
Abstract
The SARS-CoV-2 Delta variant is highly transmissible and contains mutations that confer partial immune escape. We compared RT-PCR cycle threshold (Ct) data from 699 test-positive anterior nasal swab specimens from fully vaccinated (n = 310) or unvaccinated (n=389) individuals. We observed low Ct values (<25) in 212 of 310 fully vaccinated (68%) and 246 of 389 (63%) unvaccinated individuals. Testing a subset of these low-Ct samples revealed infectious SARS-CoV-2 in 15 of 17 specimens (88%) from unvaccinated individuals and 37 of 39 (95%) from vaccinated people. To determine whether infectious virus titers differed in vaccinated and unvaccinated persons, we performed plaque assays on an additional set of 48 samples with Ct <25, finding no difference in infectious virus titer between groups.
Introduction
The SARS-CoV-2 Delta variant is highly transmissible and contains mutations that confer partial immune escape. Outbreak investigations suggest that vaccinated persons can spread Delta1,2 but it is uncertain whether vaccine-induced immune responses reduce nasal viral RNA burden or the titer of infectious SARS-CoV-2 in people infected despite vaccination relative to unvaccinated persons.
Methods
To estimate nasal viral RNA burden, we compared RT-PCR cycle threshold (Ct) data from 699 test-positive anterior nasal swab specimens from fully vaccinated (n = 310) or unvaccinated (n=389) individuals. “Fully vaccinated” is defined as having received a second mRNA vaccine dose or single adenovirus vector vaccine dose ≥ 2 weeks prior to testing positive. Samples were collected in Wisconsin 29 June through 31 July 2021 and tested by a single contract laboratory. During the study period, estimated prevalence of Delta variants in Wisconsin increased from 69% to over 95%. Vaccination status was determined via self-reporting and validated with state immunization records (Supplemental Figure 1). Infectious virus was quantified using plaque assays on a subset of samples with Ct values <25.
Results
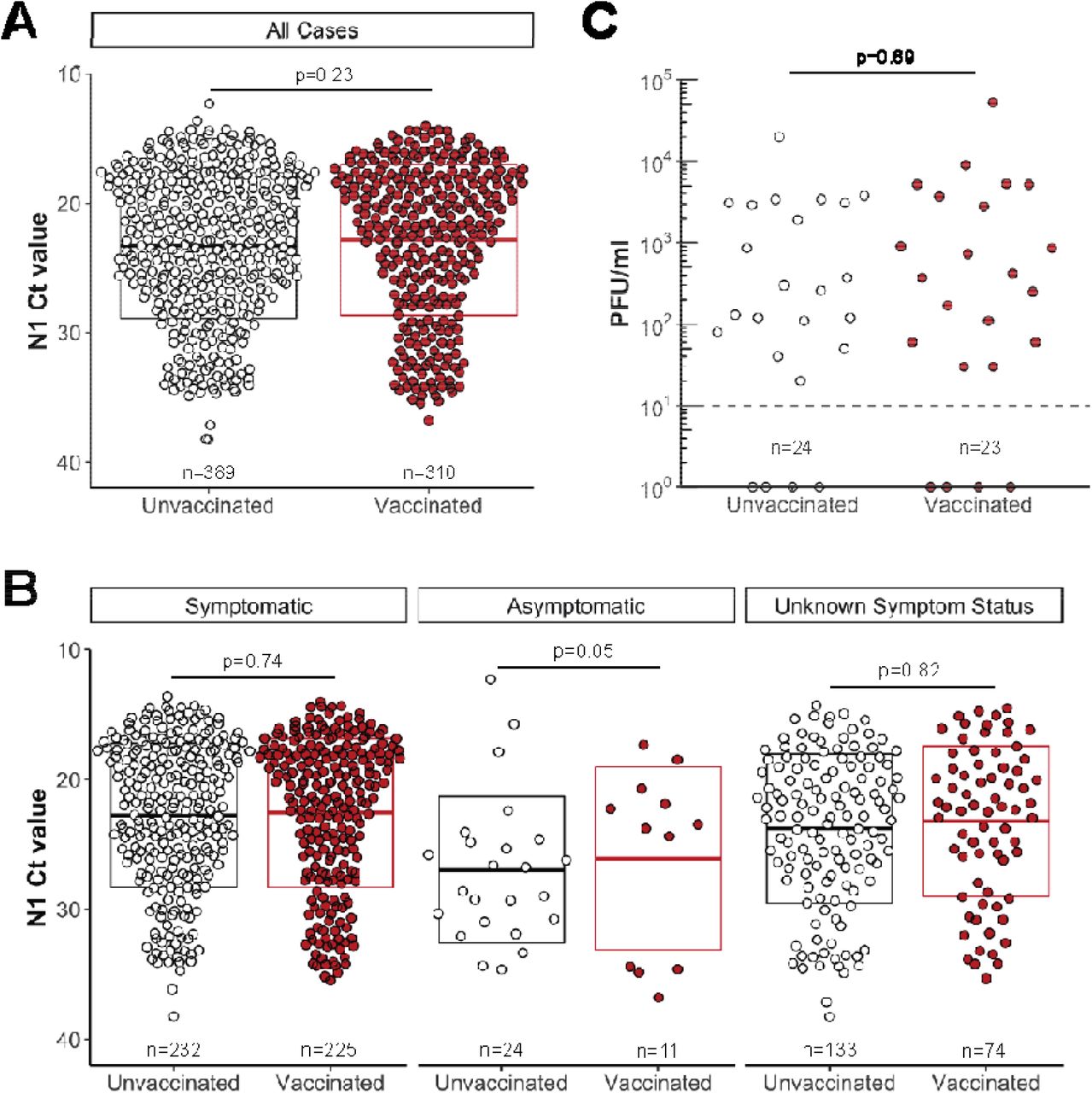
RT-PCR Ct values <25 had previously been associated with shedding of infectious SARS-CoV-2. We observed low Ct values (<25) in 212 of 310 fully vaccinated (68%; Figure 1A) and 246 of 389 (63%) unvaccinated individuals. Low Ct values were detected in vaccinated people regardless of symptoms at the time of testing (Figure 1B). Ct values <25 were detected in 7 of 24 unvaccinated (29%; CI: 13-51%) and 9 of 11 fully vaccinated asymptomatic individuals (82%; CI: 48-97%), and 158 of 232 unvaccinated (68%, CI: 62-74%) and 156 of 225 fully vaccinated (69%; CI: 63-75%) symptomatic individuals. Testing a subset of these low-Ct samples revealed infectious SARS-CoV-2 in 15 of 17 specimens (88%) from unvaccinated individuals and 37 of 39 (95%) from vaccinated people. Infectious virus was detected in the sole specimen tested from an asymptomatic fully vaccinated individual (Supplemental Figure 2). Although few asymptomatic individuals were sampled, these results indicate that even asymptomatic, fully vaccinated people might shed infectious SARS-CoV-2.

A. Ct values for SARS-CoV-2-positive specimens grouped by vaccination status. RT-PCR was performed by Exact Sciences Corporation, responsible for over 10% of all PCR tests in Wisconsin during this period, using a qualitative diagnostic assay targeting the SARS-CoV-2 N gene (oligonucleotides identical to CDC’s N1 primer and probe set) that has been authorized for emergency use by FDA (https://www.fda.gov/media/138328/download). B. N1 Ct values for SARS-CoV-2-positive specimens grouped by vaccination status for individuals who were symptomatic or asymptomatic, or those whose symptom status was not determined, at the time of testing. C. We performed plaque assays on Vero E6 TMPRSS2 cells on a subset of specimens. Specimens were selected by N1 Ct-matching between fully vaccinated and unvaccinated persons, then specimens from persons with unknown vaccination status were excluded from the analysis. Infectious titers are expressed as plaque-forming units (pfu) per milliliter specimen. Specimens underwent a freeze-thaw cycle prior to virus titration. In A and B, boxplots represent mean N1 Ct values +/- one standard deviation. P-values were calculated by comparing mean Ct values by independent two-group Mann-Whitney U tests.
To determine whether infectious virus titers differed in vaccinated and unvaccinated persons, we performed plaque assays on an additional set of 48 samples with Ct <25, finding no difference in infectious virus titer between groups (Figure 1C). Notably time from symptom onset to testing did not vary by vaccination status, suggesting that our observations are not confounded by biases in test-seeking behavior between vaccinated and unvaccinated persons (p=0.40; Supplemental Figure 3).
Discussion
Combined with other studies3,4 these data indicate that vaccinated as well as unvaccinated individuals infected with the Delta variant might transmit infection, though other studies suggest this may be relatively inefficient5. Importantly, we show that infectious SARS-CoV-2 is found at similar titers in vaccinated and unvaccinated persons when specimen Ct values are low. The inclusion of viruses from multiple counties without a linking outbreak (more than 80% of samples were not associated with an outbreak known to public health), indicate that Delta-lineage SARS-CoV-2 can achieve low Ct values consistent with transmissibility in fully vaccinated individuals across a range of settings.
Preventing infections with the Delta variant is therefore critical to stem transmission. Vaccinated and unvaccinated persons should get tested when symptomatic or after close contact with someone with suspected or confirmed COVID-19. Continued adherence to non-pharmaceutical interventions during periods of high community transmission to mitigate spread of COVID-19 remain important for both vaccinated and unvaccinated individuals. Moreover, the administration of an additional vaccine dose after the initial vaccine series dramatically reduces susceptibility to infection with the Delta variant6, providing another valuable strategy for interrupting transmission.
Data Availability
Data and processing workflows are available at https://go.wisc.edu/p22l16. To protect potentially personally identifiable information, the publicly available dataset contains only PCR Ct values, vaccine status, symptom status, culture status, and days from symptom onset to testing for each specimen.
Supplemental materials
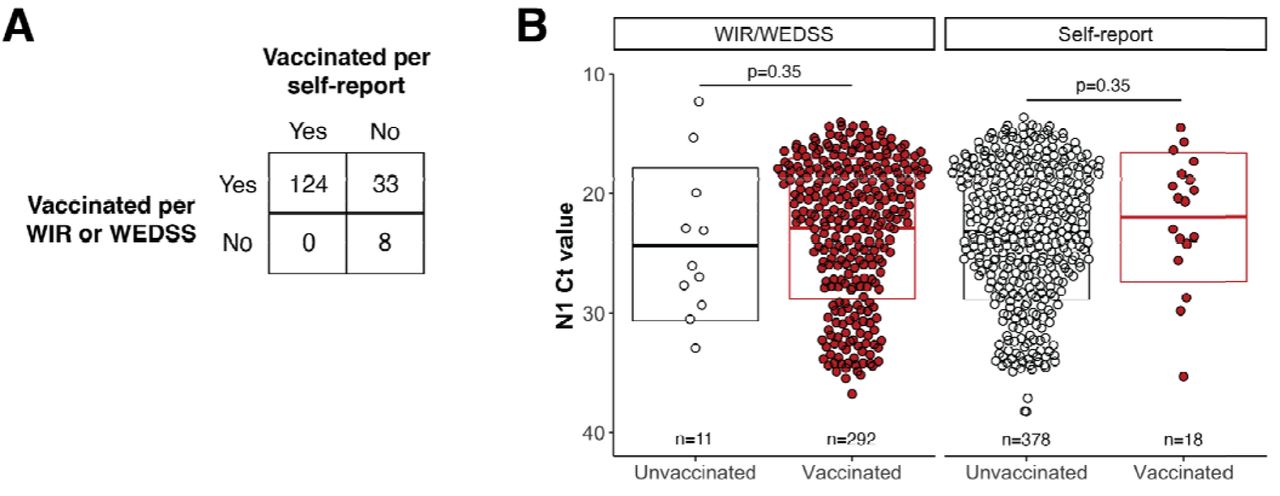
For all individuals, vaccination status was determined using WIR/WEDSS electronic registries when data were available. Individuals were identified as unvaccinated at the time of testing if WIR/WEDSS data indicated receipt of a first SARS-CoV-2 vaccine dose after the test date.
Individuals were considered fully vaccinated based on WIR/WEDSS data if the registries indicated receipt of a final vaccine dose at least 14 days prior to testing. For individuals whose vaccination status could not be verified in WIR/WEDSS, self-reported data collected at the time of testing were used.
Individuals were considered unvaccinated based on self-report only if there was an explicit declaration of unvaccinated status in the self-reported data. Individuals were considered fully vaccinated based on self-report if they fulfilled all of the following criteria: (1) indicated that they had received a COVID vaccine prior to testing; (2) indicated that they did not require another vaccine dose; and (3) reported a date of last vaccine dose that was at least 14 days prior to testing.
Specimens lacking data on vaccination status were excluded from the study. Specimens from partially vaccinated individuals (incomplete vaccine series, or <14 days post-final dose) were also excluded. Fully vaccinated status was determined by WIR/WEDSS for 292 specimens and by self-reported data for 18. Unvaccinated status was determined by WIR/WEDSS for 11 and by self-reported data by 378. A. Of the 699 specimens with vaccination status available from at least one source, 165 specimens had data available from both sources. For self-reporting, under-reporting of full vaccination status (33/157) was more common than over-reporting (0/124). B. N1 Ct values for SARS-CoV-2-positive specimens grouped by vaccination status for individuals whose vaccination status was determined by WIR/WEDDS or by self-reported data. Boxplots represent mean N1 Ct values +/- one standard deviation. P-values were calculated by comparing mean Ct values by independent two-group Mann-Whitney U tests.
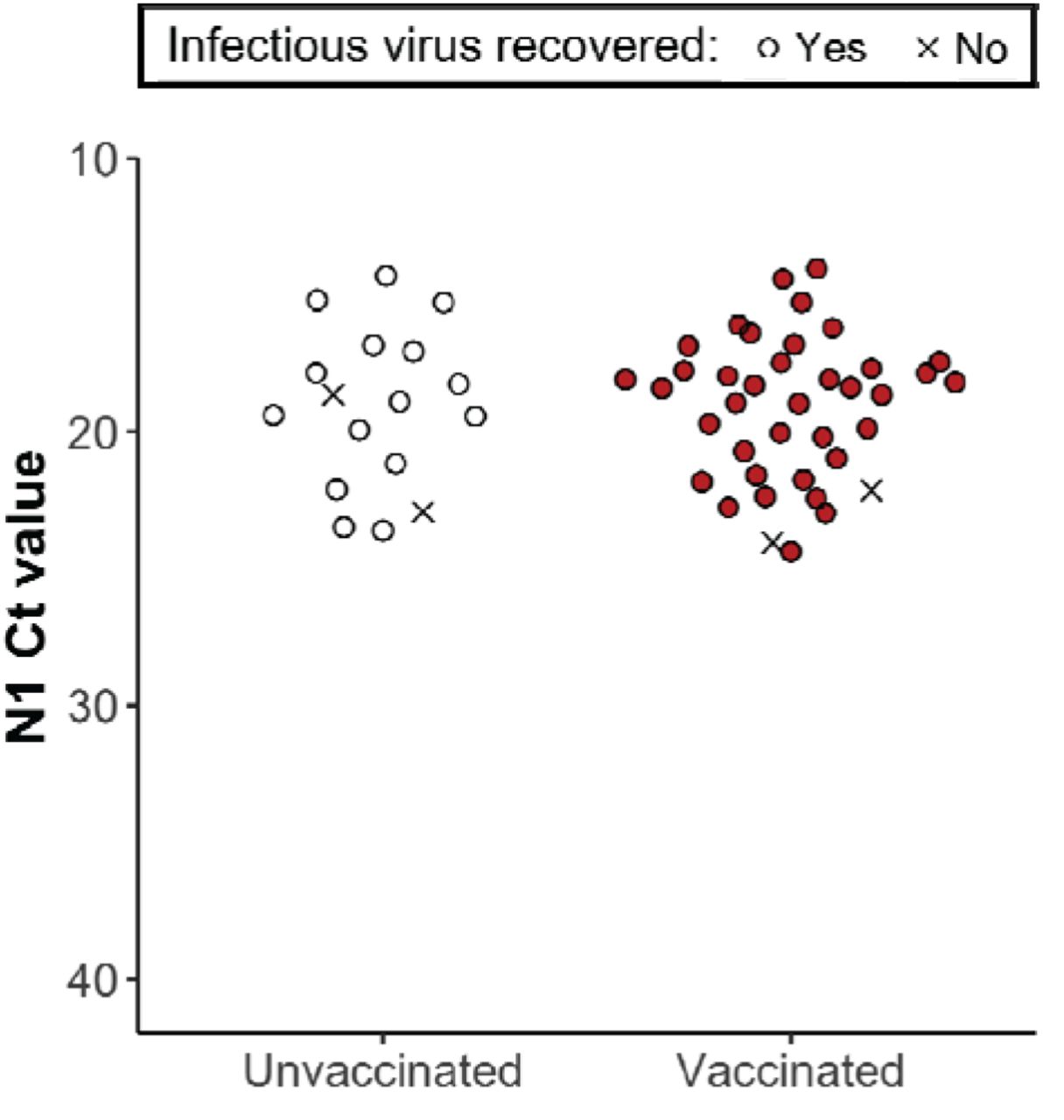
Infectiousness was determined for a subset of N1 Ct-matched specimens with Ct <25 by inoculation onto Vero E6 TMPRSS2 cells and determining presence of cytopathic effects (CPE) after 5 days in culture. Specimens with unknown vaccination status were excluded from the analysis. Circles indicate presence of CPE; ‘X’ indicates no CPE detected.

Day 0 on the x-axis denotes self-reported day of symptom onset. Negative values for days indicate specimen collection prior to symptom onset. Symptom onset data were available for n=263 unvaccinated cases and n=232 vaccinated cases.
Conflict of interest
The authors declare no conflicting interests.
Ethics statement
Per the University of Wisconsin-Madison IRB, this project qualifies as public health surveillance activities as defined in the Common Rule, 45 CFR 46.102(l)(2). As such, the project is not deemed to be research regulated under the Common Rule and therefore, does not require University of Wisconsin-Madison IRB review and oversight.
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the Centers for Disease Control and Prevention or the institutions with which the authors are affiliated.
Data availability
Data and processing workflows are available at https://go.wisc.edu/p22l16. To protect potentially personally identifiable information, the publicly available dataset contains only PCR Ct values, vaccine status, symptom status, virus culture status, and days from symptom onset to testing for each specimen.
Footnotes
The key changes in this revision are: - Lengthened text to provide additional details and cite additional recent papers





{kind=link}
{kind=link}
{kind=link}
{kind=link}