
Abstract
Introduction/Aims The primary aim of this study is to define the sonographic diaphragm phenotype of Long COVID patients with non-specific dyspnea and fatigue. We analyzed patients referred from a pulmonary medicine COVID clinic without any intrinsic cardiopulmonary explanation for their new symptoms. Additionally, we report the functional outcomes of patients who completed an outpatient cardiopulmonary physical therapy program.
Methods This was a retrospective cohort study (n = 37) of consecutive patients referred for neuromuscular assessment centered on B-mode ultrasound of the diaphragm muscle. Patients were recruited from a single academic hospital between February 25, 2021 and October 7, 2021.
Results Sonographic abnormalities were identified in 65% (24/37) of patients, and in the vast majority of cases (23/24) was defined by low diaphragm muscle thickness. Thinner diaphragm muscles positively correlated with lower serum creatinine and creatine kinase values, but there was no association with markers of systemic inflammation. Eighteen patients participated in outpatient cardiopulmonary physical therapy that included respiratory muscle training, and 77.8% (n=14) had documented improvement.
Discussion In the outpatient rehabilitation setting, patients with Long COVID frequently display low diaphragm muscle thickness, but intact muscle contractility on sonographic studies. We speculate this represents a form of disuse atrophy, which has a good response rate to cardiopulmonary physical therapy.
Introduction
Chronic functional impairments reported in survivors of the most severe coronavirus disease 2019 (COVID□19) who require inpatient rehabilitation to recover frequently have a neuromuscular underpinning.1, 2 The extent of neuromuscular contribution to persistent symptoms observed after less severe COVID-19 is not well defined. According to the Centers for Disease Control and Prevention, Long COVID, also known as “post-COVID conditions” or “post-acute sequelae of SARS CoV-2 infection”, is defined as a wide range of new, returning, or ongoing health problems four or more weeks after initial infection.3 Persistent symptoms are present in more than half of COVID-19 survivors 6 months after recovery,5 with a frequency ranging from 10-35% in those with mild disease.6 Fatigue, dyspnea, and cough are among the most commonly reported symptoms in long COVID with a prevalence of 31%-63%, 18%-47%, and 12%-25%, respectively.7
After severe COVID-19 infection, Farr et al. used neuromuscular ultrasound to demonstrate impaired diaphragmatic contractility as a contributor to persistent dyspnea and fatigue in the setting of inpatient rehabilitation.2 However, the sonographic findings in patients with Long COVID in the outpatient rehabilitation setting has not been reported. We hypothesized that in this less severely affected population, diaphragm muscle dysfunction contributes to their persistent respiratory symptoms. Here we performed a retrospective analysis on long COVID patients referred for neuromuscular rehabilitation assessments including diaphragm ultrasound after no clear cardiopulmonary etiology was identified.
Methods
This is a retrospective analysis of the first 37 consecutive Long COVID patients with suspected neuromuscular respiratory weakness referred to a single center (Shirley Ryan AbilityLab, Chicago, IL) for neuromuscular ultrasound and consultation by a physiatrist who is ABPMR board certified in physical medicine and rehabilitation, and neuromuscular medicine. All patients developed persistent dyspnea and/or fatigue after PCR-confirmation (81%) or clinical diagnosis of COVID-19. No patients in this cohort required inpatient rehabilitation services after their acute infection, most (n = 27) were never hospitalized, and none of them required invasive ventilation for their acute illness. The patients were evaluated between February 25, 2021 and October 7, 2021. Prior to rehabilitation referral, patients were evaluated by pulmonologists within a comprehensive COVID care model at an academically affiliated hospital (Northwestern Memorial Hospital, Chicago, IL). All patients were clinically evaluated for a pulmonary parenchymal or pulmonary vascular etiology for their dyspnea. In addition to history and physical examination, CT scans were obtained in 26 patients (70%), pulmonary function tests were obtained in 31 patients (84%), and 30 patients (81%) underwent 6-minute walk testing. If this testing did not reveal a pulmonary parenchymal or pulmonary vascular etiology that fully explained the degree of post-infectious dyspnea observed, the patient was referred to rehabilitation outpatient clinic.
All patients underwent point of care ultrasound and 33 patients (89%) underwent electrodiagnostic testing that included phrenic nerve conduction studies as well as a limited needle electromyography exam of the biceps brachii and/or vastus lateralis muscle. Previously published healthy control normative data set (n=150)8, as well as our prior data set of patients with more severe COVID-19 infection who subsequently underwent inpatient rehabilitation (n = 21)2 were used as a comparative populations. The diaphragm muscle was assessed on a portable ultrasound system (Xario 200, Canon Medical Systems USA Inc., Tustin, CA) with either a 5.0 to 18.0-MHz linear array (18L7) or 1.8- to 6.0-MHz convex array (6C1) selected to optimize image clarity on the basis of individual characteristics including body habitus in B-mode as previously described.2 Each hemi-diaphragm was identified in the zone of apposition, and thickness was measured at functional reserve capacity (FRC) and total lung capacity (TLC). Normative values have been established for diaphragm muscle thickness at FRC (≥ 0.14 cm) and thickening ratio (TLC/FRC muscle thickness; > 1.2) at the 8th or 9th intercostal space.8 Approval was obtained from Northwestern University IRB (STU23625789).
Cardiopulmonary physical therapy intervention was offered to all patients, which consisted of cardiovascular conditioning, with continuous monitoring of SpO2, heart rate and rate of perceived exertion. Patients were prescribed a respiratory muscle trainer, allowing for resistance during inspiration and expiration to complete as a home exercise program five times daily. In addition, patients were educated on shortness of breath, diaphragmatic breathing strategies and habit forming strategies to continue with cardiovascular conditioning and breathing program independently post-discharge.
Since this data did not have a normal distribution as determined by the Shapiro–Wilk test, The Wilcoxon Signed Rank Test was utilized to compare mean left and right hemi-diaphragm measurements. The Mann-Whittney U test was used to compare outpatient COVID-19 clinic patients (current data) with our prior data set from more severe COVID-19 rehabilitation unit inpatients. Pearson Correlation was employed to correlate sonographic findings with laboratory data and functional outcomes. Ultrasound data is reported throughout the results section as mean ± standard deviation.
Results
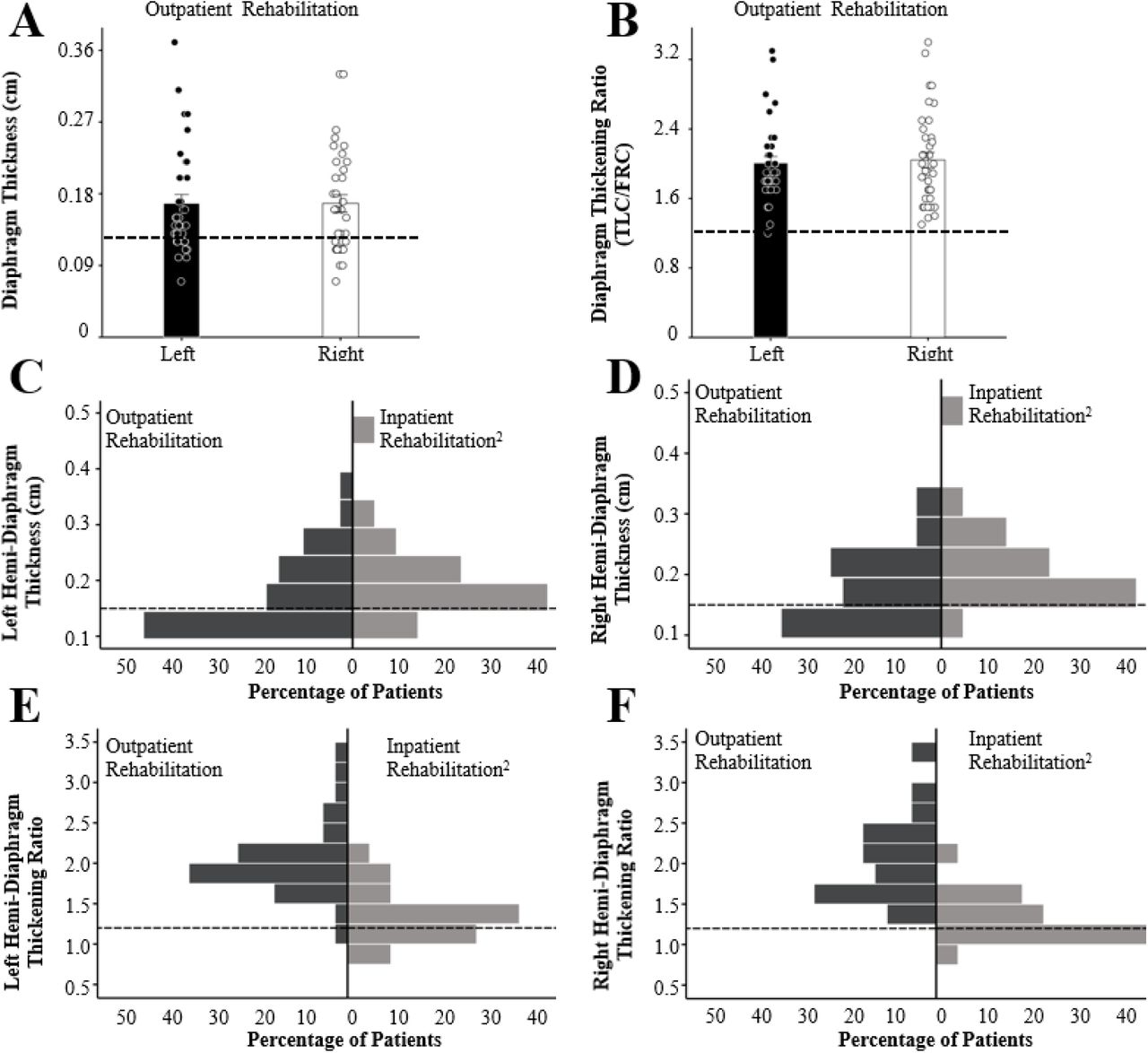
The baseline characteristics of the 37 patients assessed in outpatient rehabilitation medicine clinic after COVID-19 infection, including demographic data, hospital course, spirometry, and laboratory testing are reported in Table 1. The sonographic diaphragm thickness measured at FRC and thickening ratios of the left and right hemi-diaphragms are displayed in Figure 1A-B. The mean left hemi-diaphragm thickness was 0.17 ± 0.07 compared to 0.17 ± 0.07 (p=0.83) on the right. The mean thickening ratio was 2.0 ± 0.4 for the left hemi-diaphragm compared to 2.0 ± 0.5 for the right hemi-diaphragm (p=0.73). Sixty five percent (24/37) of patients had at least one sonographic value below the lower limit of normal, and in the vast majority of abnormal cases (23/24) it was reduced hemi-diaphragm (< 0.15 cm) muscle thickness at FRC. Sonographic findings in COVID-19 rehabilitation outpatients compared to more severe COVID-19 rehabilitation inpatients can be seen in Figure 1C-F. There was a statistically significant smaller left and right hemi-diaphragm thickness in the outpatient rehabilitation population compared to the inpatient rehabilitation population (Left p<0.01, Right p<0.01). The left and right hemi-diaphragm thickening ratio was greater in the outpatient population compared to the inpatient population (Left p=0.04; Right p=0.04).
Results are reported as Median value (range of values). Abbreviations: Intensive care unit (ICU); Forced expiratory volume (FEV1); Forced vital capacity (FVC); Diffusing capacity for carbon monoxide (DLCO); Total Lung Capacity (TLC); C-reactive protein (CRP); Creatine kinase (CK); Absolute neutrophil count (ANC); Absolute leukocyte count (ALC); 6 minute walk test (6MWT).

(A) The diaphragm muscle thickness, assessed at functional residual capacity (FRC), is plotted for the left (black bar) and right side (white bar) of each patient (n=37). (B) The diaphragm muscle thickening ratio, which is the ratio of the muscle thickness taken at total lung capacity (TLC) over functional residual capacity (FRC), is plotted for the left and right side of each patient. (C-D) Histogram comparing Left (C) and Right (D) diaphragm muscle thickness (at FRC) for Long COVID rehabilitation outpatients (dark grey bars) versus COVID-19 rehabilitation inpatients (light grey bars). (E-F) Histogram comparing Left (C) and Right (D) diaphragm muscle thickening ratio (TLC/FRC) for Long COVID rehabilitation outpatients versus COVID-19 rehabilitation inpatients. The dotted horizontal lines indicate lower limit of normal for each parameter.
Electrodiagnostic Findings
Limited needle electromyography exam was performed to screen for myopathic changes of the biceps brachii and/or vastus lateralis muscles on at least one side in most patients (34/37). There were no electrodiagnostic findings to suggest an active myopathy noted (e.g. fibrillation potentials, positive sharp waves, small amplitude and/or polyphasic motor unit potentials). None of the patients were clinically diagnosed with phrenic neuropathies, but 4/37 had absent phrenic nerve conduction responses despite normal diaphragm thickening ratios that was clinically interpreted as a false positive result, which is a known limitation of surface recordings of evoked diaphragm motor response.9
Functional Outcomes
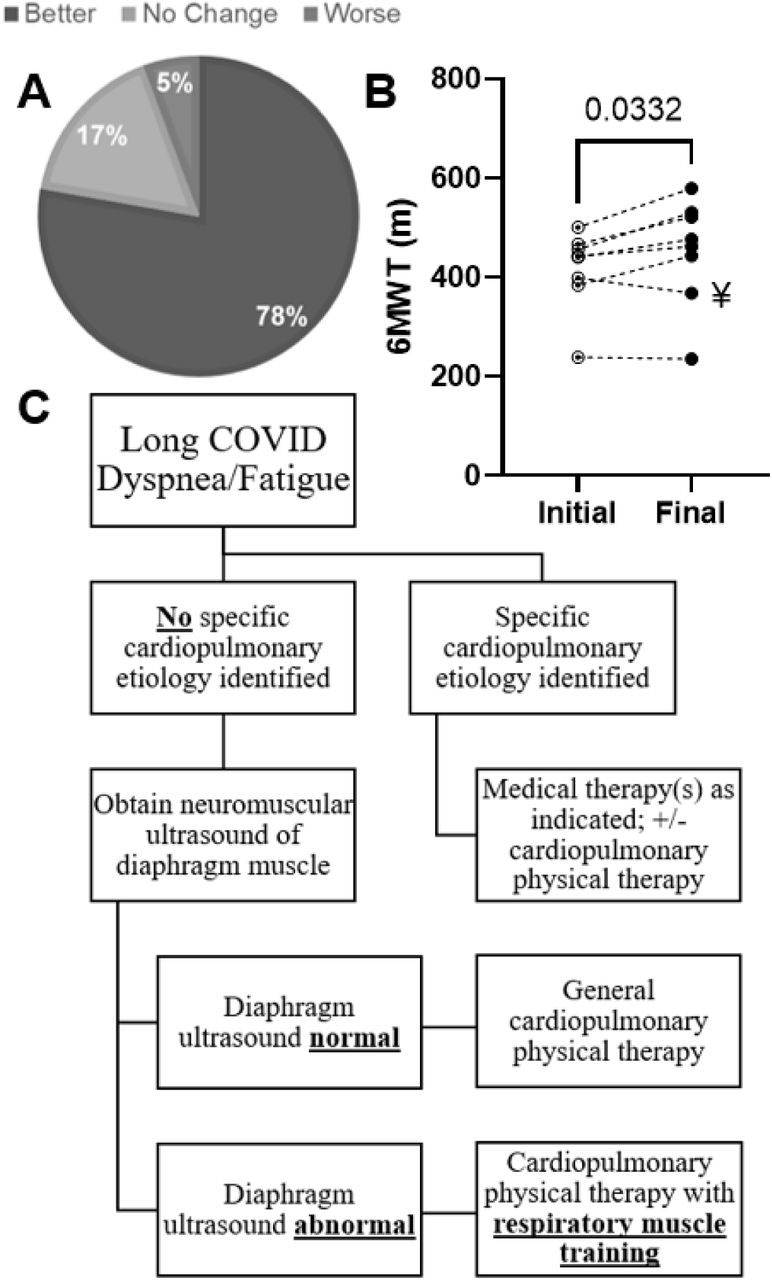
A subset of COVID-19 outpatients accepted a referral for outpatient cardiopulmonary physical therapy (n=18) with an emphasis on respiratory muscle training. Patients attended a mean of 4.0 ± 1.9 training sessions. For the patients who did not enroll in physical therapy (n=19), the main reason was preclusive distance from their residence to the outpatient therapy office in downtown Chicago. Some may have pursued outpatient cardiopulmonary rehabilitation closer to their residence at an outside facility, but no records of this were available to include. Of those who did enroll, 77.8% (14/18) showed documented functional improvement, 5.6% (1/18) worsened or plateaued, and 16.7% (3/18) could not tolerate therapy (Figure 2A). Reasons for inability to tolerate physical therapy include fatigue, chronic pain, or preexisting medical comorbidities such as arthritis. There were 8 patients who had 6-minute walk test measurements before and after completion of physical therapy, with 75.0% (n = 6) of patients showing improvement in this metric, 1 patient didn’t change, and the 1 patient who was noted to regress was attributed to aggravation of pre-existing knee osteoarthritis felt to be unrelated to cardiopulmonary physical therapy (Figure 2B).

(A) The percentage of Long COVID patients (n=18) who had documented improvement with outpatient cardiopulmonary physical therapy after being referred with non-specific pattern of dyspnea and/or fatigue. (B) The relative change in 6 meter walk test pre- (416 ± 81 m) and post- (452 ± 108 m) cardiopulmonary physical therapy (n=8) was significantly better (p=0.0332). (C) Cardiopulmonary physical therapy referrals may be considered for symptoms of dyspnea and/or fatigue in all Long COVID patients, but when there is no specific cardiopulmonary etiology identified we recommend considering a neuromuscular ultrasound of the diaphragm muscle to diagnose diaphragm dysfunction and tailor outpatient therapy with more precision.
Pulmonary Testing
Pulmonary function testing was obtained for patients at the clinical discretion of the providing physician. Spirometry, whole body plethysmography, nitrogen washout, and diffusing capacity of the lung for carbon monoxide (DLCO) were obtained. One patient was unable to tolerate lung volume assessment. Six minute walk testing was also performed in clinic prior to rehabilitation referral for 30 patients by trained medical assistants. Pulmonary function testing and 6 minute walk test results are presented in Table 1. Forced vital capacity, forced expiratory volume in 1 second, TLC, and DLCO are presented as % predicted. Briefly, the median FVC was 89% (interquartile range, IQR, 83.5-101%). The median forced expiratory volume in 1 second (FEV1) was 91% (IQR 83-99.5%). The median FEV1/FVC ratio was 79% (IQR 76-82.5%). The median TLC was 95.5% (IQR 85.5-107.5%). The median diffusing capacity for carbon monoxide (DLCO) was 84% (IQR 75-94.5%).
CT scans were obtained for patients at the clinical discretion of the pulmonary medicine physician. Clinical radiology reports were reviewed by the research team. Of the 26 patients who underwent CT scans to evaluate their dyspnea, the most common abnormality noted were pulmonary nodules, which were identified in 9 (34.6%) of patients. One nodule was 8mm, but all others were <5mm in size. Two patients (7.7%) had small areas of ground glass opacities and 3 (11.5%) were found to have band-like opacities, concerning for areas of fibrosis.
Laboratory Markers of Muscle Wasting Disease
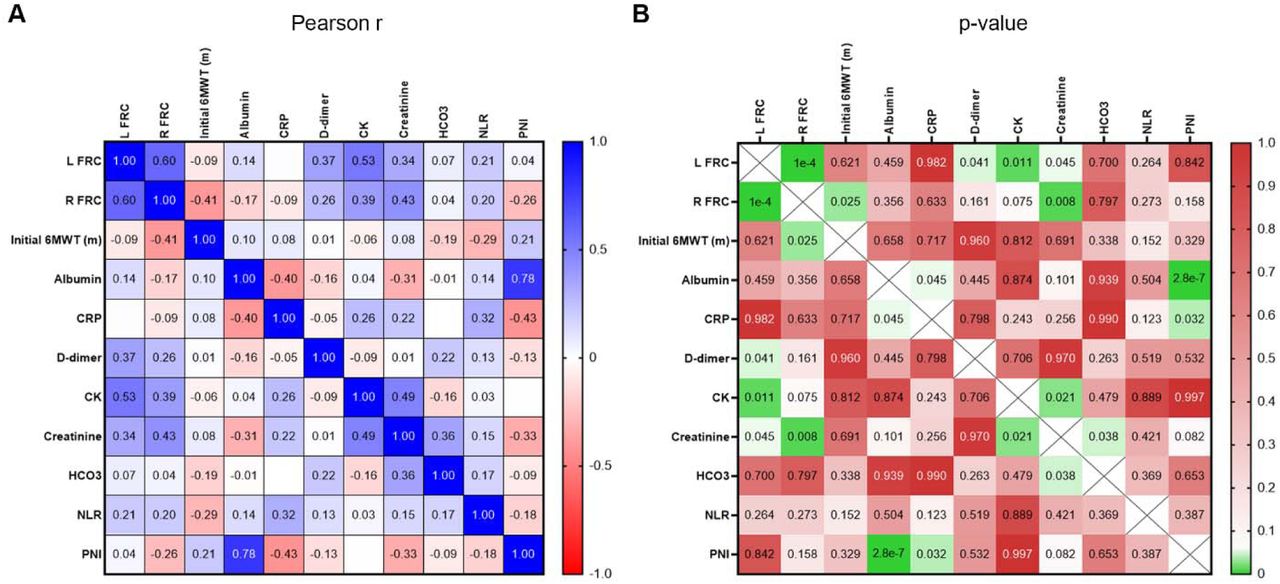
To address the possibility that this cohort is impacted by inflammatory muscle wasting, we examined C-reactive protein (CRP), CK, D-Dimer, bicarbonate, albumin, neutrophil to lymphocyte ratio, creatinine, albumin, and prognostic nutritional index (Supplemental Figure 1). The relationship between these serum-based markers of muscle wasting disease and either 6 minute walk test or diaphragm thickness was assessed through a Pearson correlation matrix. While no inflammatory based markers significantly correlated with any outcomes, both serum creatinine and CK had significant, positive correlations with diaphragm thickness (Supplemental Figure 1).

{kind=link}
{kind=link}
{kind=link}
(A&B) Heatmap of pearson correlation coefficient (r) and corresponding p-values between diaphragm thickness, initial six-minute walk test distance, and lab values including albumin, CRP, D-dimer, CK, creatinine, HCO3, neutrophil-to-lymphocyte ratio (NLR), and prognostic nutritional index (PNI).
Discussion
This study defines a distinct Long COVID diaphragm phenotype in the outpatient rehabilitation setting for patients with persistent respiratory symptoms not accounted for by intrinsic cardiopulmonary pathology. In an unexpectedly high percentage of cases (62%) these Long COVID patients presented with decreased diaphragm muscle thickness (atrophy), but intact diaphragm muscle thickening ratio (contractility). This distinguishes them from our prior study on more severe COVID-19 survivors who were assessed while in the inpatient rehabilitation setting and predominantly had impaired diaphragm contractility on sonographic exam.2 The mechanism for Long COVID diaphragm atrophy is unclear, but we did not find serological markers of persistent inflammatory or cachexia-like state correlated with atrophy (thickness) of the diaphragm muscle to account for this effect (Supplemental Table 1). Encouragingly, 77.8% of the sub-group of Long COVID patients (n=17) that accepted referrals for outpatient cardiopulmonary rehabilitation had documented improvements (Figure 2A-B).
General neuromuscular causes of diaphragm dysfunction include motor neuron disease, advanced polyneuropathy, myopathy, generalized muscle wasting (e.g. cachexia), and phrenic mononeuropathy.10, 11 In patients with severe COVID-19 infection, other proposed mechanisms include ventilator-induced diaphragm dysfunction and direct viral infiltration of SARS-CoV-2 through angiotensin converting enzyme 2 (ACE2).12,13 In our cohort of predominantly non-hospitalized patients (73%), there was no clinically diagnosed cases of phrenic mononeuropathy, polyneuropathy, or electrodiagnostic evidence of a myopathy. Additionally, while the atrophy was likely not due to an active inflammatory state, the positive correlation between diaphragm thickness, serum creatinine, and CK implies generalized loss of muscle mass may contribute to this phenotype. This is extrapolated from the use of creatinine as a proxy marker of muscle mass in other neuromuscular disease states assuming intact kidney function.14, 15 Based on the activity intolerance reported by many of our Long COVID patients, muscle disuse atrophy should be considered as a potential factor. Furthermore, this may explain why a clear majority of our patients responded favorably to cardiopulmonary physical therapy, including documented improvements in function by physical therapist or enhanced 6 minute walk test performance (Figure 2A-B). This rehabilitation framework was proposed by Severin and colleagues early in the pandemic,17 and in addition to the current results it is supported by a large meta-analysis showing positive effects of pulmonary rehabilitation on dyspnea, and quality of life.18 A small percentage of our cohort did not tolerate physical therapy, which raises the question of how best to approach treatment of their functional deficits and whether this status changes spontaneously over time.
Limitations of our study include a small sample size and the retrospective nature of the study. In addition, quantitative functional outcome data pre- and post-COVID infection and physical therapy intervention was limited. Future research on diaphragm dysfunction in Long COVID should include a larger sample and consider prospective study designs. Additionally, repeat diaphragm measurements and correlation with functional outcomes would be informative. To better assess the full impact of cardiopulmonary physical therapy, a randomized controlled trial with intent to treat analysis is desirable.
Conclusion
In this retrospective cohort study, we were able to identify evidence of diaphragm dysfunction, characterized by sonographic muscle atrophy with intact contractility, in Long COVID patients. The pathophysiologic mechanism of this finding is unclear, but we hypothesize it may be a form of disuse muscle atrophy. Our evidence suggests that patients with persistent respiratory symptoms after COVID-19 infection, which is not accounted for by an intrinsic cardiopulmonary etiology, may be referred for neuromuscular and sonographic evaluation. If referred for cardiopulmonary physical therapy, it appears more likely than not, that patients who are able to participate will experience improvement in symptoms and functional status.
Data Availability
All data produced in the present study are available upon reasonable request to the authors.
Acknowledgements
CKF acknowledges the generous support of the Belle Carnell Regenerative Neurorehabilitation fund, which made this work possible.
Footnotes
Declarations:
-Ethics approval and consent to participate: yes
-Consent for publication: not applicable
-Availability of data and materials: will be made available on request
-Competing interests: none
-Funding: no funding
None of the authors has any conflict of interest to disclose
References




