
Abstract
Purpose
We aim to study the prevalence of olfactory and taste dysfunction (OTD) in subjects residing in a Community Care Facility (CCF), a center unique to Singapore that is dedicated to isolate foreign workers with COVID-19 infection who have mild disease with minimal or no symptoms.
Methods
This is a cross-sectional study analyzing data prospectively collected from COVID-19-positive subjects who were admitted into a single-center Singapore EXPO CCF from 1st May 2020 to 1st July 2020. The following variables were collected: age, gender, ethnicity, anosmia, ageusia and acute respiratory infection (ARI) symptoms. Symptoms of anosmia and ageusia were self-declared via a mandatory questionnaire administered on admission.
Results
A total of 1983 subjects were included. The overall prevalence of anosmia and ageusia is 3.0% and 2.6%, respectively. 58% of anosmic subjects have co-existent ageusia and 72.6% of anosmic subjects have no concurrent sinonasal symptoms. OTD is less likely to present in subjects who are asymptomatic for ARI, compared to those symptomatic for ARI (anosmia: 2.0% versus 4.4% p = 0.002; ageusia: 1.6% versus 4.2% p < 0.001). There is a difference in the prevalence of OTD between the different ethnic groups (Indian, Chinese, Bangladeshi and Others), with Chinese and Bangladeshi reporting a higher prevalence (p < 0.043)
Conclusion
The true prevalence of OTD in COVID-19-positive subjects may be low with aggressive screening of all subjects, including those asymptomatic for ARI.
Similar content being viewed by others
Introduction
The coronavirus disease 2019 (COVID-19) was first reported as a mass outbreak in Wuhan, Hubei Province, China and has since proved its virulence as it spread rampantly to the rest of the world. World Health Organization (WHO) declared COVID-19 a pandemic on 11 March 2020 [1]. Since then, the number of cases has been increasing exponentially, with 20,026,186 confirmed cases globally at the time of writing this article [2].
In Singapore, there was a surge of infected cases in April 2020, mostly foreign workers residing in crowded dormitories. In response to this, the Singapore government made efforts at aggressive screening, by means of real-time Polymerase Chain Reaction (rt-PCR) of respiratory specimens of all dormitories, and admitted COVID-19-positive foreign workers into appropriately tiered facilities for medical care and isolation. A Community Care Facility (CCF) is an isolation facility for COVID-19-positive foreign workers with mild or no symptoms. They are generally well subjects who have no medical indications or co-morbidities requiring admission to acute hospital for inpatient care. The proactive screening of this population group presented an opportunity to study the prevalence of OTD in COVID-19-positive subjects.
The main clinical manifestations of COVID-19 are fever, fatigue, dyspnea and upper respiratory tract symptoms such as cough, sore throat, nasal congestion and rhinorrhea. There have been a growing number of reports on increased incidences of olfactory and taste dysfunction (OTD) following COVID-19 infection. Tong et al. quoted a 52.73% pooled prevalence of olfactory dysfunction and 43.93% prevalence of taste dysfunction among diagnosed COVID-19-positive subjects [3]. As the awareness of the association between OTD and COVID-19 rose, the Centres for Disease Control and Prevention (CDC) added “new loss of taste or smell” as a symptom that may appears 2–14 days after COVID-19 exposure [4]. The actual specificity as a criterion for screening suspected COVID-19 cases is unknown, as other viral infections may also cause OTD, and post-viral anosmia makes up only 40% of all causes of anosmia [5].
Current literature suggests COVID-19 subjects of mild-to-moderate disease profile have a higher prevalence of OTD [6,7,8]. We write with great interest with regards to this group of COVID-19 subjects in the CCF who have minimal or no symptoms to investigate the prevalence of OTD in COVID-19 subjects with a mild disease profile exclusively.
Internationally, this is the largest collection of patient data and includes asymptomatic subjects picked up on active screening, a unique population group not previously studied.
Materials and methods
Study population
This is a cross-sectional study involving foreign workers who were admitted to a dedicated Community Care Facility (CCF) for COVID-19-positive subjects from 1st May 2020 to 1st July 2020, yielding a total sample size of 1983 subjects. Aligned with the admission criteria, all subjects were male foreign workers with at least 18 years of age, diagnosed with COVID-19 infection by means of rt-PCR of their respiratory specimens, and had only minimal or no symptoms (asymptomatic). Basic demographics and symptomatology data were extracted from the online electronic medical records on GPConnect. Assessments for anosmia, ageusia and acute respiratory infection, i.e. nasal congestion, rhinorrhea, cough and sore throat, were reported as binary (yes or no). Approval for the study was obtained from the SingHealth Centralized Institutional Review for use of de-identified data (CIRB Ref: 2020/2463).
Assessment of anosmia and ageusia
Symptoms of anosmia and ageusia were self-declared by subjects via a mandatory questionnaire as part of the admission workflow. The questionnaire was translated to the respective languages to ask “did you lose your sense of smell?” and “did you lose your sense of taste?” When in doubt, the questionnaire administrators would clarify verbally with the subjects that the intention of the questions was a complete loss of smell and taste at any point of their infection, even if they subsequently regained some of their senses later on in the recovery period.
Statistical analysis
Continuous and categorical variables were expressed as median (interquartile range) and proportion, respectively, and compared using Wilcoxon rank-sum test and Chi-square test, respectively. Fisher’s exact test was used for comparison of categorical variables, where appropriate. A p value < 0.05 was considered significant. All statistical analysis was performed using R 3.6.3, [R Core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria].
Results
A total of 1983 subjects were identified in the study. The median age was 35 (IQR 29–40) years. 54% were of Bangladeshi ethnicity, 37% Indian and 5.1% Chinese (Table 1). The overall prevalence of OTD (anosmia or ageusia) was 3.8%. Of the 2 study symptoms, 59 (3.0%) subjects reported anosmia and 51 (2.6%) subjects reported ageusia; these figures are much lower than those quoted in the current literature. We observed that the Chinese and Bangladeshi subjects were more likely to have OTD, as compared to Indian and Others (Table 2, Fig. 1). This result is of statistical significance (p = 0.043).

Prevalence rates of OTD, anosmia and ageusia in COVID-19 patients by ethnicities
Of the 76 subjects with OTD, 59% had co-existent acute respiratory infection (ARI) symptoms such as cough, sore throat, nasal congestion or rhinorrhea (p < 0.001). The occurrence of anosmia in symptomatic subjects was 4.4% compared to 2.1% in asymptomatic subjects (p = 0.002), and the occurrence of ageusia in symptomatic subjects was 4.2% compared to 1.6% in asymptomatic subjects (p < 0.001) (Table 3, Fig. 2a and b). 27% of subjects with anosmia had concurrent sinonasal symptoms (rhinorrhoea and nasal congestion), while 73% of them did not (Table 4).

a (Left) Venn diagram showing proportion of anosmic patients with and without ARI symptoms. b (Right) Venn diagram showing proportion of ageusic patients with and without ARI symptoms
Discussion
Mao et al. was one of the first authors to propose a correlation between COVID-19 and OTD. He studied subjects with peripheral nervous symptoms attributed to COVID-19 and found that 5.6% had hypogeusia and 5.1% had hyposmia [9]. Following this, many authors have submitted reports to support an association between COVID-19 and OTD. Many studies are heterogeneous with respect to severity of disease, most commonly grouped together as mild-moderate disease profile (due to ethical difficulties to recruit severely ill subjects in the intensive care setting). There is scarcity of sub-group analyses to investigate possible differences in symptomatology between mild and moderate disease profiles.
This is the largest study to-date on the prevalence of OTD in COVID-19 subjects with minimal or no symptoms. We observed an overall prevalence of 3.8% for OTD, of which 3.0% were anosmic and 2.6% were ageusic; these figures are much lower than those quoted in the current literature. This can be attributed to the aggressive mass screening exercise that was carried out in foreign worker dormitories, resulting in a larger denominator, as well as the inclusion of well-asymptomatic subjects. This is as opposed to other studies that survey for OTD in symptomatic subjects who actively seek medical attention.
We were able to perform sub-group analysis to compare the prevalence of OTD in symptomatic versus asymptomatic subjects. We found that the occurrence of anosmia in subjects with ARI symptoms was twice that of asymptomatic subjects (4.4% versus 2.1%, p = 0.002), and the occurrence of ageusia in symptomatic subjects was almost three times that of asymptomatic subjects (4.2% versus 1.6%, p < 0.001). Our data suggests that OTD is less common in asymptomatic subjects.
Similar to Mao et al., our study reported a lower prevalence of OTD compared to our non-Asian counterparts. Speth et al. described a prevalence of 61.2% for COVID-19-related olfactory dysfunction (mostly anosmia) in Switzerland [10], Lechien et al. found olfactory dysfunction in 85.6% of COVID-19-positive subjects (79.6% anosmic and 20.4% hyposmic) in Europe [7], Hopkins et al. found 86.4% of COVID-19-positive subjects anosmic in England [8]. Lechien et al. proposed that Angiotensin-converting-enzyme-2 (ACE2) polymorphisms and differences in expression levels between Asian and European populations could be the reason for the different symptom presentations across ethnicities [7, 11]. In our sub-group analysis, we found that Chinese and Bangladeshi subjects were more likely to have OTD compared to other South East Asian ethnicities in the foreign worker population (such as Indian, Thai, Sri Lankan and Filipino). This further suggests that there may be genetic affinity of some viruses for some tissues and individuals. This is another area to explore so as to shed light on the potential clinical differences between subjects from different world regions [7, 12].
Our study reported that 58% of anosmic subjects also had co-existent ageusia. This can be explained by the widely proposed angiotensin-converting enzyme 2- (ACE2) mediated mechanism. ACE2 is the main host cell receptor of SARS-CoV-2 and they are highly expressed in nasal respiratory epithelial cells and olfactory epithelial cells. It was postulated that viral invasion of the olfactory epithelial cells can lead to anosmia, especially when coronaviruses have been shown to be highly neurotropic in animal models [13, 14]. Taste can potentially be affected in the same way, as ACE2 is also highly expressed on the oral mucosa and tongue.
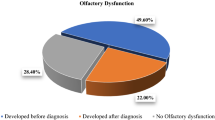
The other proposed mechanism for olfactory dysfunction is conductive—secondary to inflammation and edema of the sinonasal passage, obstructing olfactory molecules from reaching the olfactory cleft. This is less subscribed to, since there have been substantial reports on olfactory dysfunction in the absence of sinonasal symptoms. Lechien et al. found that 79.7% of COVID-19-positive subjects reported anosmia in the absence of nasal congestion of rhinorrhea [7], while Beltra´n-Corbellini et al. reported that only 12.9% of COVID-19-positive subjects in his study with OTD had nasal congestion [15]. Our results are consistent with these studies, as 72.9% of our subjects who reported anosmia had no concurrent sinonasal symptoms (nasal congestion or rhinorrhea).
Limitations
The results of our study should be interpreted within the constraints of its limitations. First, this study only assessed for anosmia and ageusia, but not other degrees of sensory loss or alteration such as hypogeusia, hyposmia and phantosmia. The study was designed to focus specifically on complete loss of olfactory function, in view of the challenge of administering the questionnaire in multiple different languages in a multi-national and multi-lingual study population. They were direct binary questions targeted at anosmia and ageusia, hence study subjects should be able to declare such symptoms with confidence. As subjects in this facility were generally well and found to be COVID-19 positive via proactive screening, their duration of stay was short, before rapid transfer to other step-down facilities. This precluded the feasibility of administering objective smell and taste testing due to time constraints. Nonetheless, we opine that the correlation of self-reported OTD and objective measurement should be undertaken in further large-scale studies involving generally well patients, as this population is significant but understudied. Secondly, there may be recall bias as it is uncertain when was the onset of anosmia or ageusia for our subjects. Third, this is an all-male study population. If gender were a significant risk factor to COVID-19-related OTD, the results of this study would be skewed. A few authors have reported females to be more susceptible to OTD [6, 10], however, this evidence has not yet been reproducible and proven to be significant. Lastly, we did not correlate OTD with cycle threshold values (Ct-values), which is a proxy for viral shedding status. We were unable to follow up on the resolution of OTD due to the large number of study subjects involved and some were transferred out to a step-down facility during this period of data collection.
Conclusion
This is the largest study on prevalence of OTD in a population of COVID-19-positive subjects with minimal or no symptoms. Our finding of a lower prevalence of OTD suggests that these symptoms may be less sensitive as screening criteria in asymptomatic carriers. There is an ethnic difference in the prevalence of OTD. Otolaryngologists should continue to exercise heightened vigilance in managing patients with acute onset of OTD symptoms. Appropriate measures of quarantine and testing should be undertaken, and these patients should be seen after a window period where viral shedding has halted and they are deemed safe to return to the community. Long-term follow-up of these patients should be considered to evaluate if these symptoms resolve and when, if they do.
Data availability
All data and materials as well as software application or custom code support our published claims and comply with field standards.
Code availability
Not applicable.
References
Mahase E (2020) Covid-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ 368:m1036
World Health Organization (2020) Coronavirus disease (COVID-2019) situation reports. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/. Accessed 10 Aug 2020
Tong JY, Wong A, Zhu D, Fastenberg JH, Tham T (2020) The prevalence of olfactory and gustatory dysfunction in Covid-19 patients: a systematic review and meta-analysis. Otolaryngol Head Neck Surg 163(1):3–11
Centres for Disease Control and Prevention (2020) Coronavirus disease 2019 (COVID-19) symptoms. Published April 17, 2020. https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html. Accessed 22 Apr 2020
Welge-Lüssen A, Wolfensberger M (2006) Olfactory disorders following upper respiratory tract infections. Adv Otorhinolaryngol 63:125–132
Giacomelli APL, Conti F, Bernacchia D, Siano M et al (2020) Self-reported olfactory and taste disorders in SARS-CoV-2 patients: a cross-sectional study. Clin Infect Dis 71(15):889–890
Lechien JR, Chiesa-Estomba CM, De Siati DR, Horoi M, Le Bon SD, Rodriguez A et al (2020) Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicentre European study. Eur Arch Otorhinolaryngol 277(8):2251–2261
Hopkins C, Surda P, Whitehead E, Kumar BN (2020) Early recovery following new onset anosmia during the COVID-19 pandemic - an observational cohort study. J Otolaryngol Head Neck Surg 49(1):26
Mao L, Jin H, Wang M et al (2020) Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan. China. JAMA Neurol 77(6):683–690
Speth MM, Singer-Cornelius T, Oberle M, Gengler I, Brockmeier SJ, Sedaghat AR (2020) Olfactory dysfunction and sinonasal symptomatology in COVID-19: prevalence, severity, timing, and associated characteristics. Otolaryngol Head Neck Surg 163(1):114–120
Cao Y, Li L, Feng Z, Wan S, Huang P, Sun X, Wen F, Huang X, Ning G, Wang W (2020) Comparative genetic analysis of the novel coronavirus (2019-nCoV/SARS-CoV-2) receptor ACE2 in different populations. Cell Discov 6:11
Chan JF, Yuan S, Kok KH et al (2020) A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet 395(10223):514–523
McCray PB Jr, Pewe L, Wohlford-Lenane C et al (2007) Lethal infection of K18-hACE2 mice infected with severe acute respiratory syndrome coronavirus. JJ Virol 81(2):813–821
Wheeler DL, Athmer J, Meyerholz DK, Perlman S (2017) Murine olfactory bulb interneurons survive infection with a neurotropic coronavirus. J Virol 91(22):e01099–e1117
Beltran-Corbellini A, Chico-Garcıa JL, Martınez-Poles J et al (2020) Acute-onset smell and taste disorders in the context of Covid19: a pilot multicentre PCR-based case-control study. Eur J Neurol 27(9):1738–1741
Funding
The authors have no funding or financial relationships to disclose.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Soh, S.H.L., See, A., Teo, N.W.Y. et al. Prevalence of olfactory and taste dysfunction in COVID-19 patients: a community care facility study. Eur Arch Otorhinolaryngol 278, 3375–3380 (2021). https://doi.org/10.1007/s00405-021-06647-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-021-06647-2