
Abstract
Background The COVID-19 pandemic is now dominated by variant lineages; the resulting impact on disease severity remains unclear. Using a retrospective cohort study, we assessed the risk of hospitalization following infection with nine variants of concern or interest (VOC/VOI).
Methods Our study includes individuals with positive SARS-CoV-2 RT-PCR in the Washington Disease Reporting System and with available viral genome data, from December 1, 2020 to July 30, 2021. The main analysis was restricted to cases with specimens collected through sentinel surveillance. Using a Cox proportional hazards model with mixed effects, we estimated hazard ratios (HR) for the risk of hospitalization following infection with a VOC/VOI, adjusting for age, sex, and vaccination status.
Findings Of the 27,814 cases, 23,170 (83.3%) were sequenced through sentinel surveillance, of which 726 (3.1%) were hospitalized due to COVID-19. Higher hospitalization risk was found for infections with Gamma (HR 3.17, 95% CI 2.15-4.67), Beta (HR: 2.97, 95% CI 1.65–5.35), Delta (HR: 2.30, 95% CI 1.69-3.15), and Alpha (HR 1.59, 95% CI 1.26–1.99) compared to infections with an ancestral lineage. Following VOC infection, unvaccinated patients show a similar higher hospitalization risk, while vaccinated patients show no significant difference in risk, both when compared to unvaccinated, ancestral lineage cases.
Interpretation Infection with a VOC results in a higher hospitalization risk, with an active vaccination attenuating that risk. Our findings support promoting hospital preparedness, vaccination, and robust genomic surveillance.
Introduction
Following initial detection in December 2019 in Wuhan, China, SARS-CoV-2 disseminated rapidly worldwide, with the first reported COVID-19 case in the United States detected in Washington State (WA) on January 19, 2020 (1). During the third quarter of 2020, distinct phenotypic changes on the SARS-CoV-2 spike protein were identified, raising concerns about increased transmission, immune evasion, or greater disease severity (2). The first detections of these variants of concern (VOCs) in WA occurred on January 23, 2021, when the first two cases of lineage B.1.1.7 (now referred to as Alpha) were found in Snohomish County (3).
Since the initial detection of the first cases of the Alpha variant, multiple VOCs and variants of interest (VOIs) have been reported in WA. In March 2021, the Washington State Department of Health (WA DOH) partnered with multiple laboratories to establish a sentinel surveillance program to monitor the genomic epidemiology of SARS-CoV-2 (4). Given the replacement of ancestral lineages due to increasingly greater effective reproductive numbers, VOC/VOIs now represent the majority of sequenced cases in WA, with more than 70% of cases sequenced between June 27, 2021 and July 10, 2021 attributed to the Delta variant (4).
The rapid emergence of VOC/VOIs has resulted in numerous studies reporting increased transmissibility and infection rate (5–8). Previous studies have identified an increased risk of hospitalization for both the Alpha and Delta variants in various regions around the world after adjusting for age and other relevant covariates (9–12). However, these studies compared a single variant lineage to an ancestral lineage or to a small aggregated subset of variant lineages, leaving a dearth of knowledge into how risk of severe disease differs among the various lineages.
To address this gap in knowledge regarding healthcare outcomes following infection with a variant lineage, we designed a retrospective cohort study analyzing epidemiologic and genomic data from WA in order to compare the risk of hospitalization among 9 VOC/VOIs.
Methods
Study Design
For this retrospective cohort study, we included cases with SARS-CoV-2 positive RT-PCR results in the Washington Disease Reporting System (WDRS) that contained linking information to corresponding sequences in the GISAID EpiCoV database (13,14) with specimen collection dates between December 1, 2020 and July 30, 2021. Sequence quality was determined using Nextclade version 1.0.0-alpha.8 (https://clades.nextstrain.org/). Lineage was assigned using the Pangolin COVID-19 Lineage Assigner version 3.1.11 (https://pangolin.cog-uk.io/); only cases with an assigned PANGO lineage were included. The primary exposure of interest was VOC/VOI lineage, taken from the WHO assignments (15) with the exception of P.2; VOC/VOI lineages lacking sufficient data were excluded, leaving Alpha, Beta, Gamma, Delta, Kappa, Iota, Epsilon, Eta and Lambda for analysis as well as ancestral or non-VOC/VOI lineages for reference.
Vaccination data was collected from the WA IIS repository that is maintained by the Office of Immunizations at WA DOH. The Data Integration and Quality Assurance (DIQA) team at WA DOH conducts linkage of the IIS COVID-19 vaccine data with the COVID-19 data from WDRS.
Cases without a known age, lineage or vaccine manufacturer, cases with multiple lineages identified for the same infection, and cases where the linked viral sequence had >10% sequencing ambiguity, were excluded from the study. For cases with multiple specimens sequenced of the same lineage, only the first sequenced specimen was used for analysis. The main analysis was limited to cases with specimens sequenced as part of sentinel surveillance.
Sentinel Surveillance
As part of an initiative to monitor the genomic epidemiology of SARS-CoV-2, WA DOH established a sentinel surveillance program with partner laboratories around the state. Designated sentinel labs include Atlas Genomics, Confluence Health/Central Washington Hospitals, Interpath Laboratories, Incyte Diagnostics Spokane, Northwest Laboratories, and University of Washington Virology. Laboratories and the percentage of randomly selected positive specimens they submit for sequencing were designated to optimize representation across the state. PCR positive samples that are most likely to be successfully sequenced are those with low cycle threshold (Ct) value, resulting in only samples with a Ct of 30 or less being selected for sequencing. This local surveillance program was supplemented by a national surveillance effort supported by the Centers for Disease Control and Prevention which included multiple commercial diagnostic laboratories sequencing randomly selected specimens (16). In addition to these designated sentinel laboratories, specimens were classified as sentinel surveillance if the sequencing laboratory indicated that they were conducting sequencing on randomly selected specimens. Specimens selected for sequencing as part of outbreak investigations, targeted due to travel history, targeted due to known vaccine breakthrough status, or targeted as part of investigations of S-gene target failures were not considered sentinel surveillance.
Hospitalizations
The primary outcome of interest was COVID-19 hospitalization; the WA DOH defines a “COVID-19 hospitalization” as a WA resident with confirmed or probable COVID-19 who is identified as being hospitalized through self-report of hospitalization, hospital records review, or linkage with a syndromic surveillance hospitalization record (RHINO). Cases known to be hospitalized for a condition other than COVID-19 (e.g. labor and delivery) were excluded as “COVID-19 hospitalization.” For this study, we only included cases where a positive viral collection date was within 14 days of hospitalization in order to prevent misclassification of hospitalizations not attributable to COVID-19. Cases with a record of hospitalization but without an admission date were excluded from the study. Individuals who first tested positive after their hospital discharge were also excluded to avoid including non-COVID associated hospitalizations.
Covariates
We identified a priori confounders that were suspected to be associated with both risk of hospitalization following a COVID-19 infection and the epidemiological risk of acquiring a VOC/VOI. These included age at sampling (categorized into 10-year increments), sex assigned at birth, and vaccination status. Calendar period (defined as the week of the year of the collection date) was later included in a supplementary sensitivity analysis. Vaccination status was made into a two tier variable of 1) “Unvaccinated to <21 days post dose one”, 2) “ ≥21 days post dose one, with or without a second dose’’ due to the fact that only a low number of hospitalized cases had a record of vaccination. The decision to consider active vaccination only after 21 days comes from CDC (Center for Disease Control and Prevention) guidance regarding active protection from symptomatic infection only after 14 days (17) and then allowing for an additional 7 days to allow for the development of protection from hospitalization, given that the mean time from symptom onset to hospitalization has been found to be about 7 days (18). Our vaccination covariate includes cases with a history of vaccination with BNT162b2 (Pfizer–BioNTech vaccine), mRNA-1273 (Moderna), and Ad26.COV2 (Johnson & Johnson). Cases with mixed brand dosage or a history of a third vaccination were excluded from the study. Additionally, cases with a repeat positive test (defined as a case where the specimen collection date was more than 21 days before or after the first positive test date) were also excluded from the study to prevent confounding from previous immunity.
Statistical Analysis
We used descriptive statistics to explore characteristics of those included in our sample stratified by SARS-CoV-2 lineage. For all descriptive analyses, we summarized categorical variables as frequencies and percentages.
We estimated the associations between SARS-CoV-2 VOI/VOCs and the risk of COVID-19 hospitalization by calculating hazard ratios (HRs) for the time to hospital admission through a Cox proportional hazard model with mixed effects using non-VOC/VOI ancestral lineages as the reference group. We adjusted the HRs for the covariates of age, sex assigned at birth, and vaccination status. Sex and vaccination status were added as random effects to regularize adjustments for under-represented categories.
In a secondary analysis to analyze how vaccination affected the risk hospitalization by variant lineage, an interaction term of vaccination*lineage was introduced into the model and reran for those variants found to have the largest sample size and effect magnitude: Alpha (B.1.1.7), Gamma (P.1), Delta (B.1.617.2). Stratified risk of hospitalization by vaccination status was conditioned on the “Unvaccinated to <21 days post dose one” or no active vaccination group for cases infected with an ancestral lineage. An aggregated analysis looking into the effect of vaccination on hospitalization regardless of lineage was subsequently conducted due to sample size limitations following stratification by lineage.
In order to account for differences in both model selection and case inclusion, sensitivity analyses were performed using a Cox proportional hazard model with fixed effects and a Poisson regression model for both the subsetted sentinel surveillance-only dataset as well as for the entire case dataset found in WDRS for the same study period. An additional sensitivity analysis was also conducted to assess the effect of time period on our estimates by repeating the main analysis with the additional covariate of calendar week. Statistical analyses were performed using R version 3.6.2 (R Project for Statistical Computing).
Results
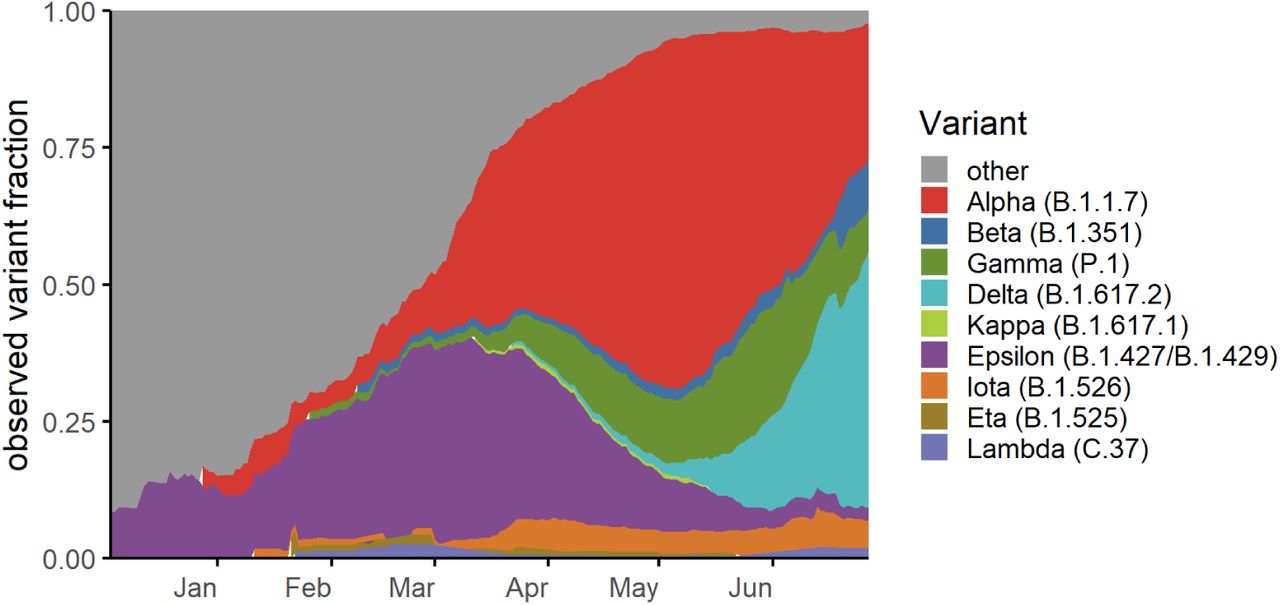
The COVID-19 epidemic in WA shows a distinct trend in the lineage distribution over time (Fig. 1). Early on, the epidemic was predominantly characterized by non-VOI/VOC lineages, while by March 2021, VOC/VOI lineages gained predominance over ancestral lineages.

Variant fraction is calculated from a 21-day rolling average from our full sequenced dataset spanning from December 1, 2020 to June 30, 2021 and normalized to 100% to better observe changes in proportion of infections from variant lineages compared to total infections.
In this study, we included 27,814 cases with viral genome data available on WDRS, with specimens collected from December 1, 2020 to July 30, 2021 (Supp. Fig 1). Of these, the final study population for the main analysis was restricted to 23,170 (83.3%) cases that were selected for sequencing as part of random, sentinel surveillance.
Table 1 represents the general characteristics of the study population. The number of cases infected with a VOC includes 8,907 (38.4%) infected with Alpha (lineage B.1.1.7), 233 (1.0%) with Beta (lineage B.1.351), 2,046 (8.8%) with Gamma (lineage P.1), and 2,026 (8.7%) with Delta (B.1.617.2). Cases infected with a VOI other than Epsilon (lineages B.1.427 and B.1.429) at 3,700 (16.0%) comprise a smaller proportion of the study population (3.3%). 5,474 (23.6%) individuals were infected with an ancestral lineage other than a variant of concern or interest as defined herein.
90.7% of our study population was under the age of 60 and 49.5% male and the majority of the study sample was unvaccinated (94.0%) at time of analysis. Of the 23,170 cases in the main analytic sample, 726 (3.1%) cases were hospitalized. 247 of the cases were hospitalized following an infection with Alpha, 12 cases with Beta, 127 with Gamma, and 74 with Delta.
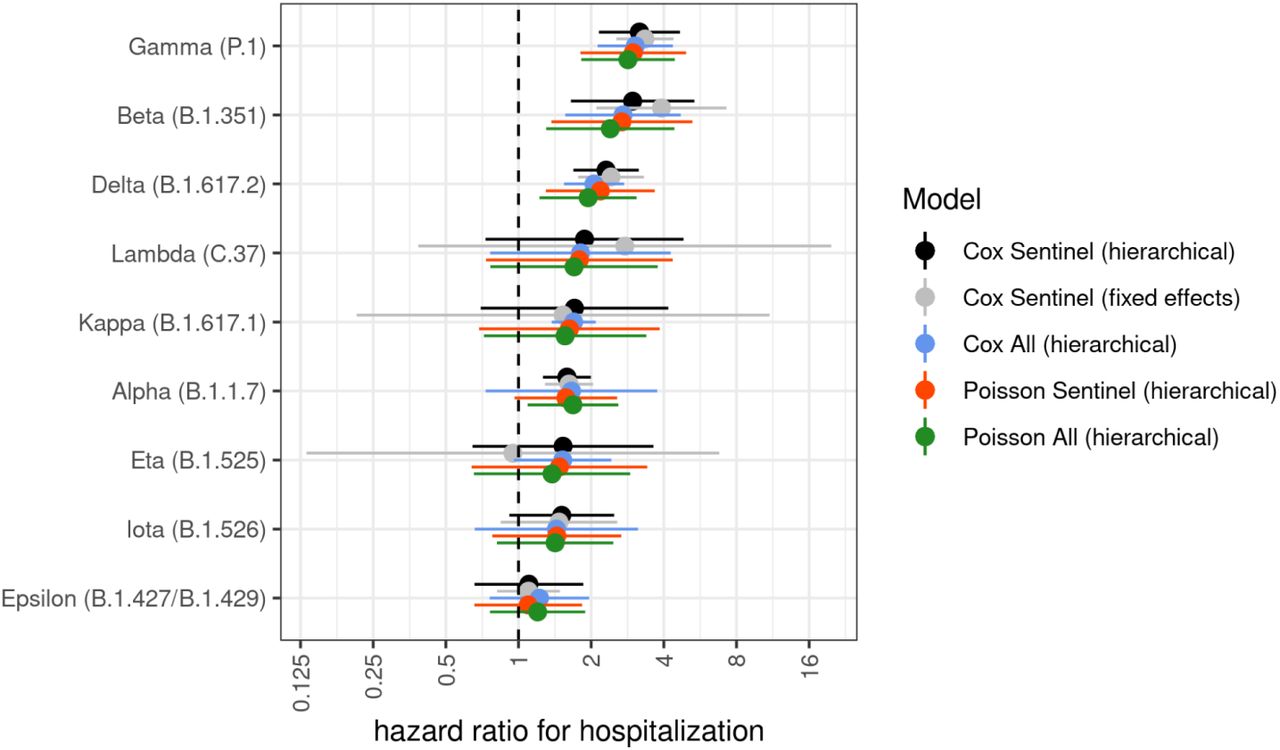
In the adjusted model, we found that cases infected with any VOC have a higher risk of hospitalization when compared to those cases without a classified VOI/VOC (Fig. 2). The highest risk of hospitalization were found in cases infected with the Gamma variant (HR 3.17, 95% CI 2.15-4.67) and in cases infected with the Beta variant (HR 2.97, 95% CI 1.65-5.35). Cases with infection with Delta (HR: 2.30, 95% CI 1.69-3.15) and Alpha (HR 1.59, 95% CI 1.26–1.99) also showed a higher risk of hospitalization when compared to those cases not infected with a VOC/VOI. All other VOC/VOIs failed to show a significant difference in risk of hospitalization. (Table 2)

Risk of hospitalization is compared to individuals infected with an ancestral lineage. Error bars represent 95% CI. Estimates are adjusted for age, sex assigned at birth, and vaccination status.
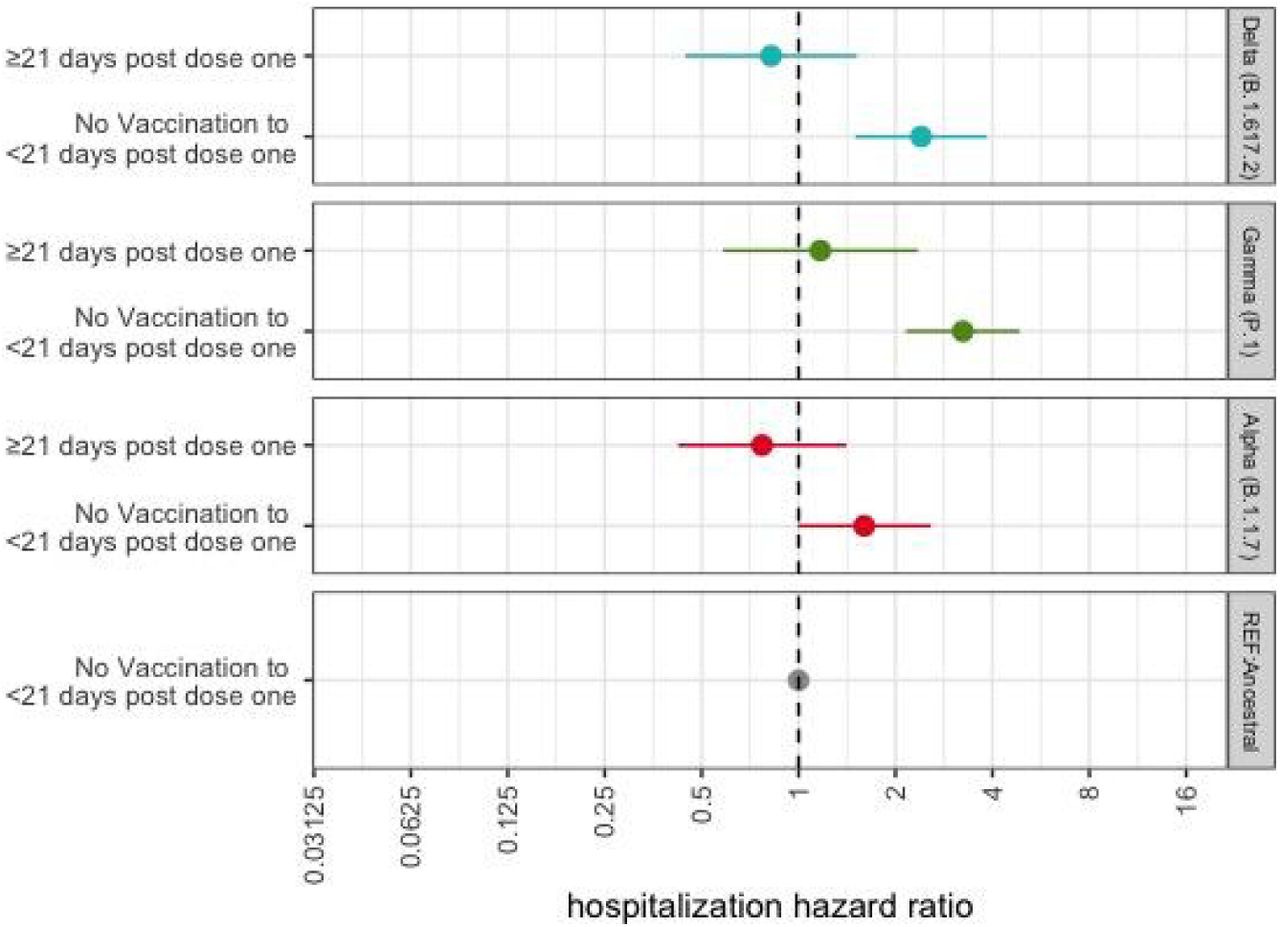
To understand how vaccination status modifies the risk of hospitalization following infection with a VOC, the interaction term of lineage*vaccination was added to the model. The association between variant lineage and risk of hospitalization stratified by vaccination status is shown in Figure 3 with unvaccinated individuals (unvaccinated or <21 days post dose one) infected with ancestral lineages as the reference category. When compared to the reference group, our model shows a higher risk of hospitalization for those unvaccinated individuals infected with Gamma (HR: 3.24, 95% CI 2.16–4.86), Delta (HR 2.40, 95% CI 1.50–3.85), and Alpha (HR 1.60, 95% CI 0.99–2.58) (Table 3). In the strata of cases with an active vaccination, no significant difference was observed in the risk of hospital admittance following infection with Gamma, Delta, or Alpha, when compared to those unvaccinated patients infected with an ancestral lineage. However, the small sample sizes limit the interpretation of these findings (Supp. Table 1). Given the reduction in sample size following stratification by lineage, we repeated the analysis to look into the association between vaccination and the risk of hospitalization following infection with SARS-CoV-2 irrespective of lineage (Table 2). We find that when compared to the unvaccinated group, cases with a record of an active vaccination have a lower risk of hospitalization (≥21 days post dose one: HR 0.34, 95%CI 0.23–0.50).

Unvaccinated individuals infected with ancestral lineages serve as the reference category for each VOC HR. Error bars represent 95% CI. Estimates are adjusted for age and sex assigned at birth.
Estimates of the HR of the risk of hospitalization for cases infected with VOC/VOIs robust to both model selection and inclusion of all sequences in our original database (Supp. Fig. 2-3).
Discussion
In this study, we use SARS-CoV-2 cases in Washington state that were sequenced as part of sentinel surveillance to evaluate the differential risk of hospitalization following infection with a variant lineage. We find that in our study period, cases infected with Alpha, Beta, Gamma, and Delta variants have a higher risk of hospitalization compared to cases infected with an ancestral lineage, after adjusting for relevant covariates. We find similar estimates of higher risk of hospital admittance in the subset of unvaccinated individuals infected with Gamma, Delta, and Alpha when compared to unvaccinated individuals infected with ancestral lineages. We subsequently see no significant difference in hospitalization risk in cases with an active vaccination following infection with the aforementioned VOCs when compared to unvaccinated individuals with ancestral lineages.
Our findings are consistent with other studies from around the world that have examined the risk of hospitalization following infection with a VOC/VOI (11). Our estimates of hospitalization risk following infection with the Delta variant (HR: 2.30, 95% CI: 1.69-3.15) are similar, and with overlapping confidence intervals, to the estimates derived from a cohort in Scotland (HR 1.85 95% CI 1.39–2.47)(12) and also to those presented by the Public Health England in early June 2021 (HR 2.61, 95% CI 1.56–4.36) (19). The estimates from Scotland compared the risk of hospitalization from an infection with Delta to Alpha, the previously dominant lineage at the time, while our study used ancestral lineages as the reference group, which potentially accounts for our higher risk estimates.
We present estimates of the risk of hospitalization following SARS-CoV-2 infection with a diverse group of VOI/VOCs, reflecting the SARS-CoV-2 genomic diversity in Washington state. While a previous study in Singapore examined the risk of severe disease among Alpha, Beta, and Delta variants (9), in addition to these three variants, we provide estimates of risk for six additional variant lineages: Gamma, Lambda, Kappa, Iota, Eta, and Epsilon. Our estimates show that Gamma has one of the highest risks of hospitalization when compared to ancestral infections which concurs with results from two other recent studies that used different designs and populations (20, 21). One recent study showed an increased mortality due to Gamma infection in Brazil across age groups and a study from seven European Union countries showed an increased risk of hospitalization following infection with Gamma, although given that their analysis was restricted to the first three months of 2021, the study was limited in sample size. We also estimate the risk of hospital admittance following infection by Epsilon and Iota but did not find any significant difference in risk. Additionally, we estimated the hospitalization risk following infection with Lambda, Kappa, and Eta variants but failed to detect any trends in these groups potentially due to our small sample sizes and the relatively few numbers of hospitalization events among these lineages. The biological mechanisms behind increased severity in variant lineages remain unclear and require further investigation.
We also sought to evaluate the hospitalization risk following infection by Alpha, Gamma, and Delta stratified by vaccination status. We saw a higher risk of hospitalization for unvaccinated individuals (no record of vaccination to <21 days post first dose) following infection with Gamma, Delta, and Alpha when compared to those unvaccinated individuals infected with an ancestral lineage. When compared to ancestral lineage cases without a record of active vaccination, the subset of cases with an active vaccination record infected with the same aforementioned VOCs showed no significant difference in risk of hospitalization. Vaccinated individuals infected with any of the three VOCs all showed estimates of hospitalization risk with overlapping confidence intervals (Gamma: HR 1.17, 95% CI 0.58-2.35; Delta: HR 0.82, 95% CI 0.44-1.52; Alpha: HR 0.77, 95% CI 0.42-1.41). The similar, overlapping estimates of risk in vaccinated individuals following infection with a VOC is supported by studies in both the United Kingdom and Denmark showing no significant difference in hospitalization risk for vaccinated individuals infected with Delta when compared to those infected with Alpha, suggesting that vaccination exerts a similar effect across VOCs (11,22). Our sample sizes in each strata, however, are small (Supp. Table 1) limiting our ability to make conclusions. Our study is also susceptible to sampling bias, potentially distorting the magnitude of our results. Specifically, cases were selected into our study based on test positivity; if vaccinated individuals are less likely to seek testing and severe illness leads to increased testing, conditioning study enrollment on testing can lead to collider stratification bias, or a distorted association between vaccination and disease severity (23). Prior to July 27, 2021, the official CDC guidance stated that fully vaccinated individuals without symptoms did not need to get laboratory tested for SARS-CoV-2 following an exposure, meaning that the cases in our sample with a record of vaccination, which are conditional on being tested, are almost certainly biased towards a subset of the population with a more severe clinical presentation than the population at large, which potentially attenuates the estimated association between vaccination and risk of hospitalization.
Given our sample size limitations, we then analyzed the association between vaccination and risk of hospitalization after adjusting with relevant covariates but without stratification by lineage. Due to the observational nature of our study, our vaccination findings are subject to collider stratification bias, making the magnitude of effects difficult to interpret, although we expect the bias to work in a conservative fashion, resulting in underestimates of vaccine protection on hospitalization risk. We find that cases with an active vaccination (≥21 days post dose one) have a lower risk of hospitalization when compared to those without a history of vaccination, which are consistent with estimates from Public Health Scotland (HR 0.34, 95% CI 0.23–0.50, vs. HR 0.32, 95% CI 0.22–0.46, respectively).
In order to increase the power of our analysis, we aggregate cases with a Pfizer–BioNTech or Moderna, or Johnson & Johnson vaccination into a singular vaccination category. While studies have shown similar findings for the two mRNA vaccines in regards to efficacy against ancestral lineages (25,26), a study from Qatar showed differences in effectiveness between the two vaccines against infection with the Alpha and Beta lineages (27), potentially impacting the generalizability of our aggregated findings. Further studies more adequately powered to analyze the difference between vaccine formulations are urgently needed.
Previous studies that examine differences in risk of hospitalization following infection with a VOC/VOI frequently include time period, often as calendar week, as an a priori confounder to account for unmeasured changes in health system performance, care-seeking behavior, laboratory practice, etc. For our study, we chose not to include this covariate in the primary analysis because including it creates an identifiability problem: unmeasured confounding trends are not separately identifiable from the trend of increasing severity attributable to increasing VOC/VOI frequency. As shown in Supplementary Figure 4, including time as a covariate uniformly attenuates the variant-specific effects on hospitalization risk associated with VOC/VOI but has no influence on the risk by vaccination. When included in the model, the temporal trend is capturing the linear aspect of the average increase in severity associated with all VOC/VOI as a class, and thus leads to underestimates of the effect of VOC/VOI in isolation. The issue that temporal trends can be mediated by the sweep of VOC/VOI as a class in principle affects any analysis of this type, but the effect should be smaller in studies comparing among VOC/VOI (like Delta relative to Alpha) than in studies comparing VOC/VOI to ancestral lineages.
Although our findings are consistent with previous studies, they are not without limitations. While we only included samples from sentinel surveillance in our primary analysis to account for changing sequencing criteria, VOC/VOI classification is conditional on whole genome sequencing and a Ct threshold <30, meaning that our sequenced cohort may have been different from the general population of cases infected with SARS-CoV-2 in Washington. Recent investigations from WA DOH found that 9.6% of vaccine breakthrough cases identified do not have updated vaccination data in the IIS dataset, mainly due to federal vaccination efforts that are not recorded in IIS (e.g., military, tribal, and commercial pharmacy vaccinations). This means that a portion of cases with an active vaccination may be misclassified as unvaccinated in our study. This misclassification would bias the vaccination results towards the null, potentially resulting in underestimation of the effect of vaccination on risk of hospitalization. The severity bias in our cases with a record of vaccination would also result in underestimation of the protective association between increasing vaccination and lower hospitalization risk. This bias combined with higher testing among hospitalized cases leads to collider stratification bias due to study selection based on testing, severely limiting the interpretation of our vaccination findings. The study is observational in nature, meaning that despite adjusting for potential confounders, there might be other confounders such as regional criteria for hospitalization that might affect the risk of hospitalization.
In conclusion, our retrospective cohort study found a higher risk of hospitalization in cases infected with a SARS-CoV-2 VOC. As the SARS-CoV-2 pandemic continues to be dominated by variant lineages, our study supports the need for hospital preparedness in areas with uncontrolled spread of the virus as well as provides an impetus for promoting uptake in effective vaccination. This study also highlights the importance of ongoing genomic surveillance at the state and federal level to monitor variant outcomes. Coordinating data integration between viral sequence data and epidemiologic data requires close collaboration between sequencing laboratories (academic, commercial, and public health) and health departments. Washington state has invested in staff in multiple areas to be able to create the data integrations needed to complete this analysis, including staff in laboratory science, bioinformatics, molecular epidemiology, and data science. Building a robust public health workforce as well as strong collaborations between public health and academia is critical to using genomic epidemiology to answer crucial questions about emerging SARS-CoV-2 variants.
Data Availability
Requests to access these data are handled by the Washington Department of Health
Funding
T.B. is a Pew Biomedical Scholar and is supported by NIH grant no. R35 GM119774, P.R. is supported by a CFAR New Investigator Award (NIH AI027757). The Seattle Flu Study is run through the Brotman Baty Institute for Precision Medicine and funded by Gates Ventures, the private office of Bill Gates. This work was supported by CDC BAA contract 75D30121C10982. Employees of the Institute for Disease Modeling (MF, RB) received no specific funding for the project. Computational analyses for UW Virology data were supported by Fred Hutch Scientific Computing (NIH ORIP grant S10OD028685).
Author Contributions
Conceived and designed the study: MF, HO, KA, MP, SL, IP, TB, LF
Collected or curated the data: KA, LF, SL, PR, HX, SMB, RP, ML, SE, SS, PM, ALG, LS, CF, ER, WZZ, LG, MT, JL, DN, DB, MH, EG, TN, JDR, JLR, JS, ET, GM, PD, DM, HG, AS, JMP, DR, LMT
Conducted the analysis: MF, MP, SL
Advised on the analysis: RB, IP, TB, KA, HO
Drafted the manuscript: MP, SL
Reviewed and edited the manuscript: All authors
Declaration of interests
ALG reports central testing lab from Abbott and research funding from Merck and Gilead. All other authors declare no competing interests.
Ethics Approval
The Washington State Institutional Review Board designated this study as exempt. Sequencing and analysis of samples from the Seattle Flu Study was approved by the Institutional Review Board (IRB) at the University of Washington (protocol STUDY00006181). Sequencing of remnant clinical specimens at UW Virology Lab was approved by the University of Washington Institutional Review Board (protocol STUDY00000408).
Supplementary Material

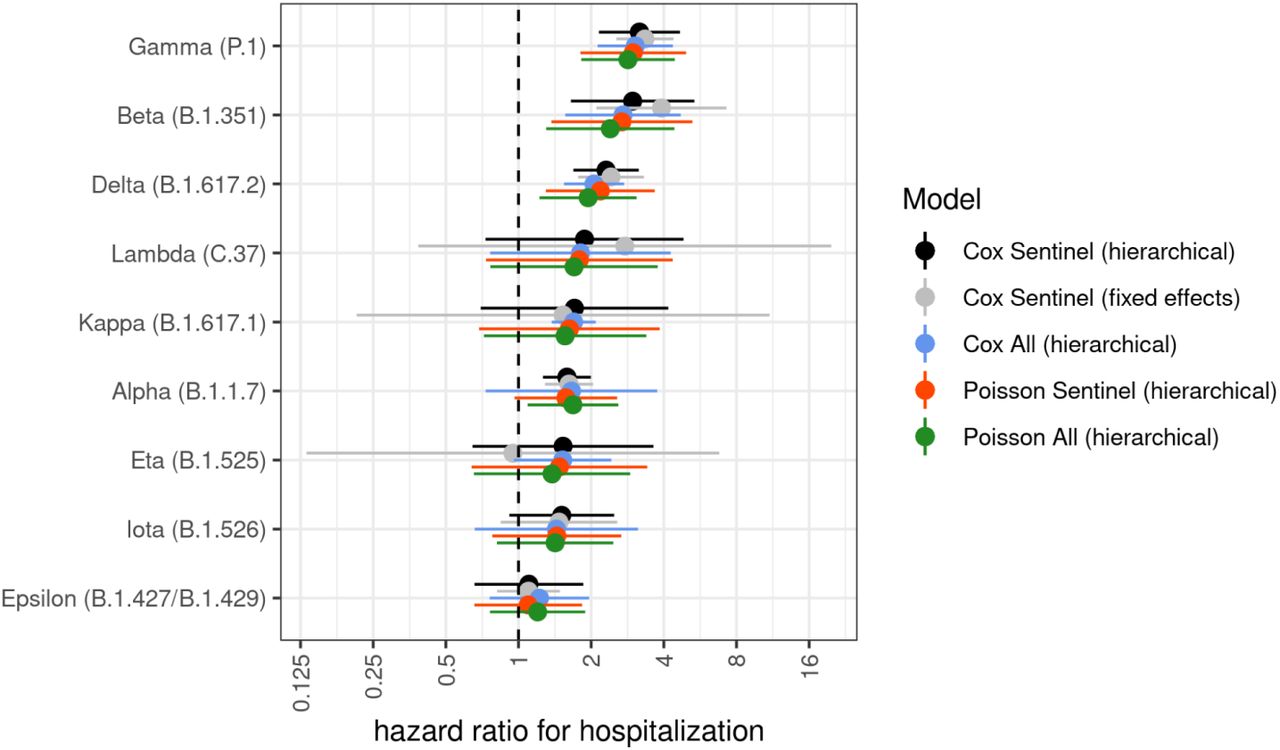
Error bars represent 95% CI. “Hierarchical” refers to a model with mixed effects and “Sentinel” refers to the sample restricted to only to cases collected through sentinel surveillance. “Fixed effects” describes all model covariates being treated as fixed effects and “All” refers to the entire dataset from Dec 1, 2020 to Jul 30, 2021, irrespective of participation in sentinel surveillance.
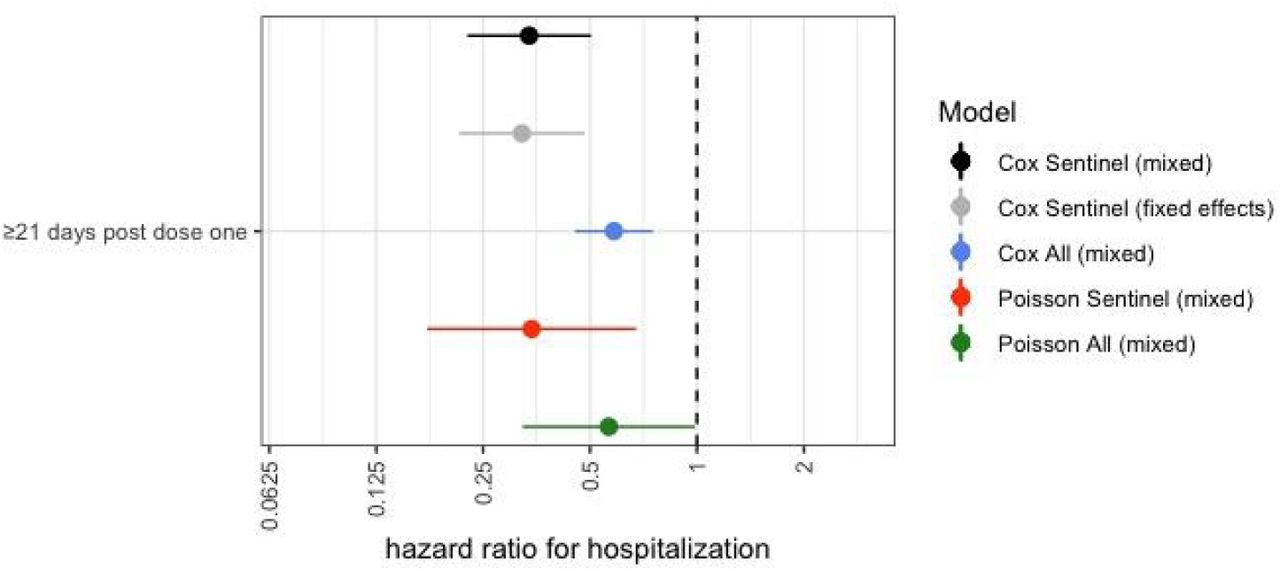
Error bars represent 95% CI. “Mixed” refers to a model with mixed effects and “Sentinel” refers to the sample restricted to only to cases collected through sentinel surveillance. “Fixed effects” describes all model covariates being treated as fixed effects and “All” refers to the entire dataset from Dec 1, 2020 to Jul 30, 2021, irrespective of participation in sentinel surveillance and includes targeted sequencing of suspected breakthrough infections.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
In order to harmonize with previous studies on hospitalization, we reran our main analyses with all the original a priori covariates and the additional covariate of calendar period (defined as week of the year). We see a lower effect magnitude of hospitalization risk by variant but show no difference in risk of hospitalization by vaccination, when compared to the original analysis. The effect of time alone is causally mediated by the VOC/VOI. When time alone is included, we estimate an increasing adjusted hazard ratio per week of 0.04 (SE=4e-05), and inclusion of VOC/VOI reduces the estimated effect by roughly 50% in coefficient to 0.02 (SE=7.5e-5) and roughly 80% in z-score. Furthermore, the residual effect of time in the VOC/VOI and time model is entirely explained by VOC/VOI only in the primary model. The coefficient of 0.02 per week corresponds to an average effect of about 0.35 on the overall hazard at week 20--the average collection week included in the primary analysis--which similarly matches the shift in the VOC/VOI estimates.
Acknowledgments
Clinical and sentinel laboratories who forwarded specimens for sequencing, and sequencing laboratories that reported data to WA DOH. The WADOH Data Science Support Unit for integrating sequencing data with epidemiologic case data. The WADOH IIS team and DIQA teams for maintaining and linking vaccination data. The WADOH surveillance team for case and hospitalization data. Natasha Close and the WA DOH RHINO team for hospitalization data. James S. Miller (Epidemic Intelligence Service Officer, Centers for Disease Control and Prevention) for manuscript review and insightful feedback. The team at Altius Institute for Biomedical Sciences: Rebecca L. Bruders, Amanda C. Gale, Clementine B.M Green, Suman Grewal, Muhammad H. Halimun, Kneshay N. Harper, Jessica M. Halow, William A. Isner, Audra K. Johnson, Jessica N. Kunder, Lauren E. Mitchell, Jemma S. Nelson, Alex S. Nguyen, Sofia E. Olsson, Sadie L. Patraw, Tobias F.C. Ragoczy, Ashly M. Senske, Julia Wald.




