
Abstract
Aims/hypothesis
Lifestyle intervention is effective to prevent type 2 diabetes. However, a considerable long-term non-response occurs to a standard lifestyle intervention. We investigated which risk phenotypes at baseline and their changes during the lifestyle intervention predict long-term glycaemic non-response to the intervention.
Methods
Of 300 participants at high risk for type 2 diabetes who participated in a 24 month lifestyle intervention with diet modification and increased physical activity, 190 participants could be re-examined after 8.7 ± 1.6 years. All individuals underwent a five-point 75 g OGTT and measurements of body fat compartments and liver fat content with MRI and spectroscopy at baseline, 9 and 24 months during the lifestyle intervention, and at long-term follow-up. Fasting proinsulin to insulin conversion (PI/I ratio) and insulin sensitivity and secretion were calculated from the OGTT. Non-response to lifestyle intervention was defined as no decrease in glycaemia, i.e. no decrease in AUC for glucose at 0–120 min during OGTT (AUCglucose0–120 min).
Results
Before the lifestyle intervention, 56% of participants had normal glucose regulation and 44% individuals had impaired fasting glucose and/or impaired glucose tolerance. At long-term follow-up, 11% had developed diabetes. Multivariable regression analysis with adjustment for age, sex, BMI and change in BMI during the lifestyle intervention revealed that baseline insulin secretion and insulin sensitivity, as well as change in insulin sensitivity during the lifestyle intervention, predicted long-term glycaemic control after 9 years. In addition, increased hepatic lipid content as well as impaired fasting proinsulin conversion at baseline were newly detected phenotypes that independently predicted long-term glycaemic control.
Conclusions/interpretation
Increased hepatic lipid content and impaired proinsulin conversion are new predictors, independent of change in body weight, for non-response to lifestyle intervention in addition to the confirmed factors, impaired insulin secretion and insulin sensitivity.
Similar content being viewed by others

Introduction
Lifestyle intervention has repeatedly and conclusively been shown to prevent or postpone the development of type 2 diabetes in high-risk individuals [1,2,3,4,5,6,7,8,9]. Long-term follow-up of several studies has also been reported [4, 6, 7]. The Finnish Diabetes Prevention Study (DPS) showed a relative diabetes risk reduction of up to 38% after 13 years of intervention, compared with a control group [7]. The Diabetes Prevention Program (DPP) study and the Da Qing Diabetes Prevention study also showed a significant reduction in diabetes risk (34–43%) compared with the control group, lasting for 10 to 20 years after the lifestyle intervention [4, 6].
However, the effectiveness of a standard lifestyle intervention on glucose metabolism is highly variable, and a substantial number of participants develop diabetes [1, 3, 10]. Impaired insulin secretion as well as insulin resistance are well-established pathophysiological mechanisms in the development of type 2 diabetes [11,12,13,14]. Recently, we found that, besides baseline impaired insulin secretion, the presence of an insulin-resistant fatty liver is an important predictor of the short-term response to a standard lifestyle intervention [15]. Sufficient data are still lacking to elucidate the contribution of fatty liver to the long-term effects of a lifestyle intervention [11].
It is well accepted that, besides baseline insulin sensitivity and insulin secretion, the changes in these variables during a lifestyle intervention may play a role in its success [16,17,18,19].
Perreault et al showed in the US Diabetes Prevention Program Outcome Study (DPPOS) that the regression from impaired fasting glucose (IFG) and/or impaired glucose tolerance (IGT) to a normal glucose regulation, which was strongly associated with improvement of BMI and insulin sensitivity during the lifestyle intervention, was strongly associated with a reduced incidence of diabetes [20, 21].
It is well accepted that fasting proinsulin, proinsulin to insulin conversion (PI/I ratio) and proinsulin to C-peptide ratio are predictors of the incidence of type 2 diabetes [22,23,24,25,26,27,28,29,30]. It is of great interest that lifestyle intervention in individuals with IFG and/or IGT seems to have only a slight influence on insulin secretion [31, 32]. One aspect of beta cell dysfunction in addition to insulin secretion is the conversion of proinsulin to insulin (PI/I ratio); where the conversion is adversely affected, the ratio increases and the individual develops hyperproinsulinaemia [33]. An increased fasting PI/I ratio, indicating impaired proinsulin conversion, has been observed in individuals with IGT and type 2 diabetes [34, 35]. Data on the impact of lifestyle intervention on fasting PI/I ratio are rare [36,37,38], but those available indicate that proinsulin conversion is improved after lifestyle intervention.
The Tübingen Lifestyle Intervention Program (TULIP; trial registration number KFO 114 [http://gepris.dfg.de/gepris/projekt/5396893?language=en]) was initiated in 2003 in a population at high risk for type 2 diabetes in Germany. All participants underwent a 24 month lifestyle intervention programme. One unique feature of the TULIP study is that participants repeatedly underwent whole-body MRI and 1H magnetic resonance spectroscopy (1H-MRS) before the lifestyle intervention and at the follow-up visits. This allows for the first time the precise assessment of liver fat content and body fat composition (total adipose tissue [TAT], visceral adipose tissue [VAT], subcutaneous adipose tissue [SCAT]) before, during and after the lifestyle intervention [10, 39,40,41].
We have performed a long-term follow-up of participants from the TULIP study, with the aim of identifying the risk phenotypes at baseline and changes during the lifestyle intervention that predict the long-term glycaemic non-response to the intervention. This information is important to identify early those individuals who will probably not benefit from lifestyle intervention and offer them alternative treatment.
Methods
Participants and study design
Individuals at high risk for type 2 diabetes from the southern part of Germany participated in TULIP, a prospective uncontrolled intervention study. They were included in the study when they fulfilled at least one of the following criteria: a family history of type 2 diabetes; BMI > 27 kg/m2; IGT (blood glucose ≥ 7.78 mmol/l); or previous diagnosis of gestational diabetes. Exclusion criteria were the diagnosis of diabetes mellitus or the presence of a severe critical mental or physical illness. Informed written consent was obtained from all participants and the local medical ethics committee approved the protocol.
A total of 413 individuals were included. At baseline, medical history was obtained and a physical examination performed. Phenotypic characterisation was performed using a 75 g OGTT, whole-body MRI and 1H-MRS, as well as a cycle exercise test (see below). These examinations were repeated at 9 and 24 months, and after the long-term follow-up period of about 9 years.
After the baseline examination, all participants underwent 15 sessions of standardised individual face-to-face dietary counselling by trained diabetes educators. In the first 9 months of intervention, i.e. the intensive lifestyle intervention phase of the study, monthly visits were scheduled. The moderate maintenance phase of the lifestyle intervention, comprising 3-monthly visits, lasted from the ninth month until the end of the second year.
Counselling aimed to reduce body weight by ≥ 5%. Furthermore, participants were recommended to reduce the energy intake from fat to < 30% of total energy consumed, and to increase dietary fibre intake to at least 15 g/4185 kJ (1000 kcal). They were also encouraged to reduce the intake of saturated fatty acids to < 10% of total fat. During each visit, participants presented a 3 day food diary and discussed it with the dietitians. Diet composition was estimated with a validated software, using two representative days of the 3 day diary (DGE-PC 3.0; Deutsche Gesellschaft für Ernährung, Bonn, Germany). Individuals were motivated to perform at least 3 h moderate exercise per week. A heart rate monitor (Polar, Büttelbronn, Germany) was given to the participants and they were instructed to exercise so that their heart rate was just below their individual anaerobic threshold. Individual anaerobic threshold was measured by a motorised treadmill (Saturn, HP-Cosmos, Traunstein, Germany).
OGTT
All individuals underwent a frequently sampled 75 g OGTT at baseline, after 9 months, after 24 months and at the long-term follow-up appointment. For the determination of plasma glucose and insulin levels, venous blood samples were obtained at 0, 30, 60, 90 and 120 min. Plasma glucose was measured using a bedside glucose analyser (YSI, Yellow Springs, CO, USA). AUC for glucose at 0–120 min during OGTT (AUCglucose0–120 min) was calculated with the trapezoid method. Plasma insulin and C-peptide were determined by an immunoassay with the ADVIA Centaur XP Immunoassay System (Siemens Healthcare Diagnostics, Erlangen, Germany).
Serum proinsulin concentrations were measured using a microparticle enzyme immunoassay (IBL, Hamburg, Germany) on a BEP III System (Siemens Healthcare, Erlangen, Germany). The proinsulin assay measures intact proinsulin and has 0% cross-reactivity with human insulin and C-peptide. There is cross-reactivity with the relevant proinsulin split products: des-31,32-proinsulin, 0.9%; des-32,33-proinsulin, 1.5%; des-64,65-proinsulin, 53%; and des-65,66-proinsulin, 55% [42]. Insulin sensitivity was calculated from glucose and insulin values during the OGTT as proposed by Matsuda and DeFronzo (i.e. to calculate the insulin sensitivity index [ISI]) [43]. Insulin secretion was estimated using the insulinogenic index (IGI) across 30 min (IGI0–30 min), calculated as Ins30−Ins0/Glc30−Glc0, where Ins0 and Glc0 is insulin and glucose at 0 min, and Ins30 and Glc30 is insulin and glucose at 30 min [17]. The relative insulin secretion (disposition index), which describes the insulin secretion relative to insulin sensitivity, was calculated as ISI × IGI0–30 min [17]. Fasting proinsulin to insulin conversion was determined by dividing proinsulin0 min by insulin0 min (PI/I ratio), where proinsulin0 min is proinsulin at 0 min and insulin0 min is insulin at 0 min. Fasting proinsulin to C-peptide ratio was determined by dividing proinsulin0 min by C-peptide at 0 min (C-peptide0 min) [28].
T1-weighted MRI to measure body fat
Determination of whole-body fat distribution was performed using an axial T1-weighted fast spin echo technique as previously described using a 1.5 T whole-body imager (Magnetom Sonata, Siemens Medical Solutions, Erlangen, Germany) [14, 40].
1H-MRS to measure intrahepatic fat content
Liver fat content was quantified by localised 1H-MRS as previously described [14, 40]. Non-alcoholic fatty liver disease (NAFLD) was defined as liver fat content ≥ 5.56% [44].
Maximal oxygen consumption
The individuals underwent a continuous, incremental exercise test on a cycle ergometer to volitional exhaustion. The cycle ergometer test was performed on an electromagnetically braked cycle ergometer (Ergometrics 800 S; Ergoline, Bitz, Germany). Oxygen consumption was measured using spiroergometry (Cortex MetaLyzer, Metasoft 3.9, Leipzig, Germany). Maximal oxygen consumption (\( \overset{\cdot }{V}{\mathrm{O}}_{2\max } \)) is expressed as \( \overset{\cdot }{V}{\mathrm{O}}_{2\max } \) per kg lean body mass (ml min−1 kg−1).
Statistical analyses
The primary endpoint of the study was change in AUCglucose0–120 min (response/non-response to lifestyle intervention). Data are given as mean ± SE. A Wilcoxon-signed-rank test was used to compare variables before and after lifestyle intervention and during long-term follow-up. Prior to multivariable regression analyses, variable distributions were tested for normality using the Shapiro–Wilk test. Non-normally distributed variables were transformed to their natural logarithm. To identify key model determinants, forward stepwise multivariable linear regression analyses were performed. A p value ≤ 0.05 was considered statistically significant. The software package JMP 11 (SAS Institute, Cary, NC, USA) was used for all other analyses.
Results
Longitudinal results
A total of 413 participants were enrolled in the study, with 357 undertaking 9 months of intensive lifestyle intervention, and 300 completing the full intervention in the 24 month study after (Fig. 1). We invited these 300 participants, via written invitation or telephone call, to a long-term follow-up visit; 190 individuals (63.3%) attended after a mean total follow-up time (time between baseline and long-term follow-up) of 8.7 ± 1.6 years (Fig. 1). The main reason for not participating in the long-term follow-up was unknown address or loss to follow-up (Fig. 1). Table 1 shows the participant characteristics during the four visits. After 9 months of intervention, AUCglucose0–120 min values improved in 63% of the participants (responders). This ratio of responders was decreased at the long-term follow-up to 43%. At the long-term follow-up, 46% of the 190 participants had a normal glucose regulation (normal glucose tolerance and normal fasting glucose), 43% participants had IFG and/or IGT and 21 participants (11%) developed diabetes (Fig. 2).

Trial profile of the TULIP study: screening, enrolment and post-intervention follow-up period (8.7 ± 1.6 years)

Progression of glycaemic status from baseline to long-term follow-up. Data are given as percentages. n = 190 participants. Black, baseline; light grey, 9 months of lifestyle intervention; dark grey, 24 months of lifestyle intervention; white, long-term follow-up. NGR, normal glucose regulation; T2DM, type 2 diabetes mellitus
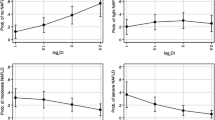
Among the 190 participants who attended all visits, fasting and postprandial plasma glucose levels, insulin sensitivity, the disposition index, fasting proinsulin, fasting insulin and fasting PI/I ratio improved during the 9 month intensive period of the lifestyle intervention. Body weight, liver fat content, TAT, SCAT and VAT decreased (Table 2, Fig. 3).

Progression of metabolic variables and fat compartments from baseline to the long-term follow-up. Data are given as mean ± SE. AUCglucose0–120 min during OGTT (a), ISI (b), insulin secretion (disposition index [ISI × IGI0–30 min]) (c), liver fat content (d), VAT (e) and fasting PI/I ratio (f) at baseline, after 9 months and 24 months of lifestyle intervention and at long-term follow-up; LT, long-term follow-up
Comparing the baseline with the long-term follow-up variables after 9 years, fasting PI/I ratio and fasting proinsulin improved from baseline to long-term follow-up (both p ≤ 0.0001), while post-challenge (2 h) plasma glucose, AUCglucose0–120 min during the OGTT and liver fat content did not change significantly. In contrast, fasting glucose levels increased and insulin sensitivity, as well as the disposition index, decreased significantly. Furthermore, body weight, TAT, SCAT, VAT and fasting insulin increased with the concomitant deterioration of cardiorespiratory fitness during this period (all p ≤ 0.05, Table 2, Fig. 3).
Impact of body weight change during the first 9 months of lifestyle intervention on long-term success
Decrease in body weight during the lifestyle intervention was found to associate with the success of the lifestyle intervention to improve glycaemia [3, 4, 16]. We therefore performed multivariable linear regression analysis with change in BMI during the intensive period of the lifestyle intervention as effect variable and AUCglucose0–120 min levels at long-term follow-up as the dependent variable. The model was additionally adjusted for sex, age, follow-up time, AUCglucose0–120 min and BMI at baseline. The change in BMI during the intensive period of the lifestyle intervention was associated with the AUCglucose0–120 min level in long-term follow-up (β = 0.206, p = 0.0006; Table 3, model 1).
Impact of insulin sensitivity and insulin secretion on long-term success of the lifestyle intervention
Insulin secretion and insulin sensitivity are important pathophysiological factors in the pathogenesis of type 2 diabetes [11]. Therefore, these variables and the change of both during the intensive phase of lifestyle intervention were added to model 1. As shown in Table 3 (model 2), the baseline insulin secretion (β = −0.436, p ≤ 0.0001) and insulin sensitivity (β = −0.405, p = 0.0009) and the change in insulin sensitivity (β = −0.230, p = 0.0015), were associated with the AUCglucose0–120 min level at the long-term follow-up.
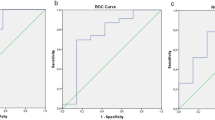
To visualise the effect of baseline insulin secretion on the cumulative probability of not developing diabetes, Kaplan–Meier survival curves were generated. Not a single diabetes case was diagnosed in individuals with a low disposition index compared with a high disposition index at baseline (Fig. 4a).

Cumulative probability of not developing type 2 diabetes and prediction models. (a) Cumulative probability of not developing type 2 diabetes in the TULIP study in a group with a high (dashed line) or low (solid line) disposition index at baseline, according to whether they were above or below the median. Logrank test, p < 0.0001. (b) Cumulative probability of not developing type 2 diabetes in the TULIP study in a group with (solid line) or without NAFLD (dashed line) at baseline (cut-off point, 5.56% liver fat). Logrank test, p = 0.0094
Impact of hepatic lipid content on the long-term success of the lifestyle intervention
In a next step, hepatic lipid content at baseline and change in content during the intensive phase of the lifestyle intervention were added to the model (Table 3, model 3). Hepatic lipid content at baseline (β = 0.231, p = 0.0207) predicted AUCglucose0–120 min at long-term follow-up, in addition to baseline insulin secretion, change in insulin sensitivity and age.
To visualise the effect of baseline hepatic lipid content on the cumulative probability of not developing diabetes, Kaplan–Meier survival curves were generated. In participants with or without NAFLD, individuals without NAFLD at baseline had a significantly lower risk for developing diabetes compared with individuals with NAFLD (logrank test, p = 0.0094) (Fig. 4b).
Impact of fasting proinsulin to insulin conversion on the long-term success of the lifestyle intervention
Proinsulin conversion has been shown to have an impact on diabetes risk [34, 35]. Therefore, the fasting PI/I ratio at baseline and the change in the fasting PI/I ratio during the intensive phase of the lifestyle intervention were added to model 3. The baseline fasting PI/I ratio predicted the long-term AUCglucose0–120 min (β = 0.204, p = 0.0444), in addition to the baseline insulin secretion and the change in insulin sensitivity during the intensive phase of the lifestyle intervention. There is an inverse correlation of fasting PI/I ratio and hepatic lipid content (β = − 0.208, p = 0.0213), thus, the impact of liver fat was no longer significant in this model. Of note, model 4 gave the highest r 2 value for glucose levels at long-term follow-up, explaining 59% of variability in AUCglucose0–120 min. Furthermore, the ratio of proinsulin to C-peptide impacts similarly on long-term glycaemia as the PI/I ratio (see electronic supplementary material [ESM] Table 1).
Discussion
This long-term follow-up analysis of a standard lifestyle intervention programme aiming at preventing type 2 diabetes provides three major results: first, we show, for the first time, data on the long-term development of body fat composition and ectopic fat deposition in the liver, together with changes in insulin sensitivity and insulin secretion following a lifestyle intervention. Second, we show that the long-term success in maintaining glycaemia can be inferred from baseline variables and short-term response to the lifestyle intervention. Third, we identified a baseline high-risk phenotype for the long-term glycaemic non-response that includes, besides impaired insulin secretion and insulin sensitivity, fatty liver or impaired fasting proinsulin conversion.
Recent studies have shown that a lifestyle intervention is effective in preventing or delaying the development of type 2 diabetes during both short- and long-term follow-up [3,4,5,6,7, 45, 46]. The lifestyle changes comprised several beneficial changes in diet, as well as increased physical activity, with beneficial effects on blood glucose levels and a significant reduction in diabetes incidence [3, 45]. The TULIP intervention was most intensive during the first 9 months. Consequently, the benefit was most prominent during this time. Body weight reduction during the intensive period was moderate, as observed in two other studies including individuals with IGT [3, 45].
Using whole-body MRI, we observed a marked reduction in major body fat compartments (TAT, VAT and SCAT) between 10% and 15% during the first 9 months of intensive intervention. Importantly, liver fat content improved by more than 30% during that period. This ‘qualified’ weight reduction with decreases in visceral fat mass and liver fat content improved insulin sensitivity by nearly 15%. These risk factors are known to be associated with metabolically unhealthy obesity [47]. VAT and intrahepatic fat are the source of several hormones and cytokines that act against insulin and initiate a chronic systemic activation of the immune system. This chronic systemic inflammation is the key driver for further impairment of insulin resistance and also for the chronic progressive nature of the disease [48]. Lifestyle interventions can only modulate disease development if there is an impact on the hormonal activity of the body fat compartments and not just on the volume of body fat [49].
In contrast to the favourable short-term effects of a lifestyle intervention, the improvements in metabolic variables are lost over time when body weight and body fat composition, as well as insulin sensitivity and insulin secretion, deteriorate. Despite gain in body weight and body fat, postprandial blood glucose levels and liver fat content were comparable with baseline levels, even after 9 years (Table 2, Fig. 3). One important variable that improved during the lifestyle intervention and was improved at long-term follow-up was fasting proinsulin conversion. As fasting insulin was doubled at long-term follow-up compared with baseline and C-peptide was unchanged, this indicates declining hepatic insulin clearance over this time (9 years), suggesting improved proinsulin conversion. Fasting proinsulin levels also decreased by ~ 50%, also indicating that proinsulin conversion was improved.
In addition, it should be highlighted that a rate of 11% incident diabetes is rather low compared with similar lifestyle intervention programmes. In the lifestyle intervention group of the Finnish DPS and the US DPPOS, 29% and 40% of participants, respectively, developed diabetes during the long-term follow-up [4, 7]. This might in part be because both studies exclusively included participants with IGT at baseline, while the TULIP study included a metabolically healthier cohort. Taken together, our results are in line with earlier studies showing that healthy changes in diet and increased exercise can have beneficial long-term effects on glycaemia, and offer encouraging evidence for the effectiveness of a lifestyle intervention, even without a large reduction in body weight [4, 6, 7, 20].
Nevertheless, the problem of non-response with respect to an improvement of glycaemia during the lifestyle intervention in a substantial number of participants remains [4, 6, 7, 20]. It is, therefore, clinically important to define risk factors and risk phenotypes associated with such a non-response.
One factor might be the decrease in insulin sensitivity that is correlated with the amount of weight loss [19]. However, the correlation of weight loss and glycaemia is not very strong [15]. Paradoxically, in the US DPPOS a stronger weight loss even adversely affected diabetes risk, independent of the previous intervention [20]. Thus, other metabolic determinants may additionally affect the long-term effectiveness of a lifestyle intervention. In the present study, we addressed the pathophysiological determinants that predict non-response to the lifestyle intervention. We were able to show that low insulin secretion capacity at baseline, low insulin sensitivity and impaired improvement in insulin sensitivity during the intensive first 9 months of the lifestyle intervention predicted non-response to the intervention. These findings accord with previous studies that have shown that both baseline insulin secretion and insulin sensitivity, as well as the change thereof during a lifestyle intervention, are predictors of diabetes development [16, 19, 50] or, vice versa, regression to normal glucose tolerance [20, 21].
A new finding was that a high liver fat content at baseline or an impaired fasting relative proinsulin to insulin conversion at baseline were important determinants of impaired glycaemia at long-term follow-up, independent of insulin secretion and insulin sensitivity. Models containing these pathophysiological factors provided a better prediction (r 2 = 0.55 and 0.59, respectively) of long-term glycaemia than a simpler model containing baseline BMI as well as change in BMI (r 2 = 0.45) (Table 3).
The conversion of proinsulin to insulin is thought to be a biomarker for beta cell function [26, 51, 52]. It is important that in the present study proinsulin to insulin conversion predicted long-term glycaemia after the lifestyle intervention, independently of insulin secretion and insulin sensitivity (model 4). Our results are in line with earlier studies that showed that increased proinsulin levels, which are the consequence of impaired proinsulin conversion to insulin, predict worsening of glucose tolerance status [53, 54]. Furthermore, it has been shown that fasting proinsulin conversion and the acute insulin response independently impact on the development of type 2 diabetes [27, 55] highlighting that there are multiple aspects to beta cell dysfunction. In this context, the improvement of proinsulin to insulin conversion after the lifestyle intervention and at the long-term follow-up is an important finding. One may speculate that proinsulin conversion is a useful biomarker for both the prediction of diabetes risk and monitoring the success of the lifestyle intervention.
For the design, development and practice of improved and more successful lifestyle intervention programmes, it is important to reveal risk factors for short- and long-term success of a lifestyle intervention. Regarding short-term success, we previously found that the phenotype encompassing participants with a low disposition index or insulin-resistant NAFLD have a high risk for acute glycaemic non-response to lifestyle intervention [15]. The present study now demonstrates that such a phenotype is also associated with long-term non-response and extends the phenotype to impaired proinsulin conversion. Individuals with such a high-risk phenotype may be put on a more intensive lifestyle intervention at an earlier stage, or even receive pharmacological therapy.
One limitation of the present analysis is that the TULIP study was designed as an uncontrolled study. Therefore, we cannot compare the risk of non-response to the lifestyle intervention (i.e. improvement in glycaemia) with the risk of developing diabetes without intervention. However, a lifestyle intervention is standard care in individuals at high risk for type 2 diabetes [56] after the publication of the landmark studies, the DPS and DPP, and thus, a non-treated control group seems inappropriate. Furthermore, our study was conducted at a single academic research centre and the results cannot probably be generalised to other populations.
In conclusion, we found that, independent of the important change in body weight, an impaired insulin secretion, a fatty liver or an impaired fasting proinsulin conversion before lifestyle intervention predicted glycaemic non-response to the lifestyle intervention programme. Our current results may help to develop individualised prevention programmes targeting those with at-risk phenotypes. Furthermore, they may also aid monitoring during such programmes and may help to identify those for whom treatment intensification will be necessary.
Abbreviations
- AUCglucose0–120 min :
-
AUC for glucose at 0–120 min during OGTT
- DPP:
-
Diabetes Prevention Program
- DPPOS:
-
Diabetes Prevention Program Outcome Study
- DPS:
-
Diabetes Prevention Study
- 1H-MRS:
-
Proton magnetic resonance spectroscopy
- IFG:
-
Impaired fasting glucose
- IGT:
-
Impaired glucose tolerance
- IGI:
-
Insulinogenic index
- ISI:
-
Insulin sensitivity index
- NAFLD:
-
Non-alcoholic fatty liver disease
- PI/I ratio:
-
Proinsulin/insulin ratio
- SCAT:
-
Subcutaneous adipose tissue
- TAT:
-
total adipose tissue
- TULIP:
-
Tübingen Lifestyle Intervention Program
- VAT:
-
Visceral adipose tissue
References
Tuomilehto J, Lindström J, Eriksson JG et al (2001) Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 344:1343–1350
Lindström J, Ilanne-Parikka P, Peltonen M et al (2006) Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: follow-up of the Finnish Diabetes Prevention Study. Lancet 368:1673–1679
Knowler WC, Barrett-Connor E, Fowler SE et al (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346:393–403
Diabetes Prevention Program Research Group, Knowler WC, Fowler SE et al (2009) 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet 374:1677–1686
Pan XR, Li GW, Hu YH et al (1997) Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care 20:537–544
Li G, Zhang P, Wang J et al (2008) The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up study. Lancet 371:1783–1789
Lindström J, Peltonen M, Eriksson JG et al (2013) Improved lifestyle and decreased diabetes risk over 13 years: long-term follow-up of the randomised Finnish Diabetes Prevention Study (DPS). Diabetologia 56:284–293
Ramachandran A, Snehalatha C, Mary S et al (2006) The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1). Diabetologia 49:289–297
Schwarz PE, Greaves CJ, Lindström J et al (2012) Nonpharmacological interventions for the prevention of type 2 diabetes mellitus. Nat Rev Endocrinol 8:363–373
Kantartzis K, Thamer C, Peter A et al (2009) High cardiorespiratory fitness is an independent predictor of the reduction in liver fat during a lifestyle intervention in non-alcoholic fatty liver disease. Gut 58:1281–1288
Häring H-U (2016) Novel phenotypes of prediabetes? Diabetologia 59:1806–1818
Ferrannini E (2014) Definition of intervention points in prediabetes. Lancet Diabetes Endocrinol 2:667–675
Kahn SE, Cooper ME, Del Prato S (2014) Pathophysiology and treatment of type 2 diabetes: perspectives on the past, present, and future. Lancet 383:1068–1083
Stefan N, Fritsche A, Schick F, Häring H-U (2016) Phenotypes of prediabetes and stratification of cardiometabolic risk. Lancet Diabetes Endocrinol 4:789–798
Stefan N, Staiger H, Wagner R et al (2015) A high-risk phenotype associates with reduced improvement in glycaemia during a lifestyle intervention in prediabetes. Diabetologia 58:2877–2884
Kitabchi AE, Temprosa M, Knowler WC et al (2005) Role of insulin secretion and sensitivity in the evolution of type 2 diabetes in the diabetes prevention program: effects of lifestyle intervention and metformin. Diabetes 54:2404–2414
Abdul-Ghani MA, Williams K, DeFronzo RA, Stern M (2007) What is the best predictor of future type 2 diabetes? Diabetes Care 30:1544–1548
Lyssenko V, Almgren P, Anevski D et al (2005) Predictors of and longitudinal changes in insulin sensitivity and secretion preceding onset of type 2 diabetes. Diabetes 54:166–174
de Mello VDF, Lindström J, Eriksson J et al (2012) Insulin secretion and its determinants in the progression of impaired glucose tolerance to type 2 diabetes in impaired glucose-tolerant individuals: the Finnish Diabetes Prevention Study. Diabetes Care 35:211–217
Perreault L, Pan Q, Mather KJ et al (2012) Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: results from the Diabetes Prevention Program Outcomes Study. Lancet 379:2243–2251
Perreault L, Kahn SE, Christophi CA et al (2009) Regression from pre-diabetes to normal glucose regulation in the diabetes prevention program. Diabetes Care 32:1583–1588
Wareham NJ, Byrne CD, Williams R et al (1999) Fasting proinsulin concentrations predict the development of type 2 diabetes. Diabetes Care 22:262–270
Pfützner A, Kunt T, Hohberg C et al (2004) Fasting intact Proinsulin is a highly specific predictor of insulin resistance in type 2 diabetes. Diabetes Care 27:682–687
Mykkänen L, Zaccaro DJ, Hales CN et al (1999) The relation of proinsulin and insulin to insulin sensitivity and acute insulin response in subjects with newly diagnosed type II diabetes: the Insulin Resistance Atherosclerosis Study. Diabetologia 42:1060–1066
Bergman RN, Finegood DT, Kahn SE (2002) The evolution of β-cell dysfunction and insulin resistance in type 2 diabetes. Eur J Clin Investig 32:35–45
Kahn SE (2000) The importance of the beta-cell in the pathogenesis of type 2 diabetes mellitus. Am J Med 108(Suppl 6a):2S–8S
Hanley AJG, D’Agostino R, Wagenknecht LE et al (2002) Increased proinsulin levels and decreased acute insulin response independently predict the incidence of type 2 diabetes in the Insulin Resistance Atherosclerosis Study. Diabetes 51:1263–1270
Loopstra-Masters RC, Haffner SM, Lorenzo C et al (2011) Proinsulin-to-C-peptide ratio versus proinsulin-to-insulin ratio in the prediction of incident diabetes: the Insulin Resistance Atherosclerosis Study (IRAS). Diabetologia 54:3047–3054
Zethelius B, Byberg L, Hales CN et al (2003) Proinsulin and acute insulin response independently predict type 2 diabetes mellitus in men—report from 27 years of follow-up study. Diabetologia 46:20–26
Pfützner A, Pfützner AH, Larbig M, Forst T (2004) Role of intact Proinsulin in diagnosis and treatment of type 2 diabetes mellitus. Diabetes Technol Ther 6:405–412
Uusitupa M, Lindi V, Louheranta A et al (2003) Long-term improvement in insulin sensitivity by changing lifestyles of people with impaired glucose tolerance: 4-year results from the Finnish Diabetes Prevention Study. Diabetes 52:2532–2538
Yoshioka N, Kuzuya T, Matsuda A, Iwamoto Y (1989) Effects of dietary treatment on serum insulin and Proinsulin response in newly diagnosed NIDDM. Diabetes 38:262–266
Kahn SE, Halban PA (1997) Release of incompletely processed proinsulin is the cause of the disproportionate proinsulinemia of NIDDM. Diabetes 46:1725–1732
Røder ME, Porte D, Schwartz RS, Kahn SE (1998) Disproportionately elevated proinsulin levels reflect the degree of impaired B cell secretory capacity in patients with noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab 83:604–608
Larsson H, Ahrén B (1999) Relative Hyperproinsulinemia as a sign of islet dysfunction in women with impaired glucose tolerance. J Clin Endocrinol Metab 84:2068–2074
Hofsø D, Jenssen T, Bollerslev J et al (2011) Beta cell function after weight loss: a clinical trial comparing gastric bypass surgery and intensive lifestyle intervention. Eur J Endocrinol 164:231–238
Ramos JS, Dalleck LC, Borrani F et al (2016) The effect of different volumes of high-intensity interval training on proinsulin in participants with the metabolic syndrome: a randomised trial. Diabetologia 59:2308–2320
McCaffery JM, Jablonski KA, Franks PW et al (2011) TCF7L2 polymorphism, weight loss and proinsulin∶insulin ratio in the diabetes prevention program. PLoS One 6:e21518
Kantartzis K, Machann J, Schick F et al (2011) Effects of a lifestyle intervention in metabolically benign and malign obesity. Diabetologia 54:864–868
Machann J, Thamer C, Stefan N et al (2010) Follow-up whole-body assessment of adipose tissue compartments during a lifestyle intervention in a large cohort at increased risk for type 2 diabetes. Radiology 257:353–363
Haupt A, Thamer C, Heni M et al (2010) Gene variants of TCF7L2 influence weight loss and body composition during lifestyle intervention in a population at risk for type 2 diabetes. Diabetes 59:747–750
Pfützner A, Kunt T, Langenfeld M et al (2005) Clinical and laboratory evaluation of specific chemiluminescence assays for intact and total proinsulin. Clin Chem Lab Med 41:1234–1238
Matsuda M, DeFronzo RA (1999) Insulin sensitivity indices obtained from oral glucose tolerance testing: comparison with the euglycemic insulin clamp. Diabetes Care 22:1462–1470
Szczepaniak LS, Nurenberg P, Leonard D et al (2005) Magnetic resonance spectroscopy to measure hepatic triglyceride content: prevalence of hepatic steatosis in the general population. Am J Physiol Endocrinol Metab 288:E462–E468
Lindström J, Louheranta A, Mannelin M et al (2003) The Finnish Diabetes Prevention Study (DPS): lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care 26:3230–3236
Schellenberg ES, Dryden DM, Vandermeer B et al (2013) Lifestyle interventions for patients with and at risk for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med 159:543–551
Stefan N, Kantartzis K, Machann J et al (2008) Identification and characterization of metabolically benign obesity in humans. Arch Intern Med 168:1609–1616
Hotamisligil GS (2006) Inflammation and metabolic disorders. Nature 444:860–867
Stefan N, Hennige AM, Staiger H et al (2006) α2-Heremans-Schmid glycoprotein/fetuin-A is associated with insulin resistance and fat accumulation in the liver in humans. Diabetes Care 29:853–857
Snehalatha C, Mary S, Selvam S et al (2009) Changes in insulin secretion and insulin sensitivity in relation to the glycemic outcomes in subjects with impaired glucose tolerance in the Indian Diabetes Prevention Programme-1 (IDPP-1). Diabetes Care 32:1796–1801
Ahrén B (2005) Type 2 diabetes, insulin secretion and beta-cell mass. Curr Mol Med 5:275–286
Fritsche A, Madaus A, Stefan N et al (2002) Relationships among age, Proinsulin conversion, and β-cell function in nondiabetic humans. Diabetes 51:S234–S239
Vangipurapu J, Stančáková A, Kuulasmaa T et al (2015) Both fasting and glucose-stimulated proinsulin levels predict hyperglycemia and incident type 2 diabetes: a population-based study of 9,396 Finnish men. PLoS One 10:e0124028
Nijpels G, Popp-Snijders C, Kostense PJ et al (1996) Fasting proinsulin and 2-h post-load glucose levels predict the conversion to NIDDM in subjects with impaired glucose tolerance: the Hoorn study. Diabetologia 39:113–118
Haffner SM, Mykkänen L, Valdez RA et al (1994) Disproportionately increased proinsulin levels are associated with the insulin resistance syndrome. J Clin Endocrinol Metab 79:1806–1810
American Diabetes Association (2016) Prevention or delay of type 2 diabetes. Diabetes Care 39(Suppl 1):S36–S38
Acknowledgements
We thank all the study participants for their cooperation with this project. We gratefully acknowledge the excellent technical assistance of A. Bury, E. Kollmar, A. Vosseler and A. Dessecker (all University of Tübingen, Germany). We further thank J. Machann and F. Schick from the Section for Experimental Radiology for the excellent body imaging and cooperation within the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Data availability
The datasets generated during and/or analysed during the current study are not publicly available because the participants have not granted permission for this. The datasets are available from the corresponding author on reasonable request.
Funding
The study was supported in part by grants from the Deutsche Forschungsgemeinschaft and the German Federal Ministry of Education and Research (BMBF) to the German Centre for Diabetes Research (DZD). The study was supported by a grant of the DZD to AF.
Duality of interest
The study was initiated by the authors and there are no other sponsors other than those acknowledged. The authors declare that there is no duality of interest associated with this manuscript.
Contribution statement
All authors provided substantial contributions to the conception and design, acquisition of data or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content. They all gave final approval of the version to be published. The most important contributions of each author were as follows. VS and AF researched data and wrote the manuscript. RW, CS, LF, KK, AP and MH researched data and edited the manuscript. AF, NS and HUH designed the study, contributed to the discussion and reviewed the manuscript. AF is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Electronic supplementary material
ESM Table 1
(PDF 321 kb)
Rights and permissions
About this article

Cite this article
Schmid, V., Wagner, R., Sailer, C. et al. Non-alcoholic fatty liver disease and impaired proinsulin conversion as newly identified predictors of the long-term non-response to a lifestyle intervention for diabetes prevention: results from the TULIP study. Diabetologia 60, 2341–2351 (2017). https://doi.org/10.1007/s00125-017-4407-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-017-4407-z