
Abstract
Purpose of Review
The antiphospholipid syndrome (APS) is characterized by the development of thrombotic events and pregnancy morbidity in the presence of antiphospholipid antibodies (aPL). An infectious etiology for this syndrome has been postulated. The present review is aimed to summarize recent evidence about the role of infections and vaccines in the pathogenesis of the APS (including its catastrophic variant).
Recent Findings
There is an increased risk of developing aPL in various infections, particularly in viral infections. The most frequent infection related to aPL has been hepatitis C virus. These antibodies may be associated with thromboembolic events, including catastrophic APS. There is a link between vaccinations, such as the tetanus toxoid and aPL, due to molecular mimicry between the two molecules.
Summary
Accumulated evidence supports that the presence of aPL is associated with a variety of infections, including viruses, bacteria, fungi, and parasites, and the main mechanism to explain this correlation is molecular mimicry. Moreover, a link between vaccinations, such as the tetanus toxoid, and APS has also been described.
Similar content being viewed by others

Introduction
The antiphospholipid syndrome (APS) is a systemic autoimmune disease with persistent elevation of antiphospholipid antibodies (aPL), namely, anticardiolipin antibodies (aCL), lupus anticoagulant (LA), and others, which may result in recurrent thromboembolic events and pregnancy-related morbidity with recurrent fetal losses [1]. The clinical significance of aPL has attracted attention since their discovery in patients with syphilis [2]. False-positive results were seen with other infections [3] and in patients with systemic lupus erythematosus (SLE) and other autoimmune diseases [4]. The disease may be life-threatening with multiple organ failure in about 1% of cases, who develop catastrophic antiphospholipid syndrome (CAPS) [5].
The prevalence of elevated aPL has been reported as 1–5% in young, healthy individuals and 50% in elderly patients with chronic diseases. No clear data are available regarding how many people with elevated aPL may develop antiphospholipid syndrome (APS) [6, 7].
Pathophysiology of aPL Generation During Infections
The aPL bind negatively charged phospholipids, mainly through the β2-glycoprotein I (β2-GPI). The wide heterogeneity of aPL has been a challenge for diagnostic tests and for the elucidation of the pathophysiologic mechanisms of the disease. The molecular pathogenesis of APS is complex, and environmental triggers may play a crucial role in genetically predisposed individuals. APS may occur in association with an infection or malignancy, or may be induced by some drugs (e.g., interferon-alpha) [8].
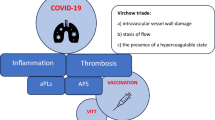
There are several mechanisms through which pathogens can initiate or perpetuate autoimmunity, and while the factors causing the production of aPL remain undefined, there is evidence that molecular mimicry is one mechanism through which experimental APS may occur in association with some pathogens. The clinical observation that thrombosis is observed only occasionally, despite the persistent presence of aPL, suggests that the procoagulant state induced by aPL (“first hit”) only leads to thrombotic events when there is an inciting factor (“second hit”) such as inflammatory responses including infections, malignancies, and other procoagulant conditions in individuals with genetic susceptibility [9]. Infectious agents could trigger aPL, sometimes temporarily, but other times persistently, and lead to thrombosis. It has been suggested that anti-β2GPI antibodies may be generated as a result of molecular mimicry between human β2GPI and molecules similar to β2GPI in invading organisms [9]. It is not clear whether infections plausibly contribute to the postulated first or second hits.
Interpretation of aPL Profile During Infection
It is reported that IgG aCL were more frequently found in patients with hepatitis C virus (HCV) than in controls [9/46 (20%) vs. 2/96 (2%)] [10]. The most frequently detected aPL antibodies in hepatitis B virus (HBV)-infected patients were IgM aCL, and titers were mostly low [11•]. According to a recent systematic review and meta-analysis of observational studies evaluating the risk of elevated aCL antibodies following viral infection, the most prevalent aPL antibodies were aCL (55 studies, 91.7%) and anti-ß2 GPI (19 studies, 31.7%), while LA were tested in eight studies (13.3%). Only four studies tested all three aPL antibodies [12], and most studies reported only one aPL titer. Therefore, the influence of triple positivity on the etiology of viral infections is still unclear [12]. Moreover, no studies have compared the risk of infections according to high or low aCL titers.
Differentiation between pathogenic and non-pathogenic aPL by laboratory techniques is of paramount importance. New assays for the detection of aPL use a variety of approaches: some use traditional ELISA techniques (such as APhL assays, which test for antibodies reactive to a mixture of phospholipids) [13], whereas others use different platforms, which could potentially affect their diagnostic accuracy. A novel line immunoassay (LIA) differentiates between APS and asymptomatic aPL carriers or patients with infectious diseases. The LIA and ELISA have good agreement in detecting aPL in APS, but the LIA differentiates patients with APS from infectious patients and asymptomatic carriers, likely through the exposure of domain 1 [14].
Viral Infections and Antiphospholipid Antibodies
Table 1 shows the main viral infections related to aPL antibodies and APS manifestations. Observational studies have shown that, while aCL occur frequently in viral infections, particularly HIV (49.75%), hepatitis B virus (HBV) (24%), and hepatitis C virus (HCV) (20%), they are very rarely associated with anti-β2GPI antibodies and do not correlate with the risk of thrombosis or the hematological manifestations of APS [15•, 16•]. aPL antibody titers in patients with chronic HCV are lower than those in patients with SLE or APS [17, 18].
Systematic reviews and meta-analysis have evaluated the role of infections, particularly viral infections, on aPL and thromboembolic events. The first included studies in patients with HIV, HCV, and HBV, and the second reported on patients with HCV or HBV [19, 20]. The results showed that HIV and viral hepatitis are significantly associated with aPL positivity and with aPL-related thrombotic complications. In a more recent systematic review and meta-analysis of observational studies that analyzed 73 publications from 60 studies, HIV and HCV were most frequently reported. Compared with healthy controls, patients with HIV were more likely to develop elevated aCL (risk ratio (RR) 10.5, 95% confidence intervals (CI) 5.6–19.4), as were those with HCV (RR 6.3, 95% CI 3.9–10.1), HBV (RR 4.2, 95% CI 1.8–9.5), and Epstein-Barr virus (EBV) (RR 10.9 95% CI 5.4–22.2). The only significantly increased risk for anti-β2GPI antibodies was observed in patients with HCV (RR 4.8 95% CI 1.0–22.3). Compared with patients with SLE, patients with HIV were more likely to develop elevated aCL (RR 1.8, 95% CI 1.3–2.6), and those with EBV elevated anti-β2GPI antibodies (RR 2.2, 95% CI 1.3–3.9) [12]. Therefore, viral infection can increase the risk of developing elevated aPL.
Thromboembolic events have been shown to be more prevalent in patients with elevated aPL who had HCV (9.1%, 95% CI 3.0–18.1) and HBV (5.9%, 95% CI 2.0–11.9) infections, and pregnancy events were the most prevalent in those with parvovirus B19 (16.3%, 95% CI 0.78–45.7), according to a recent systematic review [12]. To quantify the role of aPL in the pathogenesis of clinical events in these patients, the risk in virus-infected patients with or without aPL was evaluated: the only significantly increased risk was observed in patients with HCV (OR 3.4, 95% CI 1.6–7.4) [12]. Only one study from this systematic review evaluated the prevalence of aPL-related clinical events in patients with HCV compared with SLE patients and healthy controls. Pregnancy complications occurred in 5% of HCV patients, and none developed thromboembolic events. In SLE controls, 16% developed venous thrombosis or pregnancy events, while no clinical events were reported in healthy controls [21]. In this systematic review, the role of thromboprophylaxis was not analyzed.
Bacterial Infections and Antiphospholipid Antibodies
aPL have been associated with numerous bacterial infections (Table 2), although they are not usually associated with thrombotic events and anti-β2GPI antibodies. The association with bacterial infections was first recognized in syphilis. In 1979, Cole et al. described, for the first time, a “circulating anticoagulant” in one case of lepromatous leprosy [23]. De Larrañaga et al. found a high prevalence of aPL in leprosy [24]. Streptococcal infections may also be associated with increased aCL titers, mainly IgG isotypes, in acute post-streptococcal glomerulonephritis and streptococcal impetigo without renal involvement [25]. Coxiella burnetii has also been associated with raised aCL titers. Ordi-Ros et al. [18] described a high incidence of IgM and IgG isotypes of aCL and suggested they may aid the diagnosis of Q fever presenting only as fever [26]. A recent observational cross-sectional study at the French National Referral Center for Q fever analyzed 664 patients, of whom 47.1% had positive IgG aCL and 1.9% were diagnosed with thrombosis. Three fulfilled APS criteria. After multiple adjustment, only positive IgG aCL (RR 14.46, 95% CI 1.85–113.14) were independently associated with thrombosis [27]. The authors suggest that aCL should be systematically assessed in acute Q fever patients and hydroxychloroquine should be tested in acute Q fever patients with aCL to prevent aPL-associated complications. Increased IgM and IgG aCL have been detected in patients with cold agglutinins and extrapulmonary complications [28••]. Greco et al. reported the presence of aPL in patients with persistent symptoms of Lyme disease (Borrelia burgdorferi) [29].
APS was proposed as an extra-gastric disease associated with Helicobacter pylori (HP) in 2001 by Cicconi et al. [20], who published the case of a woman in whom APS disappeared after the eradication of an HP infection. There are no additional reports of this finding in the medical literature, most likely because it is not being considered and subsequently not studied. However, APS has been associated with other H. pylori infection-related diseases including primary immune thrombocytopenia, SLE, and central serous chorioretinitis [30, 31].
To date, the evidence supporting a role for HP eradication in the management of APS is too limited to include in routine clinical practice. In addition, even if it may be speculated that eradiating HP might result in the disappearance of aPL, an important clinical question still remains: is aPL negativization enough to change the therapeutic approach in a patient with APS. Recent data suggest that a persistently negative aPL profile is not an indication for the interruption of oral anticoagulant therapy, as patients are still at a high risk of recurrences [32].
According to a recent systematic review of case reports of APS following infections, bacterial infections were reported in 108 patients (36.9%), most commonly secondary to C. burnetii, Mycoplasma pneumonia, streptococci, and Mycobacterium tuberculosis. Most Coxiella cases resulted in the development of antibodies without clinical manifestations for APS, while for the other infections (Mycoplasma, streptococci, and Mycobacterium), the majority of reported cases had APS [22].
Rheumatic fever (RF) is a non-suppurative late autoimmune inflammatory complication of Streptococcus pyogenes infection in the upper airway and remains a public health problem in developing countries. RF and APS share clinical and pathophysiological manifestations, including carditis, chorea, arthritis, and thromboembolic events (mainly stroke). Furthermore, aPL have been related to valve manifestations that are similar in RF and APS, both echocardiographically and pathophysiologically [33]. A systematic review found that the association between APS and RF is quite rare, but is of great clinical importance, and that physicians who deal with RF should include APS in the differential diagnosis, especially in RF patients with stroke whose echocardiogram does not show intracavitary thrombi [34]. Figueroa et al. [35] showed that, during the active phase of RF, 80% of patients had positive aCL, compared with 40% during the inactive phase of the disease. Likewise, Carvalho and Goldenstein-Schainberg [36] simultaneously evaluated the presence of three routinely used aPL (aCL, lupus anticoagulant (LA), and anti-β2GPI) in nine patients with long-term RF (about 11 years). In contrast to other studies, no patient was positive for any of the antibodies.
Parasitic and Fungal Infections and Antiphospholipid Antibodies
Activation of autoimmune mechanisms has been associated with infection with various parasites. Parasitic infections, such as malaria and kala-azar (visceral leishmaniasis) [19] and systemic toxoplasmosis, have been related to APS [37]. APS secondary to acute toxoplasmosis retinochoroiditis has been also described [38]. In patients with kala-azar, the occurrence of aPL was only reported in a single Brazilian study (n = 30), where the reported frequencies of IgG aCL, IgM aCL, and IgG anti-β2GPI were 6, 3, and 53%, respectively [39]. Moreover, the frequent occurrence of aPL in a large series of 103 cases of visceral leishmaniasis has been demonstrated. However, none of the patients with aPL had thrombosis [37]. In a recent systematic review of case reports, parasitic and fungal infections were less common in patients who fulfilled the criteria for definitive APS or those who developed transient aPL with thromboembolic phenomena or patients who developed transient aPL without thromboembolic phenomena; only 12 patients (4.1%) had a parasitic infection and 5 (1.7%) had a fungal infection [22].
Catastrophic Antiphospholipid Syndrome
CAPS is characterized by the simultaneous involvement of multiple organs, with histology demonstrating a myriad of small-vessel occlusions suggestive of a thrombotic storm [40••]. Most of what we know about this condition must be credited to the impressive international “CAPS registry,” managed by the European Forum on Antiphospholipid Antibodies. This collection of clinical data on more than 500 CAPS episodes is reviewed periodically [41, 42]. Consistent with the double-hit hypothesis, nearly two thirds of cases in the CAPS registry are attributed to a clear precipitating factor, including infection (49%), malignancy (17%), and surgery (16%) [42]. The most common infectious precipitant factors are bacteria such as Shigella, E. coli, Klebsiella, Salmonella, Streptococcus, Staphylococcus, and viruses such as HCV and the herpes family [22]. Of the entire cohort, 60 out of 500 (12%) cases were aged ≥ 18 years at the onset of CAPS. Only 9% of cases were in patients aged ≥ 65 years. Infections were significantly the precipitating factor much often described in the childhood (54 vs. 28%), while in elderly patients malignancies were more often reported (33 vs. 8%). Recently, the Chikungunya virus, a single-stranded RNA mosquito-borne alphavirus of the Togaviridae family, has been implicated in some cases of CAPS [43, 44]. In a recent systematic review including 17 patients (5.8%) who fulfilled the most up-to-date CAPS criteria, HCV was the most common infection reported in this group of patients, although nine other viral and bacterial infections were also observed [22].
Molecular mimicry has been suggested as one major mechanism in the interaction between CAPS and infections, based on correlations between the clinical manifestations of CAPS and infectious agents. A strong sequence homology between some proteins in viruses and bacteria and β2-GPI-related peptides has been described [45]. Beyond its role as an initiator, infection is the cause of mortality in 14.1% of CAPS cases, which are attributable to bacterial sepsis, candidiasis, cerebral abscess, or pneumocystis-associated pneumonia [46].
Vaccines and the Antiphospholipid Syndrome
It has been shown that vaccinations such as the tetanus toxoid may trigger antibodies due to molecular mimicry between the two molecules (tetanus toxoid and β2-GPI). The pathogenic potential of anti-tetanus toxoid antibodies cross-reactive with β2-GPI have been shown to be pathogenic in animal models, inducing experimental APS [47, 48].
An association between the human papillomavirus (HPV) vaccine and autoimmunity was suggested following reports of various post-vaccination autoimmune conditions. Homology between amino acid sequences included in the vaccine and the human proteome has been demonstrated. In conjunction with an adjuvant, which accelerates the immune response, it had been believed that the induction of immunity through molecular mimicry culminates in autoimmunity. Recently, a case report described a patient who developed immune thrombocytopenic purpura and concomitant positive aPL following vaccination with a four-valent HPV vaccine [49].
A few reports have suggested that seasonal and pandemic influenza vaccination may induce aPL in inflammatory rheumatic diseases, particularly in SLE patients, but there are no data regarding new-onset thrombosis and the induction of aPL in primary APS patients.
A case-control study evaluated a large panel of aPL following pandemic influenza A/H1N1 non-adjuvant vaccination in primary APS patients and healthy controls in the short and long terms [50]. The authors found that pandemic influenza vaccination in primary APS patients does not trigger short- or long-term thrombosis or significant production of aPL-related antibodies.
It is unclear whether vaccination triggers the development of aPL in SLE. In another elegant study, SLE patients and matched controls received seasonal influenza vaccinations. Sera were tested by ELISA for aCL at baseline, 2, 6, and 12 weeks after vaccination. Patients with positive aCL were further tested for anti-β2GPI antibodies. SLE patients and healthy controls developed new onset aCL post-vaccination (12/101 cases and 7/101 controls, OR 1.81, p = 0.34). New-onset moderate aCL are slightly enriched in African-American SLE patients (5/36 cases; p = 0.094). The optical density (OD) measurements for aCL reactivity were significantly higher than baseline at 2 weeks (p < 0.05), 6 weeks (p < 0.05), and 12 weeks (p < 0.05) post vaccination. No new anti-β2GPI antibodies were detected in patients with new aCL reactivity. The vaccine response did not differ between patients with and without new onset aCL reactivity (p = 0.43). The study showed transient increases in aCL, but not anti-β2GPI responses, after influenza vaccination [51].
Conclusions
Several studies have shown there is an increased risk of developing aPL in various infections, particularly viral infections. Infection-induced aPL have been regarded as transient and were generally not associated with clinical features of APS. Infection-induced aPL have been regarded as transient and were generally not associated with the clinical features of APS. Most aPL are transient. However, in some cases of HCV infection, aPL are persistent and may be associated with thromboembolic events. Clinicians should be aware of clinical features suggestive of APS in patients with viral infections.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4:295–306.
Pangborn MC. A new serologically active phospholipid from beef heart. Proc Soc Exp Biol Med [Internet]. SAGE Publications. 1941;48:484–6. https://doi.org/10.3181/00379727-48-13365P.
Lynch FW, Boynton RE KA. False positive serologic reactions for syphilis: due to smallpox vaccinations (vaccinia). J Am Med Assoc [Internet]. 1941;117:591–595. Available from: doi:https://doi.org/10.1001/jama.1941.02820340013005
Koike T, Sueishi M, Funaki H, Tomioka H, Yoshida S. Anti-phospholipid antibodies and biological false positive serological test for syphilis in patients with systemic lupus erythematosus. Clin Exp Immunol. 1984;56:193–9.
Cervera R, Piette J-C, Font J, Khamashta MA, Shoenfeld Y, Camps MT, et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum. 2002;46:1019–27.
Juby AG, Davis P. Prevalence and disease associations of certain autoantibodies in elderly patients. Clin Invest Med. 1998;21:4–11.
Shi W, Krilis SA, Chong BH, Gordon S, Chesterman CN. Prevalence of lupus anticoagulant and anticardiolipin antibodies in a healthy population. Aust NZ J Med. 1990;20:231–6.
Asherson RA, Cervera R. “Primary”, “secondary” and other variants of the antiphospholipid syndrome. Lupus. 1994;3:293–8.
Shoenfeld Y, Blank M, Cervera R, Font J, Raschi E, Meroni P-L. Infectious origin of the antiphospholipid syndrome. Ann Rheum Dis. 2006. p. 2–6.
Cacoub P, Musset L, Amoura Z, Guilani P, Chabre H, Lunel F, et al. Anticardiolipin, anti-beta2-glycoprotein I, and antinucleosome antibodies in hepatitis C virus infection and mixed cryoglobulinemia. Multivirc Group J Rheumatol. 1997;24:2139–44.
• Huh JY, Yi DY, Hwang SG, Choi JJ, Kang MS. Characterization of antiphospholipid antibodies in chronic hepatitis B infection. Korean J Hematol. 2011, 46:36–40. Article that describes a novel technique that differentiates between antiphospholipid syndrome and asymptomatic antiphospholipid antibody carriers or patients with infectious diseases.
Abdel-Wahab N, Talathi S, Lopez-Olivo MA, Suarez-Almazor ME. Risk of developing antiphospholipid antibodies following viral infection: a systematic review and meta-analysis. Lupus. 2018;27:572–83.
Castanon A, Pierre G, Willis R, Harris EN, Papalardo E, Romay-Penabad Z, et al. Performance evaluation and clinical associations of immunoassays that detect antibodies to negatively charged phospholipids other than Cardiolipin. Am J Clin Pathol. 2018;29:401–11.
Roggenbuck D, Borghi MO, Somma V, Buttner T, Schierack P, Hanack K, et al. Antiphospholipid antibodies detected by line immunoassay differentiate among patients with antiphospholipid syndrome, with infections and asymptomatic carriers. Arthritis Res Ther. 2016;18:111.
• Palomo I, Alarcon M, Sepulveda C, Pereira J, Espinola R, Pierangeli S. Prevalence of antiphospholipid and antiplatelet antibodies in human immunodeficiency virus (HIV)-infected Chilean patients. J Clin Lab Anal. 2003;17:209–15. A systematic review and meta-analysis of articles linking viral hepatitis and antiphospholipid antibodies.
• Brew BJ, Miller J. Human immunodeficiency virus type 1-related transient neurological deficits. Am J Med. 1996, 101:257–61. A systematic review of articles linking viral infection and antiphospholipid antibodies.
Dalekos GN, Kistis KG, Boumba DS, Voulgari P, Zervou EK, Drosos AA, et al. Increased incidence of anti-cardiolipin antibodies in patients with hepatitis C is not associated with aetiopathogenetic link to anti-phospholipid syndrome. Eur J Gastroenterol Hepatol. 2000;12:67–74.
Zachou K, Liaskos C, Christodoulou DK, Kardasi M, Papadamou G, Gatselis N, et al. Anti-cardiolipin antibodies in patients with chronic viral hepatitis are independent of beta2-glycoprotein I cofactor or features of antiphospholipid syndrome. Eur J Clin Investig. 2003;33:161–8.
Sene D, Piette J-C, Cacoub P. Antiphospholipid antibodies, antiphospholipid syndrome and infections. Autoimmun Rev. 2008;7:272–7.
Ambrosino P, Lupoli R, Tarantino P, Di Minno A, Tarantino L, Di Minno MND. Viral hepatitis and anti-phospholipid antibodies positivity: a systematic review and meta-analysis. Dig Liver Dis. 2015;47:478–87.
Alessandri C, Bombardieri M, Di Prospero L, Conigliaro P, Conti F, Labbadia G, et al. Anti-lysobisphosphatidic acid antibodies in patients with antiphospholipid syndrome and systemic lupus erythematosus. Clin Exp Immunol. 2005;140:173–80.
Abdel-Wahab N, Lopez-Olivo MA, Pinto-Patarroyo GP, Suarez-Almazor ME. Systematic review of case reports of antiphospholipid syndrome following infection. Lupus. 2016;25:1520–31.
Cole FS, Brusch JL, Talarico L. A circulating anticoagulant in lepromatous leprosy. Int J Lepr Other Mycobact Dis. 1979;47:121–5.
de Larranaga GF, Forastiero RR, Martinuzzo ME, Carreras LO, Tsariktsian G, Sturno MM, et al. High prevalence of antiphospholipid antibodies in leprosy: evaluation of antigen reactivity. Lupus. 2000;9:594–600.
Ilarraza H, Marquez MF, Alcocer A, Banales JL, Nava AH, Reyes PA. Anticardiolipin antibodies are not associated with rheumatic heart disease. Lupus. 2001;10:873–5.
Ordi-Ros J, Selva-O’Callaghan A, Monegal-Ferran F, Monasterio-Aspiri Y, Juste-Sanchez C, Vilardell-Tarres M. Prevalence, significance, and specificity of antibodies to phospholipids in Q fever. Clin Infect Dis. 1994;18:213–8.
Million M, Bardin N, Bessis S, Nouiakh N, Douliery C, Edouard S, et al. Thrombosis and antiphospholipid antibody syndrome during acute Q fever: a cross-sectional study. Medicine (Baltimore). 2017;96:e7578.
•• Ascer E, Marques M, Gidlund M. M pneumoniae infection, pulmonary thromboembolism and antiphospholipid antibodies. BMJ Case Rep. 2011;pii: bcr1220103561. A systematic review of articles linking viral infections and antiphospholipid antibodies.
Greco TPJ, Conti-Kelly AM, Greco TP. Antiphospholipid antibodies in patients with purported “chronic Lyme disease”. Lupus. 2011;20:1372–7.
Stasi R, Stipa E, Masi M, Oliva F, Sciarra A, Perrotti A, et al. Prevalence and clinical significance of elevated antiphospholipid antibodies in patients with idiopathic thrombocytopenic purpura. Blood. 1994;84:4203–8.
Cotticelli L, Borrelli M, D’Alessio AC, Menzione M, Villani A, Piccolo G, et al. Central serous chorioretinopathy and Helicobacter pylori. Eur J Ophthalmol. 2006;16:274–8.
Medina G, Briones-Garcia E, Cruz-Dominguez MP, Florez-Durante OI, Jara LJ. Antiphospholipid antibodies disappearance in primary antiphospholipid syndrome: thrombosis recurrence. Autoimmun Rev. 2017;16:352–4.
Blank M, Krause I, Magrini L, Spina G, Kalil J, Jacobsen S, et al. Overlapping humoral autoimmunity links rheumatic fever and the antiphospholipid syndrome. Rheumatology (Oxford). 2006;45:833–41.
da Silva F, de Carvalho J. Rheumatic fever associated with antiphospholipid syndrome: systematic review. J Immunol Res. 2014;2014:614591.
Figueroa F, Berrios X, Gutierrez M, Carrion F, Goycolea JP, Riedel I, et al. Anticardiolipin antibodies in acute rheumatic fever. J Rheumatol. 1992;19:1175–80.
de Carvalho JF, Goldenstein-Schainberg C. Lack of antiphospolipid antibodies in long-term cardiac rheumatic fever. Rheumatol. Int. 2012. p. 2951.
Skouri H, Gandouz R, Kraiem I, Harrabi I, Ben SM. Antibodies to anionic phospholipids and cofactors in kala-azar. Comparative study with malaria, toxoplasmosis and “autoimmune diseases”. Clin Exp Rheumatol. 2008;26:894–902.
Tavakoli M, Roghaee S, Soheilian R, Soheilian M. Antiphospholipid syndrome following toxoplasma retinochoroiditis. Ocul Immunol Inflamm. 2011;19:311–3.
Santiago M, Martinelli R, Ko A, Reis EA, Fontes RD, Nascimento EG, et al. Anti-beta2 glycoprotein I and anticardiolipin antibodies in leptospirosis, syphilis and kala-azar. Clin Exp Rheumatol. 2001;19:425–30.
•• Cervera R, Font J, Gomez-Puerta JA, Espinosa G, Cucho M, Bucciarelli S, et al. Validation of the preliminary criteria for the classification of catastrophic antiphospholipid syndrome. Ann Rheum Dis. 2005;64:1205–9. A comprehensive review of the link between infectious diseases and the catastrophic antiphospholipid syndrome.
Cervera R, Rodriguez-Pinto I, Colafrancesco S, Conti F, Valesini G, Rosario C, et al. 14th International Congress on Antiphospholipid Antibodies Task Force Report on Catastrophic Antiphospholipid Syndrome. Autoimmun Rev. 2014. p. 699–707.
Rodriguez-Pinto I, Moitinho M, Santacreu I, Shoenfeld Y, Erkan D, Espinosa G, et al. Catastrophic antiphospholipid syndrome (CAPS): descriptive analysis of 500 patients from the International CAPS Registry. Autoimmun Rev. 2016;15:1120–4.
Betancur J-F, Navarro E-P, Echeverry A, Moncada PA, Canas CA, Tobon GJ. Hyperferritinemic syndrome: Still’s disease and catastrophic antiphospholipid syndrome triggered by fulminant Chikungunya infection: a case report of two patients. Clin Rheumatol. 2015;34:1989–92.
Betancur J-F, Navarro EP, Bravo Bonilla JH, Cortes AD, Velez JD, Echeverry A, et al. Catastrophic antiphospholipid syndrome triggered by fulminant chikungunya infection in a patient with systemic lupus erythematosus. Arthritis Rheumatol (Hoboken, NJ). 2016;68:1044.
Espinosa G, Cervera R, Asherson RA. Catastrophic antiphospholipid syndrome and sepsis. A common link? J Rheumatol. 2007. p. 923–6.
Bucciarelli S, Espinosa G, Cervera R. The CAPS Registry: morbidity and mortality of the catastrophic antiphospholipid syndrome. Lupus. 2009;18:905–12.
Inic-Kanada A, Stojanovic M, Zivkovic I, Kosec D, Micic M, Petrusic V, et al. Murine monoclonal antibody 26 raised against tetanus toxoid cross-reacts with beta2-glycoprotein I: its characteristics and role in molecular mimicry. Am J Reprod Immunol. 2009;61:39–51.
Zivkovic I, Stojanovic M, Petrusic V, Inic-Kanada A, Dimitrijevic L. Induction of APS after TTd hyper-immunization has a different outcome in BALB/c and C57BL/6 mice. Am J Reprod Immunol. 2011;65:492–502.
Bizjak M, Bruck O, Kanduc D, Praprotnik S, Shoenfeld Y. Vaccinations and secondary immune thrombocytopenia with antiphospholipid antibodies by human papillomavirus vaccine. Semin Hematol. 2016;53(Suppl 1):S48–50.
de Medeiros DM, Silva CA, Bueno C, Ribeiro ACM. Viana V dos ST, Carvalho JF, et al. Pandemic influenza immunization in primary antiphospholipid syndrome (PAPS): a trigger to thrombosis and autoantibody production? Lupus. 2014;23:1412–6.
Vista ES, Crowe SR, Thompson LF, Air GM, Robertson JM, Guthridge JM, et al. Influenza vaccination can induce new-onset anticardiolipins but not beta2-glycoprotein-I antibodies among patients with systemic lupus erythematosus. Lupus. 2012;21:168–74.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Antiphospholipid Syndrome
Rights and permissions
About this article

Cite this article
Mendoza-Pinto, C., García-Carrasco, M. & Cervera, R. Role of Infectious Diseases in the Antiphospholipid Syndrome (Including Its Catastrophic Variant). Curr Rheumatol Rep 20, 62 (2018). https://doi.org/10.1007/s11926-018-0773-x
Published:
DOI: https://doi.org/10.1007/s11926-018-0773-x