
ABSTRACT
Objective The COVID-19 pandemic has seen a rapid adoption of telehealth consultations, potentially creating new barriers to healthcare access for racial/ethnic minorities. This systematic review explored the use of telehealth consultations for people from racial/ethnic minority populations in relation to health outcomes, access to care, implementation facilitators and barriers, and satisfaction with care.
Materials and Methods This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis and the JBI Manual for Evidence Synthesis. Five major databases were searched to identify relevant studies. Screening, full-text review, quality appraisal and data extraction were all completed independently and in duplicate. A convergent integrated approach to data synthesis was applied with findings reported narratively.
Results A total of 28 studies met the inclusion criteria. Telehealth-delivered interventions were mostly effective for the treatment/management of physical and mental health conditions including depression, diabetes and hypertension. In several studies, telehealth improved access to care by providing financial and time benefits to patients. Technological difficulties were the main barriers to effective telehealth consultation, although overall satisfaction with telehealth-delivered care was high.
Discussion Telehealth-delivered care for racial/ethnic minorities offers promise across a range of conditions and outcomes, particularly when delivered in the patient’s preferred language. However, telehealth may be problematic for some due to cost and limited digital and health literacy.
Conclusion The development and implementation of guidelines, policies and practices in relation to telehealth consultations for racial/ethnic minorities should consider the barriers and facilitators identified in this review to ensure existing health disparities are not exacerbated.
BACKGROUND AND SIGNIFICANCE
The global COVID-19 pandemic has seen a rapid adoption of telehealth in lieu of face-to-face consultations due to the need for social distancing and minimization of patient and healthcare provider physical contact.[1–3] As a result, the use of telehealth to deliver healthcare services has become widespread.[4] Implementation of this fast transition has been ad hoc with little evidence to guide such widespread adoption. Consequently, there is a risk that quality of care could be compromised and new access barriers may emerge for underserved groups such as racial and ethnic minorities who already experience health disparities.[5 ,6]
Telehealth consultations, including telemedicine, involve the use of telecommunication technologies between healthcare providers from any healthcare or social care discipline and patients in real time to transmit voice, images and data for healthcare and health education.[7] Using telehealth consultations, healthcare providers can deliver healthcare services and information directly to patients located elsewhere, addressing access problems related to distance and transport, waiting times, cost and limited patient and clinician time.[7–10] Pre-COVID-19, telehealth consultations in Western countries were largely limited to rural and remote patients, psychiatry or niche subspecialties such as cancer genetics.[11–14]
Existing systematic reviews of telehealth consultations have been conducted in a variety of clinical settings with generally positive findings in relation to patient satisfaction outcomes and consultation effectiveness.[15–17] In a review of quantitative studies, healthcare delivered by videoconferencing was effective in assessing patients’ health conditions and improving patients’ health conditions in 98% of the included studies.[18] This review also found that telehealth consultations improved treatment compliance and accountability for some participants.[18] Additionally, telehealth services have been found to improve access to care, and communication and engagement with clinicians from patients’ and informal carers’ perspectives.[16] However, telehealth services were not an effective means of psychosocial support in some studies and poor audio-visual quality limited patients’ satisfaction with healthcare.[16]
Patients and communities from racial/ethnic minorities are at risk of poorer health outcomes than the majority population because of structural inequities, including lack of access to health information in languages other than English, underutilization of interpreter services, lack of culturally appropriate services, and racism and discrimination.[19–23] The use of telehealth consultations may further complicate healthcare access for patients from racial/ethnic minority backgrounds due to their limited health and digital literacy, and their challenges in navigating mainstream healthcare systems.[23 ,24] These access barriers are potentially heightened during the COVID-19 pandemic.[7]
Despite previous reviews of telehealth effectiveness for different patient populations such as older populations and rural and remote communities, no reviews have been undertaken of studies assessing telehealth consultations specifically for patients and communities from racial/ethnic minority backgrounds. An evidence synthesis focused on patients and communities from racial/ethnic minority groups would generate an evidence base for the tailoring of telehealth consultations to their diverse needs.
OBJECTIVE
The objective of this review was to explore the health outcomes, implementation facilitators and barriers, and satisfaction with care, in relation to telehealth consultations for racial/ethnic minority populations in order to make recommendations for practice and future research.
MATERIALS AND METHODS
Information sources and search strategy
The protocol for this systematic review was registered in the international register of systematic reviews PROSPERO (CRD 42020221017) and was conducted in accordance with the PRISMA guidelines.[25] Studies were identified from a search of the following 5 electronic databases: Ovid Medline, Ovid PsycINFO, EMBASE, and CINAHL via EbscoHOST and Scopus platforms. The search was limited to studies published in English between 1 January 2005 and 9 October 2020. Additionally, a search for existing systematic reviews on the same topic was conducted in: all EBM reviews via Ovid, Cochrane Database of Systematic Reviews, Joanna Briggs Institute, and PROSPERO. Reference lists of included studies were hand-searched for relevant studies.
A list of terms was formulated for the concepts: “telehealth” and “racial or ethnic minority”. These terms were mapped to subject headings (e.g., Medical Subject Headings or equivalent) and keywords. Boolean operators were used to group subject headings and keywords to create a search strategy (Supplementary file X).
Eligibility Criteria
To be included in the review the study had to meet the following inclusion criteria:
Sample population included patients from racial/ethnic minorities, their carers or healthcare staff who provided care to racial/ethnic minorities, with study findings disaggregated by racial/ethnic minority groups.
For this review, we describe the intervention as ‘telehealth consultation’. Telehealth consultations occurred instead of a face-to-face consultation to provide a health service such as a clinical assessment or diagnosis and/or management of a health condition (physical or mental). Support services provided as standard practice (e.g., phone interpreting, telemonitoring without direct interaction with a healthcare provider) were excluded. Studies that primarily focussed on delivery of health promotion programs or health-related education via telehealth were also excluded.
Included telehealth consultations in healthcare settings (e.g., hospitals, primary care clinics)
Reported individual health outcomes (e.g., physical health, mental health). Individual level outcomes could be related to patients/health consumers and care-givers.
Reported health service outcomes (e.g., readmission rates, barriers to implementation). Health service level outcomes may be related to access to care, service delivery, satisfaction with care and cost-effectiveness
Used quantitative, qualitative or mixed methods study designs
Published in a peer-reviewed journal
Reviews of telehealth consultations and healthcare for Indigenous peoples have been published.[26–30] We therefore did not include Indigenous peoples in the current review. Publications were excluded if they were opinion pieces, systematic reviews and meta-analyses, conference abstracts or proceedings or duplicate publications using the same sample and reporting the same outcomes.
Data screening and extraction
Search results were exported from the electronic databases into the systematic review management platform Covidence (Veritas Health Innovation, 2021). Screening was undertaken in two phases. Following the removal of duplicates, studies were screened independently in duplicate by two reviewers on title and abstract. Conflicts were resolved by a third reviewer. In the second screening phase, full text articles were screened independently in duplicate by two reviewers and conflicts were resolved by a third reviewer.
Data extraction was performed by two reviewers using Covidence, with differences resolved by a third reviewer. Extracted data comprised the characteristics of each study: country of study, health setting, study aim, study design, sample size and participants’ characteristics (e.g., gender, age, race/ethnicity/cultural background), health conditions, and the details of the telehealth intervention. Data were also extracted pertaining to study findings: health outcomes (e.g., blood pressure, depression symptoms) and health access and delivery outcomes (e.g., satisfaction with care, implementation barriers and facilitators).
Methodological quality assessment of studies
Risk of bias and critical appraisal were conducted independently in duplicate by two reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal tools.[31] The JBI Critical Appraisal Tools assess the methodological quality of studies of various design and the extent to which the risk of bias is addressed by authors. For each criterion assessed as ‘met’ on the appropriate tool, a score of ‘1’ was applied. Where criteria were assessed as ‘not met’ or if it was ‘unclear’ to the reviewer, a score of ‘0’ was applied. The scores were then calculated for each study and converted to a final quality rating of ‘low’, ‘moderate’ or ‘high’. The following JBI Critical Appraisal Tools and scoring parameters were implemented in this review: Checklist for randomized-controlled trials (RCTs) (score out of 10; Low 0-3, Moderate 4-7, High 8-10); the Checklist for quasi-experimental studies (score out of 9; Low 0-3, Moderate 4-6, High 7-9); Checklist for Analytical Cross-Sectional Studies (score out of 8; Low 0-3, Moderate 4-6, High 7-8); the Checklist for Qualitative Research (score out of 10; Low 0-3, Moderate 4-7, High 8-10); the Checklist for Cohort Studies (score out of 11; Low 0-4, Moderate 5-8, High 9-11); and, the Checklist for Case Series Studies (score out of 10; Low 0-3, Moderate 4-7, High 8-10). (See Supplementary file for critical appraisal criteria for each study design.)
For mixed methods studies, we used two questions screening questions and five questions from the ‘mixed methods studies’ section of the Mixed Methods Appraisal Tool version 2018 (MMAT),[32] (score out of 7; Low 0-2, Moderate 3-5, High 6-7) which are related to the rationale for using a mixed methods study design and level of interpretation and integration of the qualitative and quantitative components of the study.[32]
Synthesis of studies
Extracted data were exported from Covidence into a Microsoft Excel spreadsheet for analysis. A convergent integrated approach to data synthesis was taken in accordance with the JBI methodology for mixed methods systematic reviews.[31] Due to the heterogeneity of study methodology, design, sample characteristics, and outcome measures, there was no opportunity to conduct a meta-analysis of quantitative studies nor a meta-synthesis of qualitative studies. A narrative synthesis was thus conducted where both qualitative and quantitative data were tabulated together and categorized according to the four outcomes of interest: health outcomes, health access, implementation barriers and facilitators to telehealth consultations, and satisfaction with care. A comparison between studies reporting on the same outcome was performed, with similar and divergent findings reported. Study characteristics such as country and setting, study methodology and design, sample sizes and participant characteristics, were examined by calculating frequencies and proportions.
RESULTS
Study selection
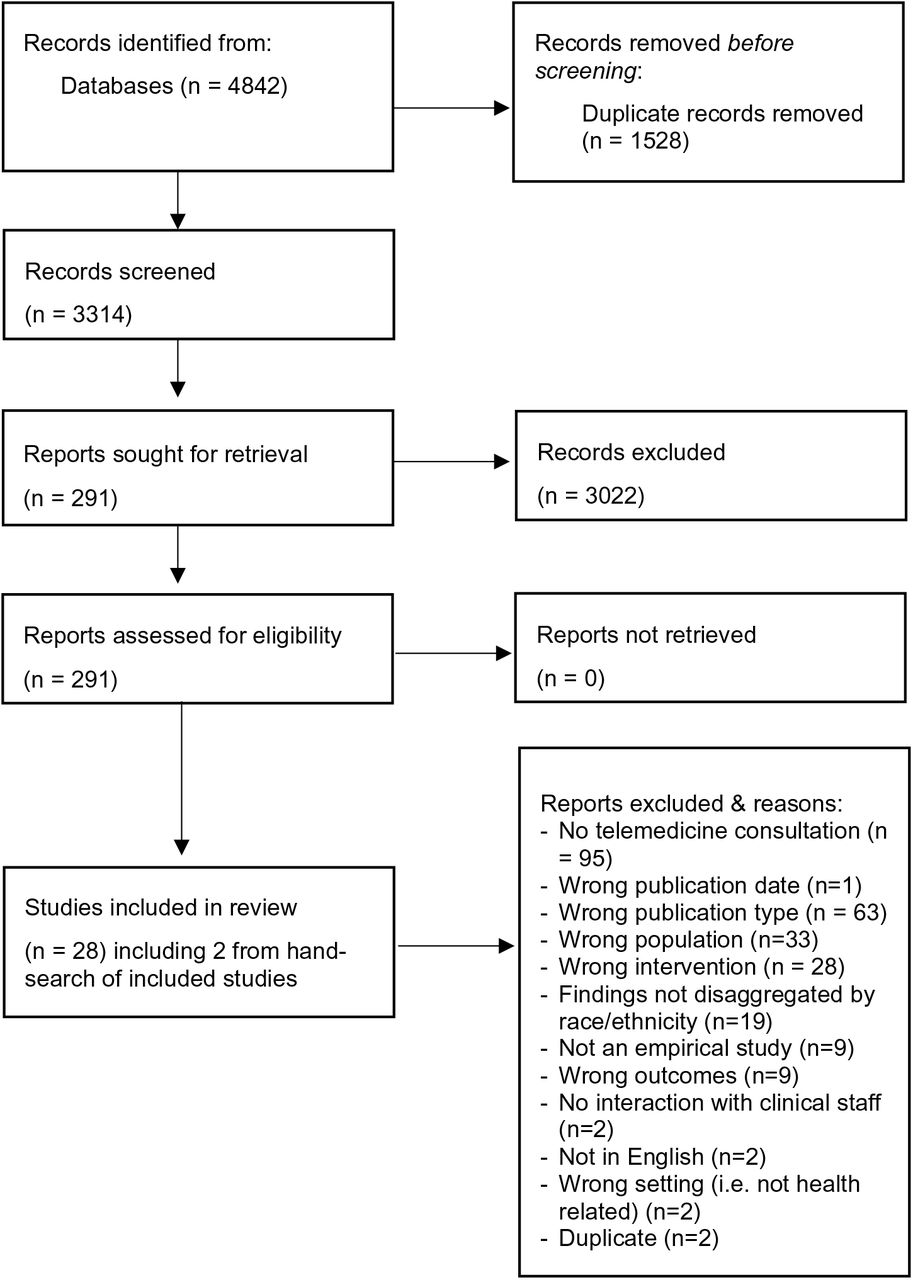
The combined searches from the four databases identified 3,314 unique articles which were screened using the inclusion and exclusion criteria. A total of 28 articles met the inclusion criteria for the systematic review (Figure 1).
{kind=link}
Flow diagram of study selection. Adapted from PRISMA flow-chart [25]
Study characteristics
Studies were published between 2005 and 2019 and comprised 4,301 patients and 12 caregivers from racial/ethnic minorities, and 34 healthcare practitioners. The majority of studies (n=23, 82.1%) examined groups located in the United States and utilized quantitative study designs (n=19, 67.9%). The most common health conditions examined were mental health conditions (n=17, 60.7%), of which nine focused on depression. The most frequent study setting was community health centers (n=8, 28.6%), followed by primary health clinics (n=5, 17.9%), psychiatric or trauma treatment centers (n=4, 14.3%), the community (n=3, 10.7%) and HIV clinics (n=2, 7.1%). The racial/ethnic minority populations included in the studies were predominantly Latino/a or Hispanic (n=13, 46.4%) and African American (n=7, 25.0%). Seven studies included Asian participants from Korean and Chinese communities, three studies included participants from refugee and immigrant backgrounds and one study described their minority population as ‘non-white ethnic group’. Characteristics of included studies are presented in Table 1. (Supplementary file Table 1 presents detailed information related to study characteristics.)
Quality assessment
The quality of the included studies was mixed (see Supplementary file). All 11 RCTs reported random sampling from patients presenting for clinical care. There was variation in the reporting of allocation concealment and differences in baseline characteristics between groups in some RCTs, however most reported completion of follow-up assessments and an intent to treat approach to data analysis. As all RCT studies investigated a telehealth consultation between a practitioner and a patient, blinding of participant and practitioner was not possible. Accordingly, no RCT studies reported blinding of participants to intervention group or blinding of practitioners delivering the intervention to group allocation. The number of quality indicators for RCT studies reported ranged from 3/10 to 7/10. Each of the two quasi-experimental studies employed a pre/post design and there were mixed results regarding study quality. The quality of reporting for the one study utilizing a cohort design and for the one study using a case series design was high. Overall, the quality of reporting for studies using cross-sectional, mixed methods and qualitative designs was low to medium.
Telehealth consultations
Data pertaining to telehealth consultations are presented in Table 2. Across the included studies, telehealth consultations were primarily mental health consultations (n=17, 61%) such as cognitive behavioral therapy (CBT) or psychiatry (telepsychiatry). Physical health consultations were related to chronic disease management (n=9, 32.1%) and clinical monitoring (n=2, 7.1%). Physical health diseases that were managed by telehealth consultations included diabetes (n=2, 7%), hypertension (n=3, 11%) and infectious diseases (n=2, 7%). Telehealth consultations were used to monitor patients’ clinical status in two studies. One study used a telephone triage system and computer-supported decision-making software.[33] The other study monitored patient’s vital signs and other health related information ‘remotely’; and this was then used to inform virtual ‘wellness’ visits by a nurse practitioner who discussed the patient’s medications and recent health data.[34]
The telehealth consultations and interventions were delivered by a range of healthcare professionals including: nurses (n=10, 35.7%),[33–42] physicians (n=13, 46.4%)[33 ,37 ,39 ,40 ,42–51] including psychiatrists, primary care physicians and specialists, allied health professionals (n=9, 32.0%)[46 ,52–59] such as social workers, counsellors and psychologists, and paraprofessional outreach workers in one study.[39] In eighteen studies (64%), the healthcare professionals delivering the telehealth intervention were bilingual. The mode used to deliver the telemedicine intervention was video conferencing in 16 studies (57.1%) and telephone in 11 studies (39.3%); one study used both internet video and telephone communication.[39]
Health outcomes
In total, 14 studies measured health outcomes with evidence of effectiveness of telemedicine on measures of mental health, cardiovascular health and diabetes related outcomes. Three RCTs focused on health outcomes related to treatment of depression. These three studies assessed the effect of a telehealth CBT intervention on depression severity compared with face-to-face CBT[55 ,60] or compared with anti-depressant therapy.[53] Among Latino patients, worry symptoms were reduced[60] and depression symptoms were improved[55] following the use of culturally adapted telephone-based CBT compared to face-to-face CBT. In the study by Dwight-Johnson[53], Latino patients receiving culturally adapted telephone-based CBT showed greater improvement in depression symptoms over 6 months compared to patients who received usual care with anti-depressant medications.
The effects of telepsychiatry consultations or remote management on improving depression outcomes were reported in three RCTs.[43 ,46 ,49>] In a study of Hispanic patients with depression, monthly telepsychiatry consultations and usual care were equally effective in reducing depression scores after 6 months.[43] In another pilot RCT [46], telephone-based depression care management plus usual care was compared with the usual care only group. The findings of this study showed a trend for lower levels of depression in the intervention group over time compared with the control group.[46] In another study, the effectiveness of culturally sensitive telepsychiatry treatment and care management was compared to usual care for Chinese Americans with depression.[49] This study found greater improvement in depressive symptoms following telepsychiatry compared with usual care.[49] In a single group pre-test post-test design with Korean immigrants, weekly sessions of telepsychiatry for four weeks significantly reduced depression scores at immediate follow-up and at three-months follow-up.[56] In a pilot study using a pre-post two group design focusing on African American caregivers of older adults with dementia, telephone-based and face-to-face CBT interventions were equally effective in reducing depression scores.[54]
Three studies assessed the effects of telemedicine on cardiovascular and diabetes health outcomes.[37–39] In one RCT study of patients with hypertension from Korea, bi-weekly and monthly hypertension-related telephone counselling, and 12-month home monitoring of BP were effective in improving long-term BP outcomes[38]. The second study employing a RCT design assessed the effectiveness of a telemedicine intervention emphasizing medication management and home BP monitoring with African American patients living with hypertension [37]. Jackson et al.[37] found significant improvement in mean systolic blood pressure at 12-months and at 18-months following the intervention compared with usual care. A study by Mayes [39] assessed the impact of telemedicine on blood glucose regulation among Hispanic patients living with type 2 diabetes and found that telemedicine monitoring significantly improved participants’ blood glucose regulation.
Barriers and facilitators
Three studies identified technology as a barrier to the implementation of telehealth, which was not unique to a health condition or study design. A mixed method study involving African Americans and Hispanics with mental health conditions identified initial issues with logging into the videoconferencing software and technical problems with the equipment.[59] A cross sectional study involving refugees with infectious diseases experienced technical difficulties in a quarter of the first telehealth consultations, although this significantly improved with experience.[42] A qualitative study involving African Americans and Hispanics with heart failure found that there were initial concerns with using the equipment, but these dissipated with use.[41] This study also reported issues with internet connection, using the equipment, patients managing the intervention alone at home, and concerns with patient literacy. The combined use of audio and text in the telemonitoring program assisted patients’ understanding.[41]
Six studies identified facilitators to telehealth implementation. The facilitators were not unique to a health condition or race/ethnic background. Telehealth consultations using video conferencing supported health professionals to provide education to patients with mental health conditions by sharing PowerPoint presentations and other written material.[58 ,59] Telehealth permitted caregiver engagement and could be delivered in a language of the patient and caregiver’s preference.[58 ,59] Patients from ethnic minorities reported ease of access to medical help through the GP telephone triage system.[33] Telehealth allowed patients with HIV quick access to their providers and increased their likelihood of attending appointments.[57] Patients with diabetes and hypertension gave favorable ratings to the accessibility of telehealth.[34] Strategies to assist with telehealth consultations included: face-to-face meetings prior to establishing telehealth to build relationships[59] and use of a
Satisfaction with telehealth consultations
Overall, 16 studies (57.1%) explored satisfaction with telehealth consultations. Of these, nine were quantitative studies[33 ,40 ,43 ,45 ,50 ,53 ,55 ,56 ,60], five studies were mixed methods [34 ,46 ,48 ,51 ,59] and two studies used qualitative methods.[52 ,57] Results across the sixteen studies were mixed, with the majority of studies (n=11, 68.8%) reporting high levels of satisfaction with telehealth among patients, carers and health professionals.[34 ,40 ,43 ,45 ,50–53 ,56 ,57 ,59] Reasons for satisfaction with telehealth consultations included increased efficiency and convenience, enhanced privacy and reduced need for travel compared to in person face-to-face consultations. Some studies found no discernible differences in levels of satisfaction between telehealth groups and comparison groups (i.e. usual care or face-to-face interventions)[46 ,55 ,60] and participants in one study gave mixed feedback about telepsychiatry.[48] In a study examining telephone triage, patients from ethnic minorities reported higher satisfaction in the GP triage arm compared to usual care but lower satisfaction compared with white patients overall.[33]
DISCUSSION
This systematic review examined the existing empirical literature on telehealth consultations related to racial/ethnic minorities. Findings from this review indicate that telehealth consultations for mental health and some physical health conditions between health practitioners and patients from racial/ethnic minorities offer promise across a range of outcomes and healthcare settings and can result in high levels of patient satisfaction. However, it is yet to be determined whether this translates to other healthcare settings, different health conditions and other racial/ethnic minority populations (particularly in countries outside the United States).
Despite the overall positive impact of telehealth consultations for patients from racial/ethnic minority backgrounds, some barriers and challenges were identified by the studies. Information technology required to implement telehealth consultations may be problematic for some patients from racial/ethnic minorities because of the cost of equipment, limited understanding of the use of equipment, and limited health literacy. This concurs with findings from previous reviews of telehealth consultations.[15 ,16 ,18] Additionally, there may be unique and unanticipated challenges to telehealth consultation delivery for some ethnic communities. Some racial and ethnic communities may experience anxiety regarding telecommunications including telehealth because of their perceived risk of fraudulent use of telecommunication or because of their fear of contact from immigration authorities.[46] Any barriers and challenges to use of telehealth consultations are likely to be further exacerbated by factors related to English language proficiency, cultural factors and lack of familiarity with mainstream health systems. This includes awareness of changes in government subsidies related to medical care and advice delivered via telehealth.[61]
Other literature notes that limited English proficiency can be a significant barrier to health service access and utilization for racial/ethnic minorities, including via telehealth consultations. A recent survey by Rodriguez et al.[62] found that patients with limited English proficiency had lower rates of telehealth consultation use compared with proficient English speakers. In English speaking countries, patients with limited English language proficiency may experience substantial difficulties with the use of telehealth and information technology equipment suggesting that these patients are at greater risk of receiving poorer quality healthcare when engaging in telehealth.
Furthermore, providing culturally appropriate healthcare is also important for racial/ethnic minorities.[63] In our review, some of the studies included culturally adapted materials in their telehealth consultations and used bilingual staff or interpreters and is likely to have contributed to the overall positive findings across the included studies. The cultural appropriateness and acceptability of telehealth consultations and development of cultural frameworks to guide telehealth use should be considered more broadly, particularly if services are being delivered transnationally.[64 ,65]
Overcoming barriers and challenges to telehealth should address the need for digital literacy and linguistically appropriate online information. Although the use of bilingual staff or interpreters to deliver a telehealth consultation may mitigate some of the challenges experienced by racial/ethnic minorities when using telehealth, patients may still face significant barriers due to poor digital literacy skills. Digital literacy refers to a person’s ability to use digital tools (e.g., health applications, patient portals, appointment booking) to access, understand and analyse information and communicate with others.[66 ,67] Previous studies suggest low digital literacy to be a contributing factor to racial/ethnic disparities among telehealth users.[68 ,69]
Limitations of the current evidence-base and areas for further research
This review identified key limitations of existing research in telehealth for racial/ethnic minorities. Given the increasing and more widespread adoption of telehealth consultations across the health system due to the COVID-19 pandemic, it is important to understand its impact for patients from racial/ethnic minority groups to ensure equity of healthcare access and utilization. A recent study of telemedicine use during COVID-19 has already identified disparities in telemedicine access for African American patients compared to white patients.[6]
Further research is required in other areas such as acute and chronic disease management and in other care settings for racial/ethnic minorities such as cancer care, kidney disease, emergency department admissions, critical care, pediatrics and obstetrics/midwifery. Healthcare services and institutions should monitor use of telehealth consultations across patient demographics, including language and racial/ethnic background, to measure the impact on health equity. Although our search strategy identified studies conducted in non-English speaking countries, most studies were based in the United States of America. Additional studies are required in other countries with underserved populations who may have less access to information technologies.
Included studies were also limited by a lack of methodological rigor across most study designs, resulting in a significant gap in the current evidence base. Longitudinal studies are needed to determine whether, and to what extent, telehealth consultations affect health-related outcomes over time for racial/ethnic minorities. In particular, the effects of telehealth on early identification of disease and on the long-term management of chronic health conditions are required to maximize long-term health outcomes for racial/ethnic minorities.
Patients from marginalized racial/ethnic minority groups such as refugees were only specifically studied in three of the 28 studies.[42 ,45 ,51] Issues related to caregiver support and the optimal mode of telehealth consultation delivery (i.e., telephone vs videoconferencing) should also be explored in future research.
Limitations of the review
Our review has several limitations. Only articles published in English were included therefore there is risk of publication bias. Additionally, the search period of 1 January 2005 to 9 October 2020, may have omitted earlier relevant studies. However, information technology enabling telehealth consultation has evolved considerably since the early 21st century. We anticipate that studies published prior to 2005 would have limited relevance.
CONCLUSION
This review has shown telehealth consultations to be mostly positive and beneficial to patients from racial/ethnic minority groups in terms of health outcomes, satisfaction with healthcare and accessibility of health services. Telehealth consultations delivered to patients in their preferred language or by bilingual health providers contributed to positive outcomes. Challenges to implementation of telehealth consultations across racial/ethnic minority populations were also identified and should be considered in the development and implementation of guidelines, policies and practices in relation to the use of telehealth consultations across healthcare. Further research is needed to understand the long-term impacts of telehealth use to ensure health disparities are not worsened.
Data Availability
Data is available upon request to authors
CONFLICTS OF INTEREST STATEMENT
None of the authors have conflicts of interests to declare.
FUNDING
This work did not receive any funding.
SUPPLEMENTARY FILE
ACKNOWLEDGMENTS
None.
REFERENCES




