
Summary
Background Vaccines have greatly reduced the impact of COVID-19 globally. Unfortunately, evidence indicates that immunity wanes following vaccination, especially with the Delta variant (B.1.617.2). Protection against severe disease and death remain high, but protection against milder disease and infection have dropped significantly. A third “booster” dose of two-dose vaccines has been approved in several countries to individuals at higher risk of severe disease to protect those individuals, but the benefit to boosting immunity in younger healthy individuals and the effects on transmission are less clear.
Methods Here we use relationships between neutralizing antibody titers and vaccine protection against infection and transmission, combined with data on waning and boosting of neutralizing antibody titers to examine the impact of a third dose of the Pfizer vaccine on infection and transmission and its impact on the pathogen effective reproductive number Rt.
Findings Eight months of waning reduced protection of the Pfizer vaccine against all infections from 80.0% (95% CI: 77% to 83%) to 60.4% (95% CI: 53% to 67%); a third dose (which increased neutralizing antibody titers 25.9-fold relative to levels after 8 months of waning) increased protection to 87.2% (95% CI: 83% to 91%). Increased protection against infection and transmission from third doses reduced Rt by 21% to 66% depending on vaccine coverage and previous infection and reduced Rt below 1 when vaccination coverage was high or contact rates were well below pre-pandemic levels.
Interpretation A third dose of the Pfizer vaccine could reduce transmission of SARS-CoV-2, which would reduce infection in unvaccinated individuals and breakthrough infections in vaccinated individuals. While vaccination of unvaccinated individuals, especially in developing countries, would be more effective for reducing disease than providing a third dose to vaccinated individuals, the benefit of a third dose in reducing transmission is sizeable and increases with vaccine coverage and contact rates among individuals.
Funding California Department of Health, National Science Foundation
Introduction
The emergence of the Delta variant (B.1.617.2) of SARS-CoV-2 has caused a surge of infections globally, even in populations with high vaccination coverage [1]. This is due, in part, to the much higher infectiousness of this virus variant [2], moderate immune evasion [3-5], and, increasingly, waning vaccine immunity, based on both levels of neutralizing antibodies [6-9] and studies of vaccine effectiveness [10-12]. Several countries have recently offered third doses to individuals at higher risk of severe disease [13] because protection for these individuals, even against severe disease, has waned the most [10]. However, protection against severe disease for heathy individuals has waned far less and the need and benefit of providing third doses for young healthy individuals has been questioned [14]. Many populations, especially those in Africa, have received very few vaccine doses and many have argued that vaccinating these populations would provide a larger public health benefit than providing third doses to already vaccinated individuals [14] and for reducing the evolutionary potential of the virus [15].
While the direct benefit of providing third doses to elderly and other at-risk individuals is now clear [16], the indirect benefit for reducing transmission of SARS-CoV-2 is poorly understood. Most studies examining waning of vaccine effectiveness over time have focused on protection against symptomatic disease [10-12]. The impact of waning immunity and boosting on vaccine protection against all infections (symptomatic and asymptomatic) and against virus transmission has been mentioned [14], but not quantified, despite its potential importance for reducing infection in unvaccinated individuals and breakthrough infections in vaccinated individuals.
Here we extend a previous approach that showed strong correlations between a measure of immunity, neutralizing antibody titers and vaccine protection [17]. This study examined protection against symptomatic disease against non-Delta variants using data from randomized control trials [17]. We extend this approach by mapping neutralizing antibody titers to protection against both symptomatic disease and all infections for both Delta and non-Delta variants. We then use measurements of waning neutralizing antibody titers and boosting with a third dose to estimate the impact on protection against all infections, and the reproductive number of the virus, Rt which quantifies the average number of cases that each case goes on to infect.
Methods
Protection against infection, disease, and transmission
We collected data from the literature (including ongoing systematic reviews: [18, 19]) on protective efficacy and effectiveness of vaccines and convalescent sera for SARS-CoV-2 and categorized each study by variant type (Delta and non-Delta; estimates of protection against the Beta variant were excluded) and endpoint (symptomatic infections and all infections) (Table S1). We excluded studies of protection where the endpoint was “any infection” because these studies do not capture all infections; they include an unknown fraction of the asymptomatic infections. We also obtained a lower bound of the estimate of vaccine effectiveness against transmission (given infection) for Astrazeneca (ChAdOx1) and Pfizer-BioNTech (BNT162b2) for the Delta variant [20]. This study quantified secondary attack rates using qPCR tests of contacts that were symptomatic or tested positive using lateral flow tests [20], but likely missed some asymptomatic or mildly symptomatic infected contacts, and thus provides a lower estimate of protection. We gathered neutralizing antibody titer data for each vaccine and ratios of titers to convalescent sera from [17]. Finally, we estimated the ratio of neutralizing antibody titers to the Delta variant relative to earlier variants (Table S2), and used these to adjust neutralizing antibody titer ratio estimates in analyses with vaccine effectiveness or protection from previous infection against the Delta variant (Table S1).
Estimating neutralizing antibody titers after waning and third doses
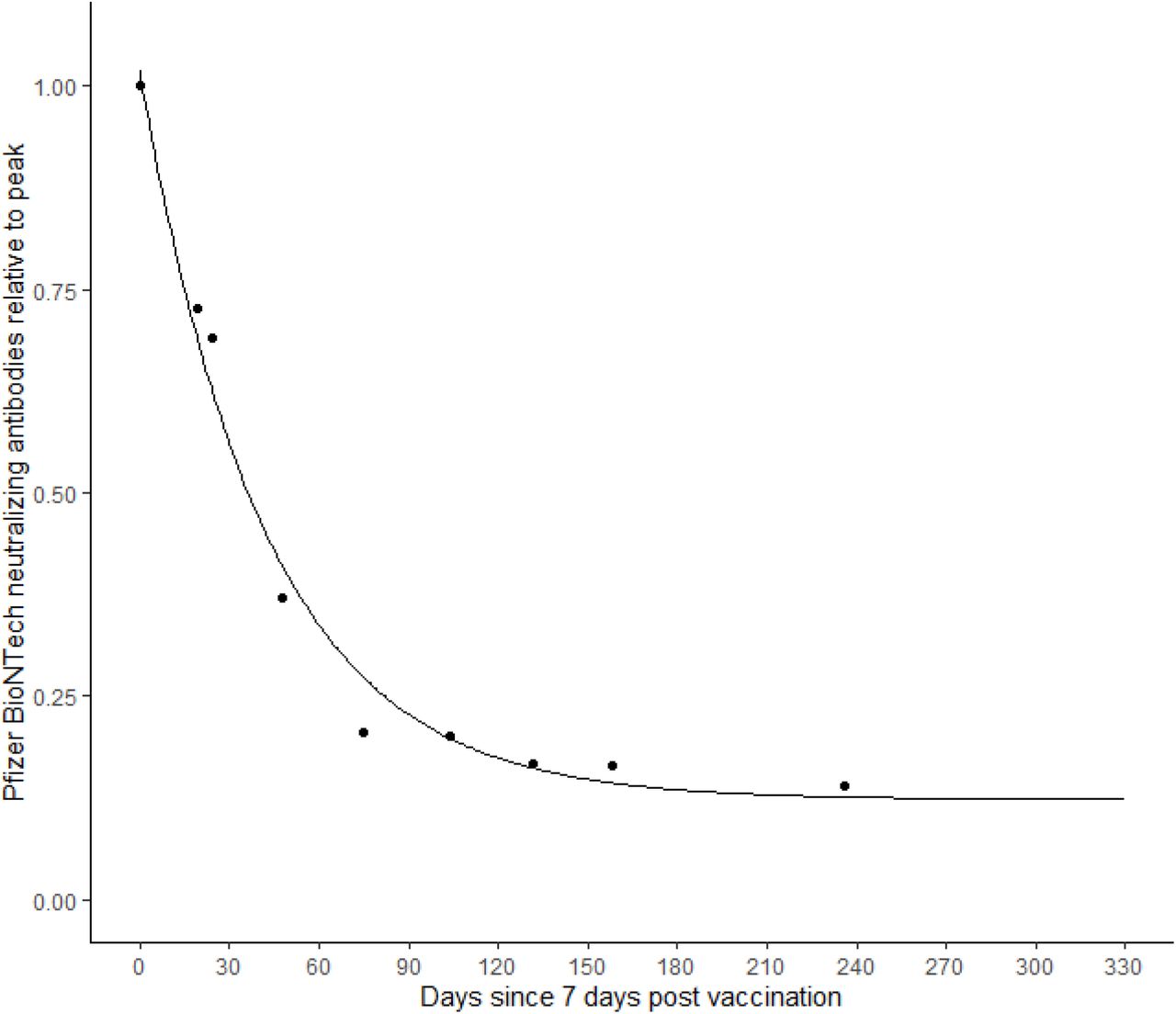
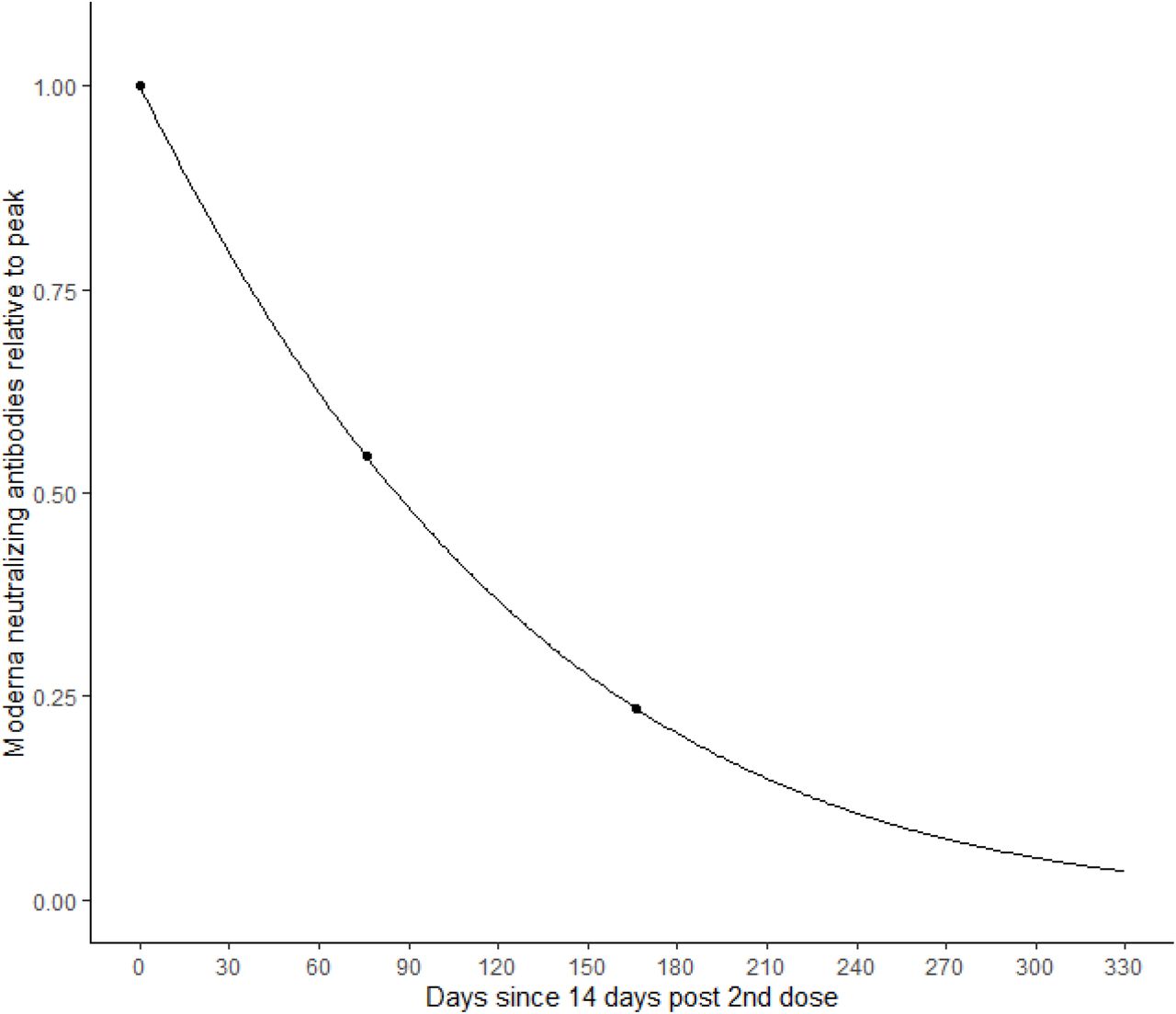
We obtained data on neutralizing antibody titers following vaccination for the Pfizer-BioNTech vaccine at several time points between 1 month after the second dose and 8 months post second dose, as well as 1 month after a third dose [9, 21]. One of these studies [21] reported data for two age groups separately (18-55 and 65+), so we weighted these estimates by the fraction of individuals in the age groups 18-60 and 60+ in the United States (71.0% and 29.0%), which is similar to the age distribution in the European Union [22]. We fit these data to a 3-parameter exponentially decaying function (y = c0ec1*t+c2) to estimate the neutralizing antibody titer on any day, t, post vaccination (Figure S1). We also fit similar relationships to data on neutralizing antibody titers over time for the Moderna vaccine [8] (Figure S2), and following infection with SARS-CoV-2 [6] (starting when titers peak at 25 days post symptom onset [23]) (Figure S3). Rates of waning for hybrid immunity following infection and vaccination with Pfizer-BioNtech and Moderna vaccines combined were statistically similar to rates of waning following vaccination with Pfizer-BioNtech [7], so we used the same relative rates of waning as for Pfizer-BioNtech (Figure S1) but adjusted titers for the much higher initial level in those with hybrid immunity [7]. We assumed that boosting individuals that had been infected and then vaccinated resulted in similar neutralizing antibody titers as people that had been vaccinated but not previously infected, because after 6 months of waning post-vaccination, these individuals with hybrid immunity had neutralizing antibody titers that had fallen below levels for newly vaccinated individuals [7].
Linking protection against infection and disease with neutralizing antibody titers
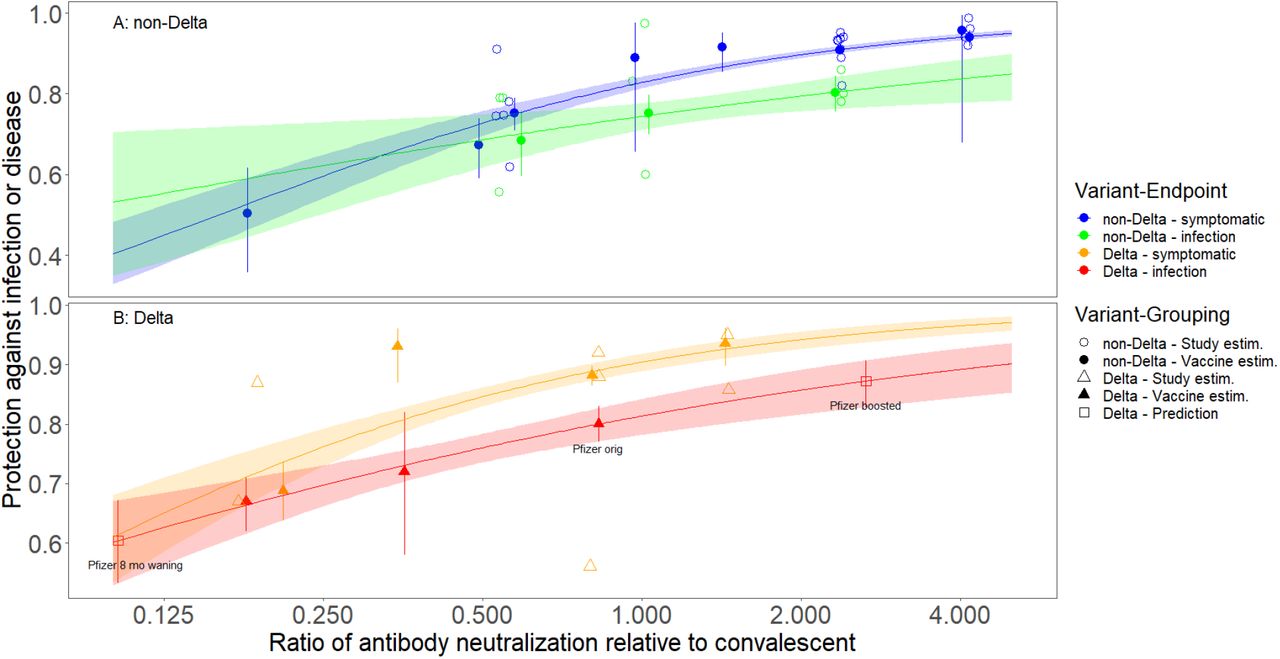
We modeled the relationship between protection from SARS-CoV-2 infections or disease and the ratio of neutralizing antibody titers relative to convalescent sera using logistic regression, following a previous approach [17]. In this analysis each data point is a single study of protection against SARS-CoV-2 infection or disease for a single virus variant. We included an interaction between neutralizing antibody titers and variant-endpoint to estimate separate relationships for each of four variant-endpoints (pairwise combinations of Delta and non-Delta, symptomatic disease, and all infections). We used the separate relationship for the Delta – all infections endpoint for all analyses described below.
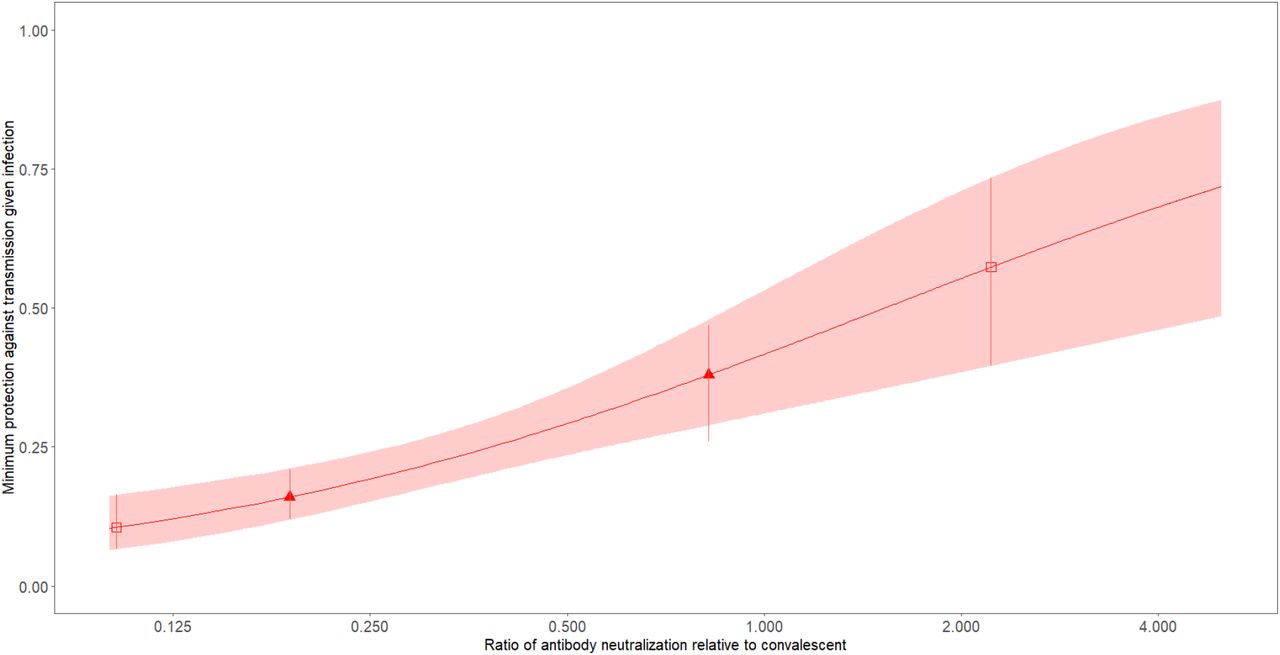
The raw data for each estimate of protection (vaccine efficacy, vaccine effectiveness, or protection from previous infection) were unavailable, so we determined the effective sample sizes for a sample from a binomial distribution that matched the confidence intervals of the protection estimates (Table S1). We used the fitted model (Figure 1) to estimate protection against all infections for the Delta variant from Pfizer - BioNTech vaccination using neutralizing antibody titers measured after eight months of waning and titers measured after a 3rd dose [21]. We performed a similar analysis using the limited data available to link neutralizing antibody titers to the minimum protection against transmission given infection [20] (Figure S4).

The impact of a third dose on the reproductive number, Rt
We used patterns of waning and boosting of neutralizing antibody titers and the relationships between neutralizing antibody titers and protection against all infections and transmission to estimate the impact of providing a third dose of the Pfizer – BioNTech vaccine to increasing fractions of vaccinated individuals on the reproductive number of SARS-CoV-2, Rt. The effective reproductive number, Rt, is the average number of secondary cases that each case infects. It is equal to the basic reproductive number for a fully susceptible population, R0, multiplied by the fraction of the population that is still susceptible. We split the population based on vaccination and infection to determine the effective fraction susceptible: fraction previously infected and unvaccinated, fPU, fraction previously infected and vaccinated, fPV; fraction unvaccinated, fU, fraction vaccinated (with two doses of either Pfizer-BioNtech or Moderna), fV, and fraction boosted with a third dose, fB (fU+fV+fB=1). We estimated the susceptibility of each group using estimates of the protection against infection, VEI, (Figure 1) and the minimum reduced probability of transmitting given infection, VET, (Figure S4) for each group using the subscripts above, except VEIH and VETH which are estimates of protection from hybrid immunity from infection and vaccination. We used these estimates of protection to calculate Rt for five groups of people : fully susceptible unvaccinated (1-fP)fU, previously infected unvaccinated fPfU, previously uninfected vaccinated (1-fP)fV, previously infected vaccinated fPfV, and previously uninfected vaccinated and boosted with a third dose (1-fP)fB:
 We examined the effect of boosting vaccinated individuals with a third dose by considering five scenarios that differ in contact rates/R0 (R0 = 3.7 or 7 reflecting mid-summer 2021 levels in the USA and pre-pandemic behavior, respectively), vaccination coverage (56% similar to USA in mid-October [22]; 60%, 75% and 100%), and the fraction of the population previously infected (0.5%, 28.2% and 56.4%, with the last value being similar to estimates of the fraction of the USA population that had been infected by mid-October, based on 44 million cases and an infection to case ratio of 4.2 [24]). The scenarios and rationale were (Table S3):
We examined the effect of boosting vaccinated individuals with a third dose by considering five scenarios that differ in contact rates/R0 (R0 = 3.7 or 7 reflecting mid-summer 2021 levels in the USA and pre-pandemic behavior, respectively), vaccination coverage (56% similar to USA in mid-October [22]; 60%, 75% and 100%), and the fraction of the population previously infected (0.5%, 28.2% and 56.4%, with the last value being similar to estimates of the fraction of the USA population that had been infected by mid-October, based on 44 million cases and an infection to case ratio of 4.2 [24]). The scenarios and rationale were (Table S3):
R0 = 3.7, 56% vaccinated, 56.4% previously infected: approximates USA population in mid-October with contact rates similar to summer 2021, as might occur in winter 2021S
R0 = 3.7, 60% vaccinated, 0.5% previously infected: approximates countries/populations that effectively suppressed transmission and haven’t yet reached high vaccination levels and have somewhat reduced contact rates (e.g. New Zealand, Australia, Hong Kong, etc.)
R0 = 3.7, 75% vaccinated, 28.2% previously infected: approximates some populations with higher vaccination and lower fraction infected than scenario (1) (e.g. California)
R0 = 7, 100% vaccinated, 56.4% previously infected: a hypothetical optimistic scenario to compare to scenario (1) to determine if vaccination with or without boosting could limit transmission if behavior returns to pre-pandemic levels
R0 = 7, 56% vaccinated, 56.4% previously infected: a more realistic optimistic scenario to compare to scenario (1) to determine if boosting could limit transmission if behavior returns to pre-pandemic levels
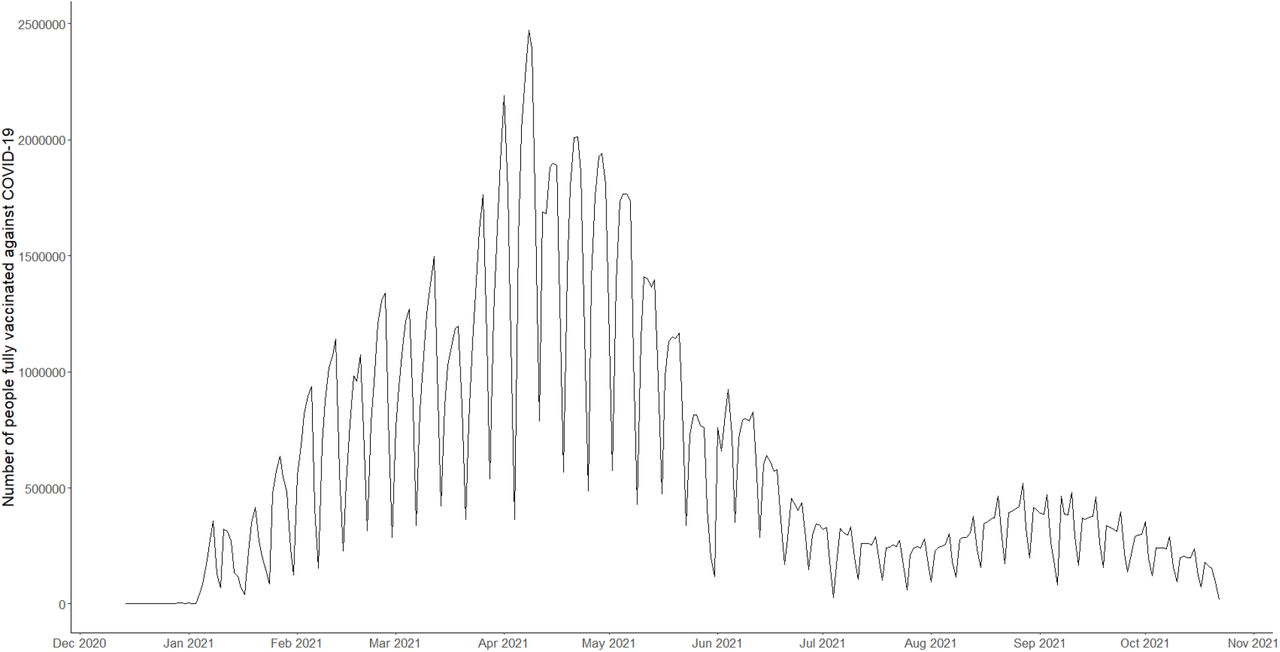
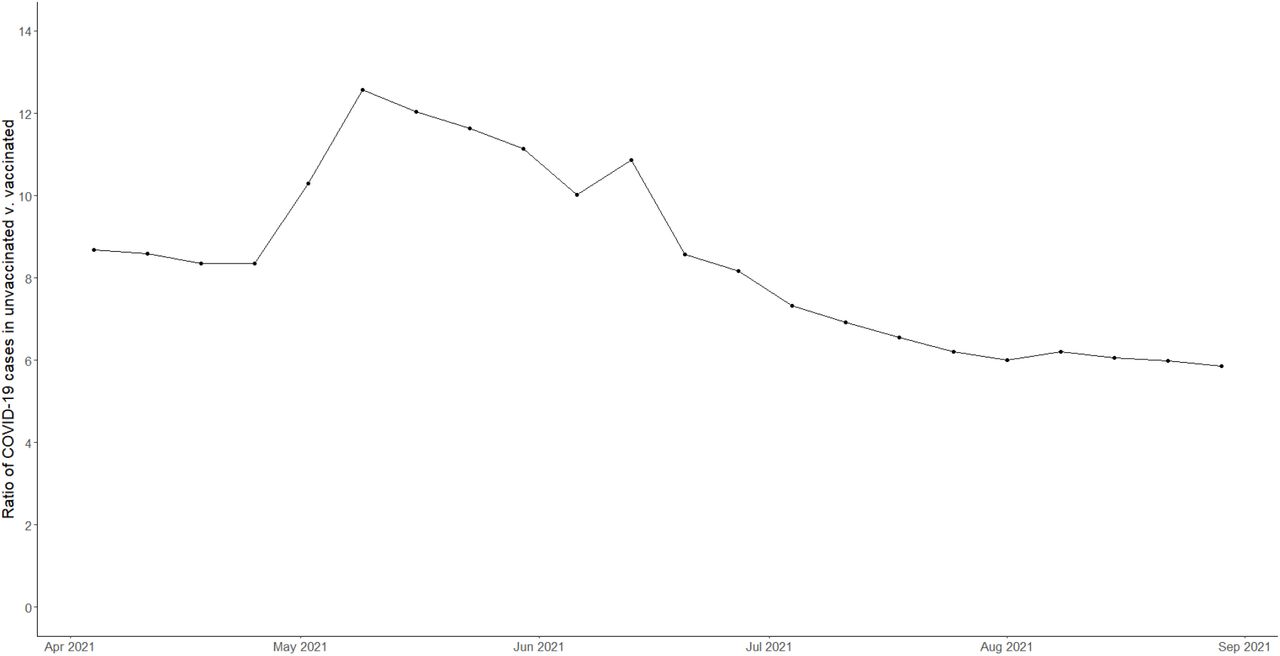
For all scenarios we estimated the waning of vaccine-derived immunity as of October 15, 2021 using the timing of vaccination in the USA [25]; Figure S5) and patterns of waning neutralizing antibody titers over time for Pfizer-BioNtech (Figure S1) and Moderna vaccines (Figure S2) or hybrid immunity (Figure S1 with a higher initial starting value – see above). We estimated the waning of infection-derived immunity as of October 15, 2021 using the timing of deaths in the USA [22] shifted by 24 days [26] (Figure S6) and the rate of waning of infection-derived immunity (Figure S3). We estimated the number of infections in vaccinated and unvaccinated people using the ratios of cases in these two groups over time [27] (Figure S7). We used these data on the timing of vaccination and infection and rates of antibody waning to determine the protection against infection and transmission as of October 15, 2021 (Table S4). We calculated 95% CIs for predicted values of Rt that incorporated uncertainty in the relationships between neutralizing antibody titers and protection against infection and transmission (Figures 1 and S4). We drew 10,000 samples from a uniform distribution c(0,1) and used these as quantiles for a normal distribution to generate draws (on a logit scale) for values of protection VE for each value of neutralizing antibody titer adjusted for waning for the fraction of the population that was vaccinated or infected at each day in the past. This approach essentially drew a single line from the 95% CI of lines in Figure 1 and used that for all levels of waning. We then inverse-logit transformed these values of VE and used them to generate 10,000 values of Rt for that scenario. We took the 2.5% and 97.5% quantiles to estimate the 95% confidence intervals (CIs) for Rt for each point of each scenario.
Results
There were strong relationships between the ratio of neutralizing antibody titers to convalescent sera and protection against both symptomatic infection and all infections (Figure 1; Table S3). Protection was highest for symptomatic disease for non-Delta variants and lower for protection against all infections for both non-Delta and Delta variants (Figure 1; Table S3).
Neutralizing antibodies generated by vaccination with the Pfizer-BioNtech vaccine wane 8.06-fold after 8 months (Figure 1), with most of this waning occurring in the first 3 months (Figure S1). The strong relationship between protection and neutralizing antibody titers (Figure 1; Table S3) suggests that this waning of neutralizing antibody titers will reduce protection against all infections for the Delta variant from 80.0% (95% CI: 77.0% to 83.0%) to 60.4% (95% CI: 53.3% to 67.2%) (Figure 1, red line, compare points labelled “Pfizer 1 week” to “Pfizer 8 mo waning”). Similarly, this waning reduced the minimum protection against transmission given infection from 38% (95% CI: 28% to 47%) to 10.5% (95% CI: 6.6% to 16.4%) (Figure S4). A third dose of the Pfizer-BioNtech vaccine boosted antibody titers 25.9-fold relative to levels after 8 months of waning, or 25.9/8.06 = 3.22 higher than one week after dose 2 [21]. The fitted relationship (Figure 1; Table S3) suggests a third dose of the Pfizer-BioNtech vaccine would increase protection against infection from an eight-month waned value of 60.4% (95% CI: 53.3% to 67.2%) to a boosted value of 87.2% (95% CI: 82.8% to 90.7%) and would boost minimum protection against transmission given infection from 10.5% to 60.7% (95% CI: 42.3% to 76.5%).
Boosting immunity, by providing a third dose of the Pfizer-BioNtech to all doubly vaccinated individuals in the USA (56% of the total population), could reduce the reproductive number Rt by 22% from 1.26 to 0.98 and stop a surge (Figure 2, red line), assuming current levels of vaccination coverage (56%), estimated immunity from previous infection (56.4%), and behavior consistent with the summer Delta surge (R0=3.7) (see Methods for further details).

Unfortunately, in places where vaccination is slightly higher (60%), but previous infection is much lower, (0.5%; e.g. New Zealand), boosting with a third dose would be unable to prevent a surge with the same contact rates (Figure 2, grey line). Conversely, in populations where vaccination is higher (75%) and previously infection is lower (28.2%) (e.g. California), boosting at least 45% of the population (60% of those vaccinated) could push Rt below 1 (Figure 2 blue line).
If contact rates return to pre-pandemic levels (R0=7), with mid-October USA vaccine coverage (56%) and infection history (56.4%), then boosting could reduce Rt by a larger absolute amount (but the same relative amount, 21%) than with lower contact rates, from 2.37 to 1.85 (Figure 2, green line) but cases would still rise rapidly because 1.85 is still far above 1. Using the same number of 3rd doses to doubly vaccinate unvaccinated individuals would be more impactful, and could reduce Rt to 1.49 (Figure 2, compare right end of green line to black point labelled 84% vaccinated on left side). With contact rates return at pre-pandemic levels (R0=7), then even if a population had 100% vaccination coverage and 56.4% previously infected, waning of vaccine and infection-derived immunity would cause cases to continue to grow without boosting (Figure 2, left end of yellow line: Rt=1.17 which is great than 1; without waning Rt would be 0.74, well below 1). However, boosting >21% of a fully (100%) vaccinated population could prevent a surge in cases even with pre-pandemic behavior (Figure 1, yellow line).
Discussion
Vaccines have greatly reduced the impact of COVID-19 globally, but waning immunity and the emergence of the Delta variant have led to surges in cases despite high vaccination coverage in many populations [1, 6-9]. This has led to many countries recommending third doses to boost immunity to protect at-risk individuals [13]. However, the impact of third doses on transmission of SARS-CoV-2 has received far less attention [14].
We found that a third dose could substantially reduce transmission, especially in highly vaccinated populations and the effect was larger in populations with lower acquired immunity from infection and when contact rates (which scale R0) were higher. We showed that neutralizing antibodies are strongly correlated not just with protection against symptomatic disease [3, 17], but also with protection against all infection and transmission given infection. This allowed us to estimate the effect of waning and boosting on transmission, and the pathogen reproductive number Rt. Boosting immunity by providing a third dose to individuals vaccinated more than three months ago (when most waning occurs: Figure S1, S2) could reduce transmission substantially and could prevent a winter surge in many populations where vaccination coverage is high, as long as contact rates and behavior don’t fully return to pre-pandemic levels. In contrast, with pre-pandemic contact rates, only very high levels of vaccine coverage, and a combination of a moderate level of previous infection and boosting could prevent a surge.
We also show that despite the substantial potential impact of boosting on transmission, deploying vaccine doses to unvaccinated individuals has a larger effect on transmission (Figure 2, black circle versus the right end of the green line). In addition, the direct effect of vaccinating unvaccinated people is much larger than the benefit of providing a third dose for severe disease and death since protection against severe disease has barely waned except in older or at-risk individuals [10]. Unfortunately, vaccine hesitancy among those not vaccinated is quite high in many populations (e.g., USA, Russia, etc.) and many people are unwilling to get vaccinated despite strong incentives, often due to misinformation [28-30], making it difficult to increase vaccine coverage in some populations. In contrast, there other populations where vaccine coverage is very low, primarily due to poor availability, especially in Africa [31]. Clearly, limited vaccine doses would be most effectively used in these populations and should be deployed there until supplies are no longer limiting.
Our study has several limitations. First and foremost is the reliance on neutralizing antibody titers as a predictor of protection against infection and transmission. Although the analyses here, and elsewhere suggest a strong relationship between neutralizing antibody titers and protection at the population level [3, 17] and individual level [32], other parts of the immune system, such as T-cells, also play key roles in protection from infection and disease. Second, our analyses use population averages for estimates of protection against infection and transmission and ignore age-specific variation among individuals (as well as other factors). Third, the data available to estimate vaccine protection against all infections was very limited and we are unaware of any studies that have estimated the full impact of vaccination against transmission given infection from the Delta variant. Finally, we assume well-mixed populations in calculating reductions in the reproductive number Rt. Clearly a targeted vaccination approach would be more effective than that outlined here if individuals that were highly connected to at-risk individuals could be targeted for third doses [33]. Finally, we focused on third dose boosters using the Pfizer vaccine, but third doses for other vaccines, including heterologous boosting [34], have also recently been approved in the USA and elsewhere.
In summary, many countries have already begun to deploy third doses to protect at-risk individuals, and some countries (e.g. Israel, [16]) have even deployed third doses to the general population to reduce transmission. However, uptake in most countries has been low, criteria for third doses are still vague [13], and only moderate effort has been deployed to deploy third doses widely. Our results suggest that widespread boosting of the general population could substantially reduce transmission. Polls in some countries suggest a large fraction of the population would be willing to get a third dose (e.g., 76% of Americans; [35]). If vaccine supplies can be increased to provide initial doses to populations with very low coverage, then offering third doses to the general public could play a significant role in reducing transmission. This would directly protect boosted individuals, indirectly protect unvaccinated and vaccinated individuals, and reduce the possibilities for viral evolution [15].
Data Availability
All data produced in the present work are contained in the manuscript
Contributors
AMK conceived the study. BJG and AMK performed the analyses and wrote the paper.
Declaration of interests
All authors declare no competing interests.
Data sharing
Code and data files to replicate the figures and analyses of this paper can be found at: https://github.com/marmkilpatrick/Vaccine-boosters
Supplemental Tables and Figures




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgements
We thank the Kilpatrick lab for helpful comments.
References




