
Abstract
Background
Interscalene nerve blocks provide adequate analgesia, but there are no objective criteria for early assessment of correct catheter placement. In the present study, pulse oximetry technology was used to evaluate changes in the perfusion index (PI) in both blocked and unblocked arms, and changes in the plethysmographic variability index (PVI) were evaluated once mechanical ventilation was instituted.
Methods
The PI and PVI values were assessed using a Radical-7™ finger pulse oximetry device (Masimo Corp., Irvine, CA, USA) in both arms of 30 orthopedic patients who received an interscalene catheter at least 25 min before induction of general anesthesia. Data were evaluated at baseline, on application of local anesthetics; five, ten, and 15 min after onset of interscalene nerve blocks; after induction of general anesthesia; before and after a 500 mL colloid fluid challenge; and five minutes thereafter.
Results
In the 25 patients with successful blocks, the difference between the PI values in the blocked arm and the PI values in the contralateral arm increased within five minutes of the application of the local anesthetics (P < 0.05) and increased progressively until 15 min. After induction of general anesthesia, the PI increased in the unblocked arm while it remained relatively constant in the blocked arm, thus reducing the difference in the PI. A fluid challenge resulted in a decrease in PVI values in both arms.
Conclusion
The perfusion index increases after successful interscalene nerve blockade and may be used as an indicator for successful block placement in awake patients. The PVI values before and after a fluid challenge can be useful to detect changes in preload, and this can be performed in both blocked and unblocked arms. (ClinicalTrials.gov number: NCT 01389011).
Résumé
Contexte
Les blocs nerveux interscaléniquesprocurent une analgésie adéquate, mais il n’existe pas de critères objectifs permettant une évaluation précoce du positionnement du cathéter. Dans cette étude, la technologie de l’oxymétrie de pouls a permis d’évaluer les variations de l’indice de perfusion (IP) dans des membres supérieurs avec ou sans bloc nerveux, ainsi que les variations de l’indice de variabilité pléthysmographique (IVP), une fois la ventilation mécanique installée.
Méthode
Les valeurs de l’IP et de l’IVP ont été évaluées à l’aide d’un oxymètre de pouls digital Radical 7 (Masimo Corp., Irvine, CA, É.-U.) aux deux membres supérieurs de 30 patients orthopédiques qui avaient reçu un cathéter interscaléniqueau moins 25 min avant l’induction de l’anesthésie générale. Les données ont été évaluées au départ, au moment de l’administration des anesthésiques locaux, 5, 10 et 15 min après l’installation du bloc nerveux interscalénique, après l’induction de l’anesthésie générale, avant et après administrationde 500 mLde colloïde, puis après 5 min.
Résultats
Chez les 25 patients ayant des blocs réussis, la différence de valeur de l’IP entre le bras sous bloc et le bras controlatéral a augmenté dans les 5 min suivant l’utilisation des anesthésiques locaux (P < 0,05), puis a continué à augmenter progressivement pendant 15 min. Après l’induction de l’anesthésie générale, l’IP a augmenté dans le bras non soumis à un bloc tandis qu’il restait relativement constant dans le bras ayant le bloc, réduisant ainsi la différence d’IP. L’administration de liquide a provoqué une diminution de la valeur de l’IVP dans les deux bras.
Conclusion
L’indice de perfusion est augmenté en cas de bloc nerveux interscalénique réussi. Il peut servir d’indicateur d’un bloc réussi chez des patients éveillés. Les valeurs de l’IVP avant et après administration de liquide peuvent être utiles pour détecter des variations de la précharge et cela peut être effectué aussi bien dans un bras ayant eu un bloc et dans un bras n’ayant pas eu de bloc. Numéro ClinicalTrials.gov de l’étude : NCT 01389011.
Similar content being viewed by others

Interscalene nerve blocks are effective for intraoperative regional anesthesia and postoperative pain treatment. In shoulder surgery, use of interscalene nerve blocks is common and has been shown more efficient as pain therapy than patient-controlled analgesia with opioids.1 Nevertheless, there is a lack of precise and objective criteria for early evaluation of onset and correct nerve catheter placement. Sensory and motor examination tests are commonly used for assessment.2 While these require patient cooperation, which cannot be expected in all cases (e.g., patients with a history of dementia or sedated patients), a more objective method to determine a successful interscalene nerve block seems to be of added value. A pulse oximeter perfusion index (PI) is an accurate and early indicator of sympathetic blockade after lumbar epidural anesthesia when compared with other clinical diagnostic parameters, such as skin temperature or changes in mean arterial blood pressure.3 The perfusion index can accurately reflect functional sympathetic blockade after interscalene nerve block placement as regional anesthesia induces vasodilatation and increased blood flow.4
The objective of the current study was to assess the influence of interscalene nerve blockade on the PI of the anesthetized arm in comparison with PI values of the contralateral arm, and evaluate its use as an indicator for successful block placement.
This study also investigates the validity of the plethysmographic variability index (PVI) in this setting. In previous studies, the PVI has been labelled a predictor of fluid responsiveness5-7 however, it is unclear whether this parameter can also be used in patients with nerve blocks. It is possible that the application of local anesthetics might result in changes in the state of peripheral perfusion, which could influence the accuracy of PVI to predict changes in preload reliably following volume expansion.8
Methods
Patients
After approval by the Research Ethical Care Committee of the state of Rhineland-Palatinate, Germany [Ref: 837.226.10 (7235); approved on August 18th, 2010] and written informed consent, 30 patients (American Society of Anesthesiologists’ [ASA] physical status I-III) were prospectively studied. All patients were scheduled for surgery of the shoulder or upper arm under general anesthesia combined with interscalene nerve catheter placement. Exclusion criteria included: age < 18 yr or > 80 yr; ASA status IV and V; severe vascular disease; coronary artery disease; arrhythmia; anemia (hemoglobin < 70 g·L−1; infections or deformity of the upper limb; patients in whom a tidal volume of 8 mL·kg−1 body weight cannot be delivered safely; or any contraindication for regional anesthesia.
Anesthesia
This single-centre observational study was performed in the anesthesia holding area and the operating room of orthopedic and trauma surgery of the Johannes Gutenberg-University Medical Center, Mainz, Germany. Patients were studied prior to the surgical procedure. All patients received midazolam 7.5 mg po or lorazepam 1.0 mg po for premedication. Prior to interscalene nerve catheter placement, a venous cannula was placed in the non-anesthetized arm. At baseline, a body-warm balanced crystalloid solution (Sterofundin ISO®, B Braun AG, Melsungen, Germany) was infused at a rate 2 mL·kg−1·hr−1 based on lean body weight. For postoperative pain therapy, all patients received an interscalene nerve catheter under combined ultrasound and nerve stimulation guidance. Patients received up to 2 mg midazolam iv for block placement. Prilocaine 1% (20 mL) and ropivacaine 0.75% (10 mL) were administered through the interscalene nerve catheter with frequent aspiration under ultrasound control. The interscalene block was considered effective when a motor block (inability to elevate arm against gravity) and a sensory block (inability to recognize pinprick on skin of the anesthetized arm) developed within 25 min after application of local anesthetics. General anesthesia was induced after at least 25 min with sufentanil 0.3 μg·kg−1, followed by propofol 2-3 mg·kg−1 and atracurium 0.5 mg·kg−1 or succinylcholine 1.0-1.5 mg·kg−1. The concentration of sevoflurane was adjusted to keep the bispectral index at 40-60 (BIS, Covidien-Nellcor, Boulder, CO, USA and Infinity Delta, Dräger, Lübeck, Germany). The patients’ lungs were ventilated using a volume-controlled mode with a tidal volume of > 8 mL·kg−1 body weight. A positive end-expiratory pressure of at least 5 mmHg was administered.
Peripheral oxygen saturation, heart rate, fraction of inspired and expired oxygen, and sevoflurane, respectively, were continuously monitored (Pallas and Infinity Delta, Dräger, Lübeck, Germany). Noninvasive blood pressure was measured at five-minute intervals. After induction of anesthesia, a fluid challenge consisting of 6% HES 500 mL 130/0.4 (Volulyte®, Fresenius Kabi, Bad Homburg, Germany) was administered.
Measurements
A commercially available noninvasive pulse oximetry monitoring system (Radical-7™, Masimo Corp., Irvine, CA, USA) was used to measure PI and PVI on the middle finger of both hands. Sensors were shielded from ambient light with a manufacturer-specified cover (Masimo Corp., Irvine, CA, USA). The PI and PVI were recorded continuously every two seconds. Data were measured before (baseline) and at zero, five, ten, and 15 min after administration of the local anesthetic mixture; after induction of general anesthesia; at the end of the fluid bolus; and five minutes after the end of the fluid bolus.
The PI value is calculated from pulse oximetry data and is derived from the extent of absorption of red and infrared light. The device measures the variation in light intensity during the cardiac cycle and is an estimate of the variation in arterial blood caused by blood flow. As a marker of peripheral perfusion, the PI is expressed as the ratio of the pulsatile component of light (i.e., the arterial compartment [AC]) to the non-pulsatile component of light (i.e., the direct current [DC] in other tissue) reaching the pulse oximetry sensor, and this value is independent of patient oxygen saturation.9
The PI can be expressed by the following formula: PI = (AC/DC) x 100 [%].10
The value PVI is a noninvasive dynamic variable that reflects fluid status. It is calculated from the changes in PI over one or more complete respiratory cycles in mechanically ventilated patients using the following formula10:
where PImax and PImin are the maximum and minimum PI values observed during a respiratory cycle.
Analysis
Patients with clinically evaluated successful block placement and patients with ineffective blocks were analyzed separately in this study. An interscalene block was defined to be ineffective when supplementary analgesia was needed beyond the protocol during surgery and in the postoperative area. The primary outcome measurement was the difference in PI values between both arms (PI values of anesthetized arm − PI values of non-anesthetized arm) measured five minutes after the application of the local anesthetic through the interscalene catheter.
Statistical analysis
The calculation of our sample size was based on the assumption that a 95% confidence interval for the mean of values should have a length of one standard deviation and a 90% coverage probability. This yielded a sample size of 24 patients. We assumed that there might be a dropout rate of about 20%; therefore, 30 patients were included in this study.
Data were collected using TrendCom software (Masimo Corporation, Irvine, CA, USA). The PI values and the difference in PI values between arms were statistically analyzed at the following times: start of observation and before placement of interscalene nerve catheter (baseline); interscalene application of local anesthetics; five, ten and 15 min after application of local anesthetics; start of invasive ventilation; start and end of the volume bolus; and five minutes after giving a fluid bolus. The PVI values were analyzed after induction of general anesthesia, as PVI is only suitable for mechanically ventilated patients.
Statistical analysis was performed using SAS® 9.3 (2002-2010 SAS Institute Inc., Cary, NC, USA), and we computed the mean and standard deviation for quantitative traits in the sample. In order to describe the changes in PI and PVI under various conditions at different times, we computed the mean, standard deviation, minimum and maximum, median, and quartiles and displayed them in box plots. Further, 95% confidence intervals for the means of PI and PVI were computed assuming normally distributed measurements. The influence of these conditions was assessed using a linear mixed model, thereby taking into account repeated measurements on patients. We considered P values < 0.05 as significant. We adjusted for multiple testing using Tukey-Kramer tests for post hoc comparisons.
Results
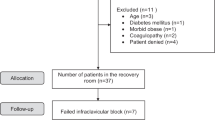
Thirty patients were enrolled in this study, and the mean age of this cohort was 52.1 yr (range: 20-76 yr) (Table 1). Block was deemed unsuccessful in five patients as there was a need for supplementary analgesia beyond the protocol during surgery and during postoperative care. Measurements were analyzed separately for the remaining 25 patients with a successful block. Although data from the five patients with an unsuccessful block are also presented, their small number was insufficient to make statistical comparisons between the successful and unsuccessful blocks. A flow diagram of patients involved in this study is shown in Fig. 1.

Flow chart of the study
Perfusion index
The difference in PI values between the blocked and unblocked arms increased within the first five minutes after application of local anesthetics (P = 0.03 compared with baseline). This effect was even more pronounced after ten (P = 0.0002) and 15 min (P ≤ 0.0001) following induction of regional anesthesia (Fig. 2). At five minutes, absolute values of PI were larger than baseline values in the blocked arm (P = 0.04 compared with baseline), while there was no change in the contralateral arm (P = 0.99 compared with baseline) (Fig. 2).

A: Perfusion index (PI) in an arm where an interscalene block was inserted (anesthetized - light grey) and in the contralateral (non-anesthetized - dark grey) arm; and B: difference in PI values at different time points between blocked and contralateral arms in 25 patients with successful blocks. LA = injection of local anesthetics in the catheter; GA = induction of general anesthesia. Data are presented as box plots (median and interquartile range [IQR]). Whiskers show range or extend to 1.5 times the IQR, whichever is smaller. Outliners are values that differ from the quartiles by > 3 times the IQR (° or +)
In 20 patients with successful blocks (80%), there was an increase in the difference between PI values measured in both arms. Only one of the five patients with an unsuccessful block showed this pattern. Data showing the difference in PI values between arms are in Table 2 (the 25 successful and the five unsuccessful blocks are presented separately).
After induction of general anesthesia, the differences in PI between the arms (Fig. 2) were attenuated because the PI increased in the unblocked arm but not in the blocked arm. Administration of a fluid bolus did not further influence PI values (Fig. 2; P > 0.5 for both arms in comparison with PI values before and five minutes after a fluid bolus).
Plethysmographic variability index
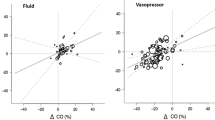
The PVI data were studied in mechanically ventilated patients under general anesthesia. A fluid bolus resulted in a significant decrease in PVI values, both in the arm with an interscalene nerve block in place and in the contralateral arm, and the magnitude of this change was similar in both arms (Fig. 3).

Changes in the plethysmographic variability index (PVI) at different time points in an arm where an interscalene block was inserted (anesthetized - light grey) and in the contralateral (non-anesthetized - dark grey) arm in 25 patients with successful interscalene blocks. LA = injection of local anesthetics in the catheter; GA = induction of general anesthesia. Data are presented as box plots (median and interquartile range [IQR]). Whiskers show range or extend to 1.5 times the IQR, whichever is smaller. Outliners are values that differ from the quartiles by > 3 times the IQR (° or +)
Discussion
We hypothesized that PI values would increase as a result of sympathetic blockade and consecutive vasodilatation produced by the administration of local anesthetic agents through an interscalene nerve catheter. This hypothesis was verified: in the present study, the PI values increased within five minutes of interscalene local anesthetic injection. The PI, a marker of peripheral perfusion, is obtained by calculating the ratio of a pulsating signal (AC) to a non-pulsating signal (DC) and is influenced by vasodilatation. In previous studies, vasodilatation caused by epidural anesthesia increased the pulse oximeter PI.3,11 Therefore, the PI could be a valuable indicator for correct placement of interscalene nerve block. An increase in the difference in PI between both arms (PI blocked arm − PI contralateral arm) was seen in 80% of patients with successful blocks, which can be considered acceptable. Further studies may re-evaluate this aspect.
The laser Doppler peripheral flow index (PFI) is a reliable parameter to predict successful regional anesthesia after axillary or sciatic blocks.4 An increase in PFI went along with an increase in local blood flow and local vasodilatation. The present data show that PI (like PFI) is a sensitive parameter to indicate loss of vasomotor tone induced by local anesthetics. The profile in the PI changes suggests that the parameter can be used as an early indicator (after five minutes) of a sufficient sympathetic blockade.
Skin temperature has been evaluated in some studies as a parameter to indicate the effectiveness of regional anesthesia.12 Skin temperature was found to be a valuable predictor of correct infraclavicular plexus block placement,13 which is consistent with our results of PI measurements in patients with interscalene nerve blocks. On the other hand, another study in 45 patients showed that the increase in skin temperature occurred very late, after loss of sensory and motor functions in patients with interscalene nerve blocks.14 Thus, the PI seems to be a more useful parameter than skin temperature for the evaluation of correct interscalene nerve block placement, as the changes in the PI occur within five minutes after administration of local anesthetics.
After induction of general anesthesia, there was no difference between the PI values of both arms, but the PI values were greater than at baseline. This can be explained by the influence of sevoflurane, which increases blood flow and capillary pressure in muscle tissue,15 resulting in rising PI values in the unblocked arm. Administration of sevoflurane was not associated with an increase in PI values in the blocked arm, probably because vessels were maximally dilated after regional anesthesia.
The PVI values were greater in the unblocked arm than in the blocked arm after induction of anesthesia, but the difference was not statistically significant. A study involving 24 patients investigated the effect of fluctuations in vasomotor tone induced by skin incision on changes in PI and PVI measurements after induction of general anesthesia. The study results showed a negative correlation between changes in PI and PVI.16 This result suggests that sympathetic blockade has an impact on changes of vessel vasomotor tone and consequently on PVI. In the present study, a fluid bolus resulted in a greater decrease in PVI in the unblocked arm than in the blocked arm. Clear threshold discriminant values between responders and non-responders may need to be established by taking peripheral vasodilatation into consideration. This might have important implications for the practicability of PVI in patients with peripheral vasodilatation, e.g., in patients suffering from sepsis or even after administration of a vasodilating agent (like sevoflurane). Nevertheless, PVI decreased as expected after intravascular volume expansion, irrespective of sympathetic blockade. Dynamic parameters of fluid responsiveness, such as PVI, evaluate the response to a cyclic preload variation.17,18 There are controversial findings in the literature about the ability of PVI to predict fluid responsiveness. Studies have shown the usefulness of this noninvasive dynamic parameter in mechanically ventilated patients in the operating room and in the intensive care unit (ICU).6,10,19 Conversely, other studies have concluded that PVI was of limited value in predicting fluid responsiveness in laparoscopic surgery20 and in the ICU setting, respectively.21 Several observations have shown the limitations of this parameter. It seems to be difficult to define a clear threshold value to discriminate between responders and non-responders to a fluid bolus, with variations from 12-17% among the studies and settings being described. The site of measurement has an influence,7 and PVI values also depend on PI values.8,16 The present study confirms these findings; however, regardless of nerve blockade and vasomotor state, the application of a fluid bolus is reflected by a decrease in PVI values in both limbs.
A limitation of the present study is lack of a control group, as there is no real gold standard for the prediction of a successful nerve block. The PI values were not compared with other parameters; the PI values in both arms of the same individual were compared instead. This comparison seems to be more reliable as changes in physiological parameters and the influence of sedatives do not interfere with the results.
In conclusion, the present study reveals that interscalene nerve catheter placement enhances PI values at an early stage. Comparisons in PVI values before and after fluid challenge can be useful to assess changes in preload following volume expansion. In patients with nerve blocks, it should be kept in mind that regional anesthesia may influence absolute PVI measurements. Further studies should revalue these findings.
References
Borgeat A, Schappi B, Biasca N, Gerber C. Patient-controlled analgesia after major shoulder surgery: patient-controlled interscalene analgesia versus patient-controlled analgesia. Anesthesiology 1997; 87: 1343-7.
Spence BC, Beach ML, Gallagher JD, Sites BD. Ultrasound-guided interscalene blocks: understanding where to inject the local anaesthetic. Anaesthesia 2011; 66: 509-14.
Ginosar Y, Weiniger CF, Meroz Y, et al. Pulse oximeter perfusion index as an early indicator of sympathectomy after epidural anesthesia. Acta Anaesthesiol Scand 2009; 53: 1018-26.
Galvin EM, Niehof S, Verbrugge SJ, et al. Peripheral flow index is a reliable and early indicator of regional block success. Anesth Analg 2006; 103: 239-43.
Renner J, Broch O, Gruenewald M, et al. Non-invasive prediction of fluid responsiveness in infants using pleth variability index. Anaesthesia 2011; 66: 582-9.
Loupec T, Nanadoumgar H, Frasca D, et al. Pleth variability index predicts fluid responsiveness in critically ill patients. Crit Care Med 2011; 39: 294-9.
Desgranges FP, Desebbe O, Ghazouani A, et al. Influence of the site of measurement on the ability of plethysmographic variability index to predict fluid responsiveness. Br J Anaesth 2011; 107: 329-35.
Broch O, Bein B, Gruenewald M, et al. Accuracy of the pleth variability index to predict fluid responsiveness depends on the perfusion index. Acta Anaesthesiol Scand 2011; 55: 686-93.
Lima A, Bakker J. Noninvasive monitoring of peripheral perfusion. Intensive Care Med 2005; 31: 1316-26.
Cannesson M, Desebbe O, Rosamel P, et al. Pleth variability index to monitor the respiratory variations in the pulse oximeter plethysmographic waveform amplitude and predict fluid responsiveness in the operating theatre. Br J Anaesth 2008; 101: 200-6.
Ginosar Y, Weiniger CF, Kurz V, Babchenko A, Nitzan M, Davidson E. Sympathectomy-mediated vasodilatation: a randomized concentration ranging study of epidural bupivacaine. Can J Anesth 2009; 56: 213-21.
Stevens MF, Werdehausen R, Hermanns H, Lipfert P. Skin temperature during regional anesthesia of the lower extremity. Anesth Analg 2006; 102: 1247-51.
Minville V, Gendre A, Hirsch J, et al. The efficacy of skin temperature for block assessment after infraclavicular brachial plexus block. Anesth Analg 2009; 108: 1034-6.
Hermanns H, Braun S, Werdehausen R, Werner A, Lipfert P, Stevens MF. Skin temperature after interscalene brachial plexus blockade. Reg Anesth Pain Med 2007; 32: 481-7.
Albertin A, La Colla L, Gandolfi A, et al. Greater peripheral blood flow but less bleeding with propofol versus sevoflurane during spine surgery: a possible physiologic model? Spine (Phila Pa 1976) 2008; 33: 2017-22.
Takeyama M, Matsunaga A, Kakihana Y, Masuda M, Kuniyoshi T, Kanmura Y. Impact of skin incision on the pleth variability index. J Clin Monit Comput 2011; 25: 215-21.
Marik PE, Cavallazzi R, Vasu T, Hirani A. Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic review of the literature. Crit Care Med 2009; 37: 2642-7.
Desebbe O, Cannesson M. Using ventilation-induced plethysmographic variations to optimize patient fluid status. Curr Opin Anaesthesiol 2008; 21: 772-8.
Cannesson M, Delannoy B, Morand A, et al. Does the pleth variability index indicate the respiratory-induced variation in the plethysmogram and arterial pressure waveforms? Anesth Analg 2008; 106: 1189-94.
Hoiseth LO, Hoff IE, Myre K, Landsverk SA, Kirkeboen KA. Dynamic variables of fluid responsiveness during pneumoperitoneum and laparoscopic surgery. Acta Anaesthesiol Scand 2012; 56: 777-86.
Landsverk SA, Hoiseth LO, Kvandal P, Hisdal J, Skare O, Kirkeboen KA. Poor agreement between respiratory variations in pulse oximetry photoplethysmographic waveform amplitude and pulse pressure in intensive care unit patients. Anesthesiology 2008; 109: 849-55.
Acknowledgements
The authors sincerely thank Dr. Maren Baeres, Herbert Guenther, Dr. Annette Hegering, and Dr. Benno Wolcke for their help in conducting the study.
Funding or commercial and non-commercial affiliations: Gunther J. Pestel received unrestricted educational grants from Masimo Corp., Irvine, CA, USA; BMEye, Amsterdam, The Netherlands, and CN Systems, Graz, Austria.
Author information
Authors and Affiliations
Corresponding author
Additional information
Author contributions
Anne Sebastiani is responsible for data analysis and drafting the manuscript. Anne Sebastiani, Larissa Philippi, Stefan Boehme, and Dorothea Closhen are responsible for data acquisition. Anne Sebastiani, Larissa Philippi, Stefan Boehme, Dorothea Closhen, Irene Schmidtmann, Anton Scherhag, Klaus Markstaller, Kristin Engelhard, and Gunther Pestel are responsible for data interpretation and critical revision of the manuscript.
Rights and permissions
About this article
Cite this article
Sebastiani, A., Philippi, L., Boehme, S. et al. Perfusion index and plethysmographic variability index in patients with interscalene nerve catheters. Can J Anesth/J Can Anesth 59, 1095–1101 (2012). https://doi.org/10.1007/s12630-012-9796-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-012-9796-3