
ABSTRACT
Background Little is known regarding the effectiveness of tixagevimab/cilgavimab in preventing SARS-CoV-2 infection in this population, particularly after the emergence of the Omicron variant.
Objective To determine the effectiveness of tixagevimab/cilgavimab for prevention of SARS-CoV-2 infection and severe disease among immunocompromised patients.
Design Retrospective cohort study with propensity matching and difference-in-difference analyses.
Setting U.S. Department of Veterans Affairs (VA) healthcare system.
Participants Veterans age ≥18 years as of January 1, 2022, receiving VA healthcare. We compared a cohort of 1,848 patients treated with at least one dose of intramuscular tixagevimab/cilgavimab to matched controls selected from 251,756 patients who were on immunocompromised or otherwise at high risk for COVID-19. Patients were followed through April 30, 2022, or until death, whichever occurred earlier.
Main Outcomes Composite of SARS-CoV-2 infection, COVID-19-related hospitalization, and all-cause mortality. We used cox proportional hazards modelling to estimate the hazard ratios (HR) and 95% CI for the association between receipt of tixagevimab/cilgavimab and outcomes.
Results Most (69%) tixagevimab/cilgavimab recipients were ≥65 years old, 92% were identified as immunocompromised in electronic data, and 73% had ≥3 mRNA vaccine doses or two doses of Ad26.COV2. Compared to propensity-matched controls, tixagevimab/cilgavimab-treated patients had a lower incidence of the composite COVID-19 outcome (17/1733 [1.0%] vs 206/6354 [3.2%]; HR 0.31; 95%CI, 0.18-0.53), and individually SARS-CoV-2 infection (HR 0.34; 95%CI, 0.13-0.87), COVID-19 hospitalization (HR 0.13; 95%CI, 0.02-0.99), and all-cause mortality (HR 0.36; 95%CI, 0.18-0.73).
Limitations Confounding by indication and immortal time bias.
Conclusions Using national real-world data from predominantly vaccinated, immunocompromised Veterans, administration of tixagevimab/cilgavimab was associated with lower rates of SARS-CoV-2 infection, COVID-19 hospitalization, and all-cause mortality during the Omicron surge.
INTRODUCTION
Immunocompromised patients are at high risk for morbidity and mortality related to COVID-19.1 While vaccines have helped to prevent the spread of SARS-CoV-2 and decrease the risk of severe disease in the general population, immunocompromised patients remain at higher risk for breakthrough infections and persistent viral replication.2,3,4,5
The PROVENT study, a Phase 3, multicenter, randomized, placebo-controlled trial, demonstrated a single dose of intramuscular tixagevimab/cilgavimab (Evusheld, AstraZeneca) significantly reduced the incidence of symptomatic SARS-CoV-2 infection by 76.7% after 90 days in a broad population of adults with an increased risk of inadequate response to vaccination and/or increased risk of exposure to SARS-CoV-2.6 Based on these findings, on December 8, 2021, the US Food and Drug Administration (FDA) granted an emergency use authorization (EUA) of tixagevimab/cilgavimab as pre-exposure prophylaxis for moderate to severe immune compromised individuals or for whom vaccination with any available COVID-19 vaccine is not recommended due to a history of severe adverse reaction.7 The PROVENT trial also included those with chronic health conditions that could put individuals at elevated risk for complications owing to COVID-19.
Importantly, questions remain regarding effectiveness of tixagevimab/cilgavimab for the prevention of COVID-19. Only a small proportion (11%) of participants in the PROVENT trial were immunocompromised (i.e., receipt of immunosuppressive therapy, have immunosuppressive disease or cancer), and treatment effectiveness in this crucial subgroup could not be estimated in the trial.
Furthermore, all participants in the PROVENT trial were unvaccinated at the time of trial entry; therefore, indications for tixagevimab/cilgavimab among vaccinated persons is unknown. Finally, follow-up of participants in the PROVENT trial ended in September 2021; therefore, an analysis regarding real-world effectiveness is needed for tixagevimab/cilgavimab among vaccinated immunocompromised patients after the emergence of the Omicron variant (December 2021 in the US).8
Our objective was to assess the effectiveness of tixagevimab/cilgavimab for prevention of COVID-19 during the Omicron surge using electronic data from the U.S. Department of Veterans Affairs (VA), the largest integrated health care system in the US., the largest integrated healthcare system in the US. Using propensity score matching and Difference-in-Difference (DiD) approaches, we estimated the real-world effectiveness of tixagevimab/cilgavimab among immunocompromised Veterans for the prevention of SARS-CoV-2 infection, COVID-19 related hospitalization, and all-cause mortality.
METHODS
Study Setting and Data Sources
The VA provides care to nearly 9 million Veterans at 171 medical centers and 1112 outpatient clinics across the US. The first dose of tixagevimab/cilgavimab was given at VA on January 13, 2022. We analyzed electronic health records (EHR) using the VA Corporate Data Warehouse (CDW), which contains patient-level information on all patient encounters in VA medical facilities, including treatments, prescriptions, vaccinations, laboratory results, healthcare utilization, and vital status.9,10 We identified tixagevimab/cilgavimab use through the VA Pharmacy Benefits Management (PBM) EUA prescription dashboard, which captures and links records of recipients, date, and dosage of tixagevimab/cilgavimab administered in medical facilities across VA.11
This study was approved by the institutional review board of the VA Medical Center in White River Junction, Vermont, and was granted a waiver of informed consent because the study was deemed minimal risk and consent impractical to acquire. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Study population and outcomes
We included Veterans who were ≥18 years (as of January 1, 2022) and received VA healthcare through April 30, 2022 or until death, whichever occurred earlier, and who fulfilled study period and other inclusion criteria. Tixagevimab/cilgavimab (150 mg/150 mg) was first administered in the VA on January 13, 2022. On February 24, 2022, in response to concerns regarding effectiveness of the tixagevimab/cilgavimab against the Omicron variant, the FDA revised the EUA to increase the initial dose tixagevimab/cilgavimab to 300 mg/300 mg; patients who received the previously authorized (lower) dose were advised to receive an additional dose.12 In our current analysis, we included any patient who received at least one dose of tixagevimab/cilgavimab during the observation period in the treatment arm. Controls were immunocompromised or other high-risk patients who did not receive tixagevimab/cilgavimab. To address immortal time bias control patients were assigned pseudo-administration dates to match the real treatment dates of the tixagevimab/cilgavimab patient cohort. These dates, real and imitated, served as the index date of follow-up. The study period was then divided into phases. We looked back over a maximum of two years before the date of treatment to assess baseline characteristics, with a follow-up period from date of receiving tixagevimab/cilgavimab through April 30, 2022, or until death, whichever occurred earlier.
Characteristics measured during the baseline period included demographics, significant comorbidities, and healthcare utilization. We used VA-assigned priority group for healthcare to serve as a surrogate measure for socioeconomic status.13 Information regarding comorbidities was abstracted from diagnosis codes recorded in VA electronic data for healthcare encounters during any VA visit in the two years before the index date; significant comorbidities were defined according to an adaptation of Deyo-Charlson comorbidity index (DCCI).14 We defined immunocompromised status based on 1) whether the patient received an immunosuppressive medication during the 30 days before the index date (Appendix I) or 2) the presence of at least one qualifying immunocompromising condition, based on ICD-10 code listed in Appendix II, during the two years before index date.15 We defined severely immunocompromised as those who had a solid organ transplant or received anti-rejection medication for transplant or chemotherapy for cancer treatment in the prior month.
The primary outcome was the composite of 1) SARS-CoV-2 infections confirmed by the presence of SARS-CoV-2 virus detected by reverse-transcriptase-polymerase-chain-reaction (RT-PCR) or antigen testing; 2) COVID-19 hospitalization, defined as having both an admission and discharge diagnosis for COVID-19 from a hospital or within 30 days of positive SARS-CoV-2 RT-PCR result or antigen test; 3) all-cause mortality, defined as having a date of death (DoD) during the follow-up. Clinical visits with urinary tract infection (UTI) as the primary discharge diagnosis (UTI, ICD-9: 599) were added as a fourth outcome in falsification test as for a negative control.16
Statistical Analysis
Propensity Score Matching
We used propensity score models to account for observable baseline differences between patients who received tixagevimab/cilgavimab and controls. All covariates in the propensity score (Appendix III) were measured before the initiation of tixagevimab/cilgavimab to avoid adjustment for potential mediators. Indicator variables were generated to capture missing or unknown values for any of the matching criteria to retain patients in the study. Propensity score matching was performed using greedy nearest neighbor matching with caliper of 0.2 and ratio of 1:4 with replacement.17 In order to assess the robustness of the propensity match, we calculated the standardized mean difference (SMD); a successful match was estimated when at least 90% of the covariates included in the propensity score model had Standardized Mean Difference (SMD) of ≤10.18
To address immortal time bias,19 we generated a pseudo-tixagevimab/cilgavimab administration date for each control that follows the same distribution as those actual administration dates for recipients of tixagevimab/cilgavimab.20 In the final model, we matched patients who received tixagevimab/cilgavimab and eligible controls based on the date (or pseudo-date) and the facility where tixagevimab/cilgavimab was administered. We excluded any patients who were diagnosed with SARS-CoV-2 infection via a positive RT-PCR result or antigen testing within 3 months of the date or pseudo-date of tixagevimab/cilgavimab administration to optimize focus on new infections. We used Cox proportional hazards regression to compare patients who received tixagevimab/cilgavimab and their matched controls.
Difference-in-Difference Analysis
In addition to the propensity score model, we used a difference-in-difference (DiD) analysis to assess outcomes. The DiD analysis is a quasi-experimental method used to estimate the causal effect of an intervention.21 We calculated a person-time denominator for patients who received tixagevimab/cilgavimab and controls by tallying the number of days those patients were enrolled for an extended study period (September 1, 2021 through April 30, 2022). We calculated a numerator as total number of outcomes (including multiple outcomes for a single patient) per period. Outcome rates were then calculated for treated and controls during the baseline (last 4 months of 2021) and observation period. To simplify, we calculated events by calendar month. This was only employed to show the background rates of events during this extended period for the unmatched study population.
After propensity-score matching, we adjusted for residual confounding using the prior event rate ratio (PERR) approach.22 This method, like the difference-in-differences method used in econometrics, accounts for two distinct time periods, time before the intervention (e.g., tixagevimab/cilgavimab administration date and pseudo-tixagevimab/cilgavimab administration date) and time after the intervention. For each cohort, the rates of each outcome were calculated and compared before and after the intervention within the extended study period. To assess the impact of the intervention, the relative rate of the post-treatment period was divided by the relative rate of the pre-treatment period.
To apply the PERR method, we first computed the incidence rate ratio (RR) for each study outcome in the observation period (RRo) and then again in the baseline period (RRb). The RR is the rate of the outcome among tixagevimab/cilgavimab recipients divided by the rate of the outcome in the control arm. Next, we computed the PERR per the following formula PERR=(RRo / RRb), and, finally, the relative effectiveness of tixagevimab/cilgavimab to SPM (rE) is defined as (1-PERR) x 100%.
Analyses were performed with Stata 17 software (StataCorp), and SAS software, version 8.2 (SAS Institute).
RESULTS
Study Population
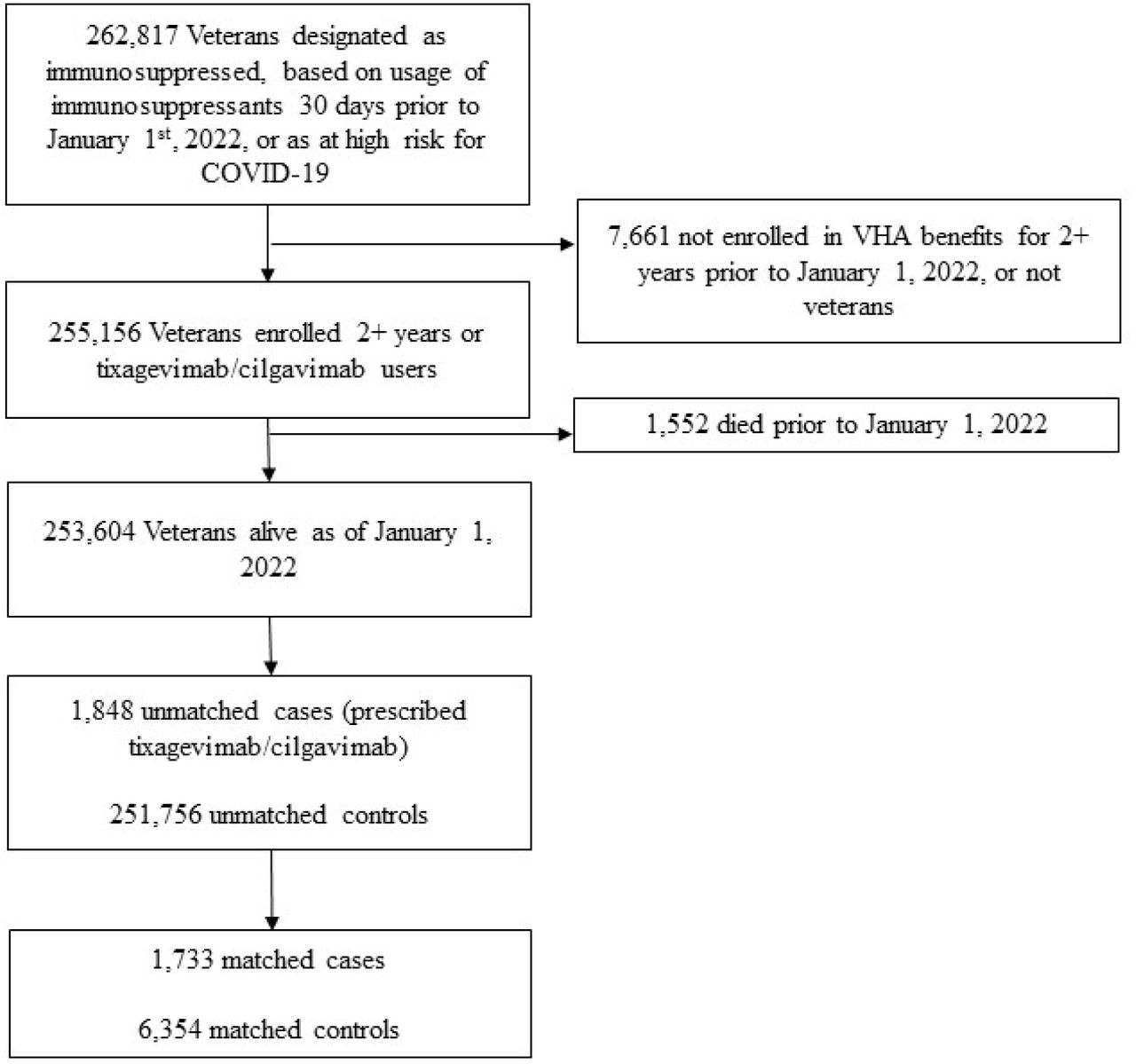
We identified 1,848 recipients of tixagevimab/cilgavimab and 251,756 control patients who were immunocompromised or otherwise at high risk for COVID-19 (Figure 1). After propensity-score matching 1,733 remained in the treatment group and 6,354 in the control group, which were well balanced across baseline characteristics (Table 1). Among the treated, 1,579 (91%) were male, 277 (16%) were Black, 76 (4%) were Hispanic, and 1250 (72%) were non-Hispanic White. Most (1,187 [69%]) of the tixagevimab/cilgavimab recipients were ≥ 65 years old and 1,238 (71%) lived in urban areas.23 We identified 1,595 (92%) tixagevimab/cilgavimab recipients as immunocompromised in the electronic data (by immunosuppressants use and diagnosis codes in Appendix Tables I, II). The propensity-matched control group had the same proportion of immunocompromised patients (5,863 [92%]). Additional common comorbidities in treated patients included 1,029 (59%) hypertension, 612 (35%) dyslipidemia, 597 (34%) cancer, and the majority were overweight (BMI [kg/m2] ≥ 25.0 and <30, 674 [39%]) or obese (BMI 30.0 or higher, 632 [36%]). Most tixagevimab/cilgavimab recipients had received 2 doses of mRNA vaccines or 1 dose of Ad26.COV2 (Janssen) (22%) or ≥ 3 vaccine doses or 2 doses of Ad26.COV2 (73%). Only 88 (5%) tixagevimab/cilgavimab recipients did not have any record of COVID-19 vaccination, compared to 67,753 (27%) among unmatched control patients.

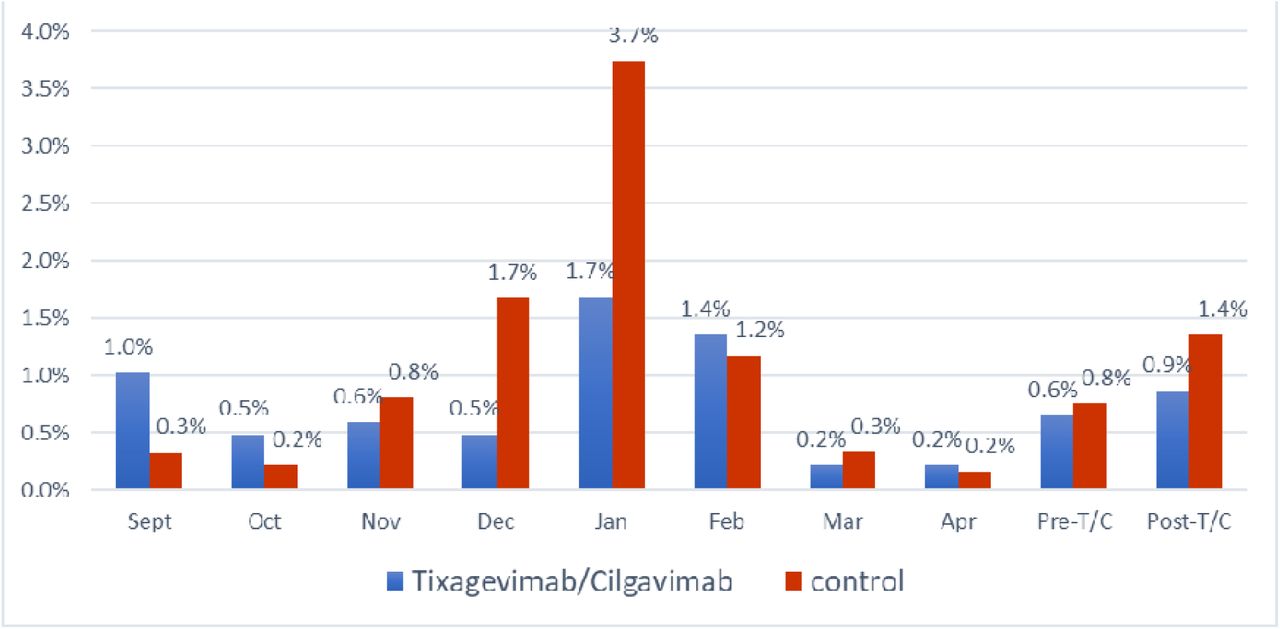
To provide an overall picture of SARS-CoV-2 infection data for the study population during the extended study period, we displayed SARS-CoV-2 infection by calendar month from September 2021 to April 2022 with January 2022 as division when tixagevimab/cilgavimab first became available in the VA (Figure 2). Immunocompromised Veterans who received tixagevimab/cilgavimab (1,848) were shown next to the control group of 251,756 who did not receive tixagevimab/cilgavimab in categories of identified events: SARS-CoV-2 infection verified by positive PCR test, COVID-19-related hospitalization, all-cause mortality. During the last 4 months of 2021, before tixagevimab/cilgavimab became available at VA, the treatment group had an average incidence of SARS-CoV-2 infection or COVID-19-related hospitalization at 0.6% per month, while the control group had an average incidence of 0.8% per month. With the Omicron surge in January 2022, the first 4-month average in 2022 increased to 0.9% and 1.4% for the treatment and control groups, respectively. Although both groups experienced a surge, the treatment group was proportionally smaller than that of the control group (50% vs. 75% increase).
Propensity Score Analysis
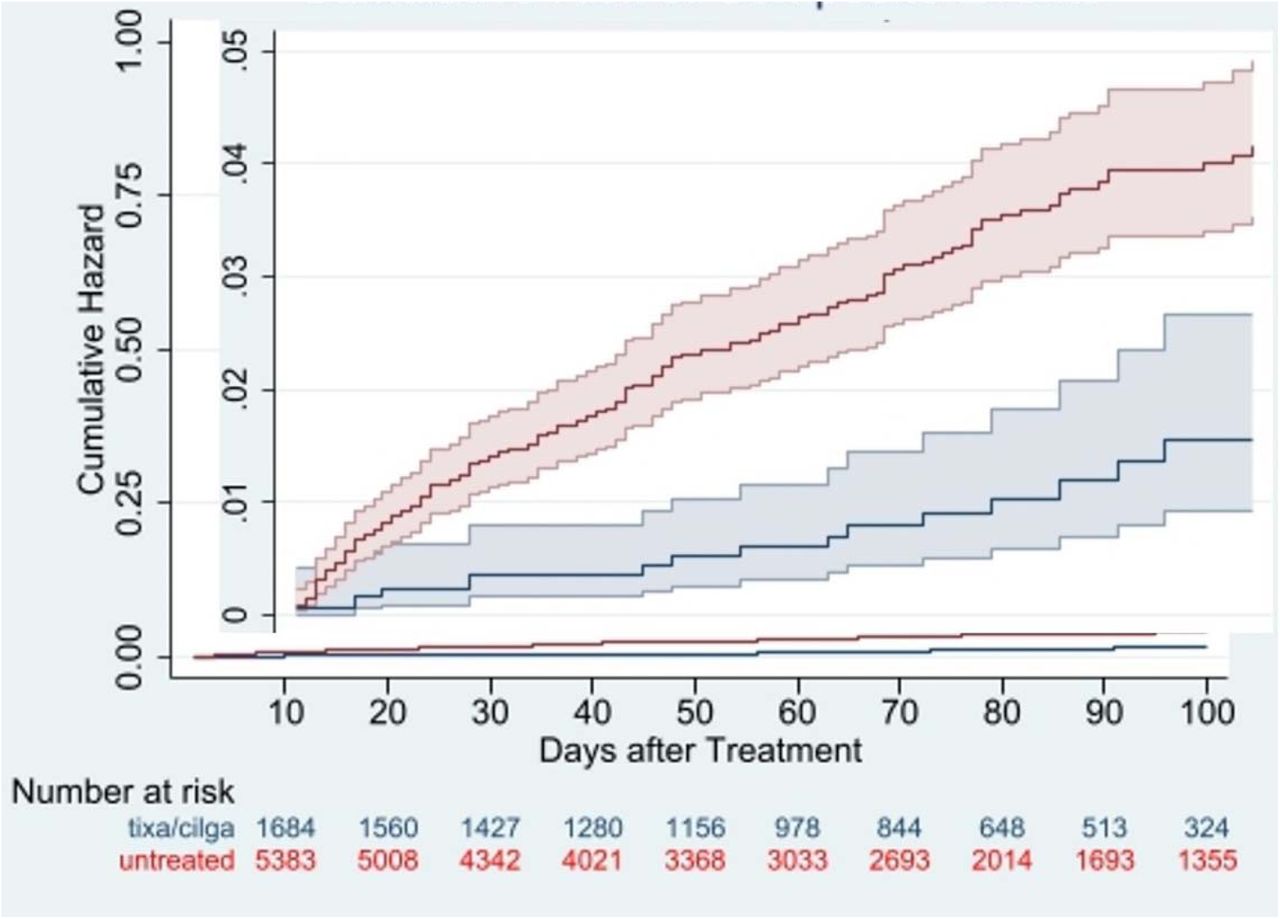
Estimated from propensity-score matched survival analyses, tixagevimab/cilgavimab recipients had a lower incidence of the composite of COVID-19 outcomes versus control patients overall (17/1733 [1.0%] vs 206/6354 [3.2%]; HR 0.31; 95%CI, 0.18-0.53). Results were similar within the study populations of EHR-confirmed immunocompromised (HR 0.32; 95%CI, 0.18-0.62), severely immunocompromised (HR 0.44; 95%CI, 0.21-0.93), and for Veterans aged 65 or older (HR 0.33; 95%CI, 0.18-0.61). The association in the overall cohort was similar across each of the individual COVID-19 outcomes, including test-confirmed SARS-CoV-2 infection (HR 0.34; 95%CI, 0.13-0.87), COVID-19 hospitalization (HR 0.13; 95%CI, 0.02-0.99), and all-cause mortality (HR 0.36; 95%CI, 0.18-0.73). (Table 2, Figure 3)

{kind=link}
{kind=link}
{kind=link}
Composite COVID-19 outcomes were SARS-CoV-2 infection, COVID-19 hospitalization, or all-cause mortality
Lastly, we were able to examine the impact of tixagevimab/cilgavimab with and without concomitant vaccination. Those fully vaccinated with at least 3 doses of any vaccine or 2 doses of Ad26.COV2, but without receiving tixagevimab/cilgavimab, had an incidence rate of 2.8% of COVID-19 infection or related hospitalization vs a rate of 3.7% among those neither vaccinated nor received tixagevimab/cilgavimab. Those not fully vaccinated but treated with tixagevimab/cilgavimab had an incidence rate of 1.35%. Most dramatically, those who were both fully vaccinated and received tixagevimab/cilgavimab had a rate of 0.85%, like the rate of a fully vaccinated and boosted non-immunocompromised adult. 24
Sensitivity (DiD) Analysis
The interaction term between intervention (tixagevimab/cilgavimab vs control) and period (baseline and observation) was used to estimate the PERR-adjusted effectiveness using a Poisson regression model. The matched, PERR-adjusted effectiveness, as measure by incidence rate ratio was 0.32 (95% CI, 0.24-0.44%) against SARS-CoV-2 infection verified by a positive test, 0.10 (95% CI, 0.05-0.22) against COVID-19-related hospitalization, almost identical to the point estimates from propensity-scores matched survival analysis (Table 2). Because both actual and pseudo tixagevimab/cilgavimab use required the subjects to be alive, we were not able to perform PERR analysis on mortality, including the composite outcome.
Falsification Analysis
Healthcare encounters with UTI as the primary discharge diagnosis were unlikely to be associated with tixagevimab/cilgavimab; therefore, served as a falsification test. One hundred sixty-three UTI visits were observed during the follow-up period. Propensity scores matched analysis demonstrated a similar effectiveness of tixagevimab/cilgavimab versus control against UTI (HR 1.05; 95% CI, 0.68-1.62) (Table 2). This lack of association between UTI and the treatment is reassuring that the protective effects associated with the treatment of tixagevimab/cilgavimab were unlikely due to bias or other major methodological flaws.
DISCUSSION
In this retrospective cohort study using real-world data from patients across the VA healthcare system in the US, administration of tixagevimab/cilgavimab was associated with a significant reduction in the risk of SARS-CoV-2 infection, COVID-19 hospitalization, and all-cause mortality among patients who received tixagevimab/cilgavimab compared with controls. Our findings were consistent across two robust statistical approaches, including propensity score matching and DiD estimations. These findings were observed among immunocompromised, severely immunocompromised, and older patients, further supporting the EUA criteria for use of tixagevimab/cilgavimab in this population. Further, we found evidence of augmented protection against SARS-CoV-2 infections among fully vaccinated immunocompromised patients who received tixagevimab/cilgavimab, akin to that of the population of fully boosted adults who were not immunocompromised.24
To our knowledge, this is the first real-world evidence of tixagevimab/cilgavimab for prevention of COVID-19 and provides important insights regarding the patient population who have received tixagevimab/cilgavimab across VA healthcare system. Of note, the EUA encourages use of tixagevimab/cilgavimab primarily among fully vaccinated immunocompromised patients; however, none of the participants in the PROVENT trial were vaccinated. In comparison, Error! Bookmark not defined. nearly all (95%) of our study population received at least two doses of a COVID-19 mRNA vaccine or one dose of Ad26.COV2 before receiving tixagevimab/cilgavimab, and most (75%) were fully vaccinated. In PROVENT, only 11% of trial participants were immunocompromised, compared to at least 92% in the current analysis. Furthermore, patients aged 65 years and older accounted for a small proportion (24%) of patients included in the PROVENT trial, compared to 69% of tixagevimab-cilgavimab recipients in the current study. However, only a small proportion of eligible patients received treatment, indicating that enhanced education and outreach are paramount to ensure that more immunocompromised Veterans across the VA healthcare system receive this medication, specifically during COVID-19 surges.
In comparison to the PROVENT trial, the observation period of our analysis coincided with the Omicron BA.1 surge across the United States and provides important clinical data in this latest evolution of the pandemic. While tixagevimab/cilgavimab is maintained neutralization against the Delta variant of SARS-CoV-2, tixagevimab/cilgavimab was shown to have decreased neutralizing activity against the Omicron BA.1 variant, prompting the FDA’s revision of EUA to increase the initial dose tixagevimab/cilgavimab. Current data indicate that tixagevimab/cilgavimab maintains neutralization against Omicron BA.2 and BA.2.12.1, but this effect may be attenuated with BA.4 and BA.5.25,26,27,28
The present analysis supports the effectiveness of tixagevimab/cilgavimab in preventing SARS-CoV-2 infections caused by the Omicron variants, including predominantly BA.1 and the early BA.2 and BA.2.12.1 surge. Future longitudinal analyses will focus on newer Omicron variants. To help address this issue, the VA has launched several initiatives including VA SHIELD (Science and Health Initiative to Combat Infectious and Emerging Life-threatening Diseases), a comprehensive biorepository of specimens from a cohort of affected Veterans with accompanying clinical data. As part of the future of VA SHIELD, clinical specimens will be collected prospectively from patients, which will help identify emerging strains as well as developing resistance in real world clinical settings. Obtaining this information rapidly will help public health officials, clinicians and researchers make important, timely decisions regarding diagnostics, prophylaxis, and therapeutics.
Our study had several notable strengths. We analyzed 1,486 patient-years of observation, making our study one of the largest ever conducted to assess tixagevimab/cilgavimab effectiveness while they were being distributed to combat a concurrent surge of the pandemic. The large sample allowed us to adjust for more potential confounding variables. Previous studies have shown that EHR data are more likely to be complete in capturing medical conditions and have a lower risk of up-coding. 29,30
Nevertheless, conventional analytical strategies such as stratification, matching (with or without propensity score), and multivariate regression analysis cannot adequately adjust for unobserved confounders. 31,32,33 These results were confirmed using two different statistical methods, including propensity-score matched models and DiD analysis. Propensity score matching of the intervention and comparison cohorts is an effective approach to control confounding. In addition, we employed an econometric technique – Difference-in-Difference (DiD) method - to adjust for bias from measured and unmeasured confounders and estimate the effectiveness of tixagevimab/cilgavimab in preventing COVID-19-related outcomes.
Finally, immortal time bias occurs when participants of a cohort study cannot experience the same outcome during a follow up period; if immortal time is misclassified or excluded during the analysis, the outcomes may be skewed. To account for immortal time bias in our analysis, we used a propensity-score matched survival analysis with Cox proportional hazards model to ensure controls were alive and COVID-free on the same day when their matched patients received tixagevimab/cilgavimab. This approach also ensured similar lengths of follow-up between the recipients and their matched controls.
Limitations
There are some limitations to acknowledge. Firstly, VA data include only healthcare encounters occur in VA medical centers, so we could have missed some infections and hospitalizations that occurred outside VA, which could bias our results towards the null. Secondly, while the EUA criteria are intended for patients who are immunocompromised, a small proportion of patients (%) who received tixagevimab/cilgavimab were not immunocompromised based on our definition and it is possible that we misclassified these patients. Thirdly, the VA has a unique population (mostly male, older), and our results may not be generalizable to a larger population of patients that were not treated at the VA. 34 Fourthly, the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes from claims data have been shown to inadequately capture comorbidity and functional status.35 Because only 289 (17%) of patients in our propensity-score matched tixagevimab/cilgavimab cohort received a single dose of 150 mg/150 mg tixagevimab/cilgavimab, we did not have the sufficient sample size to compare the original dosage of 150mg/150mg to the revised dosage of 300mg/300mg to assess the optimal dosing of tixagevimab/cilgavimab in the current analysis. Finally, we could not assess optimal timing of tixagevimab/cilgavimab in relation to COVID-19 vaccine administration, nor could we identify a target population who would be optimal to receive tixagevimab/cilgavimab.
Conclusion
Using national real-world data from predominantly vaccinated, immunocompromised Veterans, we found that administration of tixagevimab/cilgavimab was associated with lower rates of SARS-CoV-2 infection, COVID-19 hospitalization, and all-cause mortality, compared with controls, during the Omicron surge. Our results suggest that tixagevimab/cilgavimab administration, in addition to vaccination, protects vulnerable patients from SARS-CoV-2 infection and severe COVID-19 in a contemporary phase of the pandemic. Ongoing real-world data will help to understand the effectiveness of tixagevimab/cilgavimab for pre-exposure prophylaxis over time and against emerging variants.
The contents of this article do not represent the views of the U.S. Department of Veterans Affairs or the U.S. Government. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Food and Drug Administration, as well as any other agency of the U.S. Government. Assumptions made within and interpretations from the analysis do not necessarily reflect the position of any U.S. Government entity.
Data Availability
Data in the present work will not be made available.
Funding Statement
Supported by the Department of Veterans Affairs (VA) Office of Research and Development, the VA Office of Rural Health, Clinical Epidemiology Program at the White River Junction VA Medical Center, by resources and the use of facilities at the White River Junction VA Medical Center and VA Informatics and Computing Infrastructure, and data from the VA COVID-19 Shared Data Resource.
Declaration of Authors Competing Interests
VCM has received investigator-initiated research grants (to the institution) and consultation fees (both unrelated to the current work) from Eli Lilly, Bayer, Gilead Sciences and ViiV. YYX, GZ, CK, JS reported receiving grants from the US Food and Drug Administration through an interagency agreement with the Veterans Health Administration and from the US Department of Veterans Affairs Office of Rural Health. YYX, GZ, JS also reported receiving funding from Pfizer to US Department of Veterans Affairs for other research projects outside the submitted work. AAG received COVID-19 research project funding from the National Institutes of Health, Department of Defense, Centers for Disease Control and Prevention, AbbVie, and Faron Pharmaceuticals, outside the submitted work.
No other disclosures were reported.
SUPPLEMENTARY APPENDIX
Acknowledgements
We thank Dr. Hector Izurieta for his insight on observational study methods and guidance on real-world data.
References




