
Abstract
Vaccines against SARS-CoV-2, the virus that causes COVID-19, showed high efficacy against symptomatic illness caused by the ancestral strain. Yet recent variants such as Omicron and its sublineages substantially escape vaccine-induced neutralizing antibodies. In response, bivalent mRNA booster vaccines updated to better match the BA.4-5 lineages have been made available. Yet the reactogenicity of these vaccines might negatively impact willingness to receive the booster immunization. While serious side effects following vaccination are rare, mRNA vaccines frequently lead to mild adverse events such as injection site pain, lymphadenopathy, myalgia, and fever. Over-the-counter analgesics might mitigate some of these mild adverse events, but animal models of SARS-CoV-2 infection have shown that non-steroidal anti-inflammatory drugs (NSAIDs) substantially reduce antiviral antibody responses, which are the best correlates of protection against COVID-19. It remains unknown whether these same inhibitory effects are seen in humans after mRNA vaccination. We surveyed 6,010 individuals who received COVID-19 vaccines regarding analgesic use and correlated these results with Spike-specific antibody levels. We found no negative impact of analgesic use on antibody levels, and in fact observed slightly elevated concentrations of anti-Spike antibodies in individuals who used painkillers. Logistic regression analyses demonstrated a higher proportion of those experiencing fatigue and muscle aches between NSAID users and those not taking pain medication, suggesting that the elevated antibody levels were likely associated with inflammation and mild adverse events rather than analgesic use per se. Together, our results suggest no detriment to painkiller use to alleviate symptoms after vaccination against COVID-19.
Messenger RNA (mRNA) vaccines against SARS-CoV-2, the virus that causes COVID-19, showed high efficacy against symptomatic illness caused by the ancestral strain1,2. Yet largely due to viral evolution and escape from neutralizing antibodies, the initial effectiveness of these vaccines has decreased from their peaks, especially against mild symptomatic infections3. In response, bivalent vaccines updated to match the BA.4-5 lineages have been made available in hopes of restoring high levels of protection against SARS-CoV-2 infections and COVID-19, the reactogenicity of these vaccines might negatively impact willingness to receive booster immunizations. While serious side effects following vaccination are rare, mRNA vaccines frequently lead to mild local and systemic adverse events such as injection site pain, lymphadenopathy, myalgia, and fever4,5. Over-the-counter analgesics might mitigate some of these mild adverse events, but animal models of SARS-CoV-2 infection have shown that non-steroidal anti-inflammatory drugs (NSAIDs) substantially reduce antiviral antibody responses6. It remains unknown whether these same inhibitory effects are seen in humans after mRNA vaccination and how different classes of painkillers impact the antibody response.
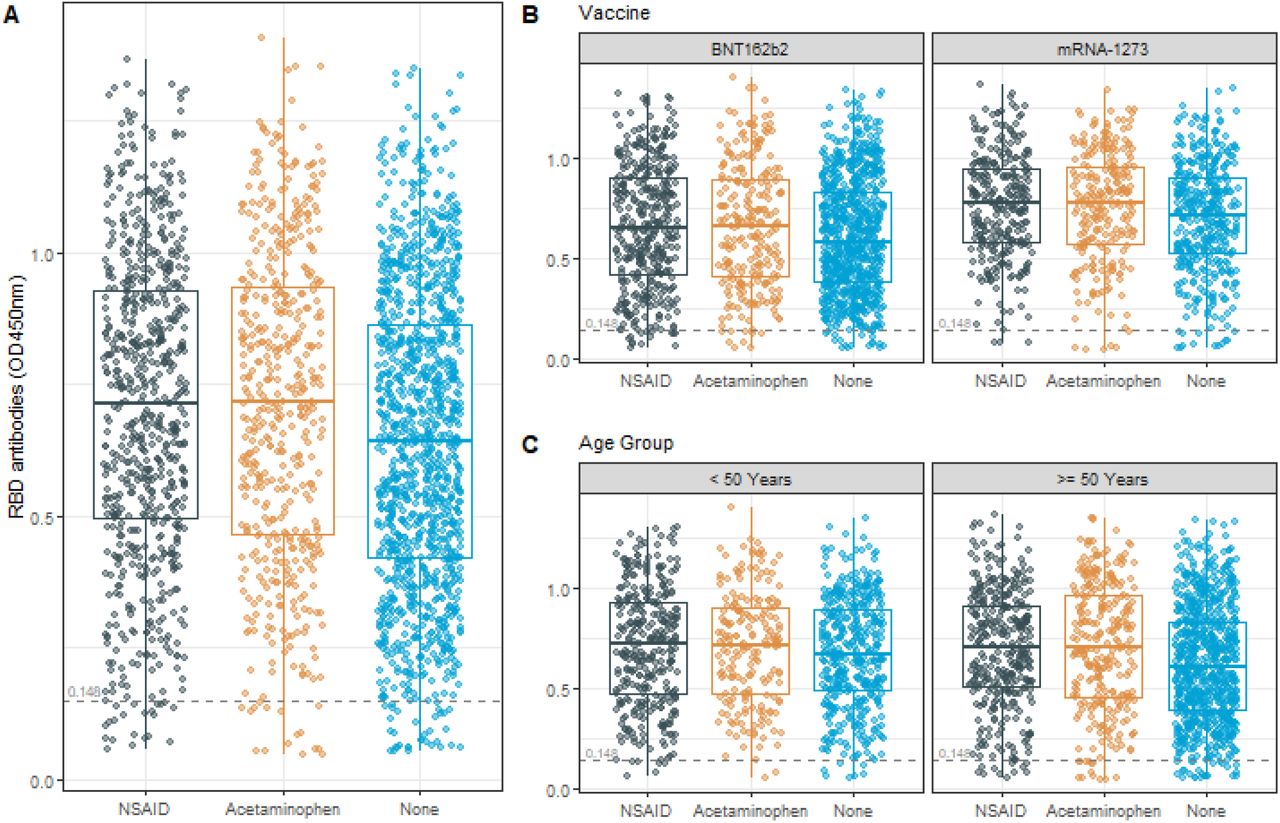
We examined survey results for analgesic use from March 15, 2021 through March 22, 2022 that included 2,354 vaccinated individuals that were part of a large statewide antibody testing initiative run by The University of Arizona. Antibodies against SARS-CoV-2 Spike receptor binding domain (RBD), self-reported vaccination information, and reported analgesic use within 48-hours after either two-dose mRNA COVID-19 vaccines (mRNA-1273 or BNT162b2) were analyzed. A one-way Analysis of Variance (ANOVA), using the t-test statistic, showed statistically significantly lower RBD-specific antibody levels in those who did not take an analgesic (n = 1,184) relative to those that took either NSAIDs or Acetaminophen (p = 0.0001 for both). There was no statistically significant difference detected between the NSAID (n = 679) and Acetaminophen (n = 491) analgesic groups (p = 0.9332). Thus, unexpectedly, analgesic use was associated with higher, rather than lower levels of anti-Spike antibodies. These differences were not modified by age group or vaccine, as determined by evaluation of the interaction effect between these variables and analgesic group (p = 0.0834 and p = 0.0819, respectively). For reasons that are unclear, and therefore results not shown, those who did not answer the painkiller questionnaire (n = 1489) had statistically significantly higher RBD levels than those that did respond to the survey.
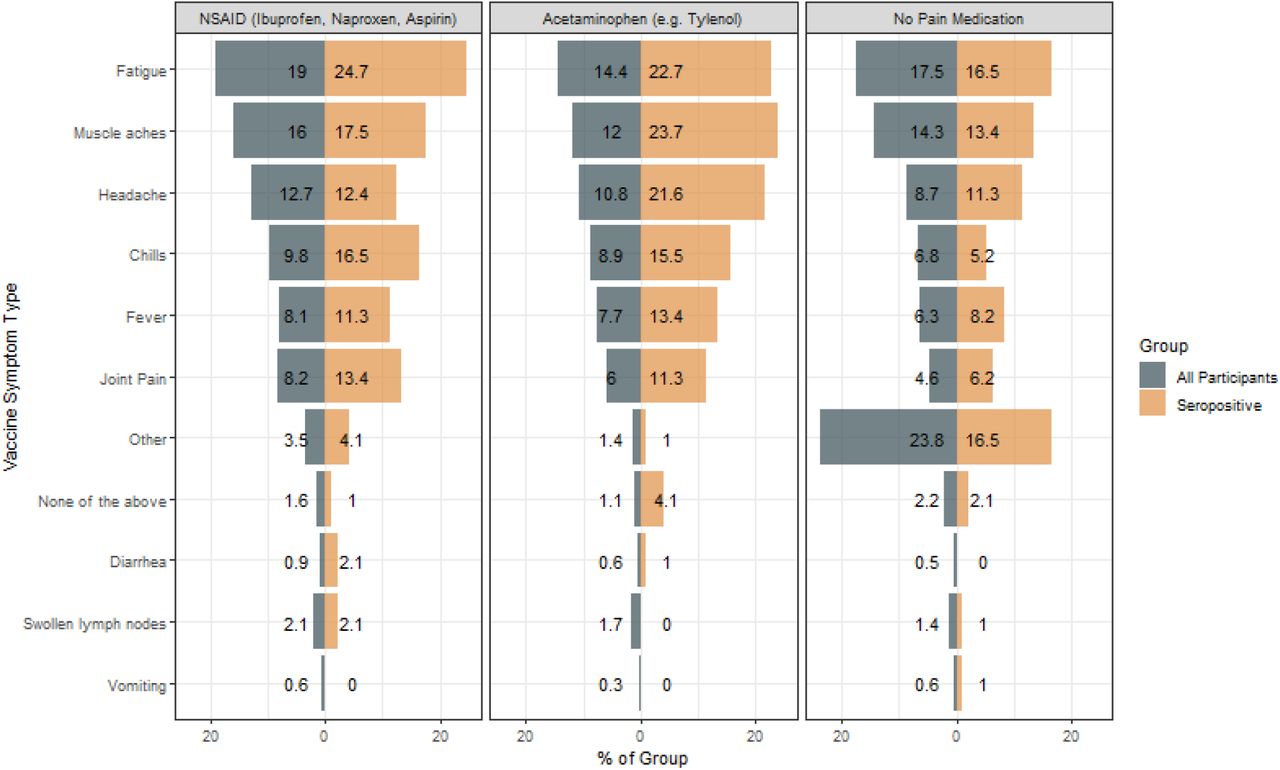
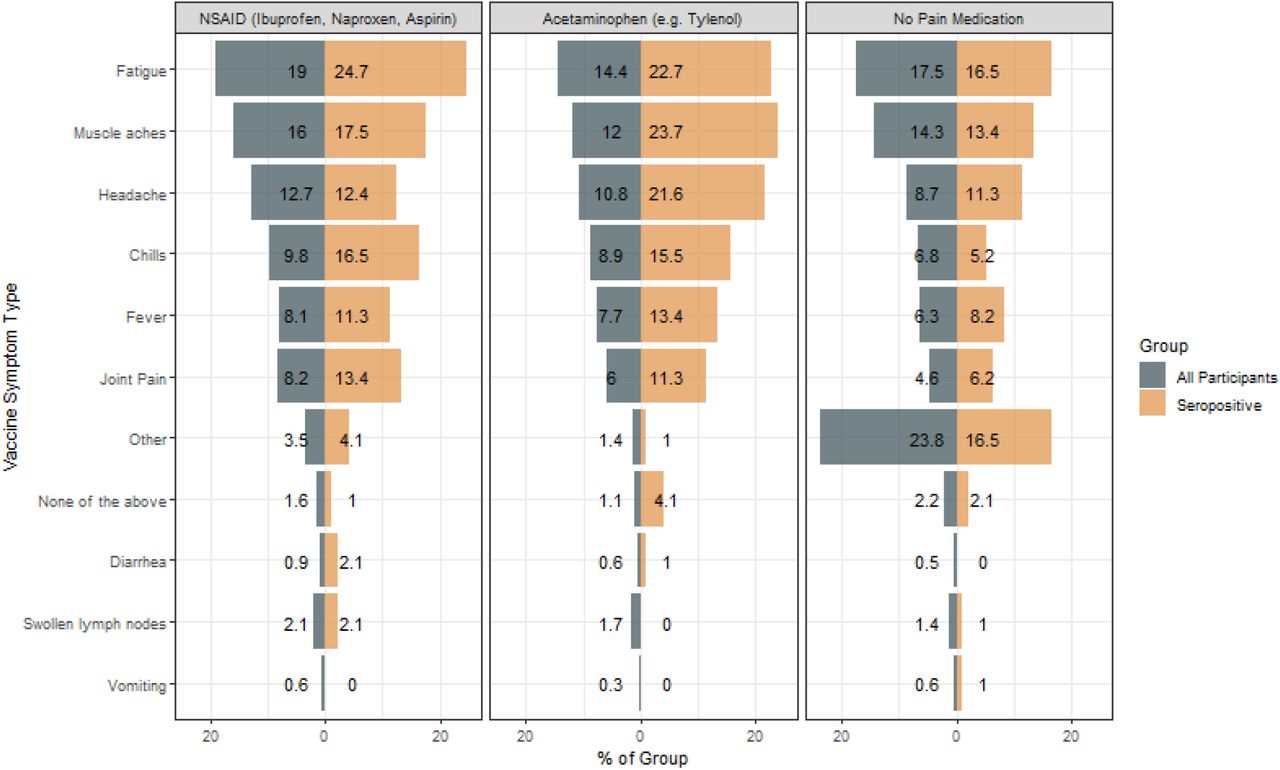
The most common vaccine-induced side effects were fatigue, muscle aches and headaches, and were highest in those taking NSAIDs. While the overwhelming majority of participants were scored as seropositive after vaccination (95%), a small fraction of individuals fell below this threshold (126/2,354). Seropositivity was increased in those experiencing these three symptoms and taking NSAIDs compared to those not taking pain medication (Figure 2). Logistic regression analyses showed that there was a statistically significantly higher proportion of those experiencing fatigue and muscle aches between NSAID users and those not taking pain medication (p < 0.0001 for both vaccine side effects). We also observed a statistically higher proportion of headaches reported by NSAID users, compared to those not taking pain medication and lower than those taking acetaminophen (p < 0.0088). There were other side effects that were not captured on the survey (denoted as “other”), which were most common among those not taking any pain medication (23.8%). Thus, the most parsimonious explanation is that inflammation and adverse events, rather than analgesic use per se, are associated with elevated antibodies, although the observational nature of this study doesn’t allow for this assessment directly. In summary, we find no evidence to suggest that analgesic use after COVID-19 vaccination detrimentally impacts antibody responses. A limitation of our study is that other immunological parameters, such as cellular memory, were not measured.
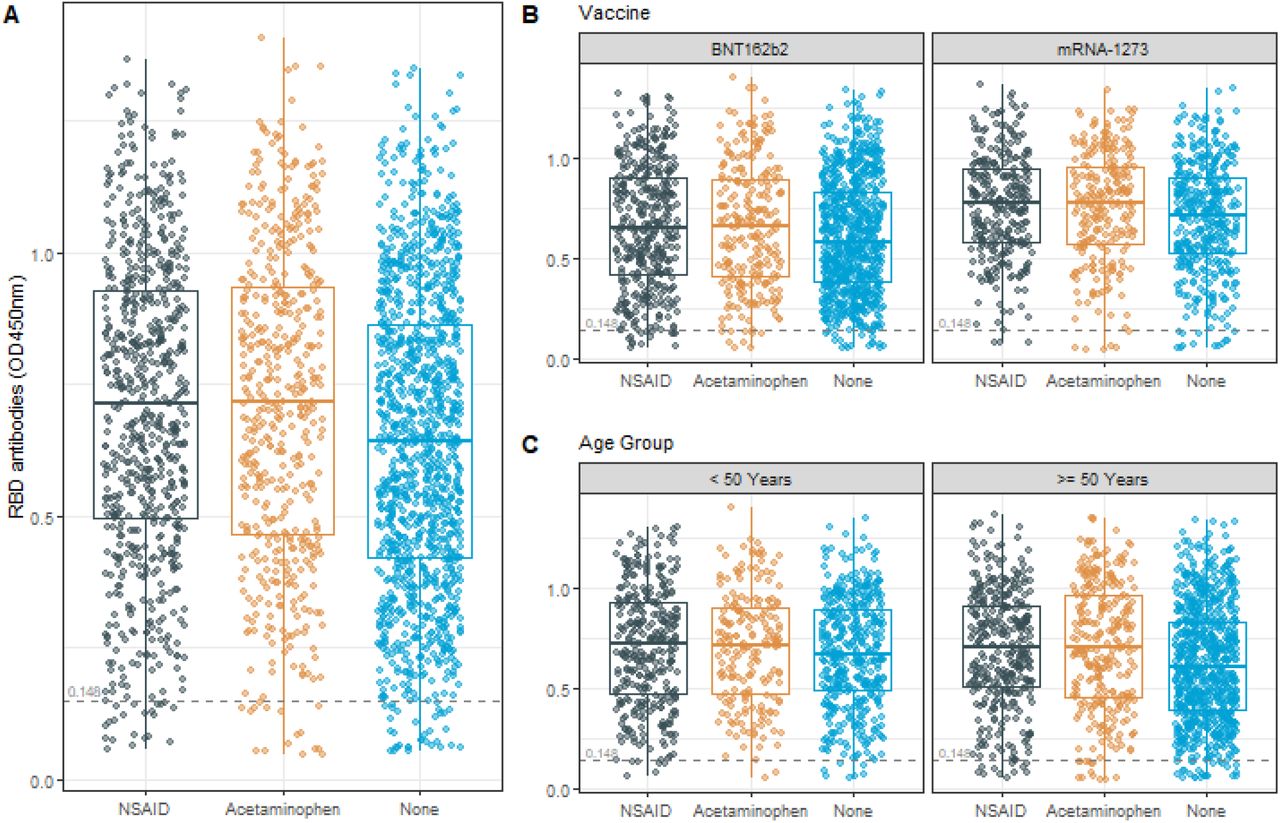
A) There was no statistically significant difference detected between the NSAID and Acetaminophen analgesic groups (p = 0.9332). Lower mean RBD antibodies between those participants that did not take any analgesics and both mean RBD antibodies between those participants taking NSAIDs and Acetaminophen (p < 0.0001 for both). B) and C) No evidence of an effect modification of the relationship between RBD antibodies by analgesic groups by either vaccine or age (p = 0.0834 and p = 0.0819, respectively).
{kind=link}
{kind=link}
Logistic regression analyses showed that there was a statistically significantly higher proportion of those experiencing fatigue and muscle aches between NSAID users and those not taking pain medication (p < 0.0001 for both vaccine side effects). We also observed a statistically higher proportion of headaches reported by NSAID users, compared to those not taking pain medication and lower than those taking acetaminophen (p < 0.0088).
Data Availability
All data produced in the present study are available upon reasonable request to the authors




