
Abstract
Anosmia (loss of smell) and Ageusia (loss of taste) are newly presenting independent symptoms in association with multiple symptoms such as Fever, Dry cough and Breathlessness in COVID 19 Patients.The Study of aims is to estimate Prevalence of Anosmia & Ageusia in Confirmed Covid 19 cases and to assess their Recovery rates. A Study conducted between June 2020 and September 2020 at a tertiary care COVID Dedicated hospital. Total 200 patients with age group 12–70 years Confirmed COVID 19 Positive Patients using RTPCR having mild to moderate symptoms were included. Patients were examined Clinically alongwith all safety measures to analyse prevalence & estimate their recoveries from sensory impairement using 10 item based DyNaCHRON questionnaire(concerned with taste and smell) at 10th, 14th & 21st Day. Out of 200 patients, Prevalence of Isolated Ageusia is 7%, Isolated Anosmia 4.5% and with Anosmia and Ageusia 4%. Complete Recovery regained in Ageusia within 14 days, while Rest all patients of Anosmia and both (Anosmia and Ageusia) within 21 days, Except 2 patients where long term Anosmia persists. Newly onset Anosmia and Ageusia are common in early stages of Covid 19 disease. They are Prevalent in mild to moderate symptomatic form of Diseases. Recovery in most cases is rapid and complete.Early Screening tests performed in suspected COVID 19 patients with loss of taste and smell sensation allows early diagnosis and treatment.
Similar content being viewed by others

Introduction
New Coronavirus Disease 2019 (Covid 19) is a highly contagious Zoonosis named by WHO in February 2020 Caused by SARS-CoV-2 that rapidly transmitted from human to human by respiratory secretions has rapidly evoluted into global pandemic [1,2,3].
SARS-CoV-2 belongs to the coronaviridae family along with SARS-CoV and MERS-CoV. It has a single stranded RNA genome [4]. Four human coronaviruses produce symptoms that are generally mild respiratory illness such as common cold in humans. (i) Human coronavirus OC43 (HCoV-OC43) beta-CoV. (ii) Human coronavirus HKU1(HCoV-HKU1) beta CoV. (iii) Human coronavirus 229E (HCoV-229E) alpha-CoV. (iv) Human coronavirus NL63 (HCoV-NL 63) alpha CoV [5]. Three human coronavirus produce symptoms that are potentially Severe (a) Middle east respiratory syndrome- related coronavirus (MERS-CoV), beta CoV outbreaks began in 2012 [6, 7]. (b) Severe acute respiratory syndrome coronavirus (SARS-CoV) beta Cov which leads to SARS epidemic in 2002–2004 [8, 9]. (c) Severe acute respiratory syndrome coronavirus 2 SARS-CoV-2 Beta CoV Outbreaks 2019–2020 [10].
There was a rapid increase in number of unidentified case of pneumonia in December 2019, detected in Wuhan City, Hubei Province in China [11]. Throat swab samples were taken of such cases Causative Microorganisms was identified at Chinese Centre of Disease Control & Prevention (CCDC) on 7th January 2020 named as Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-Cov-2 [12]. During outbreaks of Covid 19 infections, there are millions of infected people with thousand dead all over world remains a global treat [13].This is the third novel coronavirus in last 17 years and phylogenetically it is close related to bat derived SARS like coronavirus [14].
Covid 19 positive patients characterised by variety of clinical manifestation typically high fever appears after dry cough. Some clinical pneumonitis develops and progress resulting in shortness of breath [15, 16]. According to severe epidemological studies, it could case olfactory and gustatory dysfunction especially mild to moderate form Covid 19 infected cases [17,18,19,20].
Anosmia (loss of smell) and Aguesia (loss of taste) are newly presenting independent symptoms [21] with common symptoms such as fever, dry cough & shortness of breath in COVID 19 + ve cases. They are also associated with muscle ache (myalgia) headache, sore throat, rhinorrhoea, chest pain, diarrhoea, nausea/vomiting, conjunctival, Nasal congestion, Sputum production, fatigue, hemoptysis and chills [22,23,24,25,26].
Some authors reported three mechanisms for anosmia in covid 19 patients; (i) local infection of support cells and vascular pericytes in the nose and olfactory bulb that may affect the function of bipolar neurons or mitral cells. (ii) Damage to support in the sensory epithelium that may indirectly influence the signaling pathway from sensory neurons to the brain and. (iii) Damage to sustentacular cells and bowman gland cells that could leads to diffuse morphological damage to the olfactory sensory epithelium and altering the smell perception [27, 28].
Hu el at studied the cellular distribution of taste cells and ACE 2 Receptor distribution. They found that the percentage of ACE positive cells was higher in taste cells, which indicated that SARS-COV-2 might invade them and leads to ageusia in these patients. However, data regarding the exact mechanism by which SARS-COV-2 determines ageusia is limited. The virus may bind to the sialic acid receptors and occupy and accelerate the degradation of the gustatory particles leading to decrease in taste sensation [29].
Infection of upper respiratory tract can cause acute onset anosmia because of viral damage to olfactory epithelium [30]. Damage to olfactory nerve during invasion and multiplication of SARS-CoV-2 may explain anosmia may be more frequently observed in Covid 19 patients other than respiratory viral infections.
Aguesia may be secondary result of olfactory dysfunction, however angiotension converting enzyme 2 receptors which is main host cell receptor of SARS-CoV-2 for binding & penetrating cells widely expressed on epithelial cells of oral mucosa [31]. Damage of this mucosal epithelial cells may explain ageusia i.e. observed in early stage of COVID 19.The evidence may explain pathogenic mechansim underlying anosmia and ageusia in covid 19 [32].
Since there have been a rapidly growing reports of significant increase in number of patient presenting with loss of smell and taste with or without associated symptoms they also affect quality of life.
For this purpose we decided to assess the prevalence of olfactory and gustatory disorders in infected covid 19 positive patients and to analyze their olfactory and gustatory recovery.
Aims and Purpose
-
To describe the Prevalence and characterize occurrence of subjective olfactory and gustatory dysfunctions in patients with laboratory confirmed COVID 19 infections.
-
Estimate Recovery Rates from sensory disorders with laboratory confirmed COVID 19 infections.
Methods and Materials
A study was conducted between June and September 2020 at tertiary care covid dedicated hospital.
Total 200 patients with age group 12–70 years with laboratory confirmed COVID 19 infections using reverse transcriptase polymerase chain reaction (RT-PCR)Positive having mild to moderate (SpO2 > 95%) symptoms were included in study.
Mild symptoms from only low grade fever, mild cough and slight fatigue with moderate symptoms from high grade fever, shortness of breath upto pneumonitis seen in chest radiograph.
Patients with confirmed RT-PCR positive testing for the SARS-CoV-2 viral genome were assessed for symptoms and signs of olfactory and taste disturbance.
A study conducted smell and taste sensations clinically along with phone interview to analyse the prevalence and estimate recovery Using a 10 item based DyNaCHRON (Dysfonctionnement Nasal Chronique = Chronic Nasal dysfunction) questionnarrie (concerned with taste and smell) on 10th, 14th and later 21st day. (Table 1). Patient tested For smell sensation with Spirit, Rose water, while for taste sensation with Jaggery, salt, lemon etc.
Recovery at Day 10, 14 & 21; Score between 0–5 and 100-Complete Recovery, Score between 5 and 1st score obtained at day 10 out of 100-Partial Recovery, Score equal or Superior to 1st score obtained at day 10 out of 100-No Recovery.
Ethical committee clearance were taken.
A written informed consent were taken from all patients to be part of the study.
Data were recorded in excel sheet and analyzed.
Inclusion Criteria
-
Patients with laboratory confirmed COVID19 infection using Reverse transcriptase polymerase chain reaction (RT-PCR).
-
Age group between 12 and 70 years.
-
Both sexes are included.
-
Patients clinically stable and having Mild to moderate symptoms able to complete the questionnaire.
Exclusion Criteria
-
Age < 12 & > 70 yrs years old.
-
Not confirmed positive RTPCR test result.
-
Patients with Previous history of loss of smell, taste or both before the study.
-
Patients with Previous history of head trauma, acute or chronic rhinosinusitis, allergic rhinitis, dementia, malignancy or abnormal nasal anatomy.
-
Severe Respiratory failure/symptoms or treatment in the Intensive care unit having SpO2 below 95% at time of study.
-
Psycological disturbances
-
Those who lost to follow up (not responding to 3 telephonic call).
Results
In our study, 200 COVID 19 patients with RTPCR positive test with mild & moderate symptoms, the Pevalence rate of Anosmia,Ageusia and combined symptoms were evaluated comprising 109 Males and 91 Females within age group of 12–70 years.
54.5% Males are commonly affected with Chemosensory dysfunction than 45.5% Females (Fig. 1). Males are frequently affected with Ansomia (67%) more than Ageusia (57%) as shown in (Fig. 2).

Showing Gender distribution of patient studied

Gender distribution in COVID 19 positive patients related to Chemosensory Dysfunction
Maximum age group commonly affected 31–40 years which is 35.5%,so younger individuals are affected (Fig. 3).

Age distribution amongst COVID 19 Patient studied
29% patients with Chemosensory dysfunction were associated with Comorbidites. Amongst them Anosmia (33%) are highly affected with comorbidites than Ageusia (28.75%) and combined symptoms (25%).Hypertension (44%) and Diabetes (33%) are higher comorbidites (Table 2).
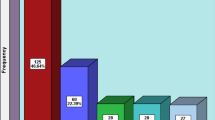
So Prevalence rate of Ageusia is 7% Anosmia 4.5% and Both (Anosmia and Ageusia) 4%. (Fig. 4), while comparison studies are shown in (Table 3).

Prevalence Rate of Isolated Anosmia, Isolated Ageusia and Anosmia & Ageusia in Confirmed COVID 19 positive Patients
Recoveries from sensory dysfunction at 10th, 14th and 21st day Complete recovery obtained Ageusia within 14 days (2 weeks), while Rest all patients of Anosmia and combined symptoms Complete recovery obtained within 21 days (3 weeks) except 2 patients where long term Anosmia persists (Table 4).
Discussion
COVID-19 manifests with wide clinical spectrum ranges from no symptoms to septic shock and multi organ dysfunctions.
Chemosensory dysfunctions are known to be common problems during the COVID-19 pandemic. Olfactory and Gustatory Dysfunction (OGD) along with other classical COVID 19 symptoms such as fever, cough and sore throat were experienced by 31 patients (15.5%) out of 200 patients. Amongst them, 13 patients (42%) experienced OGD before presentation, while 18 patients (58%) had only OGD at the time of presentation with other classic COVID 19 symptoms. Therefore these disorders are indicators of early cases of COVID 19 diseases and necessary for screening and infection control.
Our study design includes Questionaairre about loss of smell and taste clinically on 10th, 14th and 21st day. During hospital stay we analyze improvement of symptoms in patients treated with Antibiotics, T. Cetrizine, Multivitamin and Multiminerals, T. zinc, Steam inhalation and Nasal saline drops. As per protocol after Covid 19 negative report at the end of 14th day patients gets discharged. Later follow up was done on 21st day.
Complete recovery obtained in Majority of patients with Ageusia, Anosmia and both within 14–21 days due to medications while 2 patients have Persistance Sensory dysfunction after 21st day are referred to specialist of smell and taste clinics for rehabiliatation.
According to Study conducted by Harvard medical school for covid 19 suggest that viral load is a key factor to determine if covid patients is more susceptible to long term anosmia, when SARS-CoV-2 invades cells, it causes inflammation that knocks out sense of smell.so recovery time is related to how long the surrounding cells will take time to heal depending on supply of stem cell within nose lining.
In a study conducted by Sakalli et al. (June 2020),out of 172 patients, mean age 37.8 ± 12 years with range of 18–65 years, 51.2% were females. The most prevalent comorbidities in these patients were allergic rhinitis in 8%, high blood pressure in 5%, depression in 4% asthma in 3%, diabetes in 3%, renal disease in 2% thyroid disease in 2%, heart problems in 2% & autoimmune disease in 2%. Sakalli [33].
A study published by Lechien et al. (March 2020) total 417 patients, mean age of patients was 36.9 ± 11.4 years (range 19–77). There were 263 females and 154 males.The most prevalent comorbidities of patients were allergic rhinitis, asthma, high blood pressure and hypothyroidism [34].
In a study conducted by Shah et al. [35] (April–August 2020) by a Total 655 patients, mean age was 32.7 ± 10.1 years with a range of 19–85 years. In their study, 414 (63.20%) patients were males and 241 (36.80%) were females. Hypertension (15.79%) and hypothyroidism (10.52%) were most frequent comorbidities in patients. Males have greater predisposition to olfactory dysfunction because they have higher livelihood of exposure to harmful agents.in adddition estrogen and progesterone might have favourable impacts in peripheral or central olfactory region stem cells that could delay olfactory decline in women [36, 37] moreover neural function has propensity to diminish more rapidly in mens as compared to womens [38, 39].
In our study, out of 200 patients, mean age is 30 ± 5 years with range of 12–70 years. In our study, 109 (54.5%) patients were males and 91(45.5%) patients were females. Hypertension (44%) and Diabetes (33%) were most frequent comorbidities in patients.
A study published by lechien et al. (2020) described short term, olfactory rates complete recovery rate of 59 (44%) patients within 5–8 days following resolution of general symptoms.in total 72.6% of these patients recovered olfactory functions within first 8 days following resolution of the diseases.
In a study conducted by Sakalli E et al., (2020) Recovery status of loss of smell.Total 69 (78.4%) patients with 16 (18.2%) patients showing mild recovery,33 (37.5%) patients showing moderate recovery & 20 (22.7%) patients showing complete recovery. Recovery status of loss of taste total of 63 (77.8%) patients with 17 (21%) patients showing mild recovery, 27 (33.33%) patients showing moderate recovery and 19 (23.4%) patients showing complete recovery.
In our study, patients were followed up at end of 10th, 14th day & later on 21st day for improvement of symptoms. Out of 14 patients Loss of taste sensation,
10 patients (71.42%) recovered spontaneously at end of 10th day, remaining 4 patients regained their sensations after 14st day. Out of 9 patients with loss of smell sensation, 5 patients (55.55%) recovered spontaneously at end of 10th day, remaining 1 patients (11.11%) regained their sensation after 14th day and 1 patient (11.11%) at end of 21st day. Out of 8 patients with loss of both (smell & taste sensation), 5 patients (62.5%) recovered spontaneously at end of 10th day, while remaining 1 patients (12.5%) regained their sensation after 14th day while 1 patient regained sensations completely at end of 21st day while 2 patients did not regain their sense after 21st days too.
For Early Recovery of taste bud stimulation and smell stimulation with rose water and lemon. Olfactory and gustatory neurons have capability to regenerate with daily twice sniffing of rose water and lemon taste.
The pathophysiology of loss of smell developing after infection with this virus has been suggested to be due to olfactory epithelial damage or due to spread to central nervous system.The behaviour of SARS-CoV-2 is different in different patients. This prevents suspicion of diseases clinically delay diagnosis and isolation of patients infected with virus making it difficult to deal with the diseases.
Though the mechanisms for the smell and taste loss in COVID 19 disease are unclear, we observed that SARS-CoV-2 does cause anosmia and ageusia in infected patients and presents as symptoms alone.
The condition may improve gradually on its own with majority recover spontaneously or may remain same. Consideration of Loss of Smell and taste as part of screening and diagnostic approaches for COVID 19 could improve case detection and further spread of infection in community with early isolation and treatment.
Conclusion
Newly onset anosmia and ageusia are common in early stages of Covid 19 disease affecting more commonly in younger Males.
Anosmia and Ageusia are prevalent in mild to moderate symptomatic form of Diseases.
Anosmia are highly affected with comorbidites than ageusia with higher comorbidities as hypertension and Diabetes.
Recovery in most cases are rapid and complete.
First recovery of smell and taste sensation is improved in patients with Regular Rose water inhalation and use of lemon So it is advised.
Early Screening tests performed in suspected COVID 19 patients with loss of taste and smell sensation allows early diagnosis and treatment.
References
Xu X-W, Wu X-X, Jiang X-G et al (2020) Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series. BMJ 368:m606
Chen N, Zhou M, Dong X et al (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223):507–513
Zhai P, Ding Y, Wu X, Long J, Zhong Y, Li Y (2020) The epidemiology, diagnosis and treatment of COVID-19. Int J Antimicrob Agents 55(5):105955
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, Zhang W, Si HR, Zhu Y, Li B, Huang CL et al (2020) A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579:270–273. https://doi.org/10.1038/s41586-020-2012-7
King A (2020) An uncommon cold. New Sci 246(3280):32–35. https://doi.org/10.1016/S0262-4079(20)30862-9
Doucleef M (2012). Scientists Go Deep On Genes Of SARS-Like Virus. Associated Press. Archived from the original on 2012–09–27. Retrieved 2012–09–27.
Falco M (2012). New SARS-like virus poses medical mystery. CNN Health. Archived from the original on 2013–11–01. Retrieved 2013–03–16.
Pasley, James. How SARS terrified the world in 2003, infecting more than 8,000 people and killing 774. Business Insider. Retrieved 2020–11–08
Li F, Li W, Farzan M, Harrison SC (2005) Structure of SARS coronavirus spike receptor-binding domain complexed with receptor. Science 309(5742):1864–68. https://doi.org/10.1126/science.1116480
The Editorial Board (2020–01–29). "Is the World Ready for the Coronavirus?—Distrust in science and institutions could be a major problem if the outbreak worsens". The New York Times. Retrieved 2020–01–30.
Lu H, Stratton CW, Tang Y (2020) Outbreak of pneumonia of unknown etiology in Wuhan China: the mystery and the miracle. J Med Virol 92(4):401–402
Organization WH (2020) WHO Director-General’s remarks at the media briefing on 2019-nCoV on 11 February 2020. Internet World Heal Organ 5:1–9
Mahase E (2020) Covid-19: WHO declares pandemic because of ‘alarming levels’ of spread, severity, and inaction. Br Med J Publ Group 6:3–10
Lu R, Zhao X, Li J et al (2020) Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet 395(10224):565–574. https://doi.org/10.1016/S0140-6736(20)30251-8
Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H et al (2020) Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 8(5):475–481
Novel Coronavirus Pneumonia Emergency Response Epidemiology Team (2020) The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi 41(2):145–151
Mao L, Wang M, Chen S et al (2020) Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. JAMA Neurol 77(6):683–690. https://doi.org/10.1001/jamaneurol.2020.1127
Keyhan SO, Fallahi HR, Cheshmi B (2020) Dysosmia and dysgeusia due to the 2019 Novel Coronavirus; a hypothesis that needs further investigation. Maxillofac Plast Reconstr Surg 42(1):9
Lovato A, de Filippis C, Marioni G (2020) Upper airway symptoms in coronavirus disease 2019 (COVID-19). Am J Otolaryngol 4:102474
Hopkins C, Surda P, Kumar N (2020) Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology 58(3):295–329. https://doi.org/10.4193/Rhin20.11
Tanasa IA, Manciuc C, Carauleanu A, Navolan DB, Bohiltea RE, Nemescu D (2020) Anosmia and ageusia associated with coronavirus infection (COVID-19) - what is known? Exp Ther Med 20(3):2344–2347. https://doi.org/10.3892/etm.2020.8808
Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H et al (2020) Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 8(5):475–481
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y et al (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395(10223):507–513
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX et al (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382(18):1708–1720
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan. China Lancet 395(10223):497–506
Kim ES, Chin BS, Kang CK, Kim NJ, Kang YM, Choi JP et al (2020) Clinical course and outcomes of patients with severe acute respiratory syndrome coronavirus 2 infection: a preliminary report of the first 28 patients from the Korean Cohort Study on COVID-19. J Korean Med Sci 35(13):e142
Plasschaert LW, Žilionis R, Choo-Wing R, Savova V, Knehr J, Roma G, Klein AM, Jaffe AB (2018) A single-cell atlas of the airway epithelium reveals the CFTR-rich pulmonary ionocyte. Nature 560:377–381. https://doi.org/10.1038/s41586-018-0394-6
Bihun CG, Percy DH (1995) Morphologic changes in the nasal cavity associated with sialodacryoadenitis virus infection in the Wistar rat. Vet Pathol 32:1–10. https://doi.org/10.1177/030098589503200101
Pushpass RG, Pellicciotta N, Kelly C, Proctor G, Carpenter GH (2019) Reduced salivary mucin binding and glycosylation in older adults influences taste in an in vitro cell model. Nutrients. https://doi.org/10.3390/nu11102280
Hummel T, Landis BN, Hüttenbrink KB (2011) Smell and taste disorders. GMS Curr Top Otorhinolaryngol Head Neck Surg. https://doi.org/10.3205/cto000077
Xu H, Zhong L, Deng J, Peng J, Dan H, Zeng X et al (2020) High expression of ACE2 receptor of 2019- nCoV on the epithelial cells of oral mucosa. Int J Oral Sci 12(1):8
Cheng HY, Jian SW, Liu DP, Ng TC, Huang WT, Lin HH et al (2020) Contact tracing assessment of COVID-19 transmission dynamics in Taiwan and risk at different exposure periods before and after symptom onset. JAMA Intern Med 180(9):1156–63
Sakalli E, Temirbekov D, Bayri E, Alis EE, Erdurak SC, Bayraktaroglu M (2020) Ear nose throat-related symptoms with a focus Of loss of smell and/or taste in COVID-19 patients. Am J Otolaryngol. https://doi.org/10.1016/j.amjoto.2020.102622
Lechien JR, Chiesa-Estomba CM, De Siati DR et al (2020) Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Ear Arch Otorhinolaryngol 277(8):2251–2261. https://doi.org/10.1007/s00405-020-05965-1
Shah NN, Hussain RT, Mustafa H et al (2020) Evaluation of Olfactory Acuity in Patients with Coronavirus Disease 2019 (COVID-19). Indian J Otolaryngol Head Neck Surg. https://doi.org/10.1007/s12070-020-02241-w
Pawluski JL, Brummelte S, Barha CK, Crozier TM, Galea LA (2009) Effects of steroid hormones on neurogenesis in the hippocampus of the adult female rodent during the estrous cycle, pregnancy, lactation and aging. Front Neuroendocrinol 30(3):343–357. https://doi.org/10.1016/j.yfrne.2009.03.007
Lennington JB, Yang Z, Conover JC (2003) Neural stem cells and the regulation of adult neurogenesis. Reprod Biol Endocrinol. https://doi.org/10.1186/1477-7827-1-99
Lipnicki DM, Sachdev PS, Crawford J et al (2013) Risk factors for late-life cognitive decline and variation with age and sex in the Sydney Memory and Ageing Study. PLoS One. https://doi.org/10.1371/journal.pone.0065841
Doty R, Shaman P, Applebaum S, Giberson R, Siksorski L, Rosenberg L (1984) Smell identification ability: changes with age. Science 226(4681):1441–1443.http://www.jstor.org/stable/1693918. Accessed 15 Sep 2020.
Kartik Irappa Patil, Rukmini M Prabhu, Priya Jose, Harshitha Chandrashekar, B Viswanatha, (2020) Anosmia and Ageusia in Covid-19 Patients. Sch J Otolaryngol, https://doi.org/10.32474/SJO.2020.05.000211
Al-Ani RM, Acharya D (2020) Prevalence of Anosmia and Ageusia in Patients with COVID-19 at a Primary Health Center, Doha, Qatar. Indian J Otolaryngol Head Neck Surg. https://doi.org/10.1007/s12070-020-02064-9
Agyeman AA, Chin KL, Landersdorfer CB, Liew D, Ofori-Asenso R (2020) Smell and taste dysfunction in patients with COVID-19: a systematic review and meta analysis. Mayo Clin Proc 95(8):1621–1631. https://doi.org/10.1016/j.mayocp.2020.05.030
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kandakure, V.T., Valvi, H.R., Khokle, P. et al. Prevalence and Recovery from Newly Onset Anosmia and Ageusia in Covid 19 Patients at our Teritary Care Centre. Indian J Otolaryngol Head Neck Surg 74 (Suppl 2), 3399–3406 (2022). https://doi.org/10.1007/s12070-021-02540-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-021-02540-w