
Abstract
Summary
This meta-analysis synthesized current evidence from 10 trials to evaluate the association between steroid therapy and osteonecrosis incidence in patients with severe acute respiratory syndrome (SARS). Our results suggest that higher cumulative doses and longer treatment durations of steroids are more likely to lead to the development of osteonecrosis in SARS patients.
Introduction
The link between steroid treatment and the risk of osteonecrosis in SARS patients remains unknown. The present meta-analysis aimed to examine the dose-response association between steroid therapy and osteonecrosis incidence in SARS patients. The sex differences in the development of steroid-induced osteonecrosis were also examined.
Methods
We searched PubMed, Web of Science, CNKI, and WANFANG for studies that involved steroid therapy and reported osteonecrosis data in SARS patients. Two authors independently extracted the data from the individual studies, and the rate ratio (RR) of osteonecrosis was calculated using random-effect models.
Results
Ten studies with 1137 recovered SARS patients met the inclusion criteria. Close relationships between osteonecrosis incidence and both the cumulative dose and treatment duration of steroids were observed. The summary RR of osteonecrosis was 1.57 (95% confidence interval (CI) 1.30–1.89, p < 0.001) per 5.0 g increase in the cumulative dose of steroids and was 1.29 (95% CI 1.09–1.53, p = 0.003) for each 10-day increment of increase in treatment duration. The relationship was non-linear (p non-linear < 0.001 and p non-linear = 0.022). There were no significant differences in the risk of developing osteonecrosis between the male and female patients (RR 0.01, 95% CI −0.03 to 0.06, p = 0.582).
Conclusions
SARS patients who received higher cumulative doses and longer treatment durations of steroids were more likely to develop osteonecrosis, and there were no sex differences in this dose-dependent side effect. Our findings suggest that it is important to reduce osteonecrosis risk by modifying the cumulative dose and the treatment duration of steroids in SARS patients.
Similar content being viewed by others
Introduction
Steroids are the most commonly used immunomodulatory agents for modulating immune activities and reducing inflammation in various critical diseases [1]. However, since the introduction of steroids for the treatment of autoimmune diseases, investigators have become aware of injurious effects [2, 3]. There is an abundance of literature documenting steroid-related osteonecrosis [4, 5], and a causal relationship has been well established. Steroid use has become the most common non-traumatic cause of osteonecrosis, with a prevalence ranging from 3 to 38% [6].
The outbreak of severe acute respiratory syndrome (SARS) in 2003 caused approximately 8098 people to be infected with SARS-associated coronavirus (SARS-CoV) [7]. The SARS-CoV was a novel virus that human beings were encountering for the first time, and they had no effective antiviral agents for treatment. High-dose steroid treatment was frequently prescribed in severe cases to reduce immune activities and other symptoms [7, 8]. The wide use of steroids resulted in the development of serious side effects in many recovered SARS patients, including osteonecrosis [9, 10]. However, the relationship between steroid therapy and osteonecrosis remains unclear, partly because although a number of studies had reported the prevalence of steroid-related osteonecrosis in recovered patients [11–23], some of them failed to address the regimens used [21–23]. The absence of information regarding steroid administration regimens prevented researchers from making precise evaluations of this link. Additionally, Felson and colleagues [24] reported that there was a dose-response relationship between steroid use and the incidence of osteonecrosis. However, whether there is a similar dose-response relationship in SARS patients who received steroids remains unknown. Furthermore, we wondered if there were sex differences in the development of steroid-related osteonecrosis in SARS patients. Therefore, in the current meta-analysis, we aimed to examine the effects of steroid therapy on osteonecrosis in recovered SARS patients. The sex differences in the development of steroid-induced osteonecrosis were also examined.
Materials and methods
Search strategy and inclusion criteria
This meta-analysis was conducted in accordance with PRISMA recommendations and the criteria for the reporting of meta-analysis guidelines [25]. The statistical analysis methods and inclusion criteria were specified and documented in a protocol. An electronic database search was conducted using PubMed, Web of Science, CNKI (China Knowledge Resource Integrated Database), and WANFANG (WANFANG database of China) from January 1, 2003 to March 1, 2016. Studies that involved steroid therapy and reported osteonecrosis data for SARS patients were included. The search terms included the following: “severe acute respiratory syndrome,” “SARS,” “glucocorticoid(s),” “corticosteroid(s),” “steroid(s),” “cortisol(s),” “prednisolone(s),” “methylprednisolone(s),” “dexamethasone(s),” “osteonecrosis,” “bone density,” “osteoporosis,” and “MRI.” The search was restricted to “clinical trials,” and no language restrictions were applied. We also checked the reference lists of the articles and conducted a forward search.
The included studies had to meet the following criteria:
-
Cohort or case-control studies.
-
Recovered SARS patients had received steroid therapy.
-
The follow-up time lasted for at least 1 month.
-
Regimens of steroid therapy were provided.
-
Cumulative dose or treatment duration of steroids included ≥3 categories.
If the studies did not address SARS patients who did not receive steroid therapy or regimens of steroid treatment, they were excluded. Additionally, studies that reported less than three categories for cumulative dose or treatment duration of steroids were also excluded from the current meta-analysis. All the included studies used magnetic resonance imaging (MRI) to screen for osteonecrosis. Images were frequently taken of the hips, knees, shoulders, ankles and wrists. Osteonecrosis was defined as a subchondral or intramedullary area demarcated by a distinct marginal rim with low signal intensity that encompassed the medullary fat on the T1-weighted images.
Data extraction
Two authors (XW and FF) independently reviewed the extracted data from each included study and resolved any disagreements through discussion. There were two papers [18, 26] that reported the similar data, and only one study [18] was used in the final meta-analysis after discussion. We contacted the authors for additional information if necessary. The details that were extracted included the following: steroid therapy regimens (dosage, duration, pulsed steroid therapy, etc.), the total number of SARS patients, osteonecrosis cases, the respective proportions of women and men, follow-up time, mean or median age of participants, and methods of osteonecrosis detection. The data extraction followed the methods provided by the Cochrane Reviewers’ Handbook [27].
Statistical analysis
We used the rate ratio (RR) of osteonecrosis as the outcome, and random-effects models were used for the dose-response meta-analysis. Fixed-effects models were applied for the high vs. low analysis and the examination of the sex differences in the development of steroid-related osteonecrosis. For those studies that did not report RRs and 95% confidence intervals (CI), we calculated these using the category cases and the respective observed numbers of patients compared with the reference category. For each of the included studies, the reported median or mean dose of steroids in each category was designated as the steroid dosage category; we also designated the median or mean days of treatment in each category as the treatment duration category. When studies reported only the range of steroid dose or treatment duration for a category, we used the average value of the lower and upper bounds of the category. When the highest category was open-ended, we assumed its interval length to be the same as the adjacent interval. When the lowest category was open-ended, its dose category or treatment duration category was assigned as the average value of the upper bound and zero.
We first calculated the summary RR and 95% CI of the highest vs. lowest category for the cumulative dose and treatment duration of steroids using fixed-effects models proposed by DerSimonian and Laird [28]. The dose-response meta-analysis was performed using the methods described by Greenland and Longnecker [29], and the study-specific slopes (linear trends) and 95% CIs were calculated from the natural logs of the RRs and CIs across the categories of cumulative dose and treatment duration. The potential non-linear, dose-response associations of osteonecrosis with cumulative dose and treatment duration were estimated using fractional polynomial models [30].
Cochran’s Q test (p < 0.10 for statistical significance) was used to determine the between-study heterogeneity. Funnel plots were generated for cumulative dose and treatment duration of steroids to examine the possibility of publication bias. A two-tailed p value <0.05 was considered significant. Version 13 of the STATA software (StataCorp LP, College Station, TX, USA) was used to perform the meta-analysis and produce the graph.
To test the robustness of our results, we carried out a post hoc sensitivity analysis to explore the possible impact of studies with extreme results. We excluded one study at a time for the two studies with the largest negative and largest positive impacts on the summary estimates. Sensitivity analysis was performed for the cumulative dose of steroids only. We also determined the sex differences in the development of steroid-related osteonecrosis by conducting a meta-analysis for men and women.
Results
Characteristics of the included studies
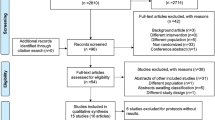
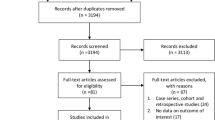
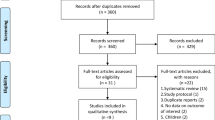
Database searches identified and screened 1260 potential abstracts, of which 1197 were excluded because they either were unrelated to the specific topic or duplicate trials from different databases. Sixty-three full-text articles were then reviewed for eligibility, and 53 studies were excluded for the following reasons: no observations of osteonecrosis, no steroid therapy regimens, abstracts, and others (including studies reporting similar data, cumulative dose and treatment durations that were <3 categories, and reporting of osteonecrosis location but not osteonecrosis cases) (Fig. 1). Ten studies including a total of 1137 SARS patients (with a mean/median age of between 30.0 and 47.0 years) met the inclusion criteria and entered final meta-analysis, of which 304 patients developed osteonecrosis. Seven articles [11, 12, 14, 15, 17–19] were published in Chinese, and 3 [13, 16, 20] were published in English. Seven studies reported the number of osteonecrosis cases in both male and female patients. Eight studies [11, 13–17, 19, 20] were cohorts, and 2 [12, 18] were nested case-controls. All the patients were from China and Hong Kong, and the publication dates ranged from 2003 to 2011. Other information regarding the patients in each study is listed in the table of characteristics of included studies (Table 1).

Flow chart for the selection of studies
Steroid treatment
All the SARS patients included had received steroid therapy, and methylprednisolones were the most commonly used drugs. Two studies [13, 16] reported prednisolone doses, and we computed the methylprednisolone-equivalent dose using a conversion factor of 0.8. One study [19] only presented the daily dose of steroids; thus, we calculated the cumulative dose by multiplying the daily dose by the mean treatment duration. The mean cumulative dose of methylprednisolones ranged from 1.5 to 7.2 g, and the mean treatment duration ranged from 11 to 41 days. Patients who were affected by progressive deterioration frequently received pulsed intravenous steroid therapy at a daily dose ≥320 mg (methylprednisolones). Information regarding the steroid treatments of the SARS patients was retrieved from hospital databases.
Meta-analysis
Summary analyses for the highest vs. lowest category
Nine studies were included in the highest vs. lowest analysis of steroid dose-related osteonecrosis (Electronic Supplementary Material 1). We excluded one study because zero events were reported in the reference category [14]. The pooled RR of osteonecrosis was 2.94 (95% CI 1.96–4.41, p < 0.001), with a relatively low level of heterogeneity (Q = 12.56, p = 0.128) (Fig. 2). Six studies were pooled for the highest vs. lowest analysis of treatment duration-related osteonecrosis (Electronic Supplementary Material 2). Four studies [13, 15, 18, 19] were removed from the analysis because they did not address the duration of treatment. The summary RR of osteonecrosis was 2.68 (95% CI 1.62–4.43, p < 0.001), with low level of between-study heterogeneity (Q = 4.60, p = 0.466) (Fig. 3).

Summary rate ratio (RR) of osteonecrosis for the highest vs. lowest category of cumulative steroid dose

Summary rate ratio (RR) of osteonecrosis for the highest vs. lowest category of treatment duration
Dose-response meta-analyses of the relationship between cumulative dose and treatment duration of steroids and osteonecrosis
In our dose-response meta-analyses, we incorporated 8 and 5 studies to detect associations of cumulative dose and treatment duration, respectively, with osteonecrosis. Two studies were excluded from the estimate of the relationship between cumulative dose and osteonecrosis because one study [11] only reported two categories of cumulative dose and another [14] had zero events in the reference category. In our analysis of associations between treatment duration and osteonecrosis, 5 studies [11, 13, 15, 18, 19] were excluded because they did not include the treatment duration data. The summary RR of osteonecrosis was 1.57 (95% CI 1.30–1.89, p < 0.001) per 5.0 g increase in the cumulative dose of steroids (Fig. 4), and it was 1.29 (95% CI 1.09–1.53, p = 0.003) for each 10-day increment of treatment duration (Fig. 5). The levels of heterogeneity between the studies were relatively high for cumulative dose (Q = 23.89, p = 0.001) and treatment duration (Q = 24.94, p < 0.001). There was pronounced evidence of non-linear associations of cumulative dose (p non-linear < 0.001) and treatment duration (p non-linear = 0.022) with osteonecrosis.

Non-linear regression of the relationship between the cumulative dose of steroids and osteonecrosis

Non-linear regression of the relationship between treatment duration and osteonecrosis
Subgroup analysis between the male and female SARS patients
A subgroup analysis of seven studies was conducted to examine the sex differences in the development of steroid-related osteonecrosis. Our findings suggested that the male and female patients had similar responses to steroid therapy, with a rate difference of osteonecrosis of approximately 0.01 (95% CI −0.03 to 0.06, p = 0.582). The level of heterogeneity between the studies was relatively low (Q = 8.66, p = 0.194).
Sensitivity analysis and funnel plots
Our sensitivity analysis suggested that our results were consistent after excluding the studies with either the largest positive impact or the largest negative impact on the summary estimates. When we removed the study with the largest positive impact [20], the summary RR of osteonecrosis was 1.49 (95% CI 1.24–1.81, p < 0.001) for each 5-g increment of the total dose of steroids. We repeated the analysis after excluding the study with the largest negative impact [16], and the summary RR of osteonecrosis was 1.68 (95% CI 1.36–2.07, p < 0.001) per 5 g increase in cumulative dose. Our visual inspection of the funnel plots of cumulative dose (Electronic Supplementary Material 3) and treatment duration (Electronic Supplementary Material 4) suggested that there was a slight asymmetry; it was likely that the heterogeneity between the studies contributed to the asymmetry because several data points were outside of the 95% confidence limits. Furthermore, our examination of the heterogeneity between studies suggested that the summary estimates of cumulative dose and treatment duration were heterogeneous.
Discussion
Our meta-analysis provides quantitative evidence of the relationship between steroid administration and osteonecrosis incidence in SARS patients. Our findings indicate that the relationships between osteonecrosis incidence and both cumulative dose and treatment duration of steroids are non-linear. The subgroup analysis revealed that there were no sex differences in the development of steroid-induced osteonecrosis between male and female patients.
Although side effects had been reported over the past decade in SARS-recovered patients who had received steroid therapy, a clear link between steroid administration and osteonecrosis incidence was previously unclear. Our study demonstrates for the first time that both cumulative dose and treatment duration of steroids are closely associated with the occurrence of osteonecrosis in recovered SARS patients. A non-linear relationship was observed between cumulative dose and osteonecrosis, and the non-linear regression (Fig. 4) suggested that the risk of osteonecrosis remained relatively low when the total dose of steroids (methylprednisolone) was ≤5 g. However, the incidence of osteonecrosis increased when the total dose increased from 5 up to 10 g and seemed to reach the highest risk with a total dose of approximately 10–15 g. Our findings suggest that lower cumulative doses of steroids (methylprednisolone <5 g) are relatively safe for SARS patients, and physicians should avoid using high doses of steroids, especially for cumulative doses >10 g.
A close relationship between total steroid dose and osteonecrosis incidence in other diseases has been well established. In a 13-year follow-up study, Nakamura and colleagues [31] reported that approximately 15% of systemic lupus erythematosus (SLE) patients requiring increased steroid doses developed osteonecrosis. Shibatani and colleagues [32] evaluated renal-transplant recipients who underwent multiple rejection cycles and demonstrated a close relationship (OR 4.2, p = 0.008) between osteonecrosis and cumulative steroid dose. Felson and colleagues [24] reported a liner dose-response relationship between steroid usage and osteonecrosis incidence, showing a 4.6% increase in the risk of osteonecrosis for every 10 mg/day increase in oral steroids during the first 6 months of therapy. It is difficult to distinguish between the effects of the total dose and mean daily dose of steroids on osteonecrosis because the patients who had received a higher cumulative dose usually had also received a higher mean daily dose. For example, the average total dose of steroids taken by SARS patients in our meta-analysis was approximately 4.6 g, which meant that they had received a mean daily dose of 158 mg. Summarily, our findings suggest that the cumulative dose of steroids is a strong predictor of the risk of osteonecrosis in SARS patients.
We observed a non-linear relationship between treatment duration with steroids and osteonecrosis incidence, suggesting that treatment duration is an important risk factor for the development of osteonecrosis. Our findings were consistent with Nakamura’s study [31] in which they demonstrated that the progression of osteonecrosis was associated with higher doses of steroid treatment for longer durations. Our work provides more important information concerning this link. Our non-linear regression (Fig. 5) indicated that treatment durations that were ≤30 days remained safe for SARS patients, with an RR for osteonecrosis of approximately 1.0, but the osteonecrosis risk increased with an increase in treatment duration from 30 up to 40 days and appeared to reach its highest risk at approximately 50 days. Our findings are clinically important because the different steroid treatment durations were associated with different levels of risk for the development of osteonecrosis.
It was previously unknown whether the incidence of steroid-related osteonecrosis was higher in female SARS patients than male patients. Our findings revealed that female and male SARS patients had similar incidences of steroid-related osteonecrosis. Our results provide pooled evidence to demonstrate that women are not more likely to develop steroid-induced osteonecrosis than men.
The occurrence of osteonecrosis was observed as early as 1 month after high-dose steroid usage in SARS patients [18], and several studies [14, 15, 18, 19] detected a high incidence of osteonecrosis within a half a year. In contrast, the mean time of occurrence of osteonecrosis in the renal-transplant cohorts included in Felson’s review ranged from 12 to 18.6 months. The onset of osteonecrosis in patients with SLE often occurs later, with a mean time from the initiation of steroid treatment to the occurrence of osteonecrosis of 3.4 to 5.5 years [33, 34]. The differences in the lengths of time for development of osteonecrosis might be due to the high doses of steroids used in SARS patients, with an average total dose of 4.6 g in a mean treatment period of 30 days. Additionally, the discrepancies between the studies might also be due to recent increases in the use of MRI for the diagnosis of early-stage osteonecrosis, which may have otherwise been undetectable by a radiographic assessment. Saito et al. [35] reported that osteonecrosis was closely associated with total steroid dose, and they detected occurrences of osteonecrosis within 2 weeks after renal-transplant surgery. They argued that MRI has a high sensitivity and specificity for the diagnosis of osteonecrosis compared with a radiographic examination. Therefore, both high-dose steroid usage and MRI use probably contributed to the earlier detection of osteonecrosis in SARS patients.
Our sensitivity analysis showed that the results of our study were robust after excluding the studies with extreme outcomes. However, the heterogeneity between studies was relatively high for the cumulative dose and treatment duration of steroids.
Limitations
Our studies had limitations. The total number of SARS patients was approximately 8098, and 764 patients died during the SARS outbreak in 2003. However, only about one-seventh of the patients had a follow-up MRI examination and were administered steroid therapy regimens, which constituted a major limitation. Because the number of participants depended mainly on the responses of the SARS patients to the follow-up visits, some of the individual studies had only a small sample size, which might pose a risk of bias. Additionally, a detection bias might exist for those who received higher doses, as they may have been more likely to undergo testing.
Conclusions
Our meta-analysis pooled the data from 1137 recovered SARS patients to determine whether the steroid dose and treatment duration were associated with osteonecrosis. Our findings provide obvious evidence of a non-linear relationship between osteonecrosis and the cumulative dose and treatment duration of steroids. The non-linear regression indicated that steroid therapy with a cumulative dose of methylprednisolone <5 g and a treatment duration <30 days resulted in a relatively low risk of development of osteonecrosis. The subgroup analysis demonstrated that there were no sex differences in the development of steroid-induced osteonecrosis between male and female patients. Summarily, the present findings indicate that the cumulative dose and treatment duration of steroids are important risk factors for the development of osteonecrosis in SARS patients.
References
Lamberts SW, Bruining HA, de Jong FH (1997) Corticosteroid therapy in severe illness. N Engl J Med 337:1285–1292
Boland EW, Headley NE (1950) Management of rheumatoid arthritis with smaller (maintenance) doses of cortisone acetate. J Am Med Assoc 144:365–372
Freyberg RH, Traeger CH, Patterson M, Squires W, Adams CH (1951) Problems of prolonged cortisone treatment for rheumatoid arthritis; further investigations. J Am Med Assoc 147:1538–1543
Powell C, Chang C, Naguwa SM, Cheema G, Gershwin ME (2010) Steroid induced osteonecrosis: an analysis of steroid dosing risk. Autoimmun Rev 9:721–743
Weinstein RS (2012) Glucocorticoid-induced osteonecrosis. Endocrine 41:183–190
Assouline-Dayan Y, Chang C, Greenspan A, Shoenfeld Y, Gershwin ME (2002) Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum 32:94–124
Chan-Yeung M, Ooi GC, Hui DS, Ho PL, Tsang KW (2003) Severe acute respiratory syndrome. The International Journal of Tuberculosis and Lung Disease: the Official Journal of the International Union Against Tuberculosis and Lung Disease 7:1117–1130
Ho JC, Ooi GC, Mok TY et al (2003) High-dose pulse versus nonpulse corticosteroid regimens in severe acute respiratory syndrome. Am J Respir Crit Care Med 168:1449–1456
Guo KJ, Zhao FC, Guo Y, Li FL, Zhu L, Zheng W (2014) The influence of age, gender and treatment with steroids on the incidence of osteonecrosis of the femoral head during the management of severe acute respiratory syndrome: a retrospective study. The Bone Joint J 96-B:259–262
Wu LH, Gao C, Wang GZ, Yang L, Hou XM, Ge H, Xia CQ, Qi M (2006) Clinical study on the relate marker of blood coagulation in the patients with avascular necrosis of the femoral head after treatment of severe acute respiratory syndrome with methylprednisolone. Chinese J Nautical Med Hyperbaric Med 13:39–41
Dong WQ, Bai B, Lin YP, Zeng QS (2007) Case control study of avascular necrosis of femoral head during SARS patients’ convalescence. Chinese J Postgraduates of Med 30:1–3
Gao HS, Wang SX, Gao X, Cao X, Hui WL, Li YM, Yang Z, Su B (2005) Nested case-control study of avascular necrosis of femoral head during SARS patients’convalescence. Acta Academiae Medicinae CPAPF 14:11–13
Griffith JF, Antonio GE, Kumta SM et al (2005) Osteonecrosis of hip and knee in patients with severe acute respiratory syndrome treated with steroids. Radiology 235:168–175
Han YK, Zhou XZ, Zeng Z et al (2005) Osteonecrosis in post-SARS patients: a clinical study. Chinese J Nosocomiol 15:481–484
Liu BL, Li ZR, Sun W, Zhao FC (2009) The relationship of the range and location of osteonecrosis of the femoral head with the dose of steroid in SARS patients. Chin J Orthop 29:554–557
Lv H, de Vlas SJ, Liu W, Wang TB, Cao ZY, Li CP, Cao WC, Richardus JH (2009) Avascular osteonecrosis after treatment of SARS: a 3-year longitudinal study. Tropical Med Int Health: TM & IH 14(Suppl 1):79–84
Wang HY (2011) The investigation of the SARS patients with ANFH in Beijing Ditan Hospital. Taishan Medical Institute, Taian, pp 1–52
Wang ZQ, Liu TS, Wang JG (2006) The clinical research of the SARS patients diagnosed with femur head necrosis. Tianjin Med J 34:50–51
Xu J, Yu XZ (2004) A study on correlativity between glucocorticoids and femoral head necrosis in patients with severe acute respiratory syndrome. Chinese J Emerg Med 13:697–699
Zhang NF, Li ZR, Wei HY, Liu ZH, Hernigou P (2008) Steroid-induced osteonecrosis: the number of lesions is related to the dosage. J Bone Joint Surg Brit Vol 90:1239–1243
Cheng XG, Qu H, Liu W, Liu X, Cheng KB, Zhao T, Li XS, Liang W, Guo J (2005) The prevalence of osteonecrosis in severe acute respiratory syndrome patients: an MRI screening study. Chin J Radiol 39:791–797
Cheng XG, Qu H, Liu W, Sun J, Cheng KB, Feng SC, Li XS (2004) MRI screening on bone ischemia of hip and knee in recovered SARS patients. Chinese J Radiol 38:230–235
Chen WH, Zhang Q, Liu DB, Zhang HM, Zhang L, Gu LJ, Sun G, Zhao TJ, Zhou W (2004) Analysis of attacking characteristics and clinical significant about osteonecrosis of the femoral head secondary to SARS. China J Orthopaedics Traumatol 17:388–390
Felson DT, Anderson JJ (1987) Across-study evaluation of association between steroid dose and bolus steroids and avascular necrosis of bone. Lancet 1:902–906
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 151:264–269 W264
Wang Z, Liu T, Wang J (2007) The clinical research of the SARS patients diagnosed with Femur Head Necrosis. Orthopaedic new technology seminar for the police force, Tianjing, pp 190–192
Higgins J, Green S (2008) Cochrane Reviewers’ handbook 5.0.1 (updated September 2008). The Cochrane library. Wiley, Chichester
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Greenland S, Longnecker MP (1992) Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am J Epidemiol 135:1301–1309
Desquilbet L, Mariotti F (2010) Dose-response analyses using restricted cubic spline functions in public health research. Stat Med 29:1037–1057
Nakamura J, Harada Y, Oinuma K, Iida S, Kishida S, Takahashi K (2010) Spontaneous repair of asymptomatic osteonecrosis associated with corticosteroid therapy in systemic lupus erythematosus: 10-year minimum follow-up with MRI. Lupus 19:1307–1314
Shibatani M, Fujioka M, Arai Y, Takahashi K, Ueshima K, Okamoto M, Yoshimura N, Hirota Y, Fukushima W, Kubo T (2008) Degree of corticosteroid treatment within the first 2 months of renal transplantation has a strong influence on the incidence of osteonecrosis of the femoral head. Acta Orthop 79:631–636
Klipper AR, Stevens MB, Zizic TM, Hungerford DS (1976) Ischemic necrosis of bone in systemic lupus erythematosus. Medicine 55:251–257
Zizic TM, Marcoux C, Hungerford DS, Dansereau JV, Stevens MB (1985) Corticosteroid therapy associated with ischemic necrosis of bone in systemic lupus erythematosus. Am J Med 79:596–604
Saito M, Ueshima K, Fujioka M, Ishida M, Goto T, Arai Y, Ikoma K, Fujiwara H, Fukushima W, Kubo T (2014) Corticosteroid administration within 2 weeks after renal transplantation affects the incidence of femoral head osteonecrosis. Acta Orthop 85:266–270
Acknowledgements
This work was supported in part by the Zhejiang Provincial Natural Science Foundation of China under Grant (No. LY14H070001).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Rights and permissions
About this article

Cite this article
Zhao, R., Wang, H., Wang, X. et al. Steroid therapy and the risk of osteonecrosis in SARS patients: a dose-response meta-analysis. Osteoporos Int 28, 1027–1034 (2017). https://doi.org/10.1007/s00198-016-3824-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-016-3824-z