so the benefit of neuroprotection must be additive. Side effects must be minimal or none, as the glaucoma patient in general has no active symptoms from the disease itself until late in its course. Adherence with neuroprotection will be minimal if the treatment has noticeable side effects. As with IOP lowering, sustained delivery of a neuroprotective agent would be highly advantageous, both for minimizing treatment effects and maximizing adherence.
In summary, we have effective glaucoma diagnosis and treatment at present that can and hopefully will improve further to prevent loss of vision from the world’s second leading cause of blindness and visual impairment.
References
Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The definition and classification of glaucoma in prevalence surveys. Br J Ophthalmol. 2002;86:238–42.
Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Manag Sci. 1963;9:458–67.
Arora KS, Robin AL, Corcoran KJ, Corcoran SL, Ramulu PY. Use of various glaucoma surgeries and procedures in Medicare beneficiaries from 1994 to 2012. Ophthalmology. 2015;122:1615–24.
Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121:2081–90.
Shiose Y, Kitazawa Y, Tsukahara S, Akamatsu T, Mizokami K, Futa R, et al. Epidemiology of glaucoma in Japan - a nationwide glaucoma survey. Jpn J Ophthalmol. 1991;35:133–55.
Brandt JD, Beiser JA, Kass MA, Gordon MO. Ocular Hypertension Treatment Study (OHTS) Group. Central corneal thickness in the Ocular Hypertension Treatment Study (OHTS). Ophthalmology. 2001;108:1779–88.
Brandt JD. Corneal thickness in glaucoma screening, diagnosis, and management. Curr Opin Ophthalmol. 2004;15:85–89.
Broman AT, Quigley HA, West SK, Katz J, Munoz B, Bandeen-Roche K, et al. Estimating the rate of progressive visual field damage among those with open-angle glaucoma from cross-sectional data. Invest Ophthalmol Vis Sci. 2008;49:66–76.
Jampel HD. Target pressure in glaucoma therapy. J Glaucoma. 1997;6:133–8.
Gordon MO, Kass MA, Ocular Hypertension Treatment Study Group. The Ocular Hypertension Treatment Study: design and baseline description of the participants. Arch Ophthalmol. 1999;117:573–83.
Musch DC, Gillespie BW, Lichter PR, Niziol LM, Janz NK. Visual field progression in the Collaborative Initial Glaucoma Treatment Study: the impact of treatment and other baseline factors. Ophthalmology. 2009;116:200–7.
Realini T, Vickers WR. Symmetry of fellow-eye intraocular pressure responses to topical glaucoma medications. Ophthalmology. 2005;112:599–602.
De Moraes CG, Mansouri K, Liebmann JM, Ritch R, Triggerfish Consortium. Association between 24-hour intraocular pressure monitored with contact lens sensor and visual field progression in older adults with glaucoma. JAMA Ophthalmol 2018. https://doi.org/10.1001/jamaophthalmol.2018.1746.
Jensen AD, Maumenee AE. Home tonometry. Am J Ophthalmol. 1973;76:929–32.
Mudie LI, LaBarre S, Varadaraj V, Karakus S, Onnela J, Munoz B, et al. The Icare HOME (TA022) Study: performance of an intraocular pressure measuring device for self-tonometry by glaucoma patients. Ophthalmology. 2016;123:1675–84.
Friedman DS, Nordstrom BL, Mozaffari E, Quigley HA. Glaucoma management among individuals enrolled in a single comprehensive insurance plan. Ophthalmology. 2005;112:1500–4.
Boland MV, Chang DS, Frazier T, Plyler R, Jefferys JL, Friedman DS. Automated telecommunication-based reminders and adherence with once-daily glaucoma medication dosing: the automated dosing reminder study. JAMA Ophthalmol. 2014;132:845–50.
Varadaraj V, Kahook MY, Ramulu PY, Pitha IF. Patient acceptance of sustained glaucoma treatment strategies. J Glaucoma. 2018;27:328–35.
Brandt JD, DuBiner HB, Benza R, Sall KN, Walker GA, Semba CP, et al. Long-term safety and efficacy of a sustained-release bimatoprost ocular ring. Ophthalmology. 2017;124:1565–6.
Lewis RA, Christie WC, Day DG, Craven ER, Walters T, Bejanian M, et al. Bimatoprost sustained-release implants for glaucoma therapy: 6-month results from a phase I/II clinical trial. Am J Ophthalmol. 2017;175:137–47.
Natarajan JV, Chattopadhyay S, Ang M, Darwitan A, Foo S, Zhen M, et al. Sustained release of an anti-glaucoma drug: demonstration of efficacy of a liposomal formulation in the rabbit eye. PLoS ONE. 2011;6:e24513.
Pitha I, Kimball EC, Oglesby EN, Pease ME, Fu J, Schaub J, et al. Sustained dorzolamide release prevents axonal and retinal ganglion cell loss in a rat model of IOP-glaucoma. Transl Vis Sci Technol. 2018;7:13.
Quigley HA, Park CK, Tracey PA, Pollack IP. Community screening for eye disease by lay persons: the Hoffberger program. Am J Ophthalmol. 2002;133:386–92.
Gurwitz JH, Glynn RJ, Monane M, Everitt DE, Gilden D, Smith N, et al. Treatment for glaucoma: adherence by the elderly. Am J Public Health. 1993;83:711–6.
Kavitha S, Zebardast N, Palaniswamy K, Wojciechowski R, Chan ES, Friedman DS, et al. Family history is a strong risk factor for prevalent angle closure in a South Indian population. Ophthalmology. 2014;121:2091–7.
Van Coevorden RE, Mills RP, Chen YY, Barnebey HS. Continuous visual field test supervision may not always be necessary. Ophthalmology. 1999;106:178–81.
Liu MM, Cho C, Jefferys JL, Quigley HA, Scott AW. Use of optical coherence tomography by nonexpert personnel as a screening approach for glaucoma. J Glaucoma. 2018;27:64–70.
Chauhan BC, Malik R, Shuba LM, Rafuse PE, Nicolela MT, Artes PH. Rates of glaucomatous visual field change in a large clinical population. Invest Ophthalmol Vis Sci. 2014;55:4135–43.
Chauhan BC, Garway-Heath DF, Goñi FJ, Rossetti L, Bengtsson L, Viswanathan B, et al. A. Practical recommendations for measuring rates of visual field change in glaucoma. Br J Ophthalmol. 2008;92:569–73.
Matsumoto C, Yamao S, Nomoto H, Takada S, Okuyama S, Kimura S, et al. Visual field testing with head-mounted perimeter ‘imo’. PLoS ONE. 2016;11:e0161974.
Wu Z, Weng DSD, Rajshekhar R, Thenappan A, Ritch R, Hood DC. Evaluation of a qualitative approach for detecting glaucomatous progression using wide-field optical coherence tomography scans. Transl Vis Sci Technol. 2018;7:5.
Schuman JS, Hee MR, Arya AV, Pedut-Kloizman T, Puliafito CA, Fujimoto JG, et al. Optical coherence tomography: a new tool for glaucoma diagnosis. Curr Opin Ophthalmol. 1995;6:89–95.
Cordeiro MF, Normando EM, Cardoso MJ, Miodragovic S, Jeylani S, Davis BM, et al. Real-time imaging of single neuronal cell apoptosis in patients with glaucoma. Brain. 2017;140:1757–67.
Welsbie DS, Yang Z, Ge Y, Mitchell KL, Zhou X, Martin SE, et al. Functional genomic screening identifies dual leucine zipper kinase as a key mediator of retinal ganglion cell death. Proc Natl Acad Sci USA. 2013;110:4045–50.
Quigley H, Arora K, Idrees S, Solano F, Bedrood S, Lee C, et al. Biomechanical responses of lamina cribrosa to intraocular pressure change assessed by optical coherence tomography in glaucoma eyes. Invest Ophthalmol Vis Sci. 2017;58:2566–77.
Gedde SJ, Feuer WJ, Shi W, Lim KS, Barton K, Goyal S, et al. Treatment outcomes in the Primary Tube Versus Trabeculectomy Study after 1 year of follow-up. Ophthalmology. 2018;125:650–63.
Quigley HA. Clinical trials for glaucoma neuroprotection are not impossible. Curr Opin Ophthalmol. 2012;23:144–54.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
The Optic UK Lecture: Royal College of Ophthalmologists, Liverpool, UK, May, 2018.
Rights and permissions
About this article

Cite this article
Quigley, H.A. 21st century glaucoma care. Eye 33, 254–260 (2019). https://doi.org/10.1038/s41433-018-0227-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-018-0227-8
This article is cited by
-
Clinical outcomes of Ahmed glaucoma valve implantation in primary open-angle glaucoma and pseudoexfoliative glaucoma
International Ophthalmology (2024)
-
Nanotechnology-based ocular drug delivery systems: recent advances and future prospects
Journal of Nanobiotechnology (2023)
-
Astrocytes of the optic nerve exhibit a region-specific and temporally distinct response to elevated intraocular pressure
Molecular Neurodegeneration (2023)
-
„Minimally invasive glaucoma surgery“ – Kammerwinkelbasierte Verfahren im Vergleich
Die Ophthalmologie (2023)
-
Validation of the SITA faster strategy for the management of glaucoma
International Ophthalmology (2022)
