
Abstract
COVID-19 measures that restrict movement may negatively impact access to HIV care and treatment. To contribute to the currently limited evidence, we used telephone interviews with quantitative and qualitative questions to examine how clients perceived COVID-19 and its effect on their HIV care and ART adherence. One hundred (n = 100) Ugandan adults on ART from an existing study were randomly selected and enrolled. Interviews were recorded, transcribed, and analyzed using descriptive statistics and rapid content analyses. 76% of clients indicated that COVID-19 negatively impacted travel to HIV clinics; 54% perceived that coming to the clinic increased their risk of acquiring COVID-19; and 14% said that COVID-19 had negatively impacted their ART adherence. Qualitative feedback suggests that fear of COVID-19 infection discouraged clinic attendance while stay-at-home orders helped routinize ART adherence and employ new community-based approaches for HIV care. Addressing negative unintended consequences of COVID-19 lockdowns on HIV care is urgently needed.
Similar content being viewed by others


Introduction
Approximately 37.9 million people worldwide are living with HIV [1] and due to existing vulnerabilities, may be at increased risk of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19) [2]. To limit the spread of COVID-19, countries have implemented measures to minimize physical contact between individuals [3]. These “lockdown” measures aim for residents to stay indoors and restrict movement [3, 4]. Yet, they can have unintended consequences on HIV services [3, 4], such as deterring or restricting clinic visits and diagnostic testing, thereby hindering continuation of antiretroviral therapy (ART) in people living with HIV (PLWH) [4, 5]. There is also concern that resources allocated to COVID-19 may reduce HIV spending and diminish HIV care [4,5,6]. As a result, COVID-19 measures are potentially likely to negatively impact HIV treatment services, access to treatment, and adherence. In addition, preliminary data suggest that respiratory complications from COVID-19 occur more rapidly in PLWH [7] who also exhibit delayed antibody responses, although more definitive research is needed [8]. PLWH may perceive facing difficult trade-offs between limiting exposure to one infectious disease while increasing potential negative consequences of another, such as minimizing or avoiding the risk of contracting COVID-19 while obtaining ART refills at HIV clinics [9, 10].
In this paper, we examine how the COVID-19 pandemic and associated lockdown affects access to HIV services and ART adherence in clinic-enrolled PLWH in Uganda to inform programmatic responses. There is little evidence to-date regarding client perspectives on the unintended consequences of the COVID-19 lockdown requirements, including minimized physical contact with others, on their ability to attend HIV clinics and continue ART. We have limited quantifiable data on the prevalence of potential consequences and harms, in addition to little qualitative information on PLWH’s opinions and views. As a result, the dearth of evidence to-date (both quantitative and qualitative) regarding PLWH “lockdown” experiences has hindered local and national efforts to support PLWH in the context of COVID-19. Uganda to-date has had a relatively limited coronavirus pandemic [11]; however, the government is working to prevent a surge of individuals requiring intensive care and ventilation [3, 12]. An uncontrolled COVID-19 epidemic in Uganda could be disastrous given the 1.4 million Ugandan PLWH [13]. On March 25, 2020, the Ugandan President instituted an initial 14-day country-wide lockdown, subsequently extended to mid-May 2020, to “deny large concentrations of people that COVID-19 could infect” [12]. The lockdown closed schools and non-food shops, imposed curfews, and banned public transport across rural and urban Uganda [12]. However, health workers were permitted to continue providing ART services [12]. This study is among the first in sub-Saharan Africa to examine HIV care experiences of PLHW during the COVID-19 pandemic [4, 5, 14].
Methods
Design
Telephone interviews asking about the impact of COVID-19 and associated lockdown were conducted among HIV-positive adults who were enrolled in the currently ongoing randomized controlled trial “Behavioral Economics Incentives to Support HIV Treatment Adherence” (BEST) (clinicaltrials.gov-NCT03494777, Principal Investigator, Sebastian Linnemayr) [15]. We used a randomized, rapid telephone interview design to examine how clients perceived COVID-19 affected their access to HIV care and ART adherence.
Methodological Rationale
Quantitative surveys by telephone are well-established in the literature [16, 17]. Conversely, qualitative telephone interviews have historically been viewed as inferior to quantitative surveys that enumerate patient preferences and, by telephone, have been criticized in comparison to qualitative in-person interviews given the challenges of building rapport and responding to visual cues [18,19,20].
However, increasingly, qualitative telephone interviews are seen as enhancing access to geographically dispersed participants, increasing interviewee privacy, reducing cost, and enriching data collection as interviewees must be explicit in explaining their points of view, not relying on visual cues [18,19,20,21,22,23,24]. Therefore, the methodological rationale of this study aimed to leverage strengths of both quantitative and qualitative telephone interviews, that are particularly appropriate in a time of government measures to minimize physical contact between individuals and restricted out-of-home movement. Specifically, this mixed methods, contactless design enabled the study to: (i) reach clinic-enrolled ART clients who were largely unable to attend in-person research activities at the HIV clinic; (ii) utilize telephone contact in lieu of in-person contact and minimize exposure and transmission of the COVID-19 virus; (iii) obtain quantifiable prevalence measures of the COVID-19 lockdown effects on ART adherence and access to HIV services using pre-coded responses; and (iv) obtain qualitative commentary using documented wording from ART clients themselves regarding their opinions, concerns, and experiences. Given the recency of the COVID-19 pandemic and corresponding lack of previous data as guidance for our quantitative questions, we felt that obtaining this additional qualitative information would allow the participants to report on items we may not have expected but were potentially perceived as important challenges brought about by the pandemic. This embedded, mixed-methods approach therefore enabled us to quantify core domains and understand the frequency of responses, and then expand on the findings by using the qualitative responses to provide important context and nuance [25, 26]. In addition to these reasons, the combination of a mixed methods telephone interview design was additionally prompted by the study’s goals of minimizing costs and enriching new COVID-19-related data collection to respond to the urgent need for empirical evidence on the impact of COVID-19 on HIV care.
Eligibility
Eligibility criteria for the COVID-19 survey were being a participant in the larger parent study (BEST trial, clinicaltrials.gov-NCT03494777) [15], which had inclusion criteria of: age ≥ 18, receiving ART for ≥ 2 years, and having demonstrated adherence problems at the study start, defined as having missed a clinic visit, obtained a late ART drug refill, or lacking viral suppression. The BEST trial uses a randomized clinical trial (RCT) design to test the efficacy of using small incentives based on behavioral economics to support ART adherence for treatment-mature HIV clients. All participants in the parent BEST trial and supplementary COVID-19 telephone surveys were active clients at Mildmay Uganda, a clinic in the capital city of Kampala that specializes in the provision of comprehensive HIV/AIDS prevention, care, and treatment services. Telephone contact information was obtained at trial enrollment and updated at every study visit.
Data Collection
One hundred thirty-six (n = 136) clients were randomly sampled from the master client list of 330 BEST trial participants who were then contacted by phone in random order until we completed 100 surveys. We aimed to survey 100 clients, assuming a non-participation rate of approximately 25%. Each randomly selected client received up to three attempted calls on separate days before being marked as “unreachable”. If phone contact was made, a coordinator confirmed his/her identity and obtained verbal consent. If the respondent was not the client, the coordinator asked when s/he should call again. The clinic or the person’s HIV status was not mentioned to prevent unintended disclosure. Following consent, the coordinator initiated the audio-recording by phone. Once completed, the recording was labeled with the clinic ID and electronically transferred to a secure data storage portal and deleted from the phone. Clients were informed of being paid 20,000 USh (~ $6USD) in cash at their next clinic visit for participation in the telephone survey.
All COVID-19 telephone interviews were conducted by the existing, trained data collectors of the parent BEST trial [15]. Interviews were conducted in English or Luganda depending on the preference of the client, and typically lasted for 20–30 min. Five core topics were examined quantitatively and qualitatively: (1) perceived effects of the COVID-19 lockdown on HIV clinic attendance; (2) perceived COVID-19 exposure at HIV clinic visits; (3) perceived COVID-19 lockdown effects on ART adherence; (4) perceived COVID-19 susceptibility among PLWH; and (5) strategies employed to reduce COVID-19 risk for PLHW and increase resilience. All recordings were translated and transcribed. Twenty percent of the transcripts were checked against the original audio recordings by another team member to ensure transcription accuracy.
Analysis
Using enrollment data from the larger BEST trial [15], we linked survey responses to information on demographics, pre-COVID-19 ART adherence (measured using electronic medication event management system or MEMS caps) and pre-COVID-19 viral load suppression (defined as (< 200 copies/mL)) from laboratory test results, and duration since last clinic visit. These analyses were conducted using Stata version 16. For the qualitative analysis, we used an inductive content analysis appropriate for research with few prior studies to identify themes that emerged from the narrative data within each of the above five previously-structured study topics [27]. To deliver valid and timely findings, we also employed a rapid qualitative assessment process as proposed for health emergencies [28, 29]. This included reducing data collection time by using phones and minimizing time spent on analysis by summarizing transcripts as opposed to more time-consuming electronic coding [30, 31]. One author closely read one third of completed transcripts, extracted exemplary quotations by study topic, and iteratively developed short phrases and memos to represent the interpreted meanings of emergent themes [31, 32]. These themes were then reviewed and refined by four additional co-authors who each closely read the remaining completed transcripts. Quotations illustrating key findings were selected and labeled by age, gender, and time since last ART visit. To understand the predominance of findings relative to others, we also noted whether themes were discussed by a minority or majority of clients.
Results
Quantitative Findings
We present data on the surveys conducted with the first hundred clients (n = 100), which required contacting 136 clients (74% response rate, 1% refusal). The average age of our sample was 37 and over half (60%) were female (Table 1). Nearly half (48%) of our sample had not completed secondary school and most (70%) were employed before the pandemic started. An average of 1.7 months had passed since the last clinic visit that coincides with ART drug refills, usually in 2-month supplies. Average ART adherence was 79% of doses before the pandemic, and 85% of the sample was virally suppressed.
Table 2 shows quantitative survey results. Most participants (76%) agreed or strongly agreed that COVID-19 impacts their ability to come to the clinic and slightly more than half (54%) agreed or strongly agreed that coming to the clinic increased their chances of getting COVID-19. Surprisingly, about two-thirds (69%) of participants said that COVID-19 had not impacted their ability to take their medication and fewer than one-quarter (17%) indicated that it had increased their ability to adhere. Nearly all participants (84%) thought PLWH should take more care to protect themselves from COVID-19, and they indicated several strategies they use to protect themselves. Hand washing (87%) and staying at home (64%) were the most common.
Qualitative Findings
We qualitatively assessed themes within each of the five core study topics. The relative frequencies of emergent themes are summarized in Table 3.
COVID-19 Lockdown Effects on HIV Clinic Attendance
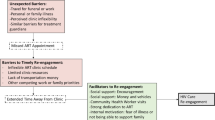
Inability to Continue ART Visits Due to Transport, Violence, and Money
Many clients indicated that COVID-19 negatively impacted their travel to HIV clinics. Lack of transportation, police violence while enforcing the lockdown, and insufficient money for transportation were commonly reported effects of the COVID-19 restrictions on clients’ travel to HIV clinics. For example, one client indicated that given the transportation ban, walking was his only means of getting to the clinic, but the distance was too far. Another client expressed similar challenges to walking to her HIV clinic given concerns of her ability to return in time prior to the curfew and given concerns of being harassed or exposed to violence by police authorities. There were also questions regarding which routes were open for travel or safe to pass. On the other hand, clients who had friends or relatives with private vehicles (that were allowed to travel during the lockdown) were reluctant to use this method due to the risk of unintended disclosure of their HIV status as a result of arriving at the HIV clinic. One client noted additionally the prohibitive costs of private transportation to travel to his HIV clinic.
“…Now am asking myself in which way am I going to move from [home] to come to the clinic? So, there it has impacted on me. It’s one of the things that affects me. It’s still transportation, because now even if you have transport money you can be hindered. Reason being, there is no transportation.” – Age 54, male, last clinic visit 2-3 months ago
“It’s only that they ban public transport. But if I had my own means of transport it can’t hinder me. Yes, it actually hinders me that way. In fact it would be possible for me to walk to the clinic, but there’s curfew. Once they get you walking, they beat you up. So COVID-19 hinders me. In case they find you walking, they ask, ‘Why you are walking? And where you are going?’ In case you have no reason, they beat you up. But I would be willing to walk to the clinic, though returning home would be difficult.” – Age 44, female, last clinic visit 1-2 months ago
“Yes, it impacts on my ability because I don’t have where I can pass. Transportation got paralyzed. So I have no way I can reach the clinic. I have even been worried on how I will be able to get the medication and how will I see you people. I don’t know where the situation will end because the cases are increasing more that’s what I hear.” – Age 57, female, last clinic visit 2-3 months ago
“We were so affected because in some of the programs that were passed by the government like the ban on public transport it didn’t think about people living with HIV who are supposed to go for their medications. So the last option was footing. Yet, now me, I live far. It’s hard for me to walk to the clinic. Then the other thing—as the President passed that directive, he did not put for us any possible means on how to get the drugs. Now as for me who lives 40 km away from that clinic, it’s hard to walk to and from the clinic. Even when I manage to walk, I may fail to manage the return journey. Even when they said that we use boda boda [moped taxi common in Uganda] guy, it’s still expensive.” – Age 25, male, last clinic visit 1-2 months ago
“Personally I can’t walk. And even if someone who has a car is given to me to bring [ART medications], but when I don’t like him…? So, there. I can’t handle…Yes, I don’t want a person knowing my things.” – Age 20, Female, last clinic visit < 1 month ago
Little Impact on Clinic Attendance
A few clients indicated that, while they would worry if COVID-19 restrictions persisted, they had not yet travelled due to having sufficient ART medications for the next month. As one client stated, given his recent ART supply, the COVID-19 lockdown had not affected his HIV clinic attendance. In contrast, a few clients noted that despite the COVID-19 restrictions, they envisioned continuing their travel routine to HIV clinics. As one client described, she was confident in her ability to identify taxi drivers who were infected with COVID-19 based on common cold-like symptoms (i.e., sneezing) in which case she would seek another taxi driver.
“There is no problem. I have not been around [the clinic]. They had given me three months [drug supply], where I am supposed to come back in May.” – Age 49, male, last clinic visit 2-3 months ago
“Because if I use a boda, I am only alone. And so, if they have it, I would not take their motorcycle. Oh you know, if any person sneezes I would just run away. And if they start sneezing, I tell them to stop.”—Age 20, female, last clinic visit < 1 month ago
Expected Limited ART Services
Although not frequently reported, another perceived effect of the COVID-19 lockdown on HIV clinic attendance related to lower quality ART services resulting in stock outages and uncertainty regarding which HIV clinic to attend. As one client detailed, the clinic staff member who answered his phone call was doubtful regarding the availability of ART services during the lockdown and suggested he travel to another, larger HIV clinic. However, upon arrival to the referral HIV clinic, he was unable to acquire his usual three-month prescription due to limited supplies. In response to the COVID-19 lockdown, the client expected having to travel more frequently and for greater distances in order to maintain his ART medications.
“… It was only [the] lock down that brought that problem. Yes, because …on that day I had not woken up early. Maybe I would have walked, but it was already 10 o’clock, and that person that I called seemed like she also did not know about much about what I was talking about. And, that is why, …she said I [should] go to Kawaala. That is where I will be worked on. But then, I was given only one bottle when I got there.” – Age 28, male, last clinic visit > 3 months ago
Perceived COVID-19 Exposure at HIV Clinics
Low Risk Given Clinical Precautions
A key factor in assessing potential effects of the COVID-19 lockdown on ART clients related to their perceptions of potential risks of exposure to the novel coronavirus while receiving HIV care. Our clients reported mixed responses. One point of view indicated confidently that there was minimal to no risk of COVID-19 exposure at HIV clinics given the high level of precautions in place. For example, one woman stated that no clients would be affected at the HIV clinic due to the implementation of fever testing on arrival and social distancing requirements. Another client was also assured that any client infected with COVID-19 would be certainly detected by the HIV clinic given the increased security and scrutiny. As described by a subsequent client, the HIV “hospital” had a track record in providing high quality HIV and non-HIV services, including vaccination, care, and treatment. He felt that this prior service now coupled with hand sanitizers, low-contact protocols, and personal protective equipment resulted in low risk of transmission or acquisition of COVID-19. In general, these clients reported that HIV clinics were “safe” in the context of COVID-19 given heightened use of protective medical equipment and law enforcement personnel.
“I know there are measures at the clinic. Like they have to check you before you enter, and there has to be distance observed at the clinic. So that in case one has come for medication for another person that person may have COVID-19, but with that distance and other measures, no one can be affected.” – Age 26, female, last clinic visit 1-2 months ago
“The hospital is big, and also you come prepared. So if there is anybody who is sick, the hospital has also noticed the person. Since the security is up tight.” - 20, female, last clinic visit < 1 month ago
“Because when I come over to the hospital, I can get vaccinated, and I can easily get good treatment. Because the hospital has availed sanitizers, and there are masks. And since you do not touch surfaces, you will not get the disease.” – Age 19, male, last clinic visit 2-3 months ago
“It is only the transport, but the hospital is safe. What I know the hospital has good machines, so if anybody has it the security would have noticed them already.”—Age 20, female, last clinic visit < 1 month ago
High Risk at Clinic Given Unknown Level of Precautions
A contrasting point of view among many clients was that there was certain and unavoidable increased exposure to COVID-19 to clients who were attending HIV clinics. Such concerns were attributed to multiple factors. For example, as two clients stated below, at any given time, typically small-size HIV clinics were frequented by several clients who may potentially be seated adjacent to each other. Clients commonly expressed not knowing and not being informed regarding what, if any, clinic-based COVID-19 precautions were in place.
“Because it’s not that you are coming alone, or you are the only person who is going to be there. There is going to be other people or contacts, and you never know those who are seated next to you how they are or how they are going to be handling their issues back home. So, you can never know. Well, I do not know the precautions that have been taken at the clinic.” – Age 20, female, last clinic visit 1-2 months ago
“Remember you also have to take caution. Keep distance from other people you find at the clinic. The only challenge is that patients may be many at the clinic, yet [the] space is small. I have not yet known the precautions there.” – Age 40, female, last clinic visit 2-3 months ago.
High Risk Travelling to the Clinic and on Arrival
As one woman described, she was also concerned that, like herself, other ART clients may be exposed to COVID-19 while traveling to the HIV clinic, thereby resulting in potential greater risk to all clients on arrival. In fact, the sentiment that travel to HIV clinics may be the period of highest COVID-19 risk to ART clients, beyond potential exposure risks at the clinic, was commonly stated among clients. As one young man said, safety measures that were implemented at the HIV clinic may be hindered by use of fewer precautions by traveling ART clients.
“It’s because if I have to use public means of transport it exposes me. My association with people on the way. I can’t be sure that at the clinic where I’m coming, [there] are some preventive measures in place to safeguard me.” – Age 37, female, last clinic visit 1–2 months ago
“Because if I travel using public transport, [it] means you can get it on the way, hence affecting people at the clinic too. Then maybe if I don’t get it in transit, I may get it from the clinic like the people you may seat with, and maybe even touching things on and at the clinic. I can’t be safe. I may be safe at the clinic, but on my way to the clinic I may not be safe.” – Age 25, male, last clinic visit 1-2 months ago
Dilemma of HIV vs. Coronavirus Risk
Some clients also described the dilemma in which skipping HIV clinic visits (and thereby not having sufficient ART medication) would increase their susceptibility to complications from AIDS, whereas attending the clinic posed potential infection risk with COVID-19. As one client noted, several efforts were in place to minimize infection due to COVID-19, but there was less attention to increased susceptibility to malaria or influenza among PLWH who were not HIV-virally suppressed. Clients were aware of the dilemma of combatting potential co-infections of COVID-19, malaria, and influenza given concurrently low CD4 counts.
“Not coming to the clinic increases my chances of getting coronavirus because right now you can get malaria and flu. So, it’s through that you can also get coronavirus …because you won’t be getting the [ART] medication. I saw that there is much security that emphasizes on not getting the coronavirus.” – Age 35, female, last clinic visit < 1 month ago
COVID-19 Effects on ART Adherence
Unchanged ART Adherence During COVID-19 Restrictions
As a result of the negative consequences of poor ART adherence, most clients emphasized that nothing would dissuade them from remaining adherent to life-saving ART medications. They referred to their current ART medication habits and a desire to continue living healthily with HIV. As one client stated below, PLWH also hoped that the COVID-19 lockdown would pose only temporary delays and be lifted prior to depleting their ART medications. A few clients also relied on faith-based convictions regarding resumption to normal day-to-day tasks in time. Other clients indicated having increased their personal food stocks to ensure that the lockdown did not lower their ART adherence. In contrast, one client reported experiencing food shortages due to lockdown-related unemployment but remaining determined to incur no changes to her ART medication routine.
“I still take the medicine the same way I was taking it, [and] at the same time. And since it [COVID-19] has not reached me yet. So, I do not get scared because I know life is better than death so let me protect myself in the meantime.” – Age 28, male, last clinic visit > 3 months ago
“Because this situation has found me in a daily routine of taking my medicine and it has not changed me and it will not change me.” – Age 19, male, last clinic visit 2-3 months ago
“I had got my medication for three months, and the three months are getting done by the end of this month. I take the medication like am supposed to. But for this situation, I did put it in my head that this is going to stay for short time, and it will go. And then we go back to the way we used to live, so it has no way it impacts on me. I haven’t changed anything. I live in the same place and eat the same things. Maybe, what I changed was that I stocked food. It’s for a short while, and I see that God will remove it [COVID-19] and it will go.” – Age 50, female, last clinic visit 2-3 months
“Eats are little. You can be there with no food or drinks and remember you would have got them if you had money, but now you don’t. You take. You take it on time. No, I haven’t changed. I try to take even if the situation is bad, but I have to make sure that I take it.” – Age 35, female, last clinic visit < 1 month ago
Lower ART Adherence Due to Coronavirus Restrictions and Stay-at-Home Orders
However, a few clients were unable to maintain their ART medication habits during the lockdown. For example, one woman stated that she had missed doses due to the side effects of having to take ART without food given her lost employment and delayed government rations. Another client expressed that she was experiencing increased difficulty in taking her ART due to greater visibility and stigma among similarly locked-down household members. In particular, she had resorted to taking her ART medications at a different time (or not at all) due to potential unintended HIV disclosure by other household members.
“Now like food, remember you first have to eat and take the medication. But right now, food is budgeted, and we no longer work. When you eat lunch, then it means you won’t eat supper. And remember you have to take the medication twice, so you’ll have to take the medication only once. Now like for me, I take in the morning and evening. So it means…I may have to take it sometimes or not take it. Because I may get what to eat in the morning and fail to get it in the evening. Like last time, I just got tea and took it. But it treated [me] so badly, when I didn’t eat at first. So it showed me that if I do it again then it may cause greater harm on me. Yes, it impacts on my ability somehow.” – Age 30, female, last clinic visit 1-2 months ago
“You leave work at 6 pm whereby you have to take that medication on time like if its 8 pm it has to be 8 pm. And what has caused that is that we take them badly, sometimes at home there are many people and you don’t want them to know so that is what causes the time to change.” – Age 20, female, last clinic visit < 1 month ago
Higher ART Adherence Due to Stay-at-Home Orders
On rare occasions, clients stated that their ART adherence had improved due to the stay-at-home orders, which minimized external distractions. As one man indicated, staying at home had relieved him of prior employment duties and fears of being seen with his ART medications by co-workers. As a result of the lockdown, he was now “free” to take his ART medications without those distractions.
“Actually keeping at home has helped me swallow my drugs on time now that I’m free. But in working days, I had challenges like being busy, and being around people I don’t feel free to swallow the drugs. So I have to first create space, so I can swallow conveniently.” – Age 43, male, last clinic visit < 1 month ago.
Using ART to Prevent COVID-19
Discussions regarding the perceived lockdown effects on ART adherence also encompassed views that ART medications were critical for prevention of AIDS as well as for prevention of infection with COVID-19. In this case, as one client describes, ART adherence was increasingly motivated by its perceived potential to minimize infection and harm from COVID-19.
“It’s because I heard from somewhere that in case COVID-19 finds when your body is weak it affects even more. So if I take my ART medication well, my body will be strong enough in that even when I get COVID-19 I will not be affected as one who doesn’t take their medication.” – Age 26, female, last clinic visit 1-2 months ago
Perceived COVID-19 Susceptibility Among PLWH
Increased Risk of COVID-19 Acquisition, Morbidity and Mortality
The question of perceived greater or lower susceptibility to COVID-19 in PLWH included several diverse perspectives. Most clients believed that PLWH had increased susceptibility to COVID-19 due to their HIV status. For example, one client reported that PLWH, despite ART medications, had weakened immune systems as compared to persons who were not living with HIV. Another two clients added to this sentiment by stating that PLWH and other immune-suppressed individuals had to take more precautions to avoid infection with COVID-19 since they would be less likely to “heal” from the disease. However, clients also revealed that the view was an assumption based on radio and TV campaigns, and not yet confirmed by HIV clinical staff.
“It’s powerful because for me even when they tell us that the viral load is okay, I expect that us who have HIV, our immune system is very low – more than the rest. So, when they talk of a lock up, then we should be the first people to lock up ourselves.” - Age 50, female, last clinic visit 2-3 months ago
“I think a person who is negative, their immunity is kind of stronger to diseases as compared to us. So, you have to take more precaution because if you add another disease it would be difficult. So, I think we are supposed to take more precautions. Yes, like maybe you are already sick and then you add corona virus? I think we would be impacted more than those who are negative.” – Age 20, female, last clinic visit 1-2 months ago
“It’s because I hear that people who have HIV when they contract COVID-19 they don’t heal. So, I decided to be more precautious. I stopped all my movements. No longer visiting people, going to work, etc. In fact, only that my phone got some technical problems. But I was about to call at Mildmay to inquire if that’s true – that people living with HIV don’t heal if they contract COVID-19.” – Age 44, female, last clinic visit 1-2 months ago
“It’s because I heard them teach it on the radio that those with HIV, cancer, diabetes, and other chronic diseases, those ones should take greater care to protect themselves against COVID-19. Because our bodies are weak, and that coronavirus can lower your CD4 count.” – Age 50, female, last clinic visit 2-3 months ago
“I have to take care that I don’t get coronavirus because I know very well what’s between me and my body, and, still, the weakness of my body. So I have to take greater care to protect myself.” – Age 44, male, last clinic visit 2–3 months ago.
Uncertain of Differential Risk of COVID-19 in PLWH
Other clients were less certain regarding differences in susceptibility to COVID-19 between individuals, including between ART-adherent PLWH, ART non-adherent PLWH, and non-PLWH. As one woman stated, although she had been informed that ART was being used to treat COVID-19, ART-adherent clients continued to be susceptible and should utilize necessary precautions. This uncertainty was also characterized by clients who had received competing information from others regarding the impact of COVID-19 on PLWH. As one man stated, he lacked a clear understanding of COVID-19 implications in PLWH due to the range of shared opinions.
“I hear some people say that those ones affected with COVID-19, they give them ART medication. But even then us who are already taking ART medication, it doesn’t guarantee us that we can’t get COVID-19. So we have to still be conscious not to get the coronavirus.” - Age 26, female, last clinic visit 1-2 months ago
“Because the positive person is ever on medicine. But I don’t have a clear idea yet. But some people say that if corona attacks a positive person, it will go into the body easily. Then other people also say that if a positive person is exposed, he is not affected much. So, I don’t really know what is true. Yes, I do not have a clear idea about it.” – Age 52, male, last clinic visit 1-2 months ago
PLWH Better Prepared for Avoiding COVID-19 Acquisition and Complications
Regardless of potential differences in susceptibility to COVID-19 in PLWH, some clients felt that PLWH were better prepared and uniquely positioned to raise awareness of the viral threats from COVID-19 to non-PLWH due to their own lived experience with HIV. Provided ART clients were comfortable in disclosing their HIV status, one woman stated that PLWH “already knew about” and understood the challenges to avoiding viral-related morbidity and mortality. She felt that PLWH could counsel non-PLWH prior to or after COVID-19 infection.
“We should be the ones counselling other people. It’s just that sometimes we don’t want to talk about our status. But even if you don’t have HIV, you can tell them to please protect yourselves. Because this thing we have gone through of AIDS is not easy at all. So, if another disease comes, it’s like we know about it, and we are ready to fight it. But now for these HIV-negative people? They see it as a hard thing. For us, we don’t see any difficulty so long as the doctor tells you what to do. And know you that, if I do it, I will survive. Or, if I don’t do it then I won’t survive. Because we have been with many people.” – Age 50, female, last clinic visit 2-3 months ago
Another view was that PLWH were better prepared to avoid complications from COVID-19 infection due to their established linkages to acute and chronic health care. One man indicated that rather than relying on COVID-19 hotlines, he would travel directly to the HIV clinic given his existing relationships there. He also expected that HIV clinics were better positioned to care for COVID-19-infected PLWH.
“There are phone numbers they gave us to call in case. But these numbers, I hear that even when you call, they don’t receive them. So, if I contracted the COVID-19 virus, I [would] run to the hospital. Most preferably Mildmay because it simplifies everything for me since I’m a known client there, unlike [at] other health centers.” – Age 43, male, last clinic visit < 1 month ago
Concern for Limited COVID-19 Care for Stigmatized PLWH
On rare occasions, clients were also concerned that if infected with COVID-19, they might receive poorer care due to HIV-related stigma. As one young man described, he had overheard that COVID-19-infected PLWH were treated poorly compared to COVID-19-infected individuals who were not living with HIV.
“Because a person with HIV has a different situation compared to a person without it. I have heard that a person with HIV, when he contracts corona, he will be treated very badly compared to a person without HIV.” – Age 19, male, last clinic visit 2-3 months ago
COVID-19 Strategies to Reduce Risk and Increase Resilience
Creative Strategies to Continue HIV Care
Strategies to reduce COVID-19 risk for PLHW and increase resilience included increasing recommended precautions such as handwashing and staying at home. However, clients reported additional, individual measures. For example, one man stated that he had hired a taxi driver to pick up ART medications on his behalf at the HIV clinic. Others sent peers in close geographical proximity to HIV clinics. Another male client noted that he had provisions in place to move-in with relatives or friends to be closer to the HIV clinic, if needed, particularly if he were exposed or co-infected with COVID-19. Lastly, clients also referenced nutrition efforts perceived to increase their immunity against COVID-19. For example, two clients described using herbal remedies such as drinking water with lemons and tea.
“… I can send the boda [moped taxi] guy to pick for me my medication” – Age 54, male, last clinic visit < 1 month ago
“If I learn that I have it then I have to run to the isolation so that I don’t infect my family. I strongly agree with it because now [I] am asking myself in which way am I going to move from [home] to come to the clinic. So there it has impacted on me.” – Age 54, male, last clinic visit 2-3 months ago
“I have been hearing from them people around talking about [COVID-19], and I also hear them on TV. Then, [I] put them into action. Even on WhatsApp, they send us audios saying that we [should] drink a mixture of warm water and lemon.” – Age 21, female, last clinic visit < 1 month ago
“Yes, as a way to protect myself from getting coronavirus…they told us to use lemons so much. So, [I] try buying lemons and put them in drinking water. So that I boost my immunity and not to be able to get that disease.” – Age 21, female, last clinic visit < 1 month ago.
Discussion
This mixed-methods rapid assessment reports results from 100 phone surveys asking about perceptions of the impact of COVID-19 on access to HIV services and ART adherence among HIV-infected adults in Uganda. Our findings underscore several factors rendering HIV clinic access more difficult, such as significant reductions in mobility due to Uganda’s COVID-19 lockdown and curfew. There were mixed responses regarding perceived increased exposure to COVID-19 at HIV clinics, with some clients fearing potential infection on the way to the clinic or while waiting to receive HIV care. Others were confident that the clinic was taking sufficient precautions to avoid infections. Somewhat surprisingly, most respondents indicated that COVID-19 had not led to disruptions in ART adherence, and in fact some reported an increased focus on ART adherence while staying at home without distractions related to work or social engagements. Still, some described missing doses due to the side effects of taking ART without food because of lost employment or delayed government rations. It is important to note that we surveyed clients at a time when most still had ART medications from their previous (i.e. prior to COVID-19) HIV clinic visit, thus it will be important to track whether and how this situation changes as the pandemic continues. Clients also shared their concerns regarding the potential consequences of contracting COVID-19 due to their compromised immune system. Some respondents indicated that this resulted in difficult trade-offs between skipping HIV clinic visits (and thereby not having sufficient ART medication) and risking potential infection with COVID-19 when going to the clinic. Finally, some clients also showed ingenious ways of continuing their HIV care, such as sending moped taxis to the clinic to obtain drug refills or moving in with relatives living close to the clinic.
Our respondents raised some of the same challenges brought about by COVID-19 for PLWH in other settings. For example, a study from China noted that PLWH faced problems getting to the clinic and obtaining drug refills on time [33]. A study among sexual minority men in the U.S. reported disruptions to HIV-related services [34]. A key strength of this study is that it contributes empirical evidence based on mixed-methods to a currently small but hopefully growing literature presenting empirical results of how COVID-19 impacts HIV care, and gives initial insights into the disruptions, perceptions of risk, and opportunities for resilience in a low-income country. It also has limitations, such as being relatively small and from a single HIV clinic in Uganda, though we expect (and see from studies in other settings) that the challenges reported by our participants are not unique to Uganda.
While the world struggles to contain the COVID-19 pandemic, millions of people are living with chronic conditions, such as HIV, that require continuous care. There is increasing concern that the emergency response to COVID-19 may lead to disruptions of non-COVID-19 health issues [35], yet little if any empirical data are available regarding how people living with chronic conditions are reacting and responding to this novel situation. Our results highlight the need to prepare infrastructure and adapt systems facilitating continued care of HIV and other chronic diseases both during the current COVID-19 emergency response, and, more importantly, in the months or years needed to return to a ‘new normal’ in health care. We hope results from this rapid, ‘pulse-taking’ study regarding the perceptions of ART clients contribute to a much-needed evidence base on the impact of COVID-19 on HIV care.
References
Joint United Nations Programme on HIV/AIDS (UNAIDS). Fact sheet: World AIDS Day 2019—global HIV statistics. Dec 1, 2019. https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Accessed 17 Apr 2020.
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Zhang L, Fan G, Xu J, Gu X, Cheng Z, Yu T, Xia J, Wei Y, Wu W, Xie X, Yin W, Li H, Liu M, Xiao Y, Gao H, Guo L, Xie J, Wang G, Jiang R, Gao Z, Jin Q, Wang J, Cao B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. https://doi.org/10.1016/S0140-6736(20)30183-5.
Hargreaves J, Davey C. Group for lessons from pandemic HIV prevention for the COVID-19 response. Three lessons for the COVID-19 response from pandemic HIV. Lancet HIV. 2020;7(5):e309. https://doi.org/10.1016/S2352-3018(20)30110-7.
Adepoju P. Tuberculosis and HIV responses threatened by COVID-19. Lancet HIV. 2020;7(5):e319. https://doi.org/10.1016/S2352-3018(20)30109-0.
Jiang H, Zhou Y, Tang W. Maintaining HIV care during the COVID-19 pandemic. Lancet HIV. 2020;7:e308. https://doi.org/10.1016/S2352-3018(20)30105-3.
Drain PK, Garrett N. SARS-CoV-2 pandemic expanding in sub-Saharan Africa: considerations for COVID-19 in people living with HIV. Clin Med. 2020. https://doi.org/10.1016/j.eclinm.2020.100342.
Chen J, Cheng X, Wang R, Zeng X. Computed tomography imaging of an HIV-infected patient with coronavirus disease 2019 (COVID-19). J Med Virol. 2020. https://doi.org/10.1002/jmv.25879.
Zhao J, Liao X, Wang H, Wei L, Xing M, Liu L, Zhang Z. Early virus clearance and delayed antibody response in a case of COVID-19 with a history of co-infection with HIV-1 and HCV. Clin Infect Dis. 2020. https://doi.org/10.1093/cid/ciaa408.
Lederman MM, Funderburg NT, Sekaly RP, Klatt NR, Hunt PW. Residual immune dysregulation syndrome in treated HIV infection. Adv Immunol. 2013;119:51–83. https://doi.org/10.1016/B978-0-12-407707-2.00002-3.
Shiau S, Krause KD, Valera P, Swaminathan S, Halkitis PN. The burden of COVID-19 in people living with HIV: a syndemic perspective. AIDS Behav. 2020. https://doi.org/10.1007/s10461-020-02871-9.
Coronavirus disease 2019 (COVID-19) Situation Report – 209. World Health Organization (WHO). 16 August 2020. https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200816-covid-19-sitrep-209.pdf?sfvrsn=5dde1ca2_2. Accessed 27 Aug 2020
Yoweri K. Museveni Fourth address on COVID-19. https://www.yowerikmuseveni.com/fourth-address-covid19. Accessed 17 Apr 2020
UNAIDS Country: Uganda. https://www.unaids.org/en/regionscountries/countries/uganda. Accessed 17 Apr 2020
Joseph Davey D, Bekker LG, Coates TJ, Myer L. Contracting HIV or Contracting SAR-CoV-2 (COVID- 19) in pregnancy? Balancing the risks and benefits. AIDS Behav. 2020. https://doi.org/10.1007/s10461-020-02861-x.
Linnemayr S, Stecher C, Saya U, MacCarthy S, Wagner Z, Jennings L, Mukasa B. Behavioral economics incentives to support HIV treatment adherence (BEST): protocol for a randomized controlled trial in Uganda. Trials. 2020;21(1):9. https://doi.org/10.1186/s13063-019-3795-4.
Smith EM. Telephone interviewing in healthcare research: a summary of the evidence. Nurse Res. 2005;12(3):32–41.
Carr ECJ, Worth A. The use of the telephone interview for research. Nursing Times Res. 2001;6:511–24.
Drabble L, Trocki KF, Salcedo B, Walker PC, Korcha RA. Conducting qualitative interviews by telephone: lessons learned from a study of alcohol use among sexual minority and heterosexual women. Qual Soc Work. 2016;15(1):118–33.
Novick G. Is there a bias against telephone interviews in qualitative research? Res Nurs Health. 2008;31(4):391–8.
Irvine A. Duration, dominance and depth in telephone and face-to-face interviews: a comparative exploration. Int J Qual Methods. 2011;10(3):202–20.
Cachia M, Millward L. The telephone medium and semi-structured interviews: a complementary fit. Qual Res Organ Manag. 2011;6(3):265–77.
Musselwhite K, Cuff L, McGregor L, et al. The telephone interview is an effective method of data collection in clinical nursing research: a discussion paper. Int J Nurs Stud. 2007;44(6):1064–70.
Trier-Bieniek A. Framing the telephone interview as a participant-centred tool for qualitative research: a methodological discussion. Qual Res. 2012;12(6):630–44.
Lechuga VM. Exploring culture from a distance: the utility of telephone interviews in qualitative research. Int J Qual Stud Educ (QSE). 2012;25(3):251–68.
Maxwell JA, Loomis DM. Mixed methods design: an alternative approach. In: Tashakkori A, Teddlie C, editors. Handbook of mixed methods in social & behavioral research. Thousand Oaks: Sage; 2003. p. 241–271.
Schoonenboom J, Johnson RB. How to construct a mixed methods research design. Kolner Z Soz Sozpsychol. 2017;69(Suppl 2):107–31. https://doi.org/10.1007/s11577-017-0454-1.
Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–46.
Vindrola-Padros C, Vindrola-Padros B. Quick and dirty? A systematic review of the use of rapid ethnographies in healthcare organization and delivery. BMJ Qual Saf. 2018;27:321.
Johnson GA, Vindrola-Padros C. Rapid qualitative research methods during complex health emergencies: a systematic review of the literature. Soc Sci Med. 2017;189:63–75.
Taylor B, Henshall C, Kenyon S, Litchfield I, Greenfield S. Can rapid approaches to qualitative analysis deliver timely, valid findings to clinical leaders? A mixed methods study comparing rapid and thematic analysis. BMJ Open. 2018;8(10):e019993. https://doi.org/10.1136/bmjopen-2017-019993.
Hsieh H-F, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277–88.
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–15.
Guo W, Weng HL, Bai H, et al. Quick community survey on the impact of COVID-19 outbreak for the healthcare of people living with HIV. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(5):663–7. https://doi.org/10.3760/cma.j.cn112338-20200314-00345.
Sanchez TH, Zlotorzynska M, Rai M, et al. Characterizing the impact of COVID-19 on men who have sex with men across the United States in April, 2020. AIDS Behav. 2020. https://doi.org/10.1007/s10461-020-02894-2.
Grady D. The pandemic’s hidden victims: sick or dying, but not from the virus. New York Times. 2020 April 20. https://www.nytimes.com/2020/04/20/health/treatment-delays-coronavirus.html?action=click&module=Well&pgtype=Homepage§ion=Health. Accessed 24 Apr 2020
Acknowledgements
The authors wish to thank the Mildmay clinic and the Ugandan RAND research staff. We are particularly grateful to our excellent study team members: Peter Wabukala, Lillian Lunkuse, Philip Aroda, and Pius Kimuli. We also extend our gratitude to the ART clients who so generously provided their time and insight to make this study possible.
Funding
This research was funded through resources and services provided by the National Institute of Mental Health (Grant: R01MH110350, PI: Linnemayr). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. Clinical trial registration: ClinicalTrials.gov NCT03494777.
Author information
Authors and Affiliations
Contributions
SL, US, and ZW conceived the study and developed the study protocol. SL, US, and ZW managed study implementation and data collection. SW transcribed the interviews. LJMW coded and initially analyzed the qualitative data and prepared the first draft of the manuscript. SL, LJMW, US, ZW, and SM contributed to interpreting the data and editing the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical Approval
This study received ethics approval from the RAND Corporation’s Human Subjects Protection Committee (#2016-0956), the Mildmay Uganda Research Ethics Committee Institutional Review Board (#02013-2018), and the Uganda National Council for Science and Technology (#2394).
Informed Consent
Verbal consent to participate was obtained from all study participants prior to the start of data collection.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Linnemayr, S., Jennings Mayo-Wilson, L., Saya, U. et al. HIV Care Experiences During the COVID-19 Pandemic: Mixed-Methods Telephone Interviews with Clinic-Enrolled HIV-Infected Adults in Uganda. AIDS Behav 25, 28–39 (2021). https://doi.org/10.1007/s10461-020-03032-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-020-03032-8