
Abstract
Background While booster vaccinations clearly reduce the risk of severe COVID-19 and death, the impact of boosters on SARS-CoV-2 infection has not been fully characterized: doing so requires understanding their impact on asymptomatic and mildly symptomatic infections that often go unreported but nevertheless play an important role in spreading SARS-CoV-2. We sought to estimate the impact of COVID-19 booster doses on SARS-CoV-2 infection in a vaccinated and actively surveilled population of young adults during an Omicron-predominant period.
Methods and Findings We implemented a cohort study of young adults in a college environment (Cornell University’s Ithaca campus) from December 5, 2021 through December 31, 2021 when Omicron was deemed the predominant SARS-CoV-2 variant on campus. Participants included 15,102 university students fully vaccinated with an FDA-authorized or approved vaccination (BNT162b2, mRNA-1273, or Ad26.COV2.S) who were enrolled in mandatory at-least-weekly surveillance PCR testing, and having no positive SARS-CoV-2 PCR test within 90 days before the start of the study period. Multivariable logistic regression considering those with full vaccination (a 2-dose series of BNT162b2 or mRNA-1273, or 1 dose of Ad26.COV2.S) with a booster dose versus those without a booster dose. 1,870 SARS-CoV-2 infections were identified in the study population. Controlling for gender, student group membership, full vaccination date and initial vaccine type, our analysis estimates that receiving a booster dose reduces the odds of having a PCR-detected SARS-CoV-2 infection relative to full vaccination by 52% (95% confidence interval [37%, 64%]). This result is robust to the choice of the delay over which a booster dose becomes effective (varied from 1 day to 14 days).
Conclusions Boosters are effective, relative to full vaccination, in reducing the odds of SARS-CoV-2 infections in a college student population during a period when Omicron was predominant. Therefore, booster vaccinations for this age group can play an important role in reducing community and institutional transmission.
Introduction
COVID-19 vaccines reduce SARS-CoV-2 infection and symptom severity [1], yet breakthrough infections occur, especially with the recently-emerged Omicron (B.1.1.529) variant [2, 3]. The effectiveness of Food and Drug Administration (FDA)-authorized or approved vaccines BNT162b2, mRNA-1273, and Ad26.COV2.S in preventing SARS-CoV-2 infection has dropped dramatically due to immune evasion and waning of vaccine-induced immunity over time [4-7]. The Omicron variant exhibits immune-system escape as the result of several mutations [8, 9]; this, and the high transmissibility of the Omicron variant, are leading to higher infection rates, strain on healthcare systems, and increased mortality [10, 11]. Therefore, to prevent symptomatic and severe outcomes of COVID-19, at the time of this study, the CDC recommended a booster vaccine six months after an initial mRNA vaccine series or two months after Ad26.COV2.S vaccination [7, 12]. The booster dose elicits an increase in antibody neutralization titers against the Omicron variant, and causes affinity maturation leading to a better antibody response, maintaining long-term protection against severe COVID-19 outcomes [12-15].
While boosters are understood to be effective against severe disease, hospitalization [16] and symptomatic infections [12, 17] resulting from the Omicron variant, limited information is available about their effectiveness against asymptomatic and mild symptomatic infections that may go unreported in the absence of asymptomatic surveillance testing. Asymptomatic and mild symptomatic infections play an important role in spreading SARS-CoV-2 [18]. Moreover, the clinical course of COVID-19 is understood to vary by age [19]; current estimates of booster effectiveness based on the general population may not apply to cohorts whose age distribution differs substantially from that of the general population.
We estimate the effectiveness of COVID-19 boosters against SARS-CoV-2 infection in a vaccinated and actively surveilled population of students at Cornell University’s Ithaca campus during December 2021, when the Omicron variant was predominant and 1,870 SARS-CoV-2 infections were identified. Understanding the effectiveness of boosters against infection with the Omicron variant in young adults is particularly important for informing vaccination policies among secondary and post-secondary student populations.
Methods
We used a retrospective observational study to estimate the effectiveness of COVID-19 boosters in reducing Omicron infections in a vaccinated and actively surveilled university student population. We utilized de-identified Ithaca campus student data from Cornell University’s COVID-19 surveillance database. We included polymerase chain reaction (PCR) positive cases identified at Cornell surveillance testing sites, the campus student health service, and a sampling site operated by the local hospital system during the period of 12/5/2021 to 12/31/2021 (referred to as the “Omicron outbreak”), in which we consider the Omicron variant to be the predominant strain. This work was completed as a part of Cornell’s institutional COVID-19 Modeling Team’s contribution to institutional planning and preparedness, and was thus designated as exempt from IRB review.
Study Context
In July 2020, as a part of its reopening strategy, Cornell University implemented a robust COVID-19 surveillance testing program for students, faculty, and staff (1,637,394 PCR tests performed as of February 2, 2022). At the start of December 2021, 23,948 students were enrolled at Cornell’s Ithaca campus. Through mid-December 2021, all undergraduates and professional (veterinary, business, and law) students (n = 16,770) were enrolled in at-least-weekly mandatory PCR surveillance using an anterior nasal swab sample. Additionally, students were asked to seek a PCR test if they were identified as a close contact of a case, if they developed COVID-like symptoms, and before leaving campus at the end of the semester (December 18, 2021). Free PCR testing was available to any constituent of the university 7-days per week. Individuals who tested positive on at-home antigen tests were asked to seek confirmatory PCR testing. Masks were required in all on-campus buildings. COVID-19 vaccination was required for all students starting 8/16/2021, though medical or religious exemptions were granted; On December 21, 2021, Cornell University required students, if eligible, to receive their booster doses by January 31, 2022. Whole genome sequencing confirmed the presence of the Omicron variant in COVID-19 surveillance samples collected on 12/1/2021. The 174 PCR-positive samples collected through surveillance on 12/11/2021 were tested for S-gene dropout and 89.1% presented this marker of the Omicron variant, suggesting predominance of the Omicron variant on the Ithaca campus during the study period.
Study Population
Study inclusion criteria were: being an active student at Cornell’s Ithaca campus subject to mandatory surveillance testing, being fully vaccinated with an FDA-authorized or approved vaccination (BNT162b2, mRNA-1273, or Ad26.COV2.S), and having no positive SARS-CoV-2 PCR test within 90 days before the start of the study period (Figure 1). Students were excluded from the study population if they had invalid vaccination records (n = 167), had unspecified gender (n = 9), were not fully vaccinated (n = 702) or were vaccinated with non-FDA-authorized or approved vaccines (e.g., CoronaVac, ChAdOx1-S, BBIBP-CorV) (n = 717), or tested PCR-positive within 90 days before the start of the study period (n = 73). Our study included 15,102 Cornell students. According to vaccination records that were self-reported by February 8, 2022, 11.3% of the study population (n = 1,706) received a booster on or before 12/5/2021, with the earliest booster dose administered on 8/3/2021. Our analysis does not distinguish the booster vaccine manufacturer, although this information is available in Supplementary Table S1.

Enrollment of the study population. Students were included if they were enrolled in an academic program based at Cornell’s Ithaca campus in Fall 2021, were subject to mandatory surveillance testing, had a valid vaccination record indicating full vaccination with an FDA-authorized or approved vaccine, specified their gender in university records, and had no positive SARS-CoV-2 PCR test within 90 days before the start of the study period.
Statistical Analysis
The primary outcome of our study was PCR-confirmed SARS-CoV-2 infection. To estimate the effectiveness of COVID-19 boosters against SARS-CoV-2 infections during this Omicron-predominant period, we calculated the person-days that each student contributed to the boosted and non-boosted population during the study period. The total number of person-days contributed by a student is the number of days between 12/5/2021 and either their final test date in the study period, or their first PCR-positive test date, whichever comes first. Of the study population, 98.2% of the students contributed at least one person-day (n = 14,830). We assume that booster vaccinations become effective 7 days after administration, based on results from a study of the Israeli general population [20] (Supplementary Figure S1).
We performed logistic regression to estimate the effect of receiving a booster dose on having a positive PCR-based diagnosis during the study period, controlling for gender, student group (undergraduate or professional student), Greek life participation (yes or no), athletic team participation (yes or no), initial vaccine type (BNT162b2, mRNA-1273, or Ad26.COV2.S), and full vaccination date (14 days after 2 doses of BNT162b2 or mRNA-1273, or 14 days after 1 dose of Ad26.COV2.S, grouped into time categories “before May 2021”, “in May 2021”, “in June 2021”, and “after June 2021”). We included student group, Greek life participation, and athletic team participation as covariates because case investigation of data from before the study period suggested that these covariates explained much of the heterogeneity in the risk of infection across students [21]. Undergraduate students were divided into 3 subgroups based on Greek life and athletic team participation. Students who were in both Greek organizations and athletic teams were classified in the Greek organization group. Thus, we had six student groups: (1) undergraduate Greek life participants; (2) undergraduate athletes not in group 1; (3) undergraduates not in groups 1 or 2; (4) law students; (5) business graduate students; (6) veterinary students. Full vaccination date was included as a covariate to adjust for heterogeneous social behavior, inclination to receive vaccination, and the waning of vaccine immune response. The level of observation was person-days. The dependent variable was whether a student tests PCR-positive for COVID-19 on a particular day. We did not include age as a covariate because there is little age variation in the study population (Supplementary Figure S2). The regression model was:

The p-values for the estimated coefficients and the 95% confidence intervals for the adjusted odds ratios were adjusted using the Bonferroni correction [22].
To estimate the effectiveness of a booster dose against Omicron we used

Covariates not statistically significant (P < 0.05) were then eliminated to yield a reduced model to assess the robustness of our results. We further performed a sensitivity analysis on the delay to boosted status, allowing person-days to count as boosted only after this delay after administration had elapsed, varying this delay from the day after booster administration (day 1) to 14 days (Supplementary Figure S1).
We also performed an individual-level Poisson regression to assess the robustness of our conclusions to model specification. Based on their booster status, each individual in the study contributed one or two exposure periods (measured in person-days). We assumed that booster vaccinations become effective 7 days after administration. The dependent variable is whether a student tests PCR-positive for SARS-CoV-2 during the exposure period. An offset equal to log(person-days) is added in the regression model to address varying exposure windows for each individual. The regression model was:

Booster effectiveness was estimated using 1 −incidence rate ratio= 1 −exp(β1).
All statistical analyses were performed in Python (V3.7.11), using the statsmodels package (V0.12.2).
Results
Table 1 describes the distribution of boosters and cases by gender, student group, full vaccination date and initial vaccine type. Boosted students were more likely to be female, professional students, and have an earlier initial vaccine series than unboosted individuals (Table 1). During the study period, a total of 1,870 PCR-positive cases were identified and reported out of 15,102 students included in this analysis (overall infection risk of 12.4%). None of the cases required hospitalization. The overall infection risk among students that received a booster dose on or before 12/5/2021 is 6.6% (112 PCR-positives out of 1,706 boosted students), whereas the infection risk among students that did not receive a booster on or before 12/5/2021 is 13.1% (1,758 PCR-positives out of 13,396 students). The cumulative incidence among students who received a booster before 12/5/2021 was approximately half the cumulative incidence among students who were unboosted at that time (Figure 2). Similarly, based on the person-day statistical analysis, the incidence rate was 0.7 per 100 person-days (118 PCR-positive cases/17,054 person-days) among students who had received the booster dose ≥ 7 days earlier, compared to 1.4 per 100 person-days (1,752 PCR-positive cases/128,585 person-days) among those who had not received the booster dose or had received the booster dose < 7 days earlier.
Distribution of person-day data by gender, student group, fully vaccination date and initial vaccine type.

SARS-CoV-2 infection cumulative incidence rate (number of infections per person) during the study period, broken out by booster dose status.
Table 2 summarizes the results of the full logistic regression model. The booster effectiveness estimate is 52% (95% CI: [37%, 64%]). Since “gender” and “initial vaccine type” were not statistically significant, we built a reduced model (Supplementary Table S2) that yields a nearly–identical booster effectiveness of 52% (95% CI: [37%, 63%]), suggesting that the estimate is robust.
Summary of the full logistic regression model with covariates for gender, student group, full vaccination date, and initial vaccine type.
We further performed a sensitivity analysis to assess the impact of the delay between booster administration and booster effectiveness. Although 5,900 students received their booster dose during the study period (Supplementary Figure S3), 5,158 of them received it after leaving the active surveillance program at the end of the semester. These students did not contribute any person-days to the study after their last surveillance test, so they contributed only unboosted person-days. For students who received a booster dose while in active surveillance, we varied this delay from 1 day to 14 days and calculated the booster effectiveness against infection using the full model (Supplementary Figure S4). The estimated booster effectiveness is consistently above 39%, suggesting that our estimate of booster effectiveness is robust to variation in the time required to mount an effective immune response after booster vaccination. Similarly, the incidence in the boosted population does not vary substantially as we change the assumed delay between booster administration and effectiveness (Supplementary Table S3).
In a separate individual-level Poisson regression analysis (Supplementary Table S4), the booster effectiveness estimated using 1 −incidence rate ratio is 52% (95% CI: [36%, 64%]), consistent with the estimate from the full logistic regression model.
Discussion
This study is one of the first community studies to quantify booster vaccine effectiveness from an actively surveilled population of young adults. Our study provides evidence that booster vaccinations significantly reduce infections in university settings during periods when the Omicron variant is predominant, supporting the implementation of booster vaccination requirements to minimize community transmission.
In this retrospective analysis of SARS-CoV-2 tests performed at the Cornell University’s Ithaca campus during a 27-day period when Omicron was the predominant variant, the incidence of COVID-19 infections was halved among participants vaccinated with a booster dose of an FDA-approved COVID-19 vaccine when compared with fully vaccinated participants without a booster dose. The calculated booster effectiveness was 52% (95% CI: [37%, 64%]), which is slightly lower than a previously reported effectiveness against symptomatic COVID-like illness in adults (66%; 95% CI: [64%, 68%]) in the same time period.[17] We found a substantially smaller reduction in cases than the booster effectiveness against infection reported in a study of national health records during August 2021, when the Delta (B.1.617.2 and AY sublineages) variant was predominant [23]. Importantly, our analysis includes both symptomatic and asymptomatic infections because the student population was under active surveillance. The difference in our estimate compared with that of Bar-On et.al. [23] could be due to differences between Omicron and Delta, a difference in vaccine effectiveness against symptomatic and asymptomatic infections, or differences between young adults and older individuals. Our estimate is similar to the reduction in cumulative incidence of reported infections associated with booster vaccination during an Omicron wave in Los Angeles County [24]. Students vaccinated with Ad26.COV2.S had a higher risk of infection relative to other vaccines, similar to other studies [25]. The difference was not statistically significant in our model, likely because a small number of students had Ad26.COV2.S initial doses (Table 1, Supplementary Table S1).
In addition to boosters, the odds of infection in our fitted regression model depends on the student group and the date of becoming fully vaccinated. The odds of infection was significantly lower among students who became fully vaccinated after May 1, 2021 compared with those becoming fully vaccinated earlier, consistent with waning protection against SARS-CoV-2 infection observed within a few months of completing the initial vaccination series [26]. During the study period, the odds of infection were significantly higher among undergraduate students participating in fraternity and sorority activities or belonging to athletic teams, and among professional students at the business school, when compared with other undergraduates. Varsity athletes and students in Greek-life organizations at institutions of higher education may have more social contact than other undergraduates; thus, consistent with previous studies, this population may be at higher risk for SARS-CoV-2 infection [21, 27, 28]. As in other higher-education institutions [28], contact tracing at Cornell identified Greek-life events as significant spreading events. Local case investigation efforts also pointed to additional events, including post-Thanksgiving break travel and a series of end-of-semester gatherings, as contributing to Omicron spread. With the emergence of highly transmissible variants, travel and social gatherings may put students at increased risk of SARS-CoV-2 infection.
The findings in this study are subject to several limitations. First, our logistic regression analysis assumes that observations are independent across days, which does not reflect the correlation in the level of risk in an individual’s behavior over time. People who avoid risk could also be more likely to get a booster vaccination, which could result in the boosted group having decreased exposure to SARS-CoV-2. Students vaccinated with non-FDA-approved or authorized vaccines were excluded because boosters were not approved at the time of the study for these individuals. Our data also does not allow us to distinguish between booster doses and additional doses for immunocompromised individuals, or to distinguish between asymptomatic and asymptomatic infections for confirmed PCR-positive cases. Although almost 90% of positive samples collected and tested during the study period exhibited S-gene dropout, suggesting they had the Omicron variant at the time of this analysis, and sequencing confirmed the presence of the Omicron variant in all samples sequenced during this period, sequencing of each PCR-positive case was not performed. Moreover, not every individual who was boosted during the study period may have uploaded their vaccination record, which may have led to misclassification bias towards the null. Further, enough COVID-19 cases were observed to provide sufficient statistical power for moderately precise booster effectiveness estimates, but not to estimate how booster effectiveness varies with the manufacturer of the booster dose or the original vaccine. Additionally, most students were boosted with BNT162b2 in this study (Supplementary Table S1). Finally, we did not include information on previous COVID-19 infections and had no information available on the students’ use of non-pharmaceutical interventions, although students were required to wear a mask (cloth, medical, or respirator) while inside campus buildings.
In conclusion, our findings highlighted that booster vaccine doses, relative to being fully vaccinated, are effective in reducing infections in young adults during Omicron-predominant periods. Increasing booster vaccination rates in young adults can reduce community transmission, helping universities and other institutions to remain open safely.
Data Availability
All data presented in the study are available upon reasonable request to the authors. One may contact Cornell University to request the de-identified, source data necessary to replicate the findings in this study.
Author Contributions
JW cleaned the data and performed the regression analyses under the direction of the remaining authors. PF led the study.
Conflict of Interests
The authors report no conflicts of interest.
Supplementary Appendix
Table of Contents
Distribution of booster dose type among students in the study population that received their booster dose on or before 12/5/2021, broken out by initial vaccination and booster dose type.

Allocation of person-days to the control and booster cohorts. The black timeline shows the main analysis, with students having a “boosted” status 7 days after SARS-CoV-2 booster vaccine administration. The red timeline shows one example of our sensitivity analysis varying the time to “boosted” status, with students in this example achieving a “boosted” status 2 days after booster vaccine administration.
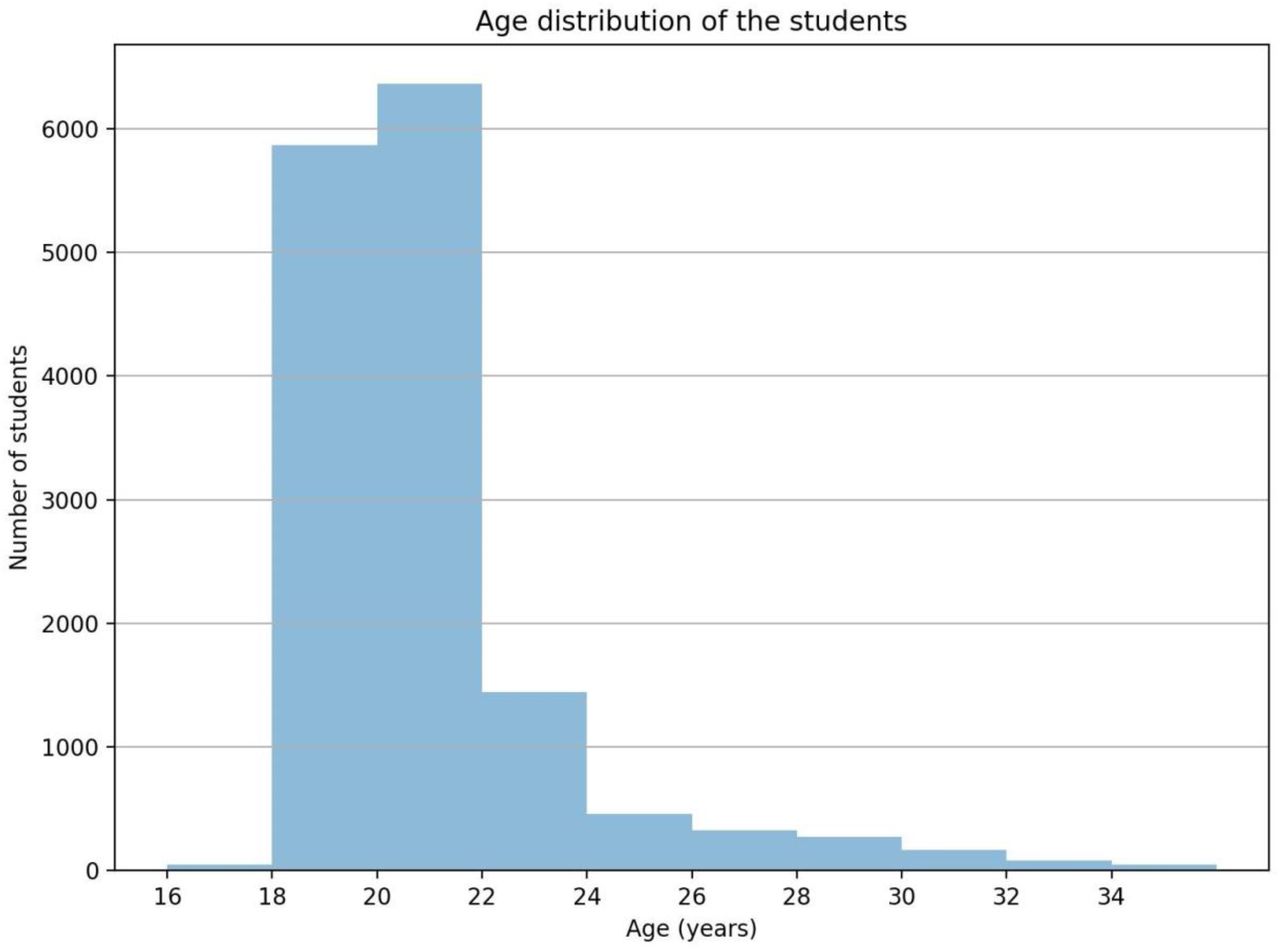
Age distribution of students in the study population (n = 15,102). Age was estimated from birth year. Mean age = 20.6 years; Median age = 20 years; Interquartile range = 2 years.
Summary of the reduced logistic regression model with covariates for student group and full vaccination date.

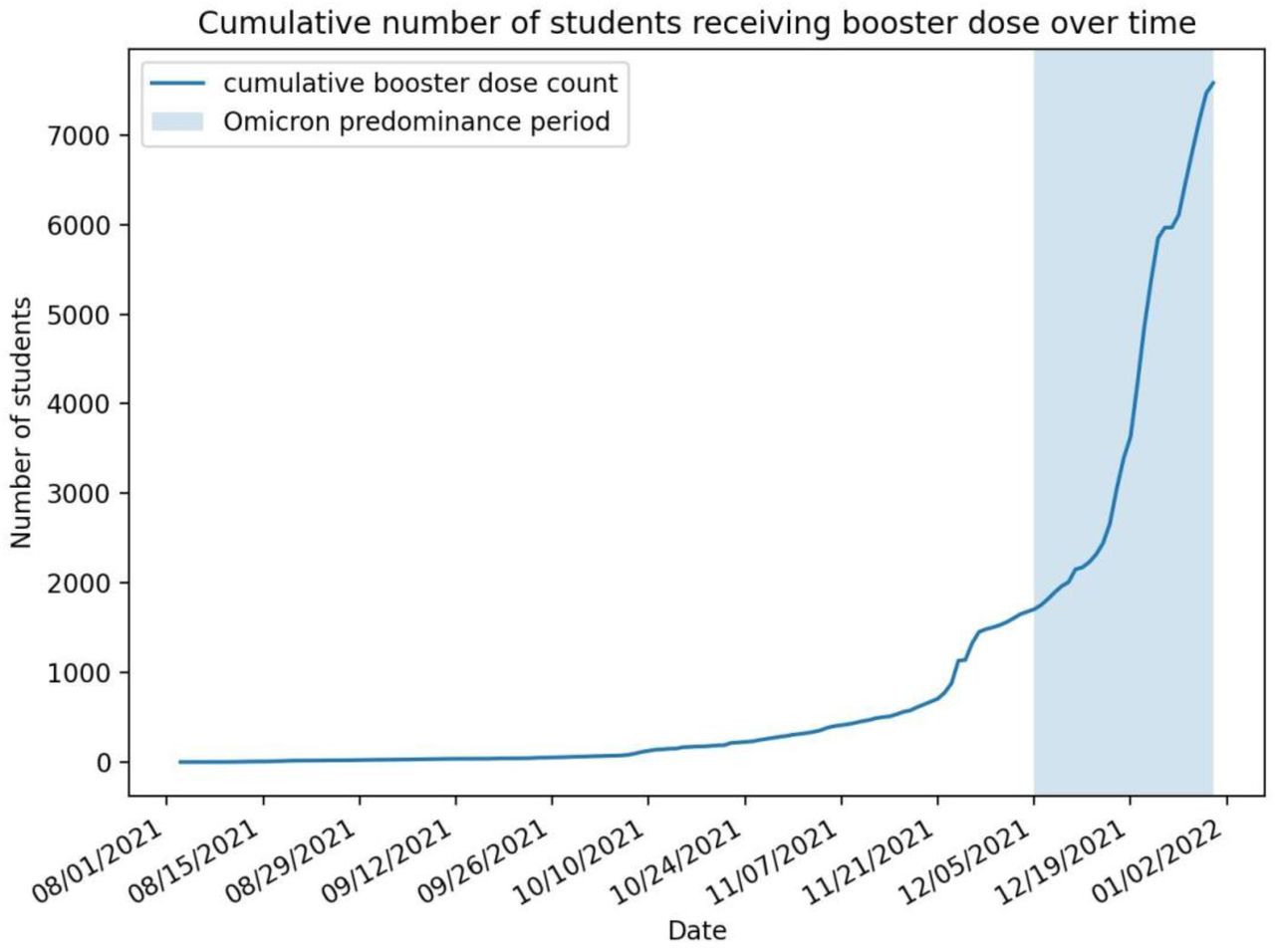
Cumulative number of students receiving COVID-19 booster dose, over time. The shaded region represents the Omicron predominance period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean and 95% confidence interval for the booster effectiveness against Omicron, as we vary the assumed delay for the booster dose to become effective after booster administration.
Number of unboosted and boosted person-days, PCR-positive cases, incidence rate with respect to different assumed delays for the booster to become effective after administration.
Summary of the Poisson regression model with covariates for gender, student group, full vaccination, and initial vaccine type.
Acknowledgments
We would like to thank the large number of people at Cornell University who supported the university’s response to COVID-19. JW and MO were supported by the Cornell University Office of the Provost. PF was supported by AFOSR FA9550-19-1-0283. SH was supported by NSF CMMI-2035086. DS was supported by NSF DCCF-1740822 and NSF DCCF-1522054. CC was supported by The David and Lucile Packard Foundation 2021-72608.
References




