
Abstract
Strongyloidiasis has been estimated to affect over 600 million people worldwide. It is caused by Strongyloides stercoralis, a roundworm endemic to the tropics and subtropics, especially areas where sanitation is suboptimal Autochthonous transmission has been documented in rural areas of the USA and Europe. Humans are infected when larvae penetrate the skin or are ingested. Autoinfection, in which larvae generated in the host go on to re-infect the host, leads to a state of chronic asymptomatic infection often with eosinophilia. Hyperinfection syndrome may develop when patients develop immune suppression, due to medications such as corticosteroids or following solid-organ transplantation. Hyperinfection is characterized by exponential increase in parasitic burden, leading to tissue invasion and life-threatening disease and associated bloodstream infections due to enteric organisms. Cases following use of corticosteroids for COVID-19 pneumonia have been described. Strongyloidiasis can be diagnosed by direct visualization of larvae in stool or other body fluids, or by serology. Ivermectin is highly effective in treating the disease. Patients with exposure to endemic areas and those expected to become immune suppressed should be screened and treated before starting immune suppressive agents. Empiric treatment should be considered when timely testing is not readily available.
Similar content being viewed by others


Introduction
Strongyloides stercoralis is a roundworm (nematode) that causes the disease known as strongyloidiasis. It has been estimated to affect over 600 million people worldwide [1], and is of particular clinical importance due to its ability to cause chronic infection that can become life-threatening in the setting of immunosuppression. Though S. fuelleborni and some other zoonotic species have been implicated as human pathogens, they are of minor medical relevance [2]. This review will focus on the epidemiology, basic parasitology, presentation, diagnosis, and management of S. stercoralis infection.
Epidemiology
Strongyloides stercoralis is endemic worldwide, but is most prevalent in tropical and subtropical climates, especially in areas with inadequate sanitary conditions. Community-based studies have estimated a prevalence of over 70% in countries such as Peru, Kenya, Namibia, and Papua New Guinea. In the USA and Europe the majority of cases are considered imported, though local transmission has been reported mainly in rural areas. A recent prospective study that enrolled patients in Cataluña (Spain) from 2003 to 2012 found seventy cases of strongyloidiasis, diagnosed either by serologic testing, or by sputum or fecal parasitology. Of these, 59% were considered to have originated in South America and the Caribbean, 26% in sub-Saharan Africa, 13% in Southeast Asia, and only 3% were considered autochthonous [3]. Infection with human immunodeficiency virus (HIV), human T-lympho-tropic virus 1 (HTLV-1), hypogammaglobulinemia, alcoholism, and malnutrition have been associated with an increased risk of strongyloidiasis [4, 5]. Institutionalized patients also seem to be more commonly affected [6]. In the USA, a seroprevalence as high as 4% has been documented in areas of rural Kentucky, with most cases occurring in American-born patients that had not traveled to endemic areas [7]. Statistical modeling has suggested that up to 16 states are at high risk of local transmission [8].
Transmission
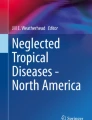
The lifecycle of S. stercoralis is summarized in Fig. 1. S. stercoralis most commonly infects humans through the cutaneous route. Filariform larvae can be found in soil and penetrate the skin of people who go barefoot, which presents as “ground itch”. After penetration, filariform larvae migrate to the lungs, where they mature, are coughed up, and swallowed. When in the small intestine, the larvae mature into adult females, which in turn intermittently produce eggs through asexual reproduction. These then hatch into rhabditiform larvae, which are excreted in stool. The rhabditiform larvae, which are non-infectious, then give rise to the infectious filariform larvae, either in soil or in the own host’s intestine. The latter causes the unique phenomenon of autoinfection, in which filariform larvae generated in the host itself invade intestinal mucosa or perianal skin and restart the infectious cycle [9], which in turn leads to a chronic and frequently subclinical infection. Primary infection can also occur by ingestion of the filariform larvae, either by consumption of contaminated food or water, or sexually, by anal–oral contact [10]. In people with delayed fecal transport, autoinfection can be significant and cause large worm burdens. In those where fecal soilage of the skin occurs for prolonged periods of time, penetration of filariform larvae can cause local irritation as well as autoinfection. Cases of transmission following kidney transplantation have also been reported [11].

Lifecycle of S. stercoralis. (1) Filariform larvae penetrate the host’s skin and migrate to pulmonary parenchyma. (2) Filariform larvae are coughed up and swallowed. (3) Filariform larvae migrate to small intestine and lay eggs, which hatch into rhabditiform larvae. (4) Rhabditiform larvae are excreted in soil and give rise to infectious filariform larvae, which are able to penetrate skin and restart the cycle. S. stercoralis also has a free-living life cycle, independent of human hosts. (5) Rhabditiform larvae may give rise to infectious filariform larvae in the host itself, leading to invasion of intestinal mucosa and/or perianal skin, process known as autoinfection. In the right host, this may lead to hyperinfection syndrome. Figure created with Biorender
Clinical Spectrum of Disease
Strongyloidiasis occurs in three forms: acute, caused by primary parasitic invasion; chronic, caused by autoinfection; and hyperinfection, which typically occurs in the setting of immunosuppression. Table 1 further outlines the wide array of manifestations that have been described in this disease. The most common pulmonary manifestations of strongyloidiasis are transient pulmonary opacities with cough, dyspnea, and bronchospasm often with associated pulmonary and peripheral eosinophilia. Chest radiographs range from being normal to showing bilateral opacities. Other manifestations that have been reported include lobar infiltrates, interstitial infiltrates, and abscess/cavitation. Strongyloidiasis may cause asthma with improvement of asthma occurring following treatment of this infection. Patients with chronic obstructive pulmonary disease (COPD) or asthma form endemic regions should be screened for strongyloidiasis, especially before starting steroids which could trigger a hyperinfection syndrome.
Acute Strongyloidiasis
Acute strongyloidiasis is typically oligosymptomatic. Larval skin invasion usually occurs in the feet and may cause a serpiginous trail of dermatitis known as larva currens (“running larvae”), similar to what occurs in toxocariasis. Though pulmonary migration of larvae may cause a Loeffler-like syndrome, it is less frequent than that classically described in ascariasis [12]. Symptoms of asthma, peripheral eosinophilia, and pulmonary infiltrates on chest imaging may develop in this stage. Upper gastrointestinal symptoms, such as heartburn and bloating are commonly reported. Diarrhea and malabsorption are less frequent [13].
Chronic Strongyloidiasis
Chronic strongyloidiasis is mostly asymptomatic. It is most frequently diagnosed during workup of peripheral eosinophilia, which tends to decrease steadily following initial exposure [3]. Serology for strongyloidiasis can be used to screen for asymptomatic chronic infection. Symptomatic patients can intermittently experience dyspnea, wheezing, diarrhea, abdominal pain, constipation, vomiting, weight loss, urticaria, and/or larva currens [3, 6, 14, 15]. Migration of larvae through the lung parenchyma can cause a foreign body reaction, inflammatory pneumonitis, and pulmonary hemorrhage [16]. Rarer manifestations of chronic infection include reactive arthritis, chronic malabsorption, nephrotic syndrome, duodenal obstruction, and hepatic lesions.
Strongyloides Hyperinfection Syndrome
Strongyloides hyperinfection syndrome typically occurs when patients with chronic infection become immunosuppressed, leading to a dramatic increase in the rate of autoinfection and consequently, in parasitic burden [17]. Dissemination of larvae throughout tissues causes direct damage. Disruption of the intestinal membrane predisposes to bacteremia caused by intestinal flora. It has been suggested that the migrating larvae may also carry bacteria from the gastrointestinal tract to the lung and other organs. Though presentation is highly variable, classically strongyloides hyperinfection syndrome manifests by recurrent unexplained enterobacterial bloodstream infections, which can be polymicrobial and seed to unusual sites such as the meninges [12]. The lung is an important target organ in hyperinfection with the usual presentation being pneumonia and cough from the migrating filiform larvae in the pulmonary parenchyma. Eosinophilia is usually not seen due to steroids being the precipitating factor in the majority of cases of strongyloides hyperinfection syndrome. Chest radiographs typically show bilateral infiltrates which can be interstitial or parenchymal; however focal lobar infiltrates are also reported to occur. Hemoptysis and respiratory failure can be seen. Hyperinfection often presents with significant gastrointestinal symptoms including abdominal pain, nausea, vomiting, and ileus. The mortality of untreated strongyloides hyperinfection syndrome varies from 85 to 100% [18].
Use of corticosteroids is the most common trigger for strongyloides hyperinfection syndrome [17] and has been reported with courses as short as 6 days [19] and doses as low as 20 mg of prednisone/day [20]. Unsurprisingly, multiple cases of strongyloides hyperinfection syndrome following use of corticosteroids in the management of COVID-19 pneumonia have been reported [21, 22]. A variety of other immunosuppressive medications, such as rituximab, mycophenolate mofetil, antithymocyte globulin, and antineoplastic agents such as adriamycin, doxorubicin, and melphalan have also been implicated in strongyloides hyperinfection syndrome. Infection with HTLV-1, hypogammaglobulinemia (associated with nephrotic syndrome and multiple myeloma), hematologic malignancies, solid-organ and hematopoietic stem cell transplantation have also been associated with strongyloides hyperinfection syndrome [18]. Though initially considered an AIDS (acquired immunodeficiency syndrome) defining illness, a relatively small number of cases of strongyloides hyperinfection syndrome associated with HIV have been reported, and most of them have occurred following use of corticosteroids for conditions such as Pneumocystis pneumonia [23,24,25]. Strongyloides hyperinfection syndrome has been seen occasionally in immune competent individuals without other significant risk factors, for example, cases have been seen following laparoscopic surgery [26, 27]. It is thought that hypomotility of the gastrointestinal tract, i.e., prolonged transit time of stool, probably permits conversion of a higher numbers of rhabditiform larvae into infectious filariform larvae facilitating hyperinfection.
Immunopathogenesis
The innate immune response to S. stercoralis is mediated by eosinophils, granulocytes, and macrophages [28,29,30]. Larval killing by eosinophils depends on eosinophil major basic protein, and by granulocytes on myeloperoxidase [31]. Both cell types rely on complement-mediated mechanisms for killing [32]. Though classically not thought of as antigen-presenting cells, eosinophils have been shown to be able to act as such in animal models of strongyloidiasis [33]. The adaptive immune response to S. stercoralis is typically Th2-skewed, with interleukin (IL)-5 leading to further recruitment and activation of eosinophils, and IL-4 and IL-5 promoting class switch of immunoglobulins secreted by B cells to IgEs [34]. IL-13 causes increased peristalsis, possibly leading to increased larval expulsion [35]. Expression of regulatory T-cells (T-reg) appears to be important in the pathogenesis of hyperinfection, i.e., increased numbers of T-regs lead to decreased levels of IL-5 and IgE, and presumably impaired larval killing [36]. In HTLV-1 co-infected patients, T-reg expression is increased and is thought to contribute to the higher frequency of hyperinfection in this population [37].
Diagnosis
Strongyloidiasis should be suspected in any patient with unexplained eosinophilia especially if they have had epidemiologic exposure in areas of high disease prevalence. There is also a role for screening patients thought to be at increased risk of developing hyperinfection, such as those undergoing transplantation [38] or starting medications, such as corticosteroids, that have been implicated in strongyloides hyperinfection syndrome [39]. Screening should also be considered in those with evidence of infection with HLTV-1 [18]. Screening prior to use of corticosteroids can involve both parasitological and serological assays.
Parasitological Testing
Direct visualization of larvae is the gold-standard for diagnosis of strongyloidiasis. Sensitivity of single specimen stool microscopy is as low as 21% [40]. This is thought to be due to intermittent parasite shedding and low infectious burden. Examination of multiple specimens obtained on different dates increases sensitivity, which approaches 100% when seven samples are sent [41]. Parasitological techniques such as the modified agar plate method and the Baermann technique can be used to improve diagnostic yield, but they are seldom performed in most parasitology labs [42]. Real-time polymerase chain reaction (PCR) has been used for diagnosis of strongyloidiasis, but estimates of sensitivity of this method vary greatly and the nucleic acid probes are not yet easily available [42]. In cases of hyperinfection, the large number of worms make detection less challenging: larvae can be seen in preparations of sputum, bronchoalveolar or gastric lavage, urine, blood, and even in lung or gastrointestinal biopsies [42].
Serologic Testing
There are several commercially available serologic tests for strongyloidiasis. Though it is challenging to estimate sensitivity and specificity of these tests, as cases of chronic strongyloidiasis have low parasitic burden, which in turn decreases the sensitivity of fecal tests used as gold-standards, the negative predictive value of serology in immigrants in low prevalence settings approaches 100% [43]. The same is not true for recently acquired infections (e.g., returning traveler), in which the negative predictive value of serological screening was found to be only 72% [44]. In these cases, a negative serology is not sufficient to rule out infection and clinicians should consider stool examination and paired serologic testing if clinical suspicion is high. Cross-reactivity with other parasites such as hookworms, ascaris, and filaria has been well described, though this appears to be less of a concern in more modern test kits [45].
Management
Clinical trials of drugs for treatment of strongyloidiasis have mostly focused on the treatment of chronic infection, not on strongyloides hyperinfection syndrome. Ivermectin, a broad-spectrum antiparasitic that causes muscle paralysis in invertebrates, has emerged as the treatment of choice for strongyloidiasis. It is better tolerated than and has similar efficacy than the previously recommended drug thiabendazole [46] and is more effective in achieving larval clearance when compared to albendazole [47]. For uncomplicated S. stercoralis infections, the usual treatment in the USA is oral ivermectin 200 μg/kg/day for two consecutive days. Some experts recommend repeating the course after 2 weeks to account for the parasite’s autoinfectious cycle [48]. However, in a randomized clinical trial, single-dose ivermectin has been shown to have similar efficacy to multiple-dose regimens [49, 50]. The same treatment recommendation as used for uncomplicated S. stercoralis infection applies to patients found to have positive serology during screening, though it is important to note that the use of comparative antibody titers as markers of parasitic eradication following treatment has not been adequately evaluated. Moreover, characteristics of different serology techniques vary greatly, and laboratory protocols are not standardized [45]. Due to the high cost and long turn-around times of tests for S. stercoralis and the safe profile of ivermectin, some experts suggest empiric treatment in patients considered to be at high risk [18].
Though there is a lack of high-quality evidence for treatment of cases of hyperinfection, experts suggest that ivermectin should be given daily at 200 μg/kg/day for at least two weeks. Ideally, treatment should be extended until no more larvae are found in stool specimens. Reduction in immunosuppressive regimens should be considered in cases where the risks of strongyloides hyperinfection syndrome outweigh the benefits of immunosuppression. In cases where oral administration is not possible, or when intestinal absorption of ivermectin is thought to be impaired, alternative routes of administration may be considered. Though not approved by the US Food and Drug Administration (FDA), rectal administration of ivermectin (200 μg/kg/day) has been reported as successful. Parenteral (subcutaneous) ivermectin, only available in veterinary formulations, should be reserved as a last resort [18]. There have also been reports of successful treatment with the addition of albendazole (400 mg orally twice a day) to ivermectin [51]. Additionally, patients with strongyloides hyperinfection syndrome should be considered infectious and placed on standard contact precautions [18].
Though there have been reports of cases of severe toxicities following use of high-dose ivermectin inappropriately used to treat COVID-19, the drug is generally well-tolerated when given in recommended doses. Use should be avoided in patients with Loa loa, a filarial disease endemic to West Africa, as it has been associated development of encephalopathy [52]. Albendazole is a possible alternative for the management of these co-infection cases. Moxidectin has shown efficacy for the treatment of strongyloides infections in a phase 2 clinical trials and is a promising addition to the armamentarium for this infection [53, 54].
Conclusion
Although infection with S. stercoralis is frequently asymptomatic, it has the potential of causing life-threatening disease in the immunocompromised. Ivermectin is a well-tolerated and highly efficacious drug for treatment of strongyloidiasis. As such, screening and adequate treatment of at-risk populations, especially the immunocompromised and those receiving immunosuppressive agents such as corticosteroids, is paramount in avoiding the devastating hyperinfection syndrome. When screening is not feasible, empiric treatment of these patients should be strongly considered.
References
Buonfrate D, Bisanzio D, Giorli G, Odermatt P, Furst T, Greenaway C et al (2020) The global prevalence of Strongyloides stercoralis Infection. Pathogens 9(6):468
Nutman TB (2017) Human infection with Strongyloides stercoralis and other related Strongyloides species. Parasitology 144(3):263–273
Valerio L, Roure S, Fernandez-Rivas G, Basile L, Martinez-Cuevas O, Ballesteros AL et al (2013) Strongyloides stercoralis, the hidden worm. Epidemiological and clinical characteristics of 70 cases diagnosed in the North Metropolitan Area of Barcelona, Spain, 2003–2012. Trans R Soc Trop Med Hyg 107(8):465–470
Schar F, Trostdorf U, Giardina F, Khieu V, Muth S, Marti H et al (2013) Strongyloides stercoralis: global distribution and risk factors. PLoS Negl Trop Dis 7(7):e2288
Scowden EB, Schaffner W, Stone WJ (1978) Overwhelming strongyloidiasis: an unappreciated opportunistic infection. Medicine (Baltimore) 57(6):527–544
Berk SL, Verghese A, Alvarez S, Hall K, Smith B (1987) Clinical and epidemiologic features of strongyloidiasis. A prospective study in rural Tennessee. Arch Intern Med 147(7):1257–1261
Russell ES, Gray EB, Marshall RE, Davis S, Beaudoin A, Handali S et al (2014) Prevalence of Strongyloides stercoralis antibodies among a rural Appalachian population—Kentucky, 2013. Am J Trop Med Hyg 91(5):1000–1001
Singer R, Sarkar S (2020) Modeling strongyloidiasis risk in the United States. Int J Infect Dis 100:366–372
Mehlhorn H (2008) Encyclopedia of parasitology, 3rd edn. Springer, New York
Sorvillo F, Mori K, Sewake W, Fishman L (1983) Sexual transmission of Strongyloides stercoralis among homosexual men. Br J Vener Dis 59(5):342
Hamilton KW, Abt PL, Rosenbach MA, Bleicher MB, Levine MS, Mehta J et al (2011) Donor-derived Strongyloides stercoralis infections in renal transplant recipients. Transplantation 91(9):1019–1024
Bennett JE, Dolin R, Blaser MJ (2019) Mandell, douglas, and bennett’s principles and practice of infectious diseases, 9th edn. Elsevier, Philadelphia
Mokhlesi B, Shulzhenko O, Garimella PS, Kuma L, Monti C (2004) Pulmonary Strongyloidiasis: the varied clinical presentations. Clin Pulm Med 11(1):6–13
Nwokolo C, Imohiosen EA (1973) Strongyloidiasis of respiratory tract presenting as “asthma.” Br Med J 2(5859):153–154
Pelletier LL Jr., Gabre-Kidan T (1985) Chronic strongyloidiasis in Vietnam veterans. Am J Med 78(1):139–140
Woodring JH, Halfhill H 2nd, Reed JC (1994) Pulmonary strongyloidiasis: clinical and imaging features. AJR Am J Roentgenol 162(3):537–542
Keiser PB, Nutman TB (2004) Strongyloides stercoralis in the immunocompromised population. Clin Microbiol Rev 17(1):208–217
Mejia R, Nutman TB (2012) Screening, prevention, and treatment for hyperinfection syndrome and disseminated infections caused by Strongyloides stercoralis. Curr Opin Infect Dis 25(4):458–463
Ghosh K, Ghosh K (2007) Strongyloides stercoralis septicaemia following steroid therapy for eosinophilia: report of three cases. Trans R Soc Trop Med Hyg 101(11):1163–1165
Wurtz R, Mirot M, Fronda G, Peters C, Kocka F (1994) Short report: gastric infection by Strongyloides stercoralis. Am J Trop Med Hyg 51(3):339–340
Marchese V, Crosato V, Gulletta M, Castelnuovo F, Cristini G, Matteelli A et al (2021) Strongyloides infection manifested during immunosuppressive therapy for SARS-CoV-2 pneumonia. Infection 49(3):539–542
Lier AJ, Tuan JJ, Davis MW, Paulson N, McManus D, Campbell S et al (2020) Case Report: disseminated Strongyloidiasis in a patient with COVID-19. Am J Trop Med Hyg 103(4):1590–1592
Celedon JC, Mathur-Wagh U, Fox J, Garcia R, Wiest PM (1994) Systemic strongyloidiasis in patients infected with the human immunodeficiency virus. A report of 3 cases and review of the literature. Medicine (Baltimore) 73(5):256–263
Mascarello M, Gobbi F, Angheben A, Gobbo M, Gaiera G, Pegoraro M et al (2011) Prevalence of Strongyloides stercoralis infection among HIV-positive immigrants attending two Italian hospitals, from 2000 to 2009. Ann Trop Med Parasitol 105(8):617–623
Walson JL, Stewart BT, Sangare L, Mbogo LW, Otieno PA, Piper BK et al (2010) Prevalence and correlates of helminth co-infection in Kenyan HIV-1 infected adults. PLoS Negl Trop Dis 4(3):e644
Husni RN, Gordon SM, Longworth DL, Adal KA (1996) Disseminated Strongyloides stercoralis infection in an immunocompetent patient. Clin Infect Dis 23(3):663
Mohammed S, Bhatia P, Chhabra S, Gupta SK, Kumar R (2019) Pulmonary hyperinfection with Strongyloides stercoralis in an immunocompetent patient. Indian J Crit Care Med 23(10):481–483
Bonne-Annee S, Kerepesi LA, Hess JA, O’Connell AE, Lok JB, Nolan TJ et al (2013) Human and mouse macrophages collaborate with neutrophils to kill larval Strongyloides stercoralis. Infect Immun 81(9):3346–3355
Galioto AM, Hess JA, Nolan TJ, Schad GA, Lee JJ, Abraham D (2006) Role of eosinophils and neutrophils in innate and adaptive protective immunity to larval Strongyloides stercoralis in mice. Infect Immun 74(10):5730–5738
Rosenberg HF, Dyer KD, Foster PS (2013) Eosinophils: changing perspectives in health and disease. Nat Rev Immunol 13(1):9–22
O’Connell AE, Hess JA, Santiago GA, Nolan TJ, Lok JB, Lee JJ et al (2011) Major basic protein from eosinophils and myeloperoxidase from neutrophils are required for protective immunity to Strongyloides stercoralis in mice. Infect Immun 79(7):2770–2778
Kerepesi LA, Hess JA, Nolan TJ, Schad GA, Abraham D (2006) Complement component C3 is required for protective innate and adaptive immunity to larval Strongyloides stercoralis in mice. J Immunol 176(7):4315–4322
Padigel UM, Lee JJ, Nolan TJ, Schad GA, Abraham D (2006) Eosinophils can function as antigen-presenting cells to induce primary and secondary immune responses to Strongyloides stercoralis. Infect Immun 74(6):3232–3238
Allen JE, Maizels RM (2011) Diversity and dialogue in immunity to helminths. Nat Rev Immunol 11(6):375–388
Mannon P, Reinisch W (2012) Interleukin 13 and its role in gut defence and inflammation. Gut 61(12):1765–1773
Montes M, Sanchez C, Verdonck K, Lake JE, Gonzalez E, Lopez G et al (2009) Regulatory T cell expansion in HTLV-1 and strongyloidiasis co-infection is associated with reduced IL-5 responses to Strongyloides stercoralis antigen. PLoS Negl Trop Dis 3(6):e456
Dykie A, Wijesinghe T, Rabson AB, Madugula K, Farinas C, Wilson S et al (2020) Human T-cell Leukemia Virus Type 1 and Strongyloides stercoralis: partners in pathogenesis. Pathogens 9(11):904
LaHoz RM, Morris MI, Practice ASTIDCo (2019) Intestinal parasites including cryptosporidium, cyclospora, giardia, and microsporidia, entamoeba histolytica, strongyloides, schistosomiasis, and echinococcus: guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant 33(9):e13618
Stauffer WM, Alpern JD, Walker PF (2020) COVID-19 and dexamethasone: a potential strategy to avoid steroid-related strongyloides hyperinfection. JAMA 324(7):623–624
Campo Polanco L, Gutierrez LA, Cardona AJ (2014) Diagnosis of Strongyloides stercoralis infection: meta-analysis on evaluation of conventional parasitological methods (1980–2013). Rev Esp Salud Publica 88(5):581–600
Nielsen PB, Mojon M (1987) Improved diagnosis of Strongyloides stercoralis by seven consecutive stool specimens. Zentralbl Bakteriol Mikrobiol Hyg A 263(4):616–618
Siddiqui AA, Berk SL (2001) Diagnosis of Strongyloides stercoralis infection. Clin Infect Dis 33(7):1040–1047
Boscolo M, Gobbo M, Mantovani W, Degani M, Anselmi M, Monteiro GB et al (2007) Evaluation of an indirect immunofluorescence assay for strongyloidiasis as a tool for diagnosis and follow-up. Clin Vaccine Immunol 14(2):129–133
Sudarshi S, Stumpfle R, Armstrong M, Ellman T, Parton S, Krishnan P et al (2003) Clinical presentation and diagnostic sensitivity of laboratory tests for Strongyloides stercoralis in travellers compared with immigrants in a non-endemic country. Trop Med Int Health 8(8):728–732
Requena-Mendez A, Chiodini P, Bisoffi Z, Buonfrate D, Gotuzzo E, Munoz J (2013) The laboratory diagnosis and follow up of strongyloidiasis: a systematic review. PLoS Negl Trop Dis 7(1):e2002
Gann PH, Neva FA, Gam AA (1994) A randomized trial of single- and two-dose ivermectin versus thiabendazole for treatment of strongyloidiasis. J Infect Dis 169(5):1076–1079
Datry A, Hilmarsdottir I, Mayorga-Sagastume R, Lyagoubi M, Gaxotte P, Biligui S et al (1994) Treatment of Strongyloides stercoralis infection with ivermectin compared with albendazole: results of an open study of 60 cases. Trans R Soc Trop Med Hyg 88(3):344–345
Greaves D, Coggle S, Pollard C, Aliyu SH, Moore EM (2013) Strongyloides stercoralis infection. BMJ 347:f4610
Hurlimann E, Keiser J (2019) A single dose of ivermectin is sufficient for strongyloidiasis. Lancet Infect Dis 19(11):1150–1151
Buonfrate D, Salas-Coronas J, Munoz J, Maruri BT, Rodari P, Castelli F et al (2019) Multiple-dose versus single-dose ivermectin for Strongyloides stercoralis infection (Strong Treat 1 to 4): a multicentre, open-label, phase 3, randomised controlled superiority trial. Lancet Infect Dis 19(11):1181–1190
Pornsuriyasak P, Niticharoenpong K, Sakapibunnan A (2004) Disseminated strongyloidiasis successfully treated with extended duration ivermectin combined with albendazole: a case report of intractable strongyloidiasis. Southeast Asian J Trop Med Public Health 35(3):531–534
Boussinesq M, Kamgno J, Pion SD, Mackenzie CD (2010) Erythropoietin for treating post-ivermectin Loa-related serious adverse events? Trends Parasitol 26(1):4–5
Hofmann D, Sayasone S, Sengngam K, Chongvilay B, Hattendorf J, Keiser J (2021) Efficacy and safety of ascending doses of moxidectin against Strongyloides stercoralis infections in adults: a randomised, parallel-group, single-blinded, placebo-controlled, dose-ranging, phase 2a trial. Lancet Infect Dis 21(8):1151–1160
Bisoffi Z, Buonfrate D (2021) Moxidectin: an ally to ivermectin for treating Strongyloides stercoralis? Lancet Infect Dis 21(8):1060–1061
Funding
The authors declare that no funds, grants, or other support were received that supported the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the preparation and editing of this article (JMC wrote the initial draft, LMW edited and revised this draft).
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no relevant financial or non-financial interests to disclose.
Ethical Approval
This manuscript does not involve research with human or animal subjects.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Czeresnia, J.M., Weiss, L.M. Strongyloides stercoralis . Lung 200, 141–148 (2022). https://doi.org/10.1007/s00408-022-00528-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00408-022-00528-z