
Abstract
BACKGROUND Natural SARS-CoV-2 infection elicits strong protection against reinfection with the Alpha (B.1.1.7), Beta (B.1.351), and Delta (B.1.617.2) variants. However, the Omicron (B.1.1.529) variant harbors multiple mutations that can mediate immune evasion. We estimated effectiveness of prior infection in preventing reinfection (PES) with Omicron and other SARS-CoV-2 variants in Qatar.
METHODS PES was estimated using the test-negative, case-control study design, employing a methodology that was recently investigated and validated for derivation of robust estimates for PES. Cases (PCR-positive persons with a variant infection) and controls (PCR-negative persons) were exact-matched by sex, 10-year age group, nationality, and calendar time of PCR test, to control for known differences in the risk of exposure to SARS-CoV-2 infection in Qatar.
RESULTS PES against symptomatic reinfection was estimated at 90.2% (95% CI: 60.2-97.6) for Alpha, 84.8% (95% CI: 74.5-91.0) for Beta, 92.0% (95% CI: 87.9-94.7) for Delta, and 56.0% (95% CI: 50.6-60.9) for Omicron. Only 1 Alpha, 2 Beta, 0 Delta, and 2 Omicron reinfections progressed to severe COVID-19. None progressed to critical or fatal COVID-19. PES against hospitalization or death due to reinfection was estimated at 69.4% (95% CI: −143.6-96.2) for Alpha, 88.0% (95% CI: 50.7-97.1) for Beta, 100% (95% CI: 43.3-99.8) for Delta, and 87.8% (95% CI: 47.5-97.1) for Omicron.
CONCLUSIONS Protection afforded by prior infection in preventing symptomatic reinfection with Alpha, Beta, or Delta is robust, at about 90%. While such protection against reinfection with Omicron is lower, it is still considerable at nearly 60%. Prior-infection protection against hospitalization or death at reinfection appears robust, regardless of variant.
Introduction
Natural severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection elicits strong protection against reinfection with the Alpha (B.1.1.7),1,2 Beta (B.1.351),1 and Delta (B.1.617.2)3 variants. However, the Omicron (B.1.1.529) variant harbors multiple mutations that can mediate immune evasion. We estimated effectiveness of prior infection in preventing reinfection (PES) with Omicron and other SARS-CoV-2 variants in Qatar.
Methods
Study population, data sources, and study design
This study was conducted in the resident population of Qatar, applying the test-negative, case-control study design4–6 to investigate the protection afforded by prior SARS-CoV-2 infection in preventing reinfection with SARS-CoV-2 variants. Effectiveness of prior infection in preventing reinfection (PES) was defined as the proportional reduction in susceptibility to infection among those with prior infection versus those without.6,7 The test-negative methodology was recently investigated and validated for the specific derivation of rigorous and robust estimates for SARS-CoV-2 PES.6
Coronavirus Disease 2019 (COVID-19) laboratory testing, vaccination, clinical infection data, and related demographic details were extracted from the national, federated SARS-CoV-2 databases that include all polymerase chain reaction (PCR) testing, COVID-19 vaccinations, and COVID-19 hospitalizations and deaths in Qatar since the start of the pandemic, with no missing information on variables included in this study.
Every PCR test conducted in Qatar is classified based on the reason for testing (clinical symptoms, contact tracing, surveys or random testing campaigns, individual requests, routine healthcare testing, pre-travel, at port of entry, or other). Qatar has unusually young, diverse demographics, in that only 9% of its residents are ≥50 years of age, and 89% are expatriates from over 150 countries.8,9 Nearly all individuals were vaccinated in Qatar, however, vaccinations performed elsewhere were still recorded in the health system at the port of entry upon arrival to Qatar per country requirements.
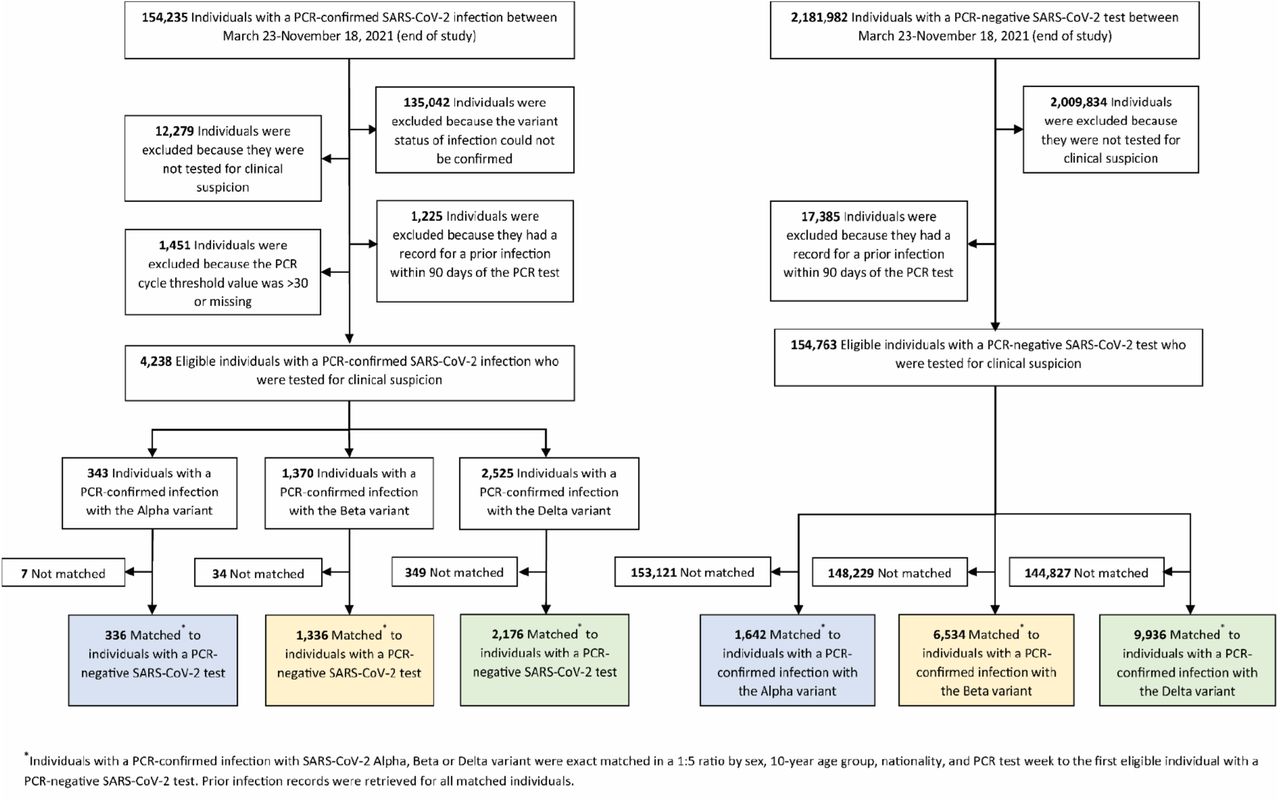
For estimation of PES against the Alpha10 (B.1.1.7), Beta10 (B.1.351), and Delta10 (B.1.617.2) variants, cases (PCR-positive persons with genotyped variant infection) and controls (PCR-negative persons) identified between March 23, 2021 (start of positive samples’ genotyping in Qatar) and November 18, 2021 (prior to suspected introduction of the Omicron variant), were exact matched in a ratio of one-to-five by sex, 10-year age group, nationality, and calendar week of the PCR test (Figure 1 and Table 1). Infection with Alpha, Beta, or Delta variants was ascertained using real-time reverse-transcription PCR (RT-qPCR) genotyping of the positive clinical samples (Section S1).11,12
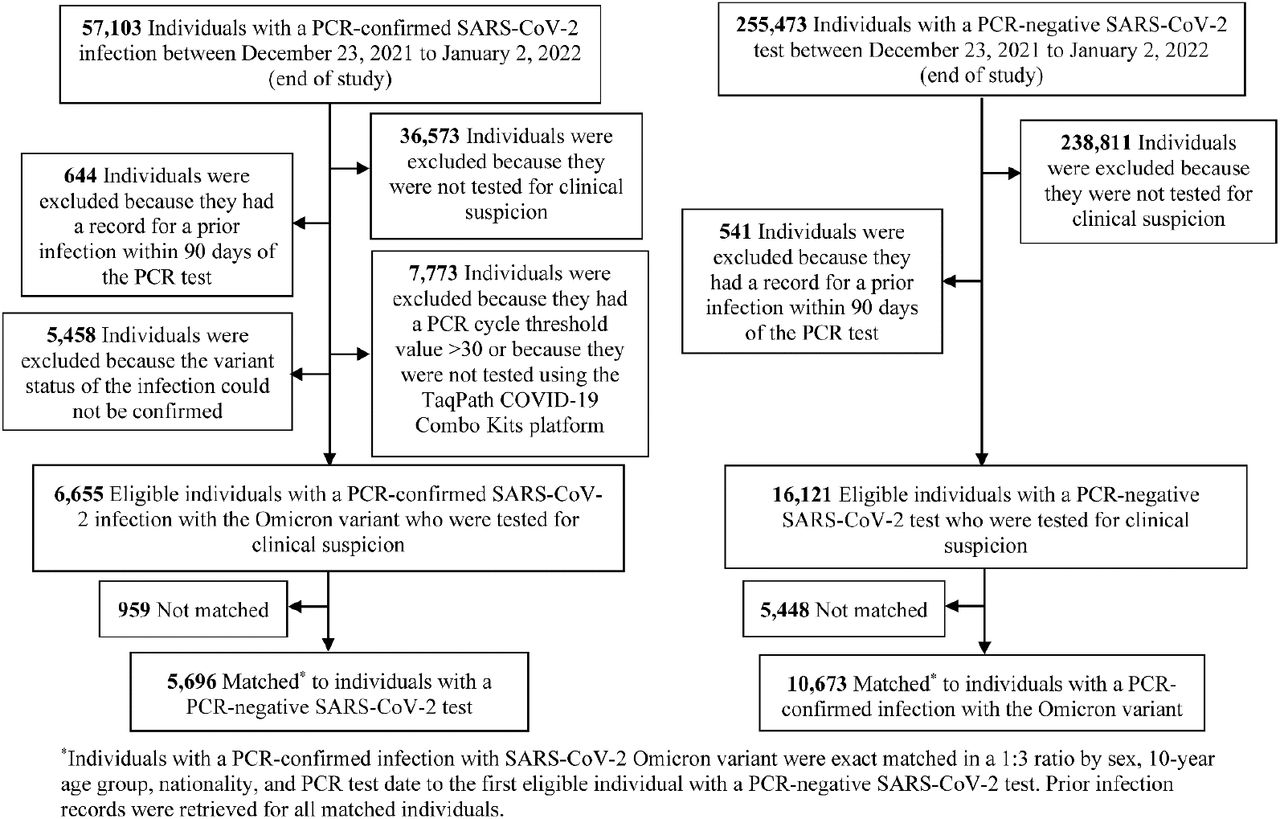
A similar methodology was applied to estimate PES against the Omicron10 (B.1.1.529) variant. However, cases (PCR-positive persons with Omicron infection) and controls (PCR-negative persons) identified between December 23 and January 2, 2022, the time during which the Omicron epidemic wave was exponentially growing in Qatar, were exact matched in a ratio of one-to-three by sex, 10-year age group, nationality, and calendar day of the PCR test (rather than calendar week of the PCR test; Figure 2 and Table 2). A SARS-CoV-2 infection with the Omicron variant was proxied as an S-gene “target failure” case using the TaqPath COVID-19 Combo Kit platform (Thermo Fisher Scientific, USA13) applying the criterion of an RT-qPCR Ct value ≤30 for both the N and ORF1ab genes, but a negative outcome for the S gene.
Description of laboratory methods for the RT-qPCR testing and variant ascertainment are found in Section S1. All PCR testing was conducted at the Hamad Medical Corporation Central Laboratory or at Sidra Medicine Laboratory, following standardized protocols.
Matching of cases and controls was performed to control for known differences in the risk of exposure to SARS-CoV-2 infection in Qatar.9,14–17 Only cases with an RT-qPCR cycle threshold (Ct) value ≤30 and individuals tested because of clinical suspicion, that is presence of symptoms compatible with a respiratory tract infection, were included in analysis. These criteria were applied to ensure that PES is estimated against reinfections with at least some symptomatic disease and epidemiological relevance, as often reinfections occur with negligible symptoms and high Ct values, which are of less public health significance.18
Only the first PCR-positive test for a specific variant of interest was included for each case. A control was defined as the first PCR-negative test for any individual tested for clinical suspicion during the study period.19–23 Prior infection was defined as a PCR-confirmed infection ≥90 days before a new PCR-positive test.7,24 Individuals PCR-positive during the 90 days preceding the PCR test were therefore excluded from both cases and controls. These inclusion and exclusion criteria were implemented to minimize different types of potential bias, as informed by prior analyses.20
Each person who had a PCR-positive test result and hospital admission was subject to an infection severity assessment every three days until discharge or death, regardless of the length of the hospital stay or the time between the PCR-positive test and the final disease outcome.
Classification of COVID-19 case severity (acute-care hospitalization),25 criticality (intensive-care-unit (ICU) hospitalization),25 and fatality26 followed World Health Organization (WHO) guidelines, and assessments were made by trained medical personnel using individual chart reviews (Section S2).
The latter protocol for infection severity assessment was applied for Alpha, Beta, and Delta cases. However, with the recency of the Omicron epidemic wave, assessment of severity, criticality, and fatality of Omicron cases was completed for only a small number of cases. Therefore, only for Omicron cases, any acute-bed hospital admission associated with infection was used as a proxy for COVID-19 severity, and any ICU-bed hospital admission associated with infection was used as a proxy for COVID-19 criticality. Alpha, Beta, Delta, and Omicron cases that progressed to severe,25 critical,25 or fatal26 COVID-19 between the PCR-positive test result and the end of the study were classified based on their worst outcome, starting with death, followed by critical disease, and then severe disease.
Effectiveness of prior infection in preventing severe, critical, or fatal COVID-19 reinfection was also estimated, applying the same methodology. Here, cases (PCR-positive persons with a variant infection that progressed to a severe, critical, or fatal COVID-19) were exact matched to controls (PCR-negative persons) using the matching criteria specified above for each variant type.
The study was approved by the Hamad Medical Corporation and Weill Cornell Medicine-Qatar Institutional Review Boards with a waiver of informed consent. Reporting of the study followed STROBE guidelines (Table S1).
Statistical analysis
All records of PCR testing in Qatar were examined for the selection of cases and controls and ascertainment of prior infection status. However, only matched samples of cases and controls were included in the analysis. Cases and controls were described using frequency distributions and measures of central tendency and compared using standardized mean differences (SMDs). SMD is defined as the difference in the mean of a covariate between groups divided by the pooled standard deviation, with SMD <0.1 indicating optimal balance across groups.
PES was derived as one minus the ratio of the odds of prior infection in cases (PCR-positive persons with variant infection), to the odds of prior infection in controls (PCR-negative persons):6

Odds ratios and associated 95% confidence intervals (CIs) were derived using conditional logistic regression, factoring the matching in the study design. This analytical approach minimizes potential bias that could arise due to variation in epidemic phase4,27 or other confounders.9,14–17,28,29 CIs were not adjusted for multiplicity. Interactions were not investigated.
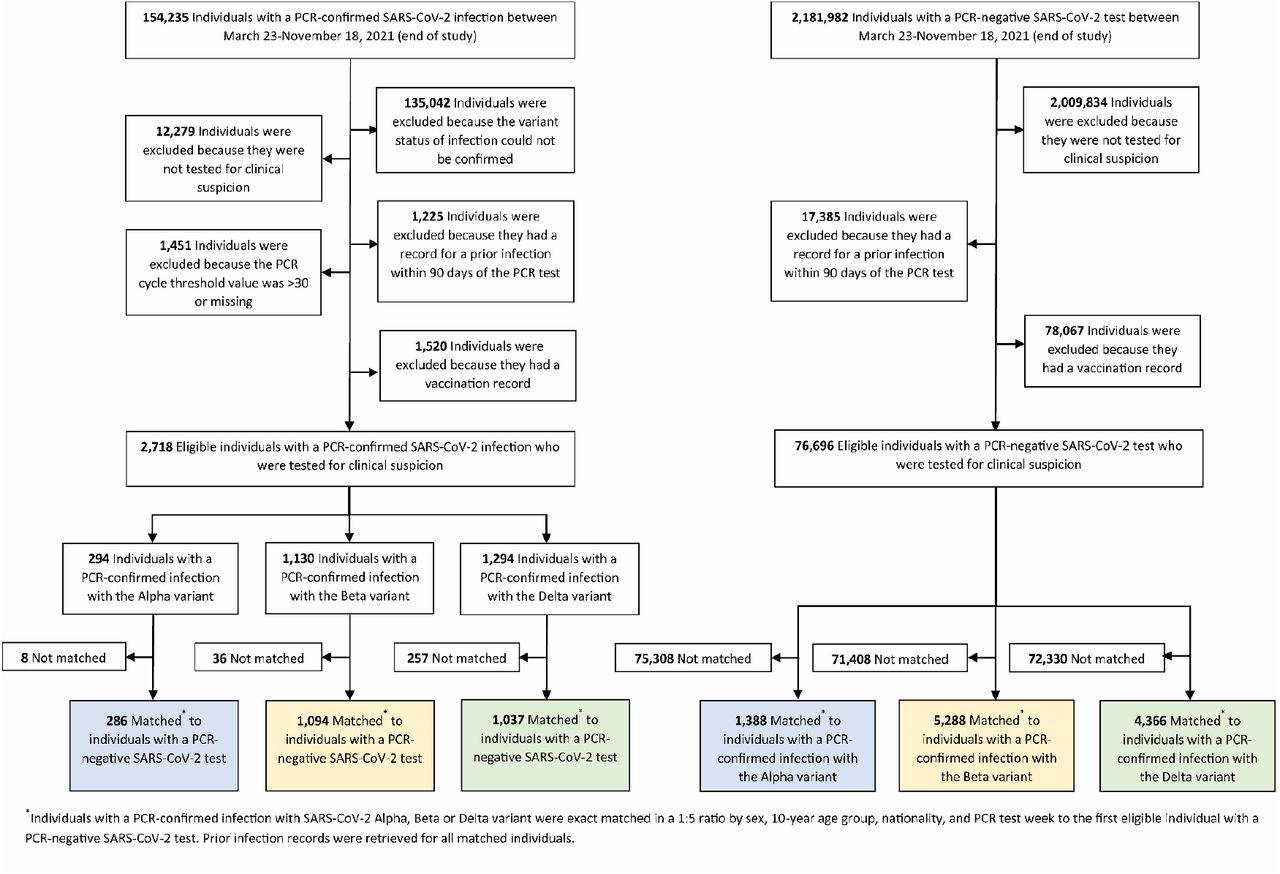
Two sensitivity analyses were conducted to assess the robustness of estimates of PES. The first estimated PES by additionally adjusting for vaccination status in the conditional logistic regression. The second estimated PES after excluding all individuals with a record of vaccination prior to the PCR test used for defining cases and controls (Figures 3 and 4).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results
Figures 1–4 depict the selection of the study populations. Tables 1–2 show study population characteristics. The median time between prior infection and PCR test among cases and controls was 279 days (interquartile range (IQR), 194-313) for Alpha, 284 days (IQR, 210-313) for Beta, 253 days (IQR, 159-375) for Delta, and 314 days (IQR, 268-487) for Omicron.
Table 3 summarizes study results. PES against symptomatic reinfection was estimated at 90.2% (95% CI: 60.2-97.6) for Alpha, 84.8% (95% CI: 74.5-91.0) for Beta, 92.0% (95% CI: 87.9-94.7) for Delta, and 56.0% (95% CI: 50.6-60.9) for Omicron. Sensitivity analyses, adjusting for vaccination status or excluding vaccinated subjects from the analysis, confirmed the study results (Table 3), as expected for this study design, which is robust, irrespective of the approach employed to control for vaccine-induced immunity.6
Only 1 Alpha, 2 Beta, 0 Delta, and 2 Omicron reinfections progressed to severe COVID-19 (Table 3). None progressed to critical or fatal COVID-19. PES against hospitalization or death due to reinfection was estimated at 69.4% (95% CI: −143.6-96.2) for Alpha, 88.0% (95% CI: 50.7-97.1) for Beta, 100% (95% CI: 43.3-99.8) for Delta, and 87.8% (95% CI: 47.5-97.1) for Omicron.
Discussion
Protection afforded by prior infection in preventing symptomatic reinfection with Alpha, Beta, or Delta is robust, at about 90%, confirming earlier estimates.1–3 While such protection against reinfection with Omicron is lower, it is still considerable at nearly 60%. Prior-infection protection against hospitalization or death at reinfection appears robust, regardless of variant.
Individual-level data on co-morbid conditions were not available; therefore, they could not be explicitly factored into our analysis. However, only a small proportion of the study population may have had serious co-morbid conditions. Only 9% of the population of Qatar are ≥50 years of age,8,9 and 60% are young, expatriate craft and manual workers working in mega-development projects.16,17,30 The national list of persons prioritized to receive the vaccine during the first phase of vaccine roll-out included only 19,800 individuals of all age groups with serious co-morbid conditions. Matching of cases and controls on age may have indirectly and partially adjusted for presence of co-morbidities. With the young population of Qatar, our findings may not be generalizable to other countries where elderly citizens constitute a larger proportion of the total population.
PES was assessed using an observational, test-negative, case-control study design,6 rather than a cohort study design where individuals are followed up over time. However, the cohort study design applied in earlier analyses to estimate PES in the same population of Qatar yielded findings similar to those of the test-negative case-control design,1,2,6,7,31 supporting the validity of this design in estimating PES. It even appears that the test-negative study design may be less susceptible to some forms of bias than the cohort study design.6
Nonetheless, one cannot exclude the possibility that in real-world data, bias could arise in unexpected ways, or from unknown sources, such as subtle differences in test-seeking behavior or changes in the pattern of testing with introduction of other testing modalities, such as rapid antigen testing.
Notwithstanding these limitations, consistent findings were reached in both the main and sensitivity analyses. Estimates for the effectiveness of prior infection against reinfection with the Alpha and Beta variants were also consistent and similar to those generated earlier in the same population of Qatar using cohort study designs.1,2
Data Availability
The dataset of this study is a property of the Qatar Ministry of Public Health that was provided to the researchers through a restricted-access agreement that prevents sharing the dataset with a third party or publicly. Future access to this dataset can be considered through a direct application for data access to Her Excellency the Minister of Public Health (https://www.moph.gov.qa/english/Pages/default.aspx). Aggregate data are available within the manuscript and its Supplementary information.
Author contributions
HNA and HC co-designed the study, performed the statistical analyses, and co-wrote the first draft of the article. LJA conceived and co-designed the study, led the statistical analyses, and co-wrote the first draft of the article. PT and MRH conducted the multiplex, RT-qPCR variant screening and viral genome sequencing. HY, FMB, and HAK conducted viral genome sequencing. All authors contributed to data collection and acquisition, database development, discussion and interpretation of the results, and to the writing of the manuscript. All authors have read and approved the final manuscript.
Competing interests
Dr. Butt has received institutional grant funding from Gilead Sciences unrelated to the work presented in this paper. Otherwise we declare no competing interests.
Supplementary Appendix
Section S1. Laboratory methods
Real-time reverse-transcription polymerase chain reaction testing
Nasopharyngeal and/or oropharyngeal swabs were collected for polymerase chain reaction (PCR) testing and placed in Universal Transport Medium (UTM). Aliquots of UTM were: extracted on a QIAsymphony platform (QIAGEN, USA) and tested with real-time reverse-transcription PCR (RT-qPCR) using TaqPath COVID-19 Combo Kits (Thermo Fisher Scientific, USA) on an ABI 7500 FAST (Thermo Fisher, USA); tested directly on the Cepheid GeneXpert system using the Xpert Xpress SARS-CoV-2 (Cepheid, USA); or loaded directly into a Roche cobas 6800 system and assayed with a cobas SARS-CoV-2 Test (Roche, Switzerland). The first assay targets the viral S, N, and ORF1ab gene regions. The second targets the viral N and E-gene regions, and the third targets the ORF1ab and E-gene regions.
All PCR testing was conducted at the Hamad Medical Corporation Central Laboratory or Sidra Medicine Laboratory, following standardized protocols.
Classification of infections by variant type
Surveillance for SARS-CoV-2 variants in Qatar is mainly based on viral genome sequencing and multiplex RT-qPCR variant screening1 of random positive clinical samples,2–7 complemented by deep sequencing of wastewater samples.4,8
Between March 23, 2021 and November 18, 2021 (prior to suspected introduction of the Omicron variant), RT-qPCR genotyping of 19,234 randomly collected SARS-CoV-2-positive specimens on a weekly basis identified 3,494 (18.2%) Alpha (B.1.1.7)-like cases, 5,768 (30.0%)
Beta (B.1.351)-like cases, 9,914 (51.5%) “other” variant cases, and 58 (0.3%) B.1.375-like or B.1.258-like cases.4,6
The accuracy of the RT-qPCR genotyping was verified against either Sanger sequencing of the receptor-binding domain (RBD) of SARS-CoV-2 surface glycoprotein (S) gene, or by viral whole-genome sequencing on a Nanopore GridION sequencing device. From 236 random samples (27 Alpha-like, 186 Beta-like, and 23 “other” variants), PCR genotyping results for Alpha-like, Beta-like, and ‘other’ variants were in 88.8% (23 out of 27), 99.5% (185 out of 186), and 100% (23 out of 23) agreement with the SARS-CoV-2 lineages assigned by sequencing.
Within the “other” variant category, Sanger sequencing and/or Illumina sequencing of the RBD of SARS-CoV-2 spike gene on 728 random samples confirmed that 701 (96.3%) were Delta cases and 17 (2.3%) were other variant cases, with 10 (1.4%) samples failing lineage assignment.6,8 Accordingly, a Delta case was proxied as any “other” case identified through the RT-qPCR based variant screening.
All the variant RT-qPCR screening was conducted at the Sidra Medicine Laboratory following standardized protocols.
Surveillance for Omicron infection was performed using the TaqPath COVID-19 Combo Kit platform (Thermo Fisher Scientific, USA9) applying the criterion of an RT-qPCR Ct value ≤30 for both the N and ORF1ab genes, but a negative outcome for the S gene (S-gene “target failure”).
Section S2. COVID-19 severity, criticality, and fatality classification
Severe Coronavirus Disease 2019 (COVID-19) disease was defined per the World health Organization (WHO) classification as a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infected person with “oxygen saturation of <90% on room air, and/or respiratory rate of >30 breaths/minute in adults and children >5 years old (or ≥60 breaths/minute in children <2 months old or ≥50 breaths/minute in children 2-11 months old or ≥40 breaths/minute in children 1–5 years old), and/or signs of severe respiratory distress (accessory muscle use and inability to complete full sentences, and, in children, very severe chest wall indrawing, grunting, central cyanosis, or presence of any other general danger signs)”.10 Detailed WHO criteria for classifying SARS-CoV-2 infection severity can be found in the WHO technical report.10
Critical COVID-19 disease was defined per WHO classification as a SARS-CoV-2 infected person with “acute respiratory distress syndrome, sepsis, septic shock, or other conditions that would normally require the provision of life sustaining therapies such as mechanical ventilation (invasive or non-invasive) or vasopressor therapy”.10 Detailed WHO criteria for classifying SARS-CoV-2 infection criticality can be found in the WHO technical report.10
COVID-19 death was defined per WHO classification as “a death resulting from a clinically compatible illness, in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death that cannot be related to COVID-19 disease (e.g. trauma). There should be no period of complete recovery from COVID-19 between illness and death. A death due to COVID-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of preexisting conditions that are suspected of triggering a severe course of COVID-19”. Detailed WHO criteria for classifying COVID-19 death can be found in the WHO technical report.11
Acknowledgements
We acknowledge the many dedicated individuals at Hamad Medical Corporation, the Ministry of Public Health, the Primary Health Care Corporation, the Qatar Biobank, Sidra Medicine, and Weill Cornell Medicine – Qatar for their diligent efforts and contributions to make this study possible.
The authors are grateful for support from the Biomedical Research Program and the Biostatistics, Epidemiology, and Biomathematics Research Core, both at Weill Cornell Medicine-Qatar, as well as for support provided by the Ministry of Public Health, Hamad Medical Corporation, and Sidra Medicine. The authors are also grateful for the Qatar Genome Programme and Qatar University Biomedical Research Center for institutional support for the reagents needed for the viral genome sequencing. Statements made herein are solely the responsibility of the authors.
The funders of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the article.
References




