
Abstract
Background Several recent studies reported that the Covid-19 pandemic induces significant mental distress. However, it remains unknown whether mental distress persists or subsides in response to consecutive Covid-19 waves. Therefore, we here examine mental distress before and across the three Covid-19 waves.
Methods We measured stress and depressive symptoms prior to and across the three Covid-19 waves in a well-established population-based sample. A total of 330 participants completed e-questionnaires prior to and during the Covid-19 waves. Friedman’s repeated-measures and Wilcoxon rank-sum pairwise test with Bonferroni correction were used to investigate repeated-measure differences, while the Kruskal-Wallis test was used to assess the effect of behavioral and physiological parameters on mental health.
Results We found significantly increased mental distress during each of the Covid-19 waves compared with the pre-Covid-19 period. Increased mental distress was more common in women and most pronounced during the 1st and in particular, the 3rd Covid-19 wave. The stress and depressive symptoms increased during the pandemic compared with the pre-Covid-19 period by a maximum of 1.58 and 3.63 times, respectively. Negative emotions and loneliness were identified as the most significant risk factors of Covid-19-induced mental distress, while resilience was found to be protective.
Conclusions Mental distress surged during all the Covid-19 waves without showing extinction. This pattern is mechanistically reminiscent of the post-traumatic stress disorder. Our results suggest that the Covid-19 pandemic underlies the development of a novel chronic mental health disorder and do not exclude possible further deterioration of mental health in the case of future Covid-19 waves.
Introduction
The Covid-19 pandemic, which hit the world in early 2020, affected most people’s lives in many areas ranging from health to their basic needs, including social interaction and free movement. Although the effects of epidemics on mental health were described previously1–4, the magnitude of their impact on mental health only emerged during the Covid-19 pandemic5–9. This impact is documented in a string of recently reported studies10–14, which all demonstrate a significant surge in mental distress during the Covid-19 pandemic. These studies, however, often lack pre-pandemic data and do not address the effects of individual Covid-19 waves and, in general, the long-term consequences of the Covid-19 pandemic on mental health. It remains, therefore,unknown whether consecutive Covid-19 waves lead to eventual extinction15 of the Covid-19-induced mental distress similarly to other fear behaviours16,17. As a result, it also remains unclear whether the observed mental distress is a temporary short-term response to the Covid-19-pandemic or a matter of a novel pandemic-driven chronic mental health disorder sustained by the consecutive Covid-19 waves. Considering the protracted and continuously evolving course of the Covid-19 pandemic, including the emergence of novel SARS-CoV-2 variants, knowledge of the dynamics of the Covid-19-induced mental distress is imperative also to inform about mental health during probable future Covid-19 waves. We here investigate longitudinal changes in mental health before and across the three waves of the Covid-19 pandemic in a well-characterized population-based sample.
Methods
Study design and study population
Kardiovize study is a prospective longitudinal epidemiological cohort investigating cardiovascular, neuropsychiatric, and other health-related topics in Central Europe. A summary of the baseline examination protocol and general characteristics of the population-based sample have been published previously18. The inclusion criteria for the Covid-19 add-on study were all the participants of the Kardiovize study with available data on stress and depressive symptoms prior to the onset of the Covid-19 pandemic. Overview of the recruitment process for the Covid-19 add-on study has been published previously9.
Procedure
The Covid-19 add-on study was conducted across the three Covid-19 waves. The first wave took place from April 23 to May 27, 2020, during the first nationwide lockdown. The second wave took place from August 31 to October 23, 2020, following the restriction-free summer. The third wave took place from March 4 to April 7, 2021, and coincided with several months of severe restrictions. Total of 1823 Kardiovize study participants were invited to join the Covid-19 add-on study, of whom 715 participated in the first wave of the study. 330 out of 715 participants who originally enrolled into the Covid-19 add-on study (46%) completed e-questionnaire prior to and during all of the three Covid-19 waves. E-questionnaire was completed through an online survey module using validated RedCap software (Research Electronic Data Capture) tool19.
E-questionnaire
The e-questionnaire consisted of several sections that surveyed demographic characteristics, mental health (levels of stress and depressive symptoms), lifestyle changes due to the government’s measures to contain the Covid-19 transmission and select other factors that may influence mental health. The primary outcomes were stress level and severity of depressive symptoms. Stress level was measured using the Percieved Stress Scale (PSS) ranging from 0-40 and categorized as ‘low’ (score of 0-13), ‘moderate’ (score of 14-26), and ‘high’ (score of 27-40) stress20. Severity of depressive symptoms was measured using the Patient Health Questionnaire (PHQ) ranging 0-6 and the presence of depressive symptoms defined as a score ≥ 321,22. A detailed description of the other tools was published previously9.
Statistical analysis
Descriptive statistics were conducted for the socio-demographic variables. Missing values amounting to 1.8% of the total sample were identified in the pre-Covid-19 stress (N = 6) and depressive symptoms (N = 6) scales. No missing value imputations were performed. The missing data were completely at random and non-overlapping in cases. The prevalence of moderate-to-high stress and the presence of depressive symptoms was estimated as the percentage of participants meeting the cut-off values of each test. Fold change in the prevalence of mental distress described how many times the presence of elevated stress and depressive symptoms increased/decreased between study timepoints (e.g., Wave 3 prevalence divided by pre-Covid prevalence). Due to violation of the normality, we used Friedman’s repeated-measures test to evaluate overall changes in stress and depressive symptoms and the Wilcoxon rank-sum pairwise test with Bonferroni correction to identify differences between study timepoints. Kruskal-Wallis test with eta-square effect size was used to examine the impact of different variables on mental health. Data analysis and visualization were performed in the R (v.4.1.0) environment with rstatix, sjmisc, ggplot2, and pheatmap packages.
Results
The sample consisted of 330 participants who completed the e-questionnaire prior to and during all three Covid-19 waves; mean age(±SD) were 45.9 (±10.7) years and 149 (45.2%) were males. Participants were largely well-educated, considering the majority of them held university degrees (Table 1). The Covid-19 add-on study sample characteristicswere similar to the baseline Kardiovize study population-based sample, maintaining its representativeness. We observed significantly increased mean stress levels (χ2=33.622, P<0.001) during the 1st and 3rd Covid-19 waves compared with the pre-Covid-19 period as well as during the 3rd compared with the 2nd Covid-19 wave (Figure 1, eTable 1 in Supplementary Appendix). Prevalence of moderate-to-high stress increased 1.58 times during the 3rd Covid-19 wave compared with the pre-Covid-19 period (eTable 2 in Supplementary Appendix). Mean stress levels and the prevalence of moderate-to-high stress were on average 1.2 times and 1.48 times higher in women compared to men (eTables 1 and 2 in Supplementary Appendix).

Boxplots show changes in stress level scores (median, IRQ) during the individual waves of the Covid-19 pandemic. Associated bar plots show presence of moderate-to-high stress (PSS score ≥ 14), filled part denotes high stress prevalence (PSS score ≥ 27). Dashed lines show changes in mean scores for males and females separately, diamonds indicate mean scores of the sample. Horizontal upper bars represent differences between individual timepoints with indicated levels of significance (* P<.05, *** P<.001).
Similarly, we observed significantly increased severity of depressive symptoms (χ2=38.961, P<0.001) between all three Covid-19 waves and the pre-Covid-19 period as well as between the 3rd compared with the 2nd and 1st Covid-19 waves (Figure 2, eTable 1 in Supplementary Appendix). The prevalence of significant depressive symptoms increased 3.63 times during the 3rd Covid-19 wave compared with the pre-Covid-19 period (eTable 2 in Supplementary Appendix). As with stress, mean severity of depressive symptoms and the prevalence of significant depressive symptoms were on average 1.28 times and 1.55 times higher in women compared to men (eTables 1 and 2 in Supplementary Appendix).
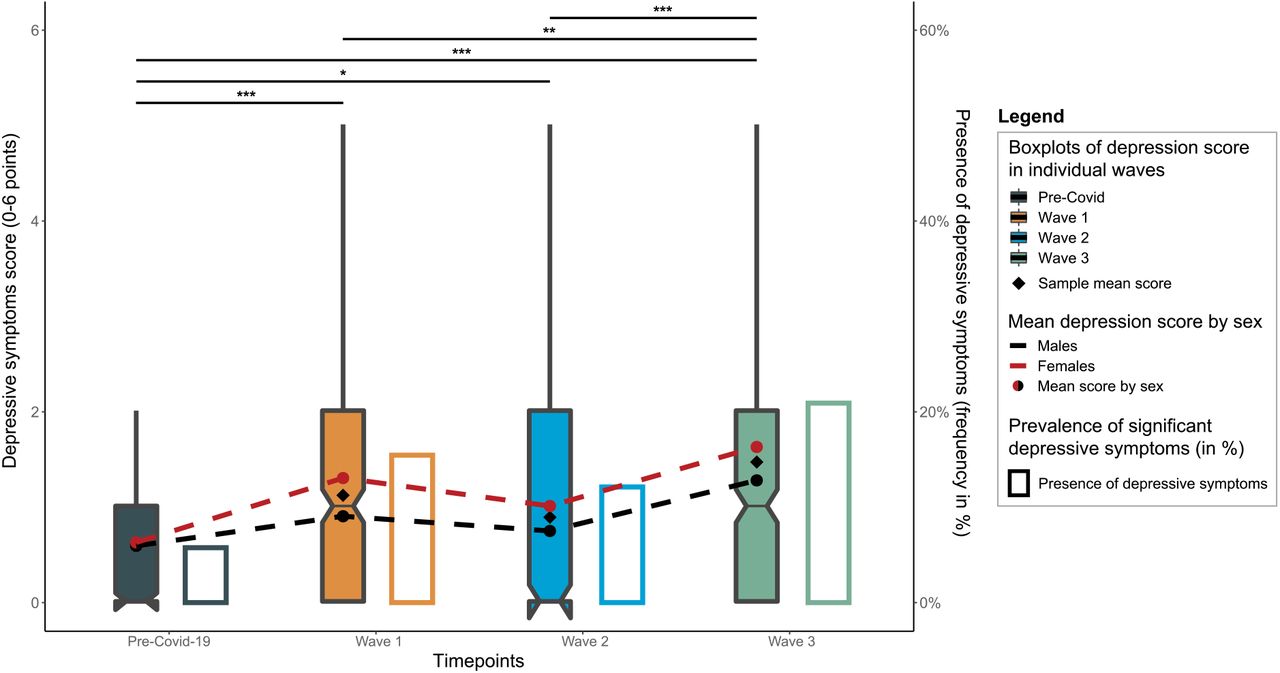
Boxplots show changes in the depressive symptoms score (median, IQR) during the individual waves of the Covid-19 pandemic. Associated bar plots show presence of significant depressive symptoms (PHQ score ≥ 3). Dashed lines show changes in mean scores for males and females separately, diamonds indicate mean scores of the sample. Horizontal upper bars represent differences between individual timepoints with indicated levels of significance (* P<.05, ** P<.01, *** P<.001).
We next searched for lifestyle and psychosocial variables that show significant association with mental distress developed during the Covid-19 pandemic. We identified negative emotional perception of the Covid-19 illness and feelings of loneliness as the most significant risk factors for developing mental distress during the Covid-19 pandemic. In contrast, higher level of resilience was found to be protective of Covid-19-induced mental distress (eFigure 1 in Supplementary Appendix).
Discussion
We examined longitudinally changes in mental health in response to the Covid-19 pandemic by measuring stress levels and severity of depressive symptoms prior to and during all three of the Covid-19 waves in a representative population-based sample. Consistent with previous findings, we find significantly increased stress levels and severity of depressive symptoms during the Covid-19 pandemic compared with the pre-Covid-19 period8,10,11,23–25 and higher mean scores and prevalence of mental distress in response to Covid-19 in women compared with men26–30.
We extend these findings by showing that the observed mental distress matched the severity of the measures undertaken during specific Covid-19 waves. More specifically, during the 1st Covid-19 wave, there were not many individuals afflicted by the SARS-CoV-2 infection in the Czech population, and people focused largely on adapting to the severely restrictive measures of the complete nationwide lockdown imposed by the government. These restrictive measures led to significant surge in mental distress7,31–34. The 2nd Covid-19 wave followed the summer vacation period with the population well acquainted with then already relaxed restrictive measures, which further increased mental distress. During the 3rd wave, however, there was a significant increase in SARS-CoV-2 infections, hospitalizations and deaths, reintroduction of severe restrictive measures, and prolonged uncertainty about “returning to the normal life” with increasing fatigue of the population, which translated into significantly increased mental distress10,35–38.
Intriguingly, consecutive Covid-19 waves did not alleviate but rather sustained mental distress. This suggests that Covid-19-induced mental distress is not a temporary short-term condition but rather a yet to be defined chronic mental health disorder. Considering fear extinction plays an important role in the pathogenesis of anxiety and the post-traumatic stress disorder17,39,40, the observed lack of decrease in mental distress following consecutive Covid-19 waves suggests that similar delayed fear extinction mechanisms may play a role also in the development of the Covid-19-induced mental distress.
We also screened for risk factors of Covid-19-induced mental distress across all the Covid-19 waves. The finding of negative emotional perception of the Covid-19 illness and feelings of loneliness as the major risk factor of Covid-19-induced mental distress is consistent with concerns about mental health, emotional experience, and in particular negative emotional perceptions of illness, as well as feelings of loneliness, both considered general risk factors of mental distress41–47. Similarly, the finding of resilience protecting against Covid-19-induced mental distress is consistent with its very definition, the ability to overcome adversity without compromising its own mental and emotional stability23,48–52.
Conclusions and recommendations
Our results demonstrate a significant increase in stress levels and severity of depressive symptoms in all three Covid-19 waves compared with the pre-Covid-19 period. This sustained state of mental distress suggests that Covid-19-induced a novel yet to be characterized chronic mental health disorder. Lack of extinction of mental distress during the consecutive Covid-19 waves further suggests that the mechanisms underlying Covid-19-related chronic mental health disorder are similar to the ones involved in the development of the post-traumatic stress syndrome. In agreement with established mental health disorders, Covid-19-induced mental distress is related primarily to the negative emotional experience and the feeling of loneliness. Further research is needed to characterize and define Covid-19-related chronic mental health disorder and decipher mechanisms underlying its pathogenesis.
Importantly, the ongoing Covid-19 pandemic with the situation in many countries now similar to the 2nd Covid-19 wave described in this study (relaxation of restrictive measures), together with delta-variant-related resurgence of Covid-19 infections, indicate high probability of further increases in mental distress. Based on the observations provided in our study, we can be concerned that future increases in mental distress might cause even greater mental health issues. Several measures can be undertaken to prevent and improve Covid-19-induced mental distress. First, more intense and better organised approaches to mental health care must be incorporated into public health policies to protect mental health. Second, individuals at high risk of developing mental distress need to be identified in a timely manner and offered appropriate interventions (increased social contacts, programs to build resilience, cognitive-behavioural techniques, etc.) 53–55. And third, the development and use of online technologies and web-based prevention and intervention tools should be incorporated into the mental health care process56,57.
Statements
Supported by the European Regional Development Fund - Project ENOCH 750 (No. CZ.02.1.01/0.0/0.0/16_019/0000868).
The research protocol was approved by St. Anne’s University Hospital ethics committee and the Internal Review Board. All participants were acquainted with the research and provided written informed consent.
Maria Vassilaki has received research funding from Roche and Biogen in the past; she currently consults for Roche, receives research funding from NIH/NIA and EU/ St. Anne’s University Hospital Brno (Czech Republic), and has equity ownership in Abbott Laboratories, Johnson and Johnson, Medtronic, and Amgen. In addition, she is currently an Associate Editor for the Journal of Alzheimer’s Disease and a Guest Editor for the Frontiers Research Topic collection ‘Multimorbidity in the Context of Neurodegenerative Disorders” (participating journals: Frontiers in Neuroscience-Neurodegeneration and Frontiers in Aging Neuroscience). No other disclosures were reported.
The data used in this study are available on request immediately following the publication to anyone who submits the online request that will be approved by the St. Anne’s University Hospital International Clinical Research Centre internal board. The researchers have to provide their research intentions and goals, and specify, and justify requested variables. The data will be provided for a limited and well-defined time via cloud service or e-mail in csv format. After defined period the data should be returned, and all other copies should be destroyed.
The authors contributed to this article as follows: GBS and JPGR conceived the idea of this study, SK, MS, APos, and APol contributed to the discussion and battery creation, JSN and Apos verified the data, JSN made the statistical analysis, JSN and GBS wrote the draft of the manuscript, MS, YEG, JRMI, FLJ, MV, GBS contributed to the discussion and reviewed. We thank the participants of the Kardiovize study for their long-term participation in this Covid-19 add-on study.
Data Availability
The data used in this study are available on request immediately following the publication to anyone who submits the online request that will be approved by the St. Anne's University Hospital International Clinical Research Centre internal board. The researches have to provide their research intentions and goals, and specify, and justify requested variables. The data will be provided for a limited and well-defined time via cloud service or e-mail in csv format. After defined period the data should be returned, and all other copies should be destroyed.
Footnotes
Minor grammatical corrections, correction of values in supplementary eTable 2, addition of statistical comparison of sexes in supplementary eTable 1, revision of comparison of mental distress within sexes based on corrected values, addition of second author affiliation.





{kind=link}
{kind=link}